Complete acetabular dissociation from axial skeleton - the 'floating acetabulum'
- SPUR SIGN is PATHOGNOMONIC - intact ilium above detached columns
- Entire articular surface is FLOATING (not attached to spine)
- Most common associated pattern in Letournel classification
- Secondary congruence may allow conservative treatment in elderly
- Young patients with displaced fractures need ORIF
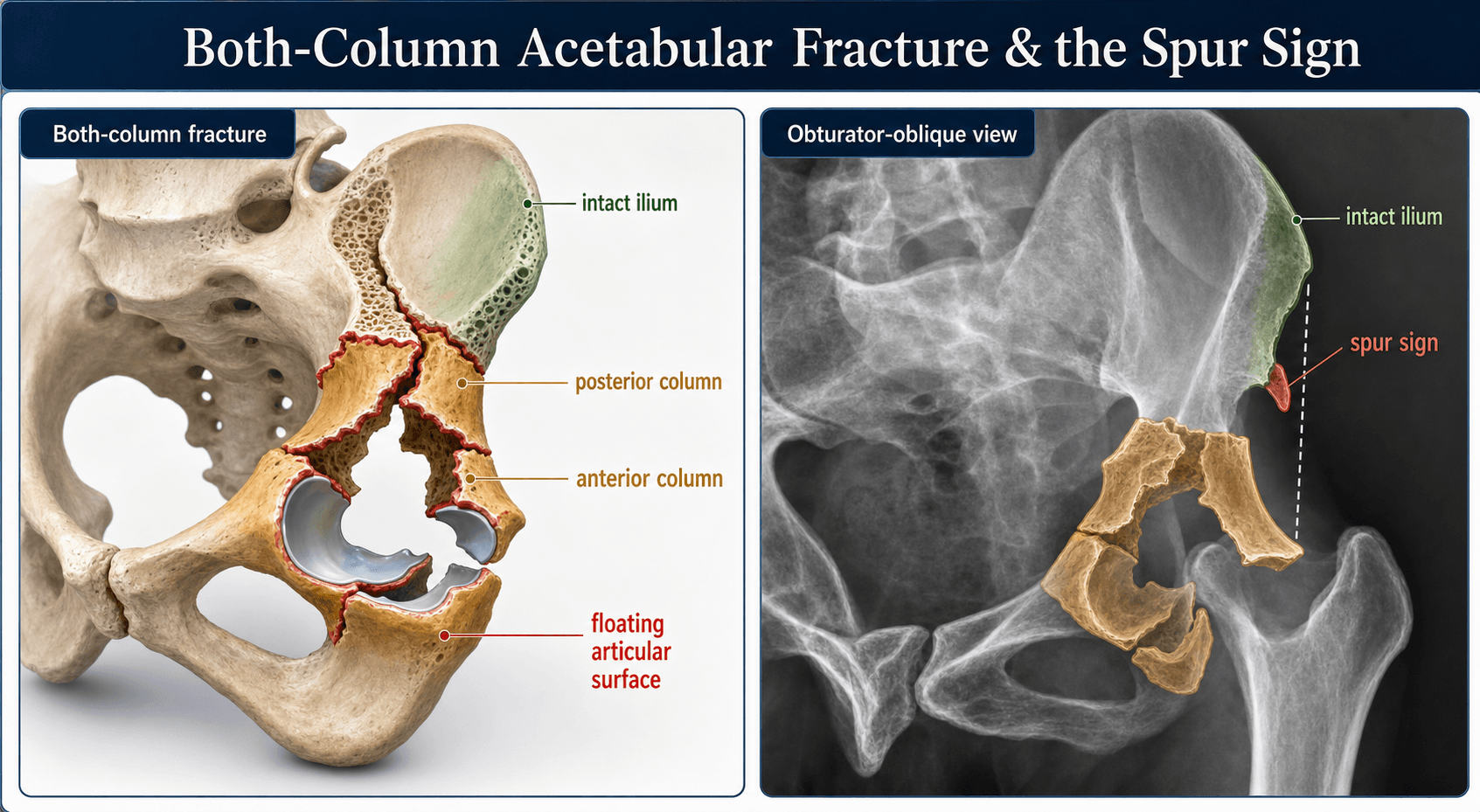
- “Spur sign = both column (on obturator oblique view)
- “Distinguishing from transverse: transverse maintains some dome attachment
- “Iliopectineal AND ilioischial lines both disrupted
- “Secondary congruence: femoral head pushes fragments into alignment
- “Combined approaches often needed (ilioinguinal + Kocher-Langenbeck)
Spur Sign (Obturator Oblique): Represents intact superior ilium above the floating acetabulum. The key diagnostic feature.
Total Dissociation: NO part of the articular surface remains attached to the axial skeleton.
Transverse: Roof remains attached to ilium. Both Column: Roof is detached (floating).
Double Trouble: Both iliopectineal (anterior) AND ilioischial (posterior) lines are disrupted.
- Finding
- Pathognomonic for both column
- Action
- CT scan for surgical planning
- Finding
- Femoral head reduces fragments
- Action
- Consider non-operative in elderly
- Finding
- Displaced fragments, incongruent
- Action
- ORIF indicated
- Finding
- Any displacement beyond 2mm
- Action
- Surgical fixation required
- Finding
- Femoral head centered under roof
- Action
- May tolerate some displacement
BOTHBOTH - Both Column Key Features
Hook:BOTH columns fractured with NO attachment to spine - look for the SPUR sign
SPURSPUR - The Pathognomonic Sign
Hook:The SPUR sign on obturator oblique confirms both column - intact ilium above floating acetabulum
FLOATFLOAT - Floating Acetabulum Concept
Hook:The entire acetabulum FLOATs free - no attachment to spine in both column fractures
Overview and Epidemiology
Introduction
Both column acetabular fractures are the most common associated pattern in the Letournel classification, representing 20-25% of all acetabular fractures. The defining characteristic is that both the anterior and posterior columns are completely fractured, with no portion of the articular surface remaining attached to the intact ilium above.
This creates a "floating acetabulum" where the entire articular segment is dissociated from the axial skeleton. The intact superior ilium remains attached to the sacrum, but the entire acetabulum floats free below.
Key Concept: The Floating Acetabulum
- Both anterior AND posterior columns fractured
- Fracture lines extend ABOVE the dome (roof)
- No articular fragment attached to axial skeleton
- Entire weight-bearing surface is "floating"
- Intact ilium forms the "spur" sign
- Transverse: Some dome remains attached to ilium above
- Both column: NO dome attachment to axial skeleton
Epidemiology
- 20-25% of all acetabular fractures
- Most common associated pattern
- Complex injury requiring expert management
- High-energy trauma (MVA, falls)
- Axial load through femoral head
- Force transmitted to both columns
- Often associated with dashboard injuries
- Young patients: High-energy trauma
- Elderly: Lower energy (osteoporotic bone)
- Male predominance in young
- Bimodal age distribution
Anatomy and Biomechanics
Acetabular Anatomy
Understanding the column concept is essential for classifying acetabular fractures.
The Two-Column Model
- Extends from iliac crest to symphysis
- Includes: Iliac wing anterior portion, anterior wall, pubic ramus
- Forms anterior half of acetabular dome
- Represented by iliopectineal line on X-ray
- Extends from greater sciatic notch to ischial tuberosity
- Includes: Greater sciatic notch, posterior wall, ischial tuberosity
- Forms posterior half of acetabular dome
- Represented by ilioischial line on X-ray
Radiographic Lines
- Runs from iliac crest to pubis
- Represents anterior column
- Disrupted in anterior column fractures
- Runs from greater sciatic notch to ischium
- Represents posterior column
- Disrupted in posterior column fractures
- BOTH iliopectineal AND ilioischial lines disrupted
- Plus SPUR SIGN
Classification Systems
Elementary Patterns (5):
Anterior wall involves isolated anterior wall fracture. Anterior column extends from iliac crest to pubis. Posterior wall is the most common elementary pattern. Posterior column involves the ilioischial line. Transverse fracture divides acetabulum into superior and inferior halves.
Associated Patterns (5):
T-shaped combines transverse with vertical component. Posterior column plus posterior wall is a common combination. Transverse plus posterior wall involves additional instability. Anterior column/wall plus posterior hemitransverse is complex associated pattern. Both column (this topic) is the most common associated pattern at 20-25%.
Both column fracture is distinguished from transverse by the spur sign and complete dissociation. In transverse fractures, some dome remains attached to axial skeleton above the fracture. In both column, NO articular surface has any attachment to the spine - the entire acetabulum floats.
Differential Diagnosis (Distinguishing Patterns)
- Discriminating feature
- NO articular fragment attached to axial skeleton (floating acetabulum)
- Lines / sign
- Spur sign on obturator oblique; both lines disrupted
- Why it matters
- Only pattern with secondary congruence; anterior/combined access
- Discriminating feature
- Roof segment remains attached to intact ilium
- Lines / sign
- No spur sign; both lines broken at one level
- Why it matters
- No secondary congruence; level dictates approach
- Discriminating feature
- Posterior column broken only below (hemitransverse); part of roof stays attached
- Lines / sign
- Iliopectineal line broken; partial ilioischial break
- Why it matters
- Mimics both column but NOT floating - no true spur
- Discriminating feature
- Transverse plus vertical (stem) split of the inferior fragment
- Lines / sign
- Both lines plus obturator ring disruption
- Why it matters
- Quadrilateral plate displacement; harder reduction
- Discriminating feature
- Marginal impaction / posterior instability dominates
- Lines / sign
- Posterior wall fragment on obturator oblique
- Why it matters
- Hip instability and AVN risk dominate
Clinical Assessment
History and Mechanism
- Motor vehicle accident (dashboard injury)
- Motorcycle accident
- Fall from height
- Pedestrian struck
- Sports (skiing, equestrian)
- Axial load through femoral head
- Position of hip determines fracture pattern
- Both columns receive force
Physical Examination
- Polytrauma common - ATLS approach
- Associated pelvic ring injury possible
- Ipsilateral lower extremity injuries
- Shortened, externally rotated limb (if dislocated)
- Pain with hip motion
- Unable to bear weight
- Tenderness over hip/pelvis
Sciatic nerve injury occurs in 10-15% of acetabular fractures, especially posterior patterns. Document detailed L5 (great toe extension) and S1 (ankle plantarflexion) function BEFORE any intervention. Peroneal division is more vulnerable - foot drop is the classic presentation.
- Hip flexion (L1-2)
- Knee extension (L3-4)
- Ankle dorsiflexion (L4-5)
- Great toe extension (L5) - most vulnerable
- Ankle plantarflexion (S1)
- Lateral thigh (L2)
- Medial leg (L4)
- Dorsum foot (L5)
- Lateral foot (S1)
Associated Injuries
Common Associations:
- Femoral head fractures (Pipkin)
- Femoral neck fractures
- Hip dislocation
- Ipsilateral knee injuries (dashboard)
- Contralateral injuries
Investigations
Imaging Protocol
Plain Radiography (Judet Views)
- AP pelvis
- Obturator oblique (45 degrees)
- Iliac oblique (45 degrees)
- Both iliopectineal AND ilioischial lines disrupted
- Roof involvement
- Femoral head position
- SPUR SIGN visible - pathognomonic
- Anterior column profile
- Posterior wall en face
- Posterior column profile
- Anterior wall en face
- Greater sciatic notch
CT Imaging
- 2mm axial cuts through acetabulum
- 3D reconstructions extremely helpful
- Coronal and sagittal reformats
- Fracture extent in both columns
- Articular surface congruence
- Femoral head integrity
- Intra-articular fragments
- Marginal impaction
- Demonstrates both column disruption
- Shows floating acetabulum concept
- Excellent for surgical planning
- Communication with patient/team
Secondary Congruence Assessment
- Femoral head pushes fractured acetabular fragments into alignment
- Creates acceptable articular surface despite fracture
- May allow conservative treatment in select cases
- Roof arc measurements
- Articular step-off
- Gap assessment
- Overall congruence
Roof Arc Angles (Matta) and the CT Subchondral Arc
The roof arc angles quantify whether the weight-bearing dome is intact. Each is measured from the geometric centre of the acetabulum between a vertical line and a line to the fracture exit through the roof, on the three plain views:
- Medial roof arc — on the AP view
- Anterior roof arc — on the obturator oblique view
- Posterior roof arc — on the iliac oblique view
If all three arcs exceed ~45°, the superior weight-bearing dome is intact and the fracture may be managed non-operatively. The CT equivalent is the subchondral (10 mm) arc rule: if the fracture spares the cranial 10 mm of subchondral bone on the top axial cuts, the dome is preserved.
Roof arc angles are validated for transverse and column (anterior/posterior) patterns — they cannot be applied to posterior wall fractures (the dome is intact but the hip is unstable) and they are not meaningful in a both-column fracture, because no roof remains attached to the axial skeleton. In the both-column fracture the analogous question is whether secondary congruence has restored a functional articular surface.

Management
Indications:
Secondary congruence present with femoral head molding fragments into alignment. Elderly low-demand patients with acceptable articular surface. Medical comorbidities precluding major surgery. Roof arc measurements greater than 45 degrees in all planes. Minimal displacement with acceptable articular congruence.
Secondary Congruence Concept:
Femoral head acts as mold and pushes fragments into alignment. Creates functional weight-bearing surface despite fracture. More common in elderly patients with comminuted fractures. Unique to both column fractures where entire acetabulum floats.
Protocol:
Skeletal traction initially for 2-4 weeks followed by progressive mobilization. Weight-bearing restrictions maintained for 6-12 weeks. Serial radiographs to monitor alignment. Conversion to surgery if alignment lost.

The key to both column management is secondary congruence assessment. If the femoral head has molded the floating acetabulum into acceptable alignment, conservative treatment may succeed in elderly patients. Young patients with displacement need ORIF regardless of secondary congruence.
Surgical Technique
Access Provided:
Anterior column from iliac crest to pubic symphysis. Quadrilateral surface and inner table of ilium. Superior pubic ramus and pelvic brim.
Indications:
Anterior column-predominant both column fractures. High both column variants exiting through iliac crest.
Key Structures at Risk:
External iliac vessels in middle window. Femoral nerve lateral to vessels. Lateral femoral cutaneous nerve over ASIS. Corona mortis (aberrant obturator artery) in 15-30% of cases.
Technique Highlights:
Three windows created (lateral, middle, medial). Lateral femoral cutaneous nerve identified and protected. Iliac vessels and femoral nerve protected in middle window.
Anterior approach: Corona mortis crosses surgical field in 15-30% - ligate before division. External iliac vessels protected in middle window. Posterior approach: Sciatic nerve must be identified and protected throughout. Avoid excessive retraction which damages medial femoral circumflex artery.
Complications
Early Complications
- Sciatic nerve (10-15%)
- Peroneal division most vulnerable
- Document preoperatively
- Corona mortis (ilioinguinal approach)
- Superior gluteal artery (posterior approach)
- External iliac vessels
- Very high DVT risk
- PE significant concern
- Prophylaxis essential
- Surgical site infection
- Higher with extensive approaches
- Proper skin handling important
Late Complications
- Most common long-term complication
- Related to reduction quality
- Greater than 3mm step-off strongly predictive
- May need THR
- Common after extensive approaches
- Prophylaxis: Indomethacin or radiation
- May limit ROM
- Associated posterior dislocation
- Delay in reduction
- Poor prognosis
Postoperative Care
First 48-72 Hours:
Monitor for compartment syndrome and neurovascular status. DVT prophylaxis is mandatory given high risk. Wound care with drain removal at 24-48 hours. Pain management and early mobilization as tolerated.
Weight-Bearing:
Touch weight-bearing initially with crutches or frame. Progression based on fracture pattern and fixation stability. Protected weight-bearing for 8-12 weeks typically.
Outcomes/Prognosis
Anatomic reduction (less than 1mm) achieves 80% good to excellent results. Reduction quality is the strongest predictor of outcome. Combined approaches allow adequate access for most patterns.
Articular step-off greater than 3mm strongly predicts arthritis. Associated femoral head injury worsens prognosis. Delay in surgery beyond 3 weeks compromises reduction.
- Step-off
- Less than 1mm
- Good/Excellent Outcome
- 80-90%
- Step-off
- 1-3mm
- Good/Excellent Outcome
- 60-70%
- Step-off
- Greater than 3mm
- Good/Excellent Outcome
- Less than 30%
Guidelines, Registries & Global Practice
Global Epidemiology
According to large registry data, the epidemiology of acetabular fractures is shifting worldwide from high-energy injuries in young men towards low-energy falls in older adults. In the German Pelvic Multicentre registry of 2,853 unilateral acetabular fractures, the mean age was 61.5 years and rising, with a parallel shift from simple patterns to complex fractures involving the anterior column. Both-column fractures are the single most common associated pattern, accounting for roughly a third of operatively treated acetabular fractures in the Matta series.
National Registry: Epidemiologic & Treatment Trends
- German Pelvic Multicentre registry: 2,853 acetabular fractures over 10 years; mean age 61.5 years and rising, with a shift from simple patterns towards complex anterior-column-involving fractures.
- Operative treatment in 62.5%; anterior intrapelvic approaches progressively replaced the extrapelvic ilioinguinal approach. Anatomical reduction in only 47.4% (31.7% imperfect, 20.9% poor); high-volume centres achieved significantly better reductions. In-hospital mortality stable at 3.3%.
Guideline & Society Positions (Side by Side)
- Position
- Restore congruent, stable joint; anatomical reduction of articular surface; anterior intrapelvic / ilioinguinal for anterior-dominant both-column
- Evidence basis
- Expert consensus + observational series
- Position
- Suspected acetabular fractures referred early to a specialist pelvic & acetabular unit; CT for all; definitive surgery by a specialist team
- Evidence basis
- Standard of care / consensus
- Position
- Centralisation to high-volume centres improves reduction quality and outcome
- Evidence basis
- Registry & observational
- Position
- Consider fix-and-replace or acute total hip arthroplasty when articular surface is non-reconstructable
- Evidence basis
- Level IV (Mears)
The "Gull Sign" in Geriatric Acetabular Fractures
In older patients (typically an anterior-column / anterior-column-posterior-hemitransverse pattern), superomedial dome impaction produces a characteristic radiographic "gull sign" (a seagull-wing appearance of the impacted roof). It is an important predictor of poor ORIF outcome — the impacted, osteoporotic articular surface is difficult to reconstruct durably — and is one of the features (alongside femoral-head impaction, marginal/articular comminution and large-area dome impaction) that favours acute total hip arthroplasty / fix-and-replace over attempted reconstruction in the frail elderly.
Registry Evidence
Joint and trauma registries (the German Pelvic Registry, and for the arthroplasty endpoint the NJR of England and Wales, AOANJRR in Australia, AJRR in the USA and the Swedish/Nordic registries) consistently show two themes: reduction quality and outcome improve with surgeon and centre volume, and a growing proportion of older patients are managed with primary or salvage total hip arthroplasty rather than ORIF.
Global Practice Variation
- High-resource settings: routine CT with 3D reconstruction, anterior intrapelvic (Stoppa-type) approaches, and increasing fix-and-replace/acute THA in the elderly.
- Limited-resource settings: greater reliance on traction and non-operative management exploiting secondary congruence, and on single-approach plating where combined exposures or arthroplasty are not feasible.
- Universal principles: early specialist referral, meticulous documentation of sciatic nerve function, thromboprophylaxis, and heterotopic ossification prophylaxis (indometacin or single-dose radiotherapy) after extensile posterior exposures.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old woman is in a high-speed MVA. X-rays show disruption of both iliopectineal and ilioischial lines, with a spur sign on obturator oblique. CT confirms both column acetabular fracture with 5mm articular step-off. Describe your management approach.”
“Explain the spur sign and how it distinguishes both column fractures from transverse fractures.”
“An 80-year-old woman with multiple comorbidities has a both column acetabular fracture from a low-energy fall. CT shows secondary congruence with acceptable articular alignment. How would you manage this patient?”
MCQ Practice Points
Q: Which radiographic sign is pathognomonic for both column acetabular fractures?
A: SPUR sign on obturator oblique view. The spur represents intact superior ilium above the completely detached anterior and posterior columns. This sign confirms that NO articular surface remains attached to the axial skeleton.
Q: How do you differentiate both column fracture from transverse fracture?
A: Spur sign is present only in both column fractures. In transverse fractures, some dome remains attached to the axial skeleton above the fracture line. In both column, NO articular surface has any attachment to the spine - the entire acetabulum floats.
Q: Which radiographic lines are disrupted in both column acetabular fractures?
A: BOTH iliopectineal AND ilioischial lines are disrupted. Iliopectineal represents anterior column, ilioischial represents posterior column. Disruption of both confirms involvement of both columns.
Q: What is secondary congruence and when does it allow conservative treatment?
A: Secondary congruence occurs when the femoral head molds the floating acetabular fragments into acceptable alignment. It is unique to both column fractures and may allow conservative treatment in elderly, low-demand patients with acceptable roof arc measurements.
Q: What is the most important prognostic factor after acetabular fracture surgery?
A: Reduction quality. Anatomic reduction (less than 1mm step-off) achieves 80-90% good outcomes. Greater than 3mm step-off is strongly predictive of post-traumatic arthritis.
Key Features
- 20-25% of acetabular fractures (most common associated)
- NO articular segment attached to axial skeleton
- BOTH iliopectineal AND ilioischial lines disrupted
- SPUR sign on obturator oblique is pathognomonic
Radiographic Findings
- Obturator oblique shows SPUR sign
- Both column lines disrupted
- CT with 3D for surgical planning
- Assess for secondary congruence
Management
- Young patient displaced: ORIF (combined approaches)
- Elderly with secondary congruence: conservative
- Timing: within 2 weeks for best outcomes
- Reduction goal: less than 2mm step-off
Surgical Approaches
- Ilioinguinal for anterior column
- Kocher-Langenbeck for posterior column
- Combined approaches often needed
- Sciatic nerve injury risk 10-15%
Key Pitfalls
- Missing spur sign (only on obturator oblique)
- Confusing with transverse (transverse has dome attached)
- Not documenting sciatic nerve preoperatively
- Delaying surgery beyond 2 weeks
Evidence Base
Letournel Classification & Congruence (Founding Paper)
- Letournel's founding paper codified the ten-pattern column classification and the principle that outcome is governed by congruence between the femoral head and acetabular roof.
- Defined total, partial and apparent (secondary) incongruence; in nine fractures, displaced fragments regrouped around the femoral head to give apparent congruence, with seven achieving very good clinical results despite overall displacement.
Both-Column Outcomes & Secondary Congruence Biomechanics
- In a cohort of both-column fractures treated with anterior and posterior (bicolumnar) plating, 80% achieved excellent-to-good results with a mean modified Harris Hip Score of 85.7.
- Highlights that biomechanical data show non-operative reliance on secondary congruence raises peak supra-acetabular contact pressures, with a risk of post-traumatic osteoarthritis, supporting operative reconstruction in fit patients.
Operative Series: Both-Column Most Common Associated Pattern
- In 262 displaced acetabular fractures operated within 21 days, associated patterns accounted for 79%, with both-column the single most common type (92 hips, 35%).
- The vast majority were managed through a single approach (Kocher-Langenbeck, ilioinguinal or extended iliofemoral); only 4 hips required a combined ilioinguinal plus Kocher-Langenbeck exposure.
Acute Total Hip Arthroplasty for Selected Fractures
- In 57 patients (mean age 69) with displaced acetabular fractures and features predicting poor ORIF outcome (articular comminution, full-thickness cartilage loss, femoral head impaction, acetabular impaction of more than 40% of the joint surface), acute THA gave 79% excellent or good results at a mean of 8.1 years.
- No cup or stem developed late loosening, establishing acute arthroplasty as a viable primary option in the elderly with non-reconstructable joint surfaces.
Corona Mortis Anatomy: Surgical Hazard
- In 62 hemipelvises dissected via the anterior intrapelvic approach, a corona mortis anastomosis between the obturator and external iliac systems was present in 50 (80.6%).
- The venous variant (40.3%) was more frequent than the arterial variant (16.1%); venous bleeding behind the superior pubic ramus is harder to control.
Reduction Quality Predicts Outcome (Matta Series)
- Across 262 displaced acetabular fractures, anatomical reduction was achieved in 71% and correlated closely with the clinical result; the overall outcome was excellent or good in 76% of hips.
- The rate of anatomical reduction fell with increasing fracture complexity, older age and longer injury-to-surgery interval; outcome was worsened by femoral head injury and operative complications.