High-Energy Posterior Pelvic Injuries | Denis Zones | Neurological Risk
- Denis zones predict NEUROLOGICAL injury risk (lateral to central progression)
- CT is ESSENTIAL - 30-50% missed on plain radiographs
- Zone III involves sacral canal = cauda equina symptoms (bowel/bladder/sexual)
- Spinopelvic dissociation = complete disconnection of spine from pelvis
- Document bowel, bladder, sexual function (sacral roots S2-S4)
- “Zone I: 5-10% neuro injury (L5 nerve - foot drop risk)
- “Zone II: 25-30% neuro injury (S1-S2 roots - plantarflexion/sensation)
- “Zone III: Up to 60% neuro injury (cauda equina - emergency!)
- “U-shaped (Roy-Camille) fractures = spinopelvic dissociation = highest neuro rate
- “SI screws must avoid foramina and target S1 body (safe corridor)
Sacral fractures are frequently MISSED on plain radiographs (30-50%). CT is ESSENTIAL for diagnosis and surgical planning. The Denis classification predicts neurological injury based on fracture location: Zone I (5-10%), Zone II (25-30%), Zone III (up to 60%). Zone III fractures involve the sacral canal and can cause cauda equina syndrome with bowel, bladder, and sexual dysfunction.
Overview
Introduction
Sacral fractures occur in approximately 45% of pelvic ring injuries and are among the most commonly missed fractures in trauma. The dense bony overlap on plain radiographs makes visualization difficult, and CT imaging is essential for diagnosis.
The sacrum plays a critical role as the posterior keystone of the pelvic ring, transferring weight from the spine to the lower extremities. Sacral fractures can occur in isolation (stress fractures, falls) or as part of complex pelvic ring injuries (vertical shear, LC, APC patterns).
Clinical Significance
Why Sacral Fractures Matter:
- Frequently missed: Up to 50% missed on plain X-ray
- Neurological injury: 5-60% depending on zone
- Pelvic stability: Posterior structures provide 60% of ring stability
- Chronic pain: Sacroiliac dysfunction common
- Associated injuries: Often part of complex polytrauma
Epidemiology
- Present in 45% of pelvic ring injuries
- Often underdiagnosed (30-50% missed initially)
- Insufficiency fractures in elderly common
- High-energy trauma (MVA, falls)
- Vertical shear injuries
- Lateral compression injuries
- Insufficiency fractures (osteoporosis)
- Bimodal distribution
- Young: High-energy trauma
- Elderly: Insufficiency fractures
Anatomy and Biomechanics
Sacral Anatomy
Bony Anatomy
- Triangular bone of 5 fused vertebrae (S1-S5)
- Forms posterior wall of pelvis
- Articulates with L5 above, coccyx below
- SI joints bilaterally
- Lateral wing-like extensions
- L5 nerve root runs on anterior surface
- Zone I fractures occur here
- Anterior and posterior openings
- Transmit sacral nerve roots
- Zone II fractures through these
- Central canal housing cauda equina
- Zone III fractures involve this
- Highest neurological risk
Neural Anatomy
- L5 root: Exits under sacral ala, anterior surface
- S1-S4 roots: Exit through sacral foramina
- Cauda equina: Within sacral canal
- L5: Great toe extension, dorsiflexion
- S1: Ankle plantarflexion, ankle jerk
- S2-S4: Bowel, bladder, sexual function
Classification Systems
Denis Classification (Most Important)
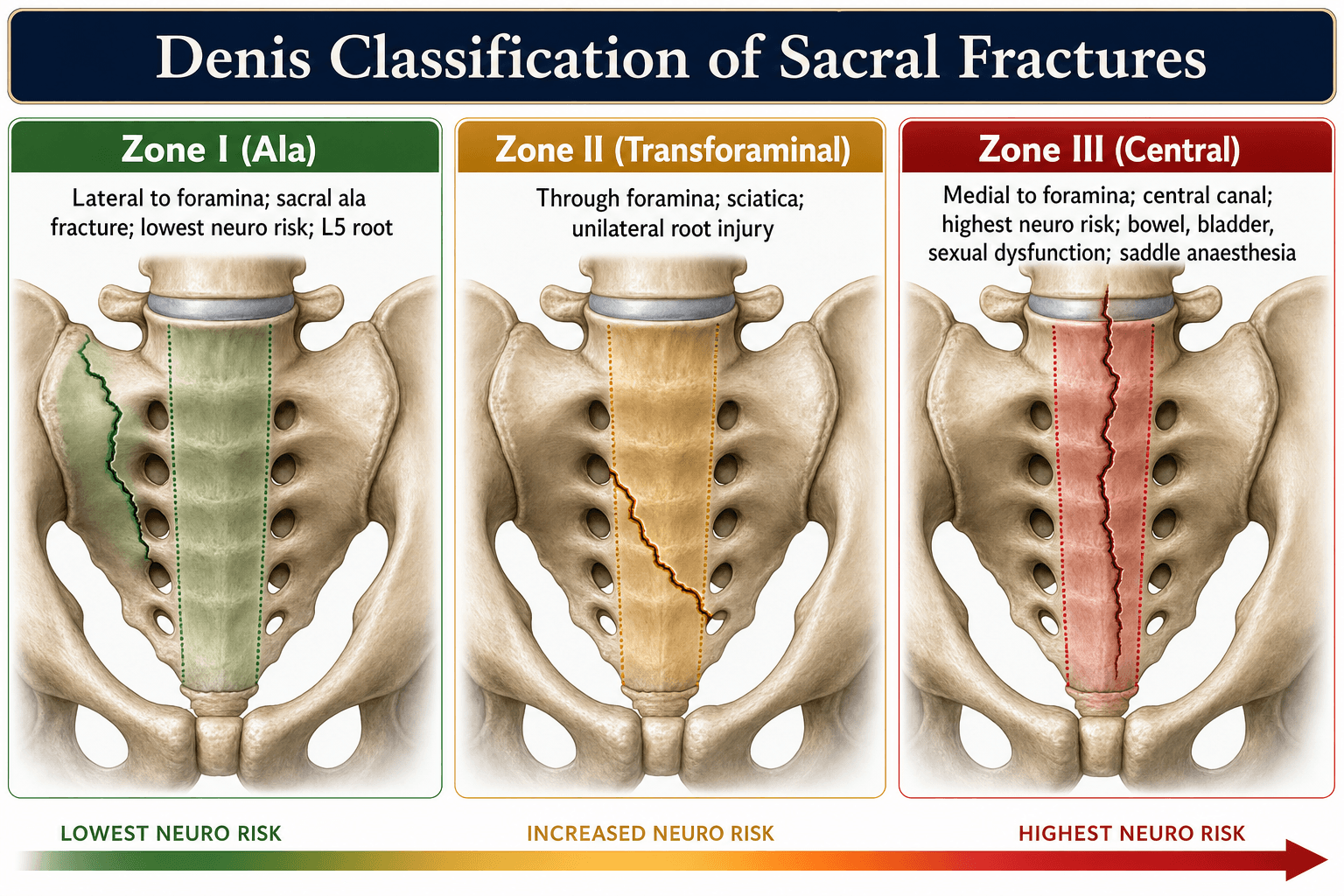
The Denis classification divides the sacrum into three longitudinal zones based on location relative to the sacral foramina. This classification predicts neurological injury risk.
- Lateral to sacral foramina
- Sacral ala region (wing)
- L5 nerve root (runs on anterior ala surface)
- 5-10%
- Foot drop (L5 weakness)
- Weak great toe extension
- Sensory loss dorsum of foot
- Usually stable fracture
- Often conservative if minimally displaced
- SI screws if unstable or displaced
.
Roy-Camille Classification (Transverse Fractures)
For transverse sacral fractures specifically:
Type I: Flexion injury, no kyphosis Type II: Flexion with posterior displacement and angulation Type III: Extension injury with anterior displacement Type IV: Comminuted fracture pattern
Spinopelvic Dissociation
- Complete disconnection of spine from pelvis
- Usually bilateral transverse sacral fractures
- U-shaped or H-shaped patterns
- Upper sacrum moves with spine
- Lower sacrum/pelvis moves independently
- Highest neurological injury rates (often greater than 60%)
- Requires lumbopelvic fixation
- Bilateral vertical fractures through sacrum
- Connecting transverse fracture component
- On imaging: spine-pelvis discontinuity
ZONESZONES - Neuro Injury Rates
Hook:ZONES increase in neuro risk as you move medially toward the canal
Denis predicts risk by fracture location; the Gibbons classification grades the actual sacral nerve deficit and is used to track recovery (it is the score quoted in outcome studies of spinopelvic dissociation): Grade 1 - no deficit; Grade 2 - sensory deficit only; Grade 3 - lower-limb motor deficit; Grade 4 - bowel or bladder (sphincter) dysfunction. The grade carries prognostic weight - higher grades (especially sphincter involvement) recover least reliably - and the change in Gibbons grade is the standard way to report neurological outcome after decompression and fixation. Pair it with a documented bulbocavernosus reflex and perianal (S2-S4) examination so the baseline deficit is unambiguous.
Clinical Assessment
Primary Survey
Sacral fractures occur in major trauma context. Assessment follows ATLS principles.
Mechanism History
- Motor vehicle accident
- Fall from height
- Pedestrian struck
- Motorcycle accident
- Insufficiency fractures
- Falls in elderly
- Osteoporosis-related
Physical Examination
- Ecchymosis over sacrum (Morel-Lavallee lesion possible)
- Lower extremity posture
- Gluteal swelling
- Sacral tenderness
- Step-off or crepitus
- SI joint tenderness
- Assess rectal tone (S2-S4)
- Rule out open fracture
- Palpate for bony fragments
Neurological Examination (CRITICAL)
Document DETAILED neurological examination in ALL sacral fractures. Include motor function (L5-S1), sensory examination, rectal tone, bulbocavernosus reflex, and specifically ask about bowel, bladder, and sexual function. Zone III fractures can cause permanent cauda equina syndrome.
- Hip extension (L5-S1)
- Knee flexion (S1-2)
- Great toe extension (L5) - KEY
- Ankle plantarflexion (S1-2)
- Ankle dorsiflexion (L4-5)
- Dorsum of foot (L5)
- Lateral foot (S1)
- Posterior thigh (S2)
- Perianal sensation (S2-S4) - saddle area
- Ankle jerk (S1-2)
- Bulbocavernosus reflex (S2-S4)
- Anal wink (S2-S4)
- Urinary retention or incontinence
- Fecal incontinence
- Erectile dysfunction (males)
- Vaginal sensation (females)
Investigations
Imaging Protocol
Plain Radiography
- Often inadequate for sacral fractures
- Look for: Asymmetry, cortical disruption
- Foraminal lines may be disrupted
- Miss rate: 30-50%
- Better visualization
- Assess for kyphosis
- Still often inadequate
- 30-degree cephalad tilt
- Better visualization of foramina
- Rarely used in acute trauma
CT Imaging (ESSENTIAL)
- Plain films miss 30-50%
- Defines fracture pattern precisely
- Denis zone classification
- Foraminal involvement
- Associated pelvic injuries
- Fracture location (Denis zone)
- Transverse vs longitudinal
- Displacement and comminution
- Foraminal compromise
- Sacral canal involvement
- Excellent for surgical planning
- Demonstrates complex patterns
- Communication tool
MRI
- Neurological deficit
- Suspected cauda equina compression
- Insufficiency fractures (edema pattern)
- Soft tissue assessment
- Nerve root compression
- Canal stenosis
- Bone marrow edema
- Soft tissue injury
Differential Diagnosis
Low back, buttock or sacral pain (especially the insidious insufficiency-fracture presentation) has several mimics. The key discriminators are mechanism, MRI signal pattern and red-flag features.
- Typical patient / clue
- Elderly, osteoporotic, no/low trauma
- Imaging discriminator
- MRI: H-shaped (Honda sign) marrow oedema, fracture line
- Why it matters
- Benign; treat conservatively + bone health
- Typical patient / clue
- Known cancer, weight loss, night pain
- Imaging discriminator
- Lytic/destructive lesion, soft-tissue mass, abnormal marrow beyond fracture plane
- Why it matters
- Must not be missed; biopsy/staging before any cement
- Typical patient / clue
- Younger, inflammatory back pain, raised CRP/HLA-B27
- Imaging discriminator
- MRI: subchondral SI joint oedema/erosions, not a fracture line
- Why it matters
- Rheumatology referral, DMARD/biologic therapy
- Typical patient / clue
- Fever, IVDU, immunosuppression
- Imaging discriminator
- MRI: joint effusion, abscess, contrast enhancement
- Why it matters
- Needs aspiration and antibiotics, not fixation
- Typical patient / clue
- Pain on sitting, distal to sacrum
- Imaging discriminator
- Localised to coccyx on lateral imaging
- Why it matters
- Usually conservative; avoids over-investigation
- Typical patient / clue
- Dermatomal leg pain, positive SLR
- Imaging discriminator
- Disc/foraminal pathology at L4-S1, sacrum normal
- Why it matters
- Different treatment pathway

Management Algorithm
Decision-Making Framework
- Zone I with minimal displacement (less than 5mm)
- Stable pelvic ring
- No neurological deficit
- Insufficiency fractures (first line)
- Initial bed rest (2-4 weeks)
- Progressive mobilization
- Weight-bearing as tolerated
- Analgesia (paracetamol, NSAIDs, opioids)
- DVT prophylaxis (LMWH)
- Serial radiographs (1, 2, 6 weeks)
- Physiotherapy for mobilization
- Most heal at 6-12 weeks
- Return to function gradual
- Monitor for late complications
.
Surgical Technique
Percutaneous Sacroiliac Screws
- Zone I and II fractures
- Longitudinal sacral fractures
- SI joint instability
- Stable to moderately unstable patterns
- Supine on radiolucent table
- Lateral decubitus alternative
- 7.3mm or 7.0mm cannulated screws
- Fluoroscopy (inlet, outlet, lateral views)
- Guidewires, cannulated instruments
-
Imaging Setup:
- Obtain true AP pelvis (inlet view)
- Obtain outlet view (40 degrees caudal)
- Obtain lateral sacrum view
- Mark S1 body corridor
-
Entry Point:
- Posterior ilium lateral to SI joint
- Approximately 1cm superior to greater sciatic notch
- Avoid L5 nerve anteriorly
-
Guidewire Insertion:
- Advance under fluoroscopic guidance
- Check all three views continuously
- Target S1 body (safe zone)
- Avoid sacral canal medially
- Avoid anterior cortex breach
-
Screw Placement:
- Measure guidewire depth
- Insert cannulated screw over wire
- Ensure bicortical purchase
- Final confirmation all views
-
S2 Screw (Optional):
- For greater stability
- Enter more cephalad
- Similar technique
- L5 nerve anterior to ala
- Sacral canal medially
- Anterior vascular structures
- Dysmorphic sacrum variants
SCREWSCREW - SI Screw Safe Placement
Hook:Use SCREW safely - target S1 body with three fluoroscopic views
Complications
Early Complications
- Most significant complication
- Zone-dependent rates (I: 5-10%, II: 25-30%, III: up to 60%)
- May be permanent especially Zone III
- Document baseline and monitor closely
- Presacral venous plexus injury
- Part of pelvic hemorrhage with ring injuries
- Usually managed with pelvic trauma protocol
- Angioembolization if ongoing bleeding
- Rarely requires surgical exploration
- High DVT risk (pelvic trauma)
- Prolonged immobility increases risk
- Chemical prophylaxis essential (LMWH)
- Mechanical prophylaxis (compression devices)
- Early mobilization when possible
- Wound infection (surgical cases)
- Deep infection rare
- Higher risk with open fractures
- Prophylactic antibiotics per protocol
Late Complications
- Sacroiliac dysfunction common (30-40%)
- Neuropathic pain
- Mechanical pain
- May require multimodal management
- SI joint injections
- Pain clinic referral
- Kyphotic deformity (transverse fractures)
- Leg length discrepancy possible
- Gait abnormality
- SI joint dysfunction
- May need corrective surgery
- Rare with adequate fixation (less than 5%)
- More common with conservative treatment
- May need revision surgery
- Bone grafting and rigid fixation
- S2-S4 root involvement
- Erectile dysfunction in males
- Vaginal sensation loss in females
- Counseling important
- May be permanent
- Impacts quality of life significantly
- S2-S4 root injury
- May require long-term management
- Intermittent catheterization
- Bowel regimen
- Multidisciplinary approach
- Urology/colorectal consultation
- Screw malposition
- Nerve injury from screw
- Implant prominence (lumbopelvic fixation)
- Implant failure (rare with modern techniques)
- May require removal after union
Postoperative Care
Immediate Postoperative Period
- Neurological observations (especially if decompression performed)
- Motor and sensory function q4h initially
- Bowel and bladder function
- Wound checks
- DVT prophylaxis
- Multimodal analgesia
- IV opioids initially
- Transition to oral medications
- Neuropathic pain agents if needed (gabapentin, pregabalin)
Early pain control is essential for neurological recovery and patient comfort.
Outcomes and Prognosis
Union Rates
- SI screw fixation: Greater than 90% union rate
- Lumbopelvic fixation: Greater than 85% union rate
- Higher union rates with stable fixation
- Nonunion rare with adequate fixation
- Most heal with conservative treatment
- Takes longer (12-16 weeks)
- Insufficiency fractures: Good healing rates
- May have residual pain even with union
Union typically occurs within 12-16 weeks with appropriate management.
Guidelines, Registries & Global Practice
OrthoVellum is a worldwide resource. The principles below describe the global standard of care and the key regional differences a candidate may be examined on at any board.
Global Epidemiology
Two distinct populations sustain sacral fractures. In Denis's defining series, sacral fractures were identified in approximately 30% of pelvic injuries (236 of 776), and modern series report sacral involvement in a large proportion of pelvic-ring trauma. The condition has a bimodal distribution: high-energy axial-loading or vertical-shear injuries in younger patients (motor-vehicle crashes, falls and jumps from height), and low-energy fragility (insufficiency) fractures in elderly osteoporotic patients, which are increasingly common as populations age.
- What it describes
- Longitudinal zone relative to foramina (I alar, II transforaminal, III central)
- What it changes in management
- Predicts neurological risk; flags Zone III for canal assessment and decompression
- What it describes
- Morphology of transverse upper-sacral fractures (Types 1-3)
- What it changes in management
- Guides reduction of kyphosis and the need for stabilisation
- What it describes
- Bilateral vertical fractures with a transverse component
- What it changes in management
- Identifies spinopelvic dissociation requiring lumbopelvic fixation
- What it describes
- Morphology plus neurological and modifier subtypes
- What it changes in management
- Standardises reporting and severity grading for comparison
Guidance Across Boards and Societies
- Practical position
- CT is mandatory; iliosacral or transsacral screws for posterior ring; triangular osteosynthesis for vertically unstable and dissociation patterns
- Evidence base
- Cadaveric biomechanics (Schildhauer 2003) and large operative series
- Practical position
- Major pelvic trauma to a specialist centre; early CT; documented lumbosacral and perianal neurological exam
- Evidence base
- Consensus standards, expert opinion
- Practical position
- Spinopelvic dissociation treated as a spinal injury: reduction quality and lumbopelvic fixation prioritised
- Evidence base
- Level IV series (Lindahl 2014)
- Practical position
- Conservative care first; bone-health work-up and anti-osteoporosis therapy; augmentation/fixation for refractory pain or instability
- Evidence base
- Level IV-V, technical reports (Tjardes 2008)
Because no high-level randomised evidence exists for most operative decisions, recommendations are largely consensus- and biomechanics-driven and converge internationally: CT for diagnosis, neurological documentation, and stabilisation of unstable or neurologically threatened patterns.
Registry and Series Evidence
Unlike arthroplasty, sacral-fracture fixation is not tracked by dedicated implant registries; the evidence base is observational. Key signals from operative series: triangular osteosynthesis resists cyclic failure far better than an isolated iliosacral screw (Schildhauer 2003), and in spinopelvic dissociation the quality of reduction, not the timing of surgery or use of laminectomy, predicts neurological and functional recovery, with around 42% of patients still having a poor clinical outcome despite fixation (Lindahl 2014).
Global Practice Variation
- High-resource settings: intraoperative 3D imaging or navigation for screw placement, dedicated pelvic-trauma teams, and ready CT/MRI.
- Limited-resource settings: greater reliance on fluoroscopy-guided technique and clinical neurological assessment; conservative management of stable patterns is appropriate worldwide.
- Fragility fractures: management is broadly conservative everywhere, but access to cement augmentation, navigated augmented screws and structured bone-health/falls-prevention services varies markedly.
Exam Focus Points
High-Yield Concepts
DENIS ZONES = NEUROLOGICAL RISK: Zone I = 5-10% (L5), Zone II = 25-30% (S1-S2), Zone III = Up to 60% (cauda equina). The zones move lateral to medial, with risk increasing toward the canal. Zone III involves the sacral canal and can cause bowel/bladder/sexual dysfunction.
Key Numbers
- 30-50%: Miss rate on plain X-ray
- Zone I: 5-10% neuro injury
- Zone II: 25-30% neuro injury
- Zone III: Up to 60% neuro injury
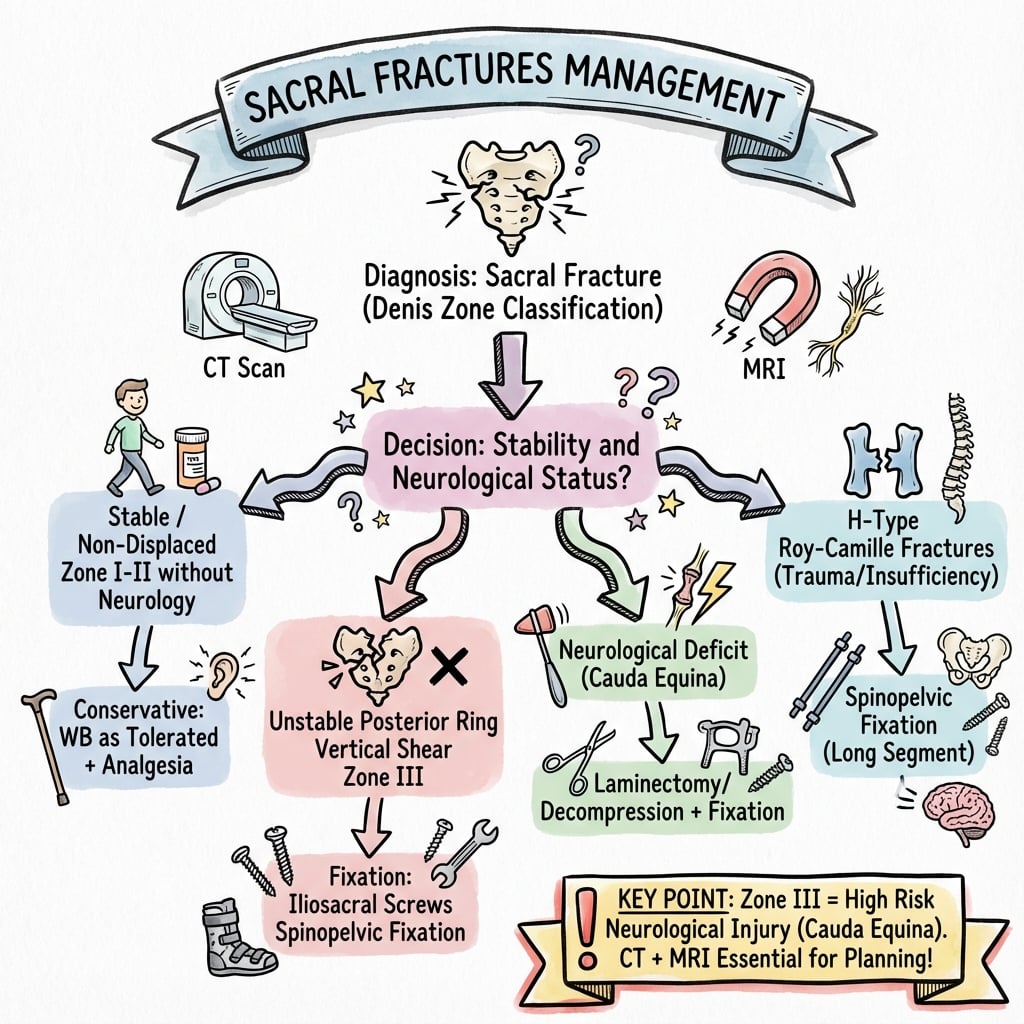
Surgical Decision-Making
- Stable, minimally displaced Zone I
- No neurological deficit
- Insufficiency fractures
- Neurological deficit with canal compromise
- Unstable pelvic ring
- Spinopelvic dissociation
- Zone III with cauda equina
Special Patterns
- U-shaped/H-shaped: Spinopelvic dissociation, lumbopelvic fixation required
- Insufficiency fractures: Conservative first, sacroplasty if refractory
Special Patterns
Insufficiency Fractures
- Fracture through weakened bone under normal physiological load
- Osteoporosis most common cause
- Elderly patient
- Low back/buttock pain
- Gradual onset
- No significant trauma
- X-ray often negative initially
- MRI: Bone marrow edema pattern
- CT: Subtle fracture lines
- Usually conservative
- Analgesia
- Osteoporosis treatment
- Sacroplasty if refractory
Denis was designed for high-energy trauma; the osteoporotic insufficiency fracture is better classified by the Fragility Fractures of the Pelvis (FFP) classification of Rommens and Hofmann, which grades by instability and directs treatment: FFP I - anterior-only injury (isolated rami) - conservative; FFP II - non-displaced posterior injury (sacral ala crush or non-displaced sacral fracture, often with anterior fractures) - conservative first, percutaneous fixation if pain or mobilisation fails; FFP III - displaced unilateral posterior injury - reduction and fixation; FFP IV - bilateral displaced posterior injury (including bilateral sacral or U-type fragility patterns) - fixation, often bilateral or transsacral/lumbopelvic. The practical message: most FFP I-II are managed conservatively with analgesia, early mobilisation and a bone-health work-up, while persistent pain or progressive displacement (II to III to IV) is the trigger for percutaneous (often cement-augmented) iliosacral or transsacral fixation. This is the framework examiners now expect for the elderly sacral insufficiency fracture.
Stress Fractures
- Athletes, military recruits
- Long-distance runners
- Activity-related pain
- Gradual onset
- Improves with rest
- Activity modification
- Typically heals with rest
- Bone health assessment
H-Type and U-Type Sacral Fractures
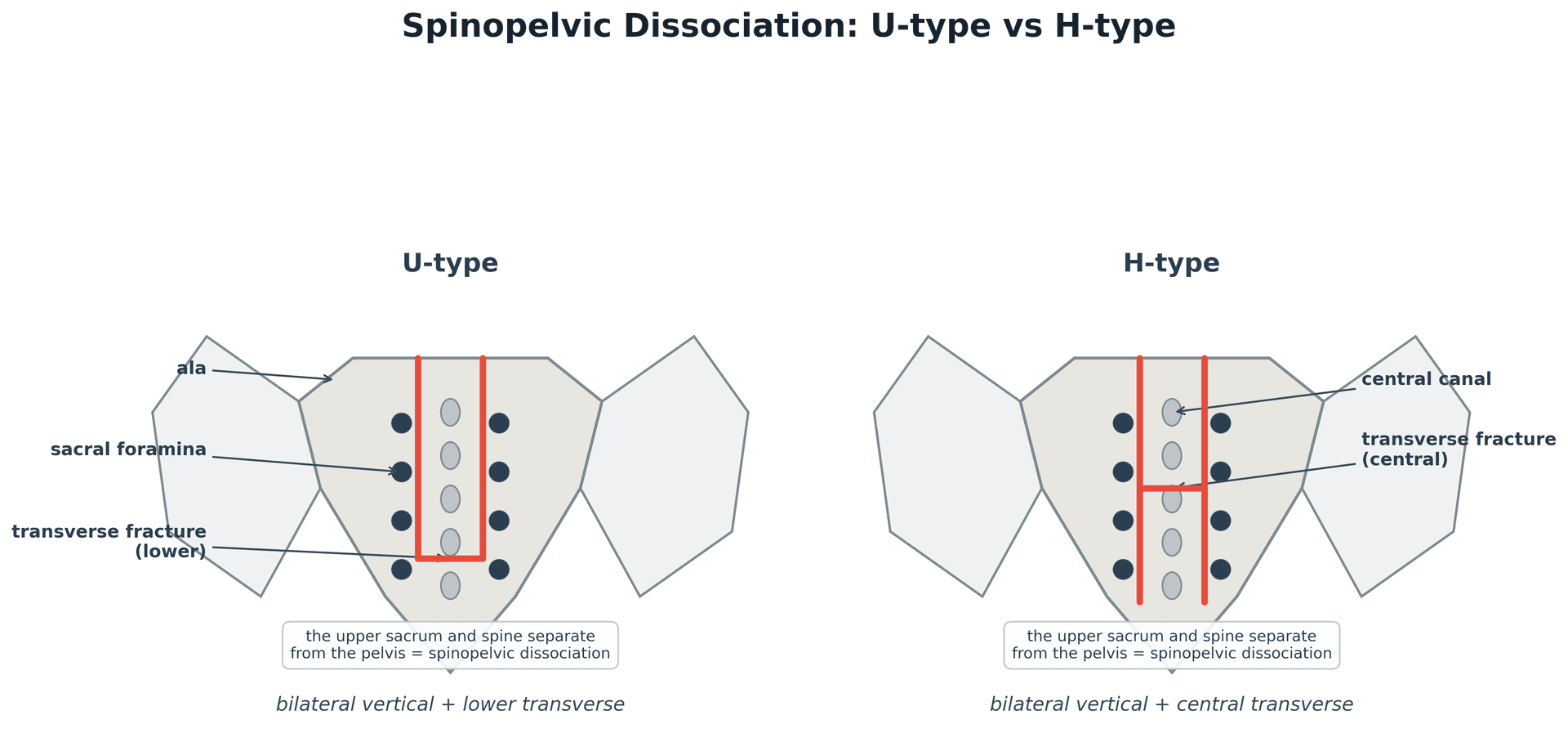
- Bilateral vertical fractures
- Connected by transverse fracture
- H-shaped pattern
- Bilateral vertical fractures through ala
- Connected by transverse fracture through body
- Complete spinopelvic dissociation
- Highest neurological injury rates
- Complete spine-pelvis disconnection
- Requires lumbopelvic fixation
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old motorcyclist is brought in after a high-speed collision. CT shows a Zone II sacral fracture with displacement through the left S1 and S2 foramina. He has 4/5 left ankle plantarflexion and absent left ankle jerk. Describe your assessment and management.”
“Explain the Denis classification for sacral fractures. Why is this classification clinically important?”
“A 75-year-old woman with osteoporosis presents with 6 weeks of low back and buttock pain. X-rays are unremarkable. MRI shows bone marrow edema in the sacrum bilaterally. What is the diagnosis and management?”
MCQ Practice Points
Q: What are the neurological injury rates for each Denis zone? A: Zone I (alar) = 5-10% (L5 nerve), Zone II (transforaminal) = 25-30% (S1-S2 roots), Zone III (central) = up to 60% (cauda equina). Zones move lateral to medial with increasing neurological risk.
Q: What is the miss rate for sacral fractures on plain X-ray? A: 30-50% of sacral fractures are missed on plain radiographs. CT is mandatory for diagnosis and classification. MRI is best for neurological assessment.
Q: What is the safe zone for SI screw placement? A: The S1 body is the target. Use three fluoroscopic views (inlet, outlet, lateral). L5 nerve is at risk anteriorly, sacral canal at risk medially. Watch for dysmorphic sacrum.
Q: What is spinopelvic dissociation and how is it treated? A: Complete disconnection of spine from pelvis seen in U-shaped or H-shaped sacral fractures. Requires lumbopelvic fixation (triangular osteosynthesis) with L4/L5 pedicle screws to bilateral iliac screws.
Q: Why is Zone III a surgical emergency? A: Zone III involves the sacral canal causing cauda equina syndrome with bowel, bladder, and sexual dysfunction (S2-S4). Early decompression (less than 72 hours) improves neurological outcomes.
At a Glance Table
- Zone I
- Lateral to foramina
- Zone II
- Through foramina
- Zone III
- Medial to foramina
- Zone I
- Alar region
- Zone II
- Transforaminal
- Zone III
- Sacral canal
- Zone I
- L5
- Zone II
- S1-S4 roots
- Zone III
- Cauda equina
- Zone I
- 5-10%
- Zone II
- 25-30%
- Zone III
- Up to 60%
- Zone I
- Foot drop
- Zone II
- Weak plantarflexion
- Zone III
- Bowel/bladder/sexual
- Zone I
- Usually stable
- Zone II
- Variable
- Zone III
- Usually unstable
SACRUMSACRUM - Key Sacral Fracture Concepts
Hook:Remember SACRUM for sacral fractures - CT is essential, zones predict neuro injury
Denis Classification
- Zone I = lateral to foramina (alar) = L5 nerve = 5-10%
- Zone II = through foramina = S1-S2 roots = 25-30%
- Zone III = medial/central = cauda equina = up to 60%
- Zones move lateral to medial = increasing neuro risk
Key Imaging
- CT MANDATORY - X-rays miss 30-50%
- Ferguson view = 30 degrees cephalad tilt
- MRI for neurological assessment
- Look for U-type or H-type patterns
Surgical Indications
- Neurological deficit with canal compromise
- Spinopelvic dissociation (U-type/H-type)
- Unstable pelvic ring
- Zone III with cauda equina
SI Screw Technique
- Target S1 body (safe zone)
- Three views: inlet, outlet, lateral
- L5 at risk anteriorly
- Canal at risk medially
Complications
- Chronic SI pain: 30-40%
- Neurological deficit (zone-dependent)
- Bowel/bladder/sexual dysfunction (S2-S4)
- Implant removal: 10-15%
Key Numbers
- 45% of pelvic fractures involve sacrum
- 30-50% missed on plain X-ray
- Greater than 90% union with operative fixation
- 72 hours = optimal decompression window
Evidence and Guidelines
Denis Classification: The Defining Study (236 cases)
- Retrospective analysis of 236 sacral fractures (from 776 pelvic injuries) plus 39 cadavers established the three-zone classification. Neurological deficit was present in roughly 6% of Zone I, 28% of Zone II and 57% of Zone III injuries, with the rate rising as the fracture line moves medially towards the central canal. Routine pelvic radiographs were 'almost useless' for these injuries; CT was crucial.
Transverse Sacral Fractures and Delayed Diagnosis
- Literature review of 90 transverse sacral fractures (29 articles, 1975-2006). Roughly 97% had neurological impairment ranging from radiculopathy to bowel/bladder disturbance. Because of associated polytrauma these fractures are frequently missed in the acute stage; CT is required, and surgically treated patients tended to have better stability and neurological outcomes.
Triangular Osteosynthesis: Biomechanical Rationale
- In 12 cadaveric lumbopelvic specimens cyclically loaded in single-leg stance, triangular osteosynthesis (lumbopelvic fixation plus an iliosacral screw) gave significantly less fracture-site displacement under peak load (mean 0.16 cm versus 0.61 cm) than an isolated iliosacral screw. All triangular constructs survived 10,000 cycles with minimal motion, whereas half of the isolated-screw constructs failed catastrophically.
Spinopelvic Dissociation: Predictors of Outcome
- In 36 H-type spinopelvic-dissociation fractures treated with lumbopelvic fixation and neural decompression (minimum 18-month follow-up), 42% still had a poor clinical outcome. The degree of initial and residual translational displacement and kyphosis of the transverse fracture predicted neurological recovery (Gibbons score) and clinical outcome. Notably, Roy-Camille type, age, ISS, timing of surgery and laminectomy were NOT significantly associated with outcome; accurate reduction was.
Roy-Camille Classification of Transverse Sacral Fractures
- Described transverse fractures of the upper sacrum ('suicidal jumper's fracture') from falls from height. The position of the lumbar spine at impact (kyphosis versus lordosis) determines the morphology: Type 1 (kyphotic angulation, no displacement), Type 2 (kyphosis with posterior displacement) and Type 3 (complete anterior displacement). These injuries are frequently missed because of associated polytrauma.
Cement-Augmented Iliosacral Screws vs Sacroplasty
- For sacral insufficiency fractures in the elderly, navigated cement-augmented iliosacral screw fixation is presented as a more durable alternative to sacroplasty. Finite-element evidence cited suggests sacroplasty alone may not permanently restore the weight-bearing capacity of the sacrum, whereas augmented screws give immediate fixation and rapid pain relief with early mobilisation.