Bankart | Hill-Sachs | Bone Loss | Bankart vs Latarjet
- Bankart lesion (labral tear) occurs in 90%+ of traumatic anterior dislocations
- Hill-Sachs lesion (humeral head defect) in 65-70% of first dislocations
- Greater than 25% glenoid bone loss = Latarjet or bone graft required
- Engaging Hill-Sachs increases recurrence - Latarjet or remplissage needed
- Age is strongest predictor of recurrence - 67% in under 20 years old
- “ISIS score predicts recurrence - greater than 6 suggests bony procedure
- “On-track vs off-track concept for Hill-Sachs engagement
- “Latarjet provides bone augmentation, sling effect, and capsular repair
- “Arthroscopic Bankart has higher recurrence than open in young athletes
Greater than 25% glenoid bone loss requires bony augmentation (Latarjet or bone graft). Simple Bankart will fail. Measure on CT with 3D reconstruction.
Off-track Hill-Sachs engages the glenoid and causes instability. Requires Latarjet or remplissage. On-track lesions do not engage and can be treated with Bankart.
Under 20 years: 67% recurrence. 20-40 years: 30-40%. Over 40: 10-15%. Young athletes with contact sports have highest recurrence after conservative treatment.
Latarjet provides: 1) Bone augmentation for glenoid, 2) Sling effect of conjoint tendon, 3) Capsulolabral repair. Addresses multiple pathologies.
- Bone Loss
- Minimal
- Recommended Procedure
- Conservative
- Key Consideration
- Rehab, reassess if recurrent
- Bone Loss
- Less than 15%
- Recommended Procedure
- Arthroscopic Bankart
- Key Consideration
- Higher recurrence in contact sports
- Bone Loss
- 15-25%
- Recommended Procedure
- Consider Latarjet
- Key Consideration
- Especially if engaging Hill-Sachs
- Bone Loss
- Greater than 25%
- Recommended Procedure
- Latarjet
- Key Consideration
- Bankart will fail
- Bone Loss
- Any
- Recommended Procedure
- Latarjet or remplissage
- Key Consideration
- Address engaging defect
BONEBankart vs Latarjet Decision
Hook:Check the BONE factors to decide Bankart vs Latarjet!
BSCLatarjet Triple Effect
Hook:BSC - Latarjet gives Bone, Sling, and Capsular repair!
ABCDEFISIS Score Components
Hook:ISIS score greater than 6 = consider Latarjet over arthroscopic Bankart!
Overview and Epidemiology
Under 20 years: 67% recurrence after first dislocation. 20-40 years: 30-40%. Over 40: 10-15% (but higher rotator cuff tear risk). Young age and contact sports indicate early surgical consideration.
- Most common major joint dislocation
- Incidence: 24/100,000/year
- Peak age: 15-25 years (males)
- Anterior = 95%, posterior = 2-4%
- Contact sports overrepresented
- Force to abducted, externally rotated arm
- Direct blow to posterior shoulder
- Fall on outstretched hand
- Sports: tackling, overhead throwing
- May be atraumatic in hyperlaxity
Pathophysiology and Mechanisms
Static Restraints
Primary static stabilizers.
Most important. Anterior band resists anterior translation in abduction/ER.
Variable anatomy. Resists anterior translation mid-range.
Resists inferior translation.
Deepens glenoid by 50%, attachment for ligaments.

Bony Bankart (glenoid fracture with labral avulsion) is associated with higher recurrence after arthroscopic repair than soft tissue Bankart. Consider Latarjet if significant bony fragment or greater than 15% glenoid bone loss.
Classification Systems
Glenoid Bone Loss Measurement

3D CT reconstruction. Fit circle to intact inferior glenoid. Measure deficiency.
- Less than 15%: Arthroscopic Bankart likely sufficient
- 15-25%: Gray zone - consider Latarjet especially with engaging Hill-Sachs
- Greater than 25%: Latarjet or bone graft required
Width and depth. Engaging vs non-engaging.
Clinical Assessment
- Mechanism: ABER position, direct blow
- Reduction: Spontaneous vs required reduction
- Number of dislocations: Recurrence pattern
- Sport level: Contact, overhead, competitive
- Age at first dislocation: Predicts recurrence
- Apprehension test: Positive with ABER
- Relocation test: Relief with posterior force
- Anterior load and shift: Grades translation
- Sulcus sign: Inferior laxity (positive if greater than 2cm)
- Generalized laxity: Beighton score
Apprehension: Patient supine, arm abducted 90°, externally rotate. Positive = apprehension (not just pain). Relocation: Apply posterior force to humeral head. Relief of apprehension = positive. Most specific clinical test for anterior instability.
Key Examination Findings
Arm held in ER and abduction. Loss of deltoid contour. Humeral head palpable anteriorly.
Assess for neurovascular injury (especially axillary nerve), rotator cuff integrity (over 40), and range of motion.
Axillary Nerve Injury
The axillary nerve is the commonest nerve injured in anterior dislocation - it is tethered as it passes around the surgical neck of the humerus and through the quadrilateral space, so it is stretched when the head dislocates anteroinferiorly. Test and document it before and after every reduction: sensation over the "regimental badge" area (lateral/upper deltoid) is the practical screen, since deltoid motor testing is unreliable in an acutely painful shoulder. Most injuries are a neurapraxia with a high rate of spontaneous recovery over weeks to a few months; persistent deficit beyond about 3 months warrants nerve conduction studies/EMG and consideration of exploration. Documenting the pre-reduction status is medicolegally essential - a deficit found only afterwards must not be wrongly attributed to the reduction.
In patients over ~40, a dislocation is more likely to combine dislocation + rotator cuff tear + neurological (axillary/brachial plexus) injury - the so-called "terrible triad" of the shoulder. Persistent weakness after reduction in an older patient should not be assumed to be nerve injury alone: actively exclude a rotator cuff tear (ultrasound/MRI) as well.
Investigations
Standard Views
Glenohumeral alignment.
Glenoid and humeral head relationship. Essential.
Confirms dislocation direction.
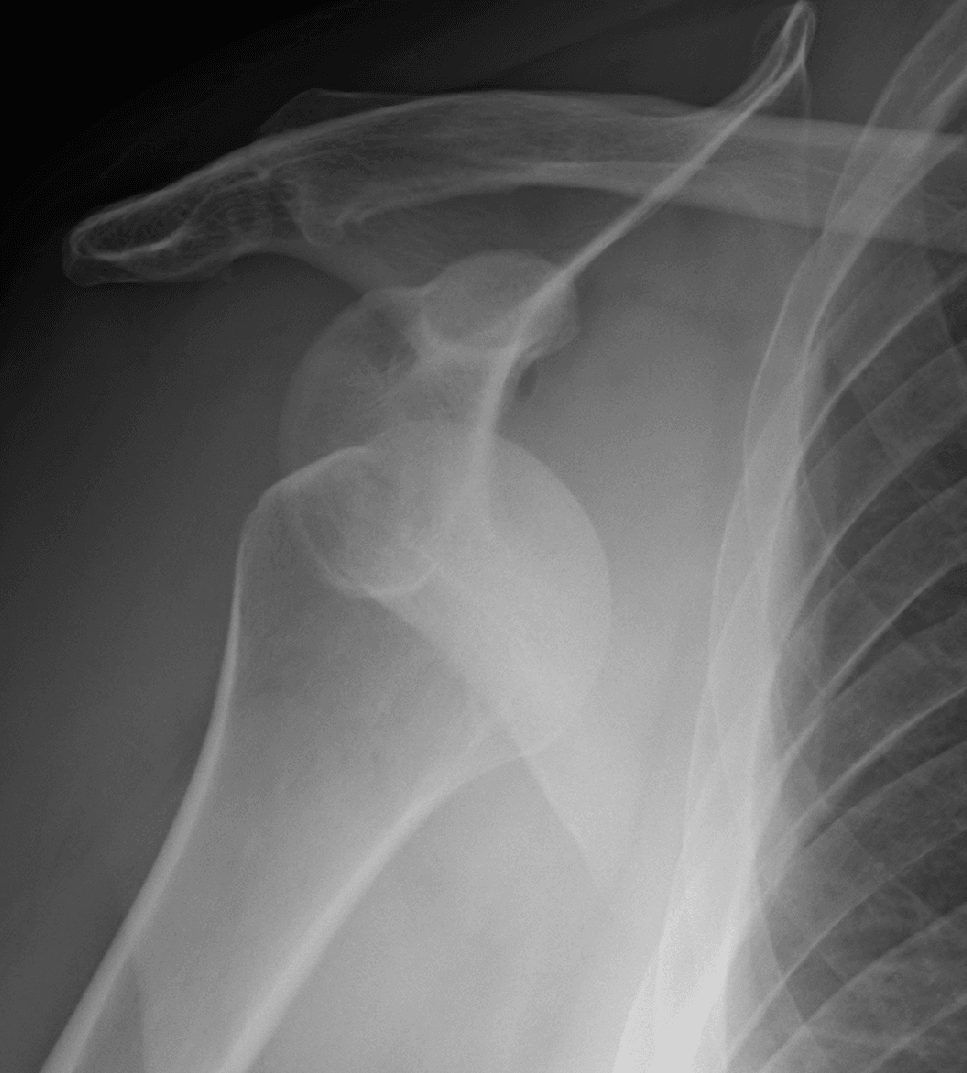
Anteroinferior glenoid (Bankart).
Hill-Sachs lesion visualization.
Hill-Sachs visible on AP: Indicates significant lesion (engaged in ER). Glenoid loss visible on AP: Suggests greater than 20% bone loss. These simple radiograph findings prompt CT quantification.
Acute Reduction Techniques
Before any instability work-up, the acute dislocation must be reduced. A clinical/OSCE favourite is to name and contrast the reduction manoeuvres and the safe principles around them. Provide adequate analgesia first - intravenous sedation/analgesia or intra-articular local anaesthetic (effective, avoids sedation risks) - and document neurovascular status (axillary nerve) before and after, with a post-reduction radiograph to confirm reduction and exclude an iatrogenic fracture.
- Principle
- Longitudinal traction on the arm against countertraction from a sheet around the chest
- Notes
- Effective and widely used; needs an assistant
- Principle
- Patient prone, arm hanging over the edge with a hanging weight; gravity fatigues spasm over 15-20 min
- Notes
- Gentle, minimal force; slow
- Principle
- Rotate the inferior scapular tip medially (often with the patient prone/seated) to reposition the glenoid
- Notes
- High success, low complication; can combine with gentle traction
- Principle
- Seated, arm adducted on the shoulder; analgesic massage of biceps/deltoid/trapezius with scapular positioning - no traction
- Notes
- Best for cooperative, atraumatic/recurrent cases
- Principle
- Abduct and externally rotate the arm overhead, then push the humeral head back with the thumb
- Notes
- Low force, low complication
- Principle
- Longitudinal traction with the arm at the side plus gentle vertical oscillations while abducting and then externally rotating
- Notes
- Single operator, quick, well tolerated
- Principle
- Lever technique: traction, external rotation, adduction, then internal rotation
- Notes
- Historically associated with humeral neck fracture and nerve/vascular injury if forced - use gently or prefer atraumatic methods
Forceful leverage (classically the original Kocher technique) risks iatrogenic proximal humeral fracture, axillary nerve injury and even vascular injury, especially in older osteopenic patients. Prefer low-force traction/scapular/gravity methods, ensure muscle relaxation, and always obtain a post-reduction radiograph (and re-check the axillary nerve) before immobilising.
Differential Diagnosis
The painful or unstable-feeling shoulder in a young patient has several mimics. The exam trap is labelling everything "anterior instability" without distinguishing the direction and the driver (traumatic structural vs atraumatic/volitional).
- Direction / Pattern
- Unidirectional anterior
- Discriminating Features
- Discrete injury in abduction-external rotation, positive apprehension-relocation, Bankart on imaging
- Key Investigation
- MRA plus CT for bone loss
- Direction / Pattern
- Unidirectional posterior
- Discriminating Features
- Seizure, electrocution or posteriorly-directed load; pain on flexion-adduction-IR; jerk test positive
- Key Investigation
- Axillary view, CT/MRI (reverse Bankart)
- Direction / Pattern
- Atraumatic, two or more directions
- Discriminating Features
- Generalised laxity (Beighton), bilateral, positive sulcus sign, no discrete trauma
- Key Investigation
- Clinical; MRI shows capsular redundancy
- Direction / Pattern
- Often muscle-patterning
- Discriminating Features
- Voluntary or positional, abnormal muscle recruitment, psychosocial factors
- Key Investigation
- Dynamic EMG; clinical observation
- Direction / Pattern
- Stable joint
- Discriminating Features
- Deep pain, catching with overhead loading, positive O'Brien/dynamic labral shear, no true apprehension
- Key Investigation
- MRA
- Direction / Pattern
- Stable joint
- Discriminating Features
- Weakness and night pain after dislocation in older patients; pseudo-instability
- Key Investigation
- MRI / ultrasound
The Stanmore (polar-type) triangle frames instability as Type I (traumatic structural), Type II (atraumatic structural) and Type III (muscle-patterning, non-structural). It is high-yield because surgery helps Type I and selected Type II but typically harms Type III - operating on a muscle-patterning shoulder makes it worse.
Management Algorithm

First-Time Anterior Dislocation
Management Pathway
Closed reduction under sedation. Post-reduction radiographs. Assess neurovascular status (axillary nerve). Sling immobilization.
MRI: Assess labrum, rotator cuff. CT with 3D: Quantify bone loss. Essential for surgical planning.
Sling 3-6 weeks. Progressive ROM. Rotator cuff and periscapular strengthening. May be appropriate if: over 40 years old, low demand, no bone loss, non-contact sport.
Consider if: under 20 years old, contact sports, significant bone loss, in-season athlete. Reduces recurrence from 67% to less than 10%.
Surgical Technique
Arthroscopic Bankart Repair
Surgical Steps
Beach chair or lateral decubitus. Standard posterior viewing portal. Anterior portals for anchor placement.
Elevate labrum from glenoid neck. Decorticate glenoid rim to bleeding bone. Ensure adequate mobilization for tension-free repair.
3-4 anchors along anteroinferior glenoid rim (5 to 3 o-clock for right shoulder). Suture anchors or knotless.
Mattress or simple sutures through labrum. Restore labral bumper. Capsular plication if redundant.
Anchors must be placed ON the glenoid rim (not neck) at the articular margin. At least 3 anchors. The 5:30 position (6:30 left shoulder) is critical to address the IGHL attachment. Avoid suprascapular nerve with superior anchors.
Complications
- Procedure
- Bankart
- Incidence
- 10-20%
- Prevention/Management
- Proper patient selection, technique
- Procedure
- Latarjet
- Incidence
- 0-5%
- Prevention/Management
- Rare if technique correct
- Procedure
- Latarjet
- Incidence
- 5-7%
- Prevention/Management
- Proper screw placement, length
- Procedure
- Latarjet
- Incidence
- 5%
- Prevention/Management
- Avoid over-medialization, good contact
- Procedure
- Latarjet
- Incidence
- Variable
- Prevention/Management
- Split (not tenotomy) preferred
- Procedure
- Both
- Incidence
- Variable
- Prevention/Management
- Early ROM, appropriate capsular tension
- Procedure
- Latarjet
- Incidence
- Rare
- Prevention/Management
- Protect musculocutaneous and axillary
Most common causes of Latarjet failure: Graft malposition (too lateral or medial), graft non-union, screw pullout, missed HAGL lesion. Meticulous technique and preoperative planning essential.
Postoperative Care
Rehabilitation Protocol
Sling immobilization. Elbow and hand exercises. Pendulum exercises only. No external rotation past neutral.
Wean sling. Gentle AROM. Limit external rotation (based on surgeon preference). Scapular stabilization exercises.
Full ROM by 12 weeks. Rotator cuff strengthening. Avoid apprehension positions.
Progressive resistance. Sport-specific training started. Avoid contact sports until 6 months (Latarjet may allow earlier).
Bankart: Return to contact sports 6-9 months. Latarjet: Some allow earlier return (4-6 months) due to bony stability. Confirm graft healing on CT before high-risk activities.
Outcomes and Prognosis
Procedure-Specific Outcomes
80-90% success in appropriate patients. Higher recurrence in young contact athletes, bone loss, and engaging Hill-Sachs.
95-98% stability. Low recurrence even in high-risk groups. Some risk of OA long-term.
Prognostic Factors
Older age, non-contact sport, minimal bone loss, first stabilization, compliant rehabilitation.
Age under 20, contact sports, significant bone loss, engaging Hill-Sachs, hyperlaxity, failed previous surgery.
Guidelines, Registries & Global Practice
Global Epidemiology
- Glenohumeral dislocation is the most common large-joint dislocation; population incidence is reported around 23-24 per 100,000 person-years, with anterior dislocations making up roughly 95% of cases.
- Bimodal distribution: a large peak in young males (15-25 years, sport and high-energy trauma) and a smaller peak in older patients (often with concomitant rotator cuff tears or greater tuberosity fractures).
- Recurrence is driven overwhelmingly by age and bone loss, a pattern consistent across cohorts worldwide (Robinson, Edinburgh; Hovelius, Sweden).
Society Guidance Side by Side
- Emphasis
- Evidence appraisal
- Practical Position
- Notes limited high-level evidence; supports surgical stabilisation reducing recurrence in young active patients; individualised first-dislocation decisions
- Emphasis
- Pathway and patient selection
- Practical Position
- Stanmore polar-type framework; reserve surgery for structural (Type I/II) instability; avoid operating on muscle-patterning shoulders
- Emphasis
- Bony injury and fixation
- Practical Position
- Structured assessment and fixation principles for bony Bankart and glenoid reconstruction
- Emphasis
- Bone-loss-driven algorithm
- Practical Position
- Glenoid track and bipolar bone loss central to choosing soft-tissue vs bony procedure
Registry and Outcome Signals
- Large series and registry-type data consistently show Latarjet with lower recurrence than isolated Bankart, balanced against a higher-acuity complication profile (An et al. meta-analysis).
- Revision and complication tracking (e.g. coracoid graft non-union, hardware removal) is increasingly captured in national shoulder-instability and arthroplasty-adjacent datasets to benchmark Latarjet safety.
High- vs Limited-Resource Practice Variation
- Routine 3D CT volumetric bone-loss quantification and MRA
- Access to arthroscopic Bankart, remplissage and arthroscopic or open Latarjet
- Structured return-to-sport testing before clearance
- Greater reliance on plain radiographs (AP in ER, axillary, Stryker/West Point) and clinical assessment
- Open Latarjet/Bristow favoured where arthroscopy or advanced imaging is scarce
- Iliac crest autograft is a low-cost bone-block option without implant dependence
Anterior shoulder instability is a common viva topic across FRCS, FRACS, EBOT, ABOS and DNB/MS. Be prepared to: quantify glenoid and bipolar bone loss, explain on-track vs off-track, articulate the Bankart vs Latarjet decision algorithm, describe both surgical techniques and their complications, and apply the ISIS and Stanmore frameworks.
Controversies and Areas of Uncertainty
No single method is universal. Best-fit circle on 3D CT is most used, but linear, area and surface-based methods give different percentages for the same defect. The "subcritical" zone (around 13.5-20%) increasingly prompts augmentation even below the classic 20-25% threshold.
Whether to stabilise every young first-time dislocator is debated. Robinson and Hovelius data show high but not universal recurrence; shared decision-making weighing sport, age, bone loss and patient preference is favoured over a blanket policy.
Arthroscopic Latarjet offers lower morbidity in expert hands but has a steep learning curve and graft-positioning/hardware concerns. Open Latarjet remains the reference standard; no high-level evidence proves one superior for stability.
Iliac crest autograft and distal tibial allograft (anatomic glenoid reconstruction) avoid the conjoint sling but lose the dynamic effect. Their role versus Latarjet, and bone-block versus screw-versus-suture fixation, is unsettled.
Latarjet lowers recurrence (An et al. meta-analysis) but carries a distinct, sometimes serious complication profile (neurovascular injury, graft non-union/resorption, hardware problems, later arthritis). The honest answer is patient- and pathology-specific selection, not "Latarjet is always better."
MCQ Practice Points
Q: Above what percentage of glenoid bone loss is Latarjet/bony procedure required? A: Greater than 25%. At this level, Bankart repair will fail. 15-25% is the gray zone where engaging Hill-Sachs tips toward Latarjet.
Q: What is the recurrence rate after first dislocation in patients under 20? A: 67%. Young age is the strongest predictor of recurrence. This justifies early surgical consideration in young athletes.
Q: What are the three stabilizing effects of the Latarjet procedure? A: 1) Bone block augmenting glenoid, 2) Sling effect of conjoint tendon, 3) Capsular repair to the bone block.
Q: Which ligament is the primary static restraint to anterior translation? A: Inferior glenohumeral ligament (IGHL) - specifically the anterior band when the arm is abducted and externally rotated.
Q: What percentage of traumatic anterior dislocations have a Bankart lesion? A: Greater than 90%. The anteroinferior labrum avulses with the IGHL attachment in almost all traumatic dislocations.
Q: What does an off-track Hill-Sachs lesion indicate? A: The Hill-Sachs engages the glenoid rim during movement, causing instability. Requires Latarjet or remplissage rather than simple Bankart.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An 18-year-old rugby player presents after his first anterior shoulder dislocation during a tackle. He required reduction in the emergency department. Radiographs show no fracture. How would you manage this?”
“A 24-year-old AFL player has had 5 anterior dislocations over 3 years. CT shows 22% glenoid bone loss and an engaging Hill-Sachs lesion. What would you recommend?”
“A 22-year-old had arthroscopic Bankart repair 2 years ago but has had 3 further dislocations. CT shows the anchors are in place but there is now 18% glenoid bone loss. What is your approach?”
Pathoanatomy
- Bankart lesion in greater than 90% of dislocations
- Hill-Sachs in 65-70% of first dislocations
- IGHL is primary static restraint
- Subscapularis is key dynamic stabilizer
- Bony Bankart reduces glenoid surface area
Bone Loss Thresholds
- Less than 15%: Arthroscopic Bankart likely sufficient
- 15-25%: Gray zone - consider Latarjet if engaging HS
- Greater than 25%: Latarjet or bone graft required
- Off-track HS: Latarjet or remplissage
- Critical bone loss dramatically increases recurrence
Age and Recurrence
- Under 20 years: 67% recurrence
- 20-40 years: 30-40% recurrence
- Over 40 years: 10-15% (but cuff tears)
- Young age = strongest predictor
- Male gender increases risk further
Latarjet Triple Effect (BSC)
- Bone block: Augments glenoid
- Sling effect: Conjoint tendon dynamics
- Capsular repair: Capsule sutured to block
- Benefits: Addresses bone loss and prevents engagement
- Ideal for high-risk contact athletes
ISIS Score greater than 6 = Consider Latarjet
- Age less than 20: 2 points
- Bony lesion on XR: 2 points
- Contact sport: 1-2 points
- Engaging Hill-Sachs: 2 points
- Shoulder hyperlaxity: 1 point
Outcomes
- Bankart: 10-20% recurrence overall
- Latarjet: 0-5% recurrence
- Latarjet superior in high-risk groups
- Both have high patient satisfaction
- Open Latarjet has higher complication rate than Bankart
Evidence Base and Key Studies
Recurrence Risk After Primary Dislocation in the Young
- Prospective cohort of 252 patients aged 15-35 years, nonoperative treatment
- Recurrent instability in 55.7% within 2 years, rising to 66.8% by 5 years
- Younger males at highest risk; females much lower risk
- 86.7% of those who recurred did so within the first 2 years
25-Year Outcome of Nonoperative Treatment
- Prospective multicentre study, 255 patients (257 shoulders), age 12-40, 25-year follow-up
- Roughly half of dislocations in patients aged 12-25 had not recurred or had stabilised over time
- 62 shoulders (27%) ultimately underwent surgical stabilisation
- Immobilisation after primary dislocation did not change the prognosis
Critical Glenoid Bone Loss After Bankart Repair
- Cadaveric study of sequential simulated glenoid defects after Bankart repair
- A defect at least 21% of glenoid LENGTH caused instability and restricted external rotation
- Average loss of 25 degrees external rotation per cm of defect
- Defined the biomechanical basis for bone-loss thresholds
Inverted-Pear Glenoid and Engaging Hill-Sachs
- 194 consecutive arthroscopic Bankart repairs (suture anchor)
- No significant bone defect: 4% recurrence
- Significant bone defect (inverted-pear or engaging Hill-Sachs): 67% recurrence
- Contact athletes with bone defect: 89% recurrence
Glenoid Track Concept
- Nine fresh-frozen cadaveric shoulders, contact mapping in abduction and external rotation
- Defined the glenoid track - the zone of glenoid-humeral contact
- Medial margin of track at 84% (plus or minus 14%) of glenoid width from the cuff footprint
- A Hill-Sachs lesion extending medial to the track risks engagement
On-Track / Off-Track Treatment Paradigm
- Translated engaging/non-engaging into the quantitative on-track/off-track concept
- Integrates bipolar (glenoid plus humeral) bone loss into one framework
- Glenoid track narrows as glenoid bone loss increases, making a fixed Hill-Sachs more likely off-track
- Provides surgical criteria for Bankart, remplissage and bony procedures
Instability Severity Index Score (ISIS)
- Prospective case-control of 131 patients after arthroscopic Bankart, mean 31 months
- 10-point preoperative score (age, sport, hyperlaxity, Hill-Sachs and glenoid contour on AP)
- Score over 6 points: 70% recurrence after arthroscopic Bankart
- Authors suggest a Bristow-Latarjet procedure instead for high scorers
Latarjet vs Bankart - Systematic Review
- Systematic review and meta-analysis, 8 comparative studies, 795 shoulders (Bankart 416, Latarjet 379)
- Latarjet conferred significantly lower risk of recurrence and redislocation
- No significant difference in reoperation rate between procedures
- Higher Rowe scores and less external-rotation loss with Latarjet