Degenerative Tendinosis | Insertional vs Mid-Portion | Eccentric Loading | FHL Transfer
- Degenerative tendinosis - NOT tendinitis (minimal inflammation)
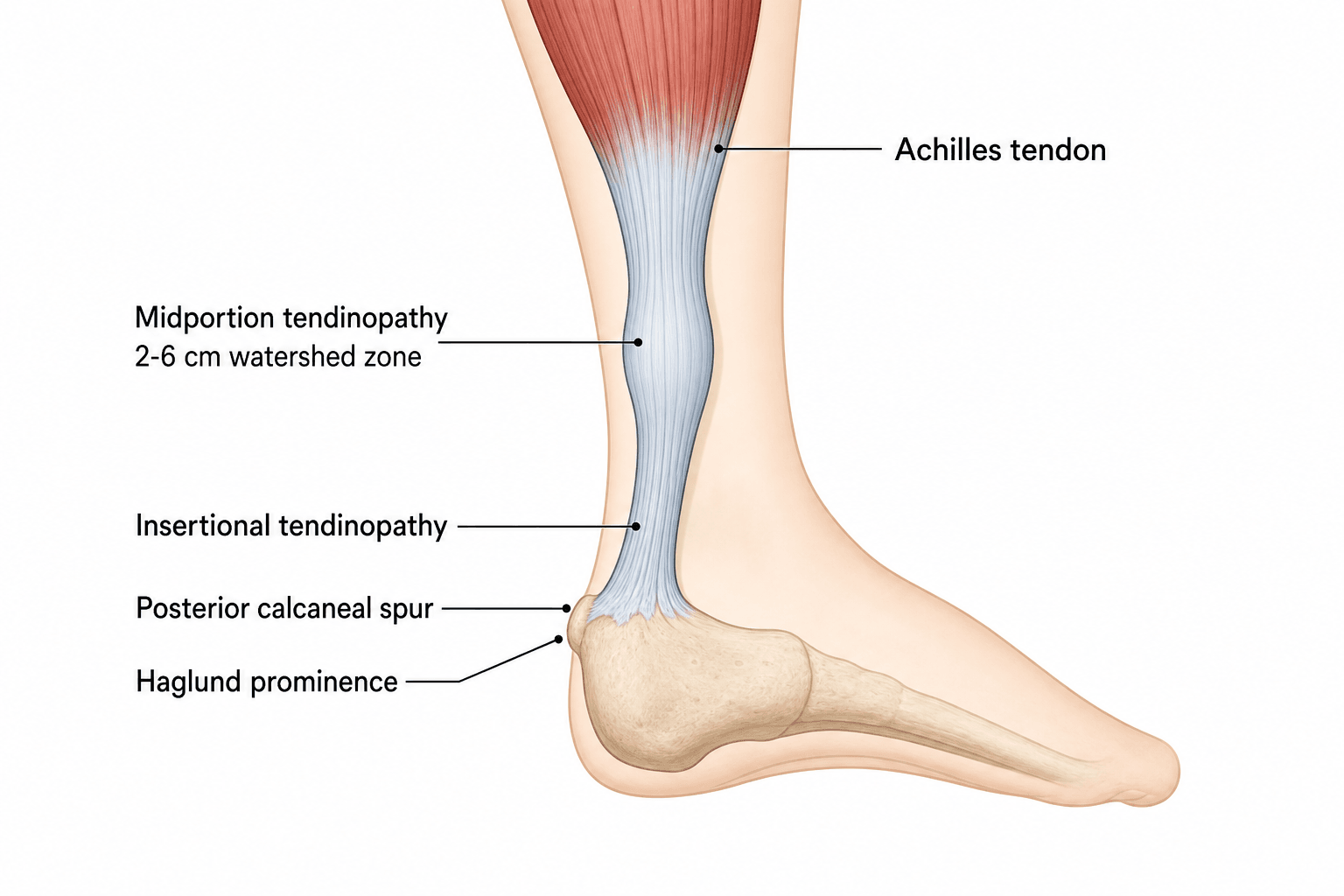
- Watershed zone 2-6cm proximal to insertion has poorest blood supply
- Eccentric exercises are first-line (Alfredson: 3x15 reps, twice daily, 12 weeks)
- Steroids contraindicated - increased rupture risk
- FHL transfer if debriding more than 50% of tendon cross-section
- “Neovascularization with nerve ingrowth causes pain
- “Arc sign: pain moves with ankle dorsiflexion in mid-portion disease
- “Thompson test normal (rules out complete rupture)
- “Insertional disease has worse prognosis than mid-portion
Failed healing response with disordered collagen (Type I replaced by Type III), mucoid degeneration, and neovascularization with nerve ingrowth. Minimal inflammatory cells present. This is why NSAIDs have limited benefit.
Mid-portion (2-6cm): Watershed zone, better prognosis with eccentric exercises. Insertional: Often associated with Haglund deformity and retrocalcaneal bursitis, responds less well to conservative treatment.
Never inject corticosteroids into or around the Achilles tendon. Associated with tendon rupture risk. Peritendinous injections may cause skin atrophy and have limited benefit.
Surgical debridement for refractory cases after 6 months conservative treatment. If more than 50% tendon debridement needed, augment with FHL transfer. Gastrocnemius recession if equinus contracture.
- Mid-Portion (Non-insertional)
- 2-6cm proximal to insertion
- Insertional
- At calcaneal attachment
- Mid-Portion (Non-insertional)
- 55-65% of cases
- Insertional
- 20-25% of cases
- Mid-Portion (Non-insertional)
- Tendinosis in watershed zone
- Insertional
- Enthesopathy, often with Haglund
- Mid-Portion (Non-insertional)
- Positive (pain moves with ankle)
- Insertional
- Negative (pain fixed at insertion)
- Mid-Portion (Non-insertional)
- 70-90%
- Insertional
- 50-60%
- Mid-Portion (Non-insertional)
- Highly effective
- Insertional
- Less effective, may exacerbate
- Mid-Portion (Non-insertional)
- Medial or posterior midline
- Insertional
- Central tendon-splitting
- Mid-Portion (Non-insertional)
- FHL transfer if more than 50% debridement
- Insertional
- Suture anchor repair, FHL rarely needed
ALFREDSONALFREDSON - Eccentric Protocol
Hook:Remember the ALFREDSON protocol creator - 3 sets of 15 reps, twice daily, 12 weeks
5050% Rule for FHL Transfer
Hook:More than 50% tendon debridement = FHL transfer for augmentation
Overview and Epidemiology
Achilles tendinopathy is a degenerative overuse condition affecting the body's largest and strongest tendon. It represents a spectrum of tendon pathology from early reactive change to advanced degenerative disease.
- Running athletes: 6-18% lifetime incidence
- Jumping sports: Basketball, volleyball, tennis at higher risk
- Age distribution: Peak 30-50 years, but can occur at any age
- Bilateral involvement: 30% of cases
- Training errors (rapid increase in intensity/duration)
- Biomechanical factors (hindfoot varus/valgus, equinus contracture)
- Fluoroquinolone antibiotics (Achilles rupture risk roughly 3-4 fold, markedly higher with concomitant corticosteroids)
- Systemic conditions (diabetes, obesity, hypercholesterolemia)
- Footwear changes
- Male gender (for rupture, not tendinopathy)
Use "tendinopathy" as the clinical diagnosis when symptoms and examination suggest tendon pathology. "Tendinosis" refers to the histological finding of degenerative change without inflammation. "Tendinitis" implies inflammation which is rarely the primary process.
Pathophysiology and Mechanisms
The Achilles tendon is formed by the confluence of the gastrocnemius and soleus tendons approximately 15cm proximal to its insertion on the posterior calcaneal tuberosity.
- Length: Approximately 15cm from musculotendinous junction to insertion
- Width: 6-8cm at musculotendinous junction, narrowing to 1.5-2cm at insertion
- Rotation: Fibers rotate 90 degrees along length (lateral gastrocnemius inserts posteromedially)
- Paratenon: Loose connective tissue sheath without synovial lining
- Cross-sectional area: Approximately 60-80 mm²
- Proximal: Muscular branches from gastrocnemius and soleus
- Middle (watershed zone): Peritendinous vessels - relatively hypovascular
- Distal: Calcaneal vessels via osseous insertion
The zone 2-6cm proximal to insertion has the poorest blood supply and is where most mid-portion tendinopathy occurs. This relative hypovascularity contributes to impaired healing and is the target zone for eccentric exercise therapy.
- Forces during running: 6-8x body weight
- Elongation: 6-8% during normal gait
- Storage of elastic energy: 35% of energy during running stored in Achilles
- Gastrocnemius: Primarily ankle plantarflexion, active with knee extended
- Soleus: Plantarflexion active regardless of knee position
- Retrocalcaneal bursa: Between tendon and calcaneus (inflamed in insertional disease)
- Haglund deformity: Posterosuperior calcaneal prominence causing impingement
- Kager's fat pad: Pre-Achilles fat triangle (obliterated in rupture)
- Plantaris tendon: Runs medial to Achilles, may contribute to medial symptoms
TENDONTENDON - Pathophysiology
Hook:TENDON reminds you this is degenerative disease with vascular and nerve changes, not acute inflammation
Classification Systems
Primary Classification (Clinically Most Useful)
- Location
- 2-6cm from insertion
- Key Features
- Watershed zone, fusiform thickening, positive arc sign
- Prognosis
- Better (70-90% non-op success)
- Location
- At calcaneal attachment
- Key Features
- Often with Haglund, may have calcification, fixed tenderness
- Prognosis
- Worse (50-60% non-op success)
- Location
- Paratenon surrounding tendon
- Key Features
- Crepitus, linear thickening on imaging, acute presentation
- Prognosis
- Good with activity modification
Approximately 20-25% of cases have combined insertional and non-insertional disease.
Clinical Assessment
History:
- Location of pain: Mid-portion vs insertional
- Onset: Usually gradual (acute suggests paratendinopathy or rupture)
- Morning stiffness: Characteristic of tendinopathy (improves with activity)
- Activity relationship: Worse with activity, especially running and jumping
- Training history: Recent changes in intensity, duration, or footwear
- Previous treatment: Physiotherapy, injections, medications
- Risk factors: Fluoroquinolones, diabetes, systemic diseases
Examination:
- Technique
- Systematic palpation along tendon
- Positive Finding
- Tenderness, thickening, nodules
- Significance
- Localizes pathology
- Technique
- Palpate tender area while dorsiflexing ankle
- Positive Finding
- Tenderness moves with ankle motion
- Significance
- Mid-portion disease (positive) vs insertional (negative)
- Technique
- Squeeze calf with patient prone, knee flexed
- Positive Finding
- No plantarflexion = positive = rupture
- Significance
- Must be NORMAL in tendinopathy (rules out complete rupture)
- Technique
- Rise onto toes on affected leg
- Positive Finding
- Unable or painful
- Significance
- Functional assessment
- Technique
- Pain on palpation decreases with ankle dorsiflexion
- Positive Finding
- Pain relief with stretch
- Significance
- Suggests mid-portion tendinopathy
Arc sign positive: Tenderness moves with ankle dorsiflexion indicating mid-portion disease. Arc sign negative: Fixed tenderness at insertion regardless of ankle position indicating insertional disease. This distinction guides treatment selection.
Biomechanical assessment:
- Hindfoot alignment (varus/valgus)
- Gastrocnemius tightness (Silfverskiold test)
- Foot posture (pronation/supination)
- Gait analysis
- Footwear assessment
Differential diagnosis:
- Distinguishing features
- Pain/swelling 2-6cm above insertion, positive arc sign
- Key test/investigation
- US/MRI: fusiform thickening, intact tendon
- Distinguishing features
- Fixed tenderness at insertion, posterior bump, worse on stairs
- Key test/investigation
- Lateral radiograph: Haglund, insertional calcification
- Distinguishing features
- Sudden pop, palpable gap, weak push-off
- Key test/investigation
- Positive Thompson (Simmonds) test, US gap
- Distinguishing features
- Acute-on-chronic pain, focal defect
- Key test/investigation
- MRI: high T2 signal with partial-thickness defect
- Distinguishing features
- Tenderness anterior to tendon at insertion
- Key test/investigation
- US/MRI: distended bursa, two-finger squeeze sign
- Distinguishing features
- Crepitus, pain fixed (does not move with ankle)
- Key test/investigation
- US: peritendinous thickening/fluid, tendon may be normal
- Distinguishing features
- Posterior ankle pain on forced plantarflexion (dancers)
- Key test/investigation
- Lateral radiograph in plantarflexion, MRI
- Distinguishing features
- Adolescents, heel pain at apophysis
- Key test/investigation
- Clinical; radiograph excludes other pathology
- Distinguishing features
- Medial mid-portion pain, focal medial tenderness
- Key test/investigation
- US/MRI: plantaris adjacent to medial Achilles
A bilaterally thickened or nodular Achilles - especially in an atypical patient (young, non-athletic, or with poor response to loading) - should trigger a search for a systemic cause, a classic examiner pivot:
- Familial hypercholesterolaemia - Achilles xanthomas: lipid deposits produce firm, often bilateral, nodular thickening of the tendon. They are a recognised clinical sign of FH and a cardiovascular red flag, so bilateral nodular Achilles thickening warrants a fasting lipid profile and cardiovascular risk assessment - the tendon finding can be the presenting clue to a treatable hyperlipidaemia.
- Seronegative spondyloarthropathy - enthesitis: the Achilles enthesis is a hallmark site of enthesitis in ankylosing spondylitis, psoriatic and reactive arthritis. Suspect it with insertional pain plus inflammatory features (other entheses, dactylitis, back stiffness, psoriasis, uveitis, raised CRP, HLA-B27) - this is an inflammatory, not a degenerative, process and is treated medically (NSAIDs/DMARDs/biologics), not with loading or debridement.
- Gout / tophaceous deposition and, rarely, sarcoid can also infiltrate the tendon/insertion.
- Why it matters: these need systemic work-up and disease-specific treatment, not an eccentric-loading programme; and a misplaced peritendinous steroid into a xanthomatous or enthesitic tendon still carries rupture risk.
Exam point: bilateral, nodular or atypical Achilles thickening is xanthoma (check lipids/FH) until proven otherwise; insertional pain with inflammatory features is enthesitis of spondyloarthropathy - both are systemic diagnoses managed medically, not degenerative tendinopathy.
Investigations
First-line imaging modality
- Tendon thickening (greater than 6mm AP diameter abnormal)
- Hypoechoic areas (degenerative regions)
- Loss of normal fibrillar pattern
- Neovascularization on Power Doppler
- Paratenon thickening in paratendinopathy
- Dynamic assessment
- Comparison with contralateral side
- Cost-effective
- Guides injections
- Power Doppler for neovascularization assessment
Ultrasound findings correlate well with symptoms and can guide treatment targeting areas of neovascularization.

Management Algorithm
Eccentric Exercise Protocol (Alfredson)
- 3 sets of 15 repetitions (original Alfredson protocol)
- Twice daily (morning and evening), 7 days per week
- 12 weeks minimum duration
- Straight knee (gastrocnemius) AND bent knee (soleus)
- Progress through moderate discomfort (pain level 4-5/10)
- Add load (backpack/weights) as pain decreases
- GTN patches (nitroglycerin): May improve collagen synthesis
- ESWT: 3 sessions, 2000 impulses per session
- Heel lifts: Reduce strain on tendon
- Activity modification: Reduce provocative activities temporarily
- Biomechanical correction: Orthotics if foot posture abnormal
- Corticosteroid injections (rupture risk)
- Complete rest (deloading harmful)
- Aggressive stretching acutely
Conservative treatment is more effective for mid-portion disease than insertional disease.
Surgical Technique
Approach and Positioning:
- Prone position, tourniquet at thigh
- Medial or posterior midline incision
- Medial approach preferred to protect sural nerve laterally
Steps:
Mid-Portion Debridement Steps
Make 8-10cm longitudinal incision centered on pathological area. Incise paratenon longitudinally. Identify and protect sural nerve if using lateral approach.
Identify degenerative tissue (yellow, soft, mucoid appearance). Excise all abnormal tissue with knife or curette. May need to split tendon longitudinally to access central disease.
Assess remaining tendon cross-section. If more than 50% debrided, plan FHL transfer for augmentation.
Close tendon defect with side-to-side repair if possible. Use non-absorbable suture (2-0 Ethibond or similar).
Close paratenon if possible. Layered skin closure. Apply well-padded splint in slight plantarflexion.
If gastrocnemius recession needed, perform through same or separate incision at musculotendinous junction.
A high-yield, often-missed contributor to medial mid-portion Achilles tendinopathy is the plantaris tendon, and recognising it changes the operation:
- Why it causes pain: the plantaris runs along the medial border of the Achilles. It is a stiffer, less compliant tendon than the Achilles, so during loading it can compress and shear against the medial Achilles, generating a focal medial painful, thickened area - the patient with stubborn medial mid-portion pain that fails standard loading.
- Recognition: tenderness and thickening localised to the medial Achilles (rather than the central/posterior tendon), often with the plantaris seen abutting the medial Achilles on ultrasound/MRI.
- Treatment: when conservative loading fails, excision of the plantaris tendon (often combined with stripping of the ventromedial paratenon and the neovascular/neural ingrowth, e.g. a minimally invasive "scraping"/debridement) targets this pain source and has good results in the medial-pain subgroup - it is a far smaller procedure than formal tendon debridement with FHL transfer.
- The principle: not all "mid-portion tendinopathy" is the same - a discrete medial pain pattern should prompt assessment for plantaris involvement before committing to major debridement.
Exam point: in refractory medial mid-portion Achilles pain, think plantaris involvement - excision of the plantaris (with paratenon/neovascular stripping) is a targeted, lower-morbidity option distinct from extensive Achilles debridement.
DEBRIDEDEBRIDE - Surgical Indications
Hook:DEBRIDE when conservative treatment fails after proper duration
Complications
- Transient increased pain (expected, should continue)
- Calf muscle soreness
- Rare: partial rupture if pre-existing weakening
- 10-30% of mid-portion cases
- 40-50% of insertional cases
- May require eventual surgery
Non-operative complications are generally minor and self-limiting.
Postoperative Care
Simple debridement (less than 50% tendon):
Rehabilitation Phases
Below-knee cast or boot. Non-weight bearing. Elevation and ice.
Weight bearing in boot. Begin gentle ROM exercises out of boot. Physiotherapy for ankle mobility.
Wean from boot. Progressive weight bearing. Begin eccentric exercises at 8 weeks. Stationary cycling.
Sport-specific rehabilitation. Running progression from week 16. Full activity 4-6 months.
Earlier rehabilitation leads to better outcomes than prolonged immobilization.
Outcomes and Prognosis
- Success Rate
- 70-90%
- Return to Sport
- 3-6 months
- Recurrence
- 10-20%
- Success Rate
- 50-60%
- Return to Sport
- 4-8 months
- Recurrence
- 20-30%
- Success Rate
- +10-15%
- Return to Sport
- 3-6 months
- Recurrence
- Similar to eccentric alone
- Success Rate
- 75-85%
- Return to Sport
- 6-9 months
- Recurrence
- 5-10%
- Success Rate
- 80-90%
- Return to Sport
- 9-12 months
- Recurrence
- Less than 5%
Prognostic factors:
- Better Prognosis
- Mid-portion
- Worse Prognosis
- Insertional
- Better Prognosis
- Less than 3 months
- Worse Prognosis
- Greater than 12 months
- Better Prognosis
- Under 40 years
- Worse Prognosis
- Over 50 years
- Better Prognosis
- Recreational athlete
- Worse Prognosis
- Sedentary or elite athlete
- Better Prognosis
- Full eccentric protocol
- Worse Prognosis
- Incomplete exercise program
- Better Prognosis
- Grade I-II
- Worse Prognosis
- Grade III (partial tear)
- Better Prognosis
- First presentation
- Worse Prognosis
- Multiple failed treatments
Long-term outcomes are generally good with appropriate treatment matching. Patient education about the chronic nature and need for sustained rehabilitation is essential.
Guidelines, Registries & Global Practice
Global epidemiology
- Lifetime incidence in runners is estimated at 6-18%, with mid-portion disease accounting for roughly 55-65% and insertional disease 20-25% of presentations.
- Achilles tendinopathy is also common in sedentary middle-aged adults, where metabolic risk factors (obesity, type 2 diabetes, dyslipidaemia) and reduced tendon vascularity predominate over training error.
- Bilateral involvement occurs in up to 30% of cases and should prompt consideration of systemic contributors (inflammatory arthropathy, familial hypercholesterolaemia, fluoroquinolone exposure).
Side-by-side guideline and consensus positions
- Position on first-line care
- Progressive loading (eccentric or heavy slow resistance) first-line
- Notable emphasis
- Strong recommendation against routine PRP and against corticosteroid injection
- Position on first-line care
- Graded loading programme, then ESWT for recalcitrant disease
- Notable emphasis
- Surgery reserved for failure of 6 months structured non-operative care
- Position on first-line care
- Loading programme plus activity modification; ESWT as adjunct
- Notable emphasis
- Caution on injectables; FHL augmentation for extensive degeneration
- Position on first-line care
- Fluoroquinolone class warnings for tendinopathy and rupture
- Notable emphasis
- Avoid fluoroquinolones in tendinopathy where alternatives exist
There is broad international agreement that progressive mechanical loading is first-line, that corticosteroid injection is contraindicated, and that PRP is not supported by high-quality evidence. Differences are largely in the threshold and sequencing of ESWT and the timing of surgery rather than in the fundamental principles.
High- vs limited-resource practice variation
- Well-resourced settings: ready access to ultrasound (including Power Doppler for neovascularisation), MRI for surgical planning, formal physiotherapy-supervised loading, ESWT machines, and foot-and-ankle subspecialty surgery with FHL augmentation.
- Limited-resource settings: diagnosis is clinical; a home-based loading programme (which requires no equipment beyond a step) is the mainstay and is highly cost-effective. Imaging is reserved for diagnostic doubt or pre-operative planning, and ESWT/advanced reconstructive surgery may be unavailable, raising the relative importance of supervised conservative care.
Controversies and Areas of Uncertainty
Several aspects of Achilles tendinopathy management remain debated and are favourite examiner territory because they expose whether a candidate reasons from evidence or from dogma.
The original Alfredson eccentric protocol is historical first-line, but heavy slow resistance (Beyer 2015) gives equivalent outcomes with better compliance. The mechanism of benefit (mechanotransduction and tendon remodelling rather than simply the eccentric phase) means the loading dose matters more than the specific contraction type.
Power Doppler neovascularisation correlates with pain, yet improvement does not require its abolition - some patients improve while vessels persist. Treatments targeting vessels (sclerosis, high-volume injection, surgical stripping) have inconsistent evidence and are not routine.
The highest-quality RCT for PRP (de Vos 2010) is negative. PRP, high-volume image-guided injection and sclerosing agents remain unproven for routine use; corticosteroid is contraindicated. Examiners expect you to NOT default to an injection.
The widely quoted "augment with FHL if more than 50% of the tendon is excised" is a pragmatic intra-operative guide, not a validated threshold. Decision should integrate residual tendon quality, patient demand and age rather than a single percentage.
Most series mandate at least 3-6 months of structured loading before surgery, but the optimal duration and whether minimally invasive/percutaneous techniques match open debridement are unresolved. Many "failures" reflect inadequate or unsupervised loading rather than true conservative failure.
Whether to retain or fully detach-and-reattach the insertion, the value of Haglund resection in isolation, and the place of central tendon-splitting versus medial approaches are all debated. Full-range eccentric loading is best avoided as it aggravates insertional impingement (Wiegerinck 2012).
MCQ Practice Points
Q: What is the location of the watershed zone in the Achilles tendon and why is it clinically significant? A: The watershed zone is located 2-6cm proximal to the insertion. It has the poorest blood supply (peritendinous vessels only) and is where most mid-portion tendinopathy occurs.
Q: A patient has posterior heel pain. Tenderness moves distally when the ankle is dorsiflexed. What does this indicate? A: This is a positive arc sign, indicating mid-portion tendinopathy. A negative arc sign (fixed tenderness) indicates insertional disease.
Q: Describe the Alfredson eccentric exercise protocol for Achilles tendinopathy. A: 3 sets of 15 reps, twice daily, for 12 weeks, performed with both straight knee (gastrocnemius) AND bent knee (soleus). Patients should work through moderate pain (4-5/10).
Q: When is FHL transfer indicated during Achilles debridement surgery? A: When more than 50% of the tendon requires debridement. FHL is in-phase (plantarflexor), has excellent tendon quality, and brings new blood supply.
Q: Why are corticosteroid injections contraindicated in Achilles tendinopathy? A: Corticosteroids increase rupture risk, with highest risk in the first 4 weeks post-injection. They provide no long-term benefit for this degenerative condition.
Exam Cheat Sheet
Key Numbers
- Watershed zone: 2-6cm from insertion
- Eccentric protocol: 3x15 reps, twice daily, 12 weeks
- FHL transfer: If debriding more than 50% tendon
- Non-op success: 70-90% mid-portion, 50-60% insertional
Clinical Pearls
- Tendinosis NOT tendinitis - degenerative, minimal inflammation
- Arc sign positive = mid-portion (moves with dorsiflexion)
- Arc sign negative = insertional (fixed)
- Thompson test must be NORMAL (rules out complete rupture)
Treatment Principles
- Eccentric exercises first-line for mid-portion
- Insertional disease responds poorly to eccentric loading
- NEVER inject corticosteroids - rupture risk
- Surgery after 6 months failed conservative treatment
Surgical Points
- Medial approach protects sural nerve
- FHL transfer for greater than 50% debridement
- FHL in-phase with Achilles (plantarflexor)
- Central tendon-splitting for insertional surgery
Exam Traps
- Steroid injection recommendation
- Not knowing Alfredson protocol details
- Confusing insertional and mid-portion treatment
- Operating too early or too late
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old recreational runner presents with 6 months of posterior heel pain, 4cm above the heel. Pain is worse in the morning and improves with warming up. He has tried rest and NSAIDs without improvement. Examination shows fusiform thickening with tenderness that moves when you dorsiflex the ankle.”
“A 45-year-old woman presents with posterior heel pain at the Achilles insertion. She has a prominent posterior heel bump. Pain is worse with stairs and inclines. Previous physiotherapy with eccentric exercises made her symptoms worse. X-ray shows a Haglund deformity and retrocalcaneal spurring.”
“A 40-year-old athlete presents after 9 months of failed conservative treatment for mid-portion Achilles tendinopathy. MRI shows extensive fusiform thickening with high T2 signal involving approximately 60% of the tendon cross-section. He wants to return to competitive sport.”
Evidence Base
Eccentric Exercise - The Alfredson Protocol (Landmark)
- 15 of 15 returned to pre-injury running at 12 weeks
- Significant reduction in activity-related pain (VAS)
- Injured-side calf strength normalised to the uninjured side
- Defined the 3x15 reps, twice-daily, 12-week eccentric protocol
Eccentric vs Heavy Slow Resistance (RCT)
- 58 patients randomised, intention-to-treat, Level I
- Equivalent VISA-A and pain improvement at 12 and 52 weeks
- Reduced tendon thickness and neovascularisation in both
- HSR superior compliance (92% vs 78%, p less than 0.005)
Eccentric Loading vs Shockwave vs Wait-and-See (RCT)
- 75 patients randomised, Level I
- Eccentric loading 60% vs ESWT 52% vs wait-and-see 24% recovered
- Eccentric and ESWT statistically equivalent
- Wait-and-see ineffective for recalcitrant disease
Platelet-Rich Plasma - No Benefit (RCT)
- 54 patients, double-blind, placebo-controlled, Level I
- VISA-A improved ~21 (PRP) vs ~20 (placebo) points
- No clinically or statistically significant PRP benefit
- High-quality evidence against routine PRP
Topical Glyceryl Trinitrate (RCT)
- 65 patients / 84 tendons, double-blind RCT, Level I
- 78% vs 49% asymptomatic for ADLs at 6 months (p=0.001)
- Reduced activity pain at 12 and 24 weeks
- Headache is the main limiting side effect
Insertional Tendinopathy - Treatment Evidence
- 14 studies, 452 procedures, systematic review
- Mean surgical satisfaction ~89% across techniques
- ESWT superior to eccentric exercise for insertional disease
- Full-range eccentrics poorly tolerated at the insertion
FHL Transfer for Chronic Tendinosis
- 26 patients / 29 tendons, mean 35-month follow-up
- AOFAS improved 41.7 to 90.1
- Good/excellent in 23 of 26 patients
- No significant hallux flexion deficit after transfer
Tendon Pathology Continuum Model
- Three-stage reactive / dysrepair / degenerative continuum
- Early reactive stage is reversible with load modification
- Degenerative regions show cell death and disorganised matrix
- Framework for stage-matched treatment selection
Fluoroquinolone-Associated Tendon Rupture
- Adjusted IRR 3.14 for Achilles rupture with current use
- Risk persists for 60 days after exposure
- Concomitant corticosteroid raises risk ~19-fold
- Greatest absolute risk in patients aged 60 years and over