Chondral Defects | Size-Based Treatment | Microfracture vs OATS vs ACI
- Articular cartilage has NO blood supply - cannot heal spontaneously
- Treatment algorithm based on DEFECT SIZE and patient factors
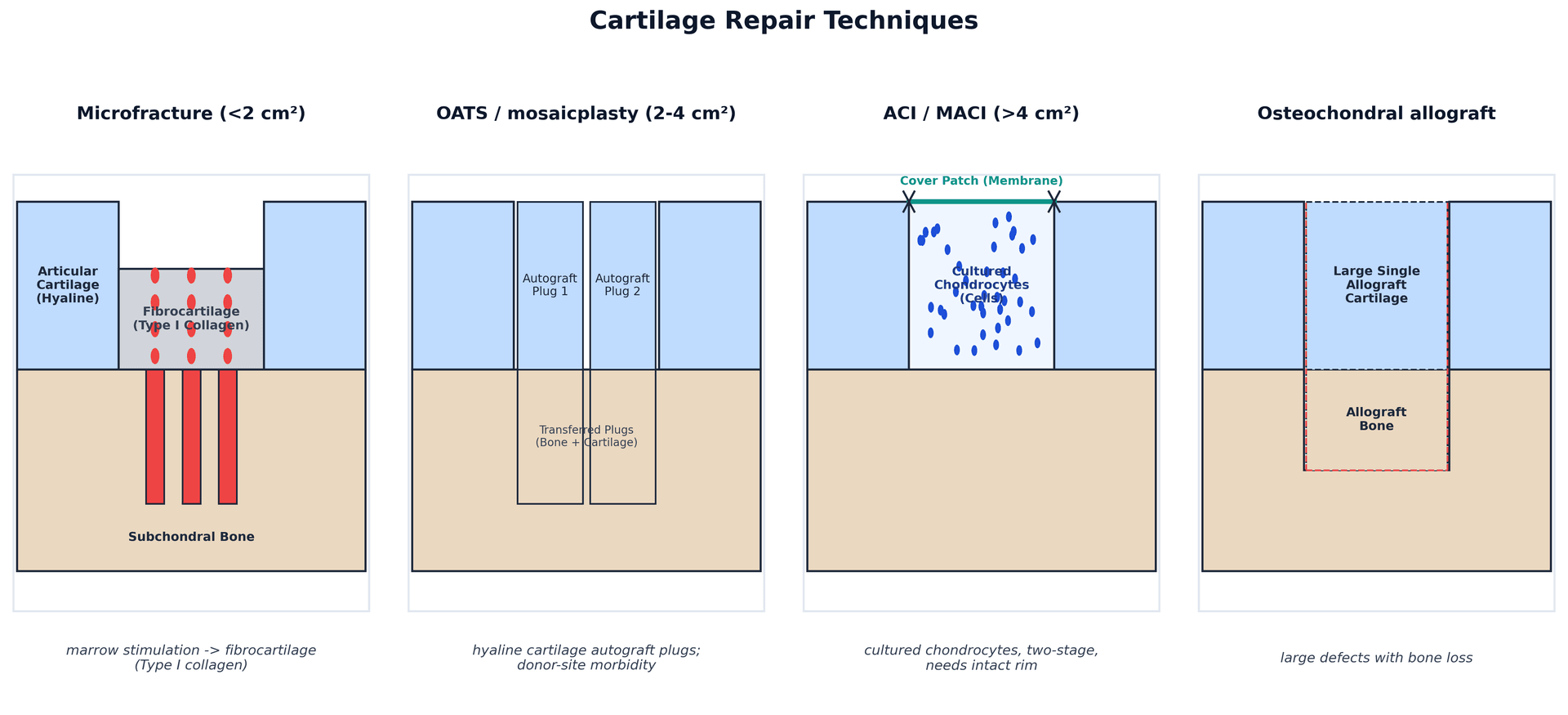
- Microfracture: less than 2cm² - creates fibrocartilage (Type I collagen)
- OATS: 2-4cm² - hyaline cartilage transfer, limited donor site
- ACI/MACI: greater than 4cm² - cultured chondrocytes, expensive, two-stage
- “Fibrocartilage from microfracture is mechanically inferior to hyaline
- “OATS donor site morbidity limits graft size
- “ACI requires intact cartilage rim (shoulders)
- “Osteochondral allograft for large defects with bone loss
Size is the primary determinant. Less than 2cm² = microfracture. 2-4cm² = OATS. Greater than 4cm² = ACI/MACI. Know these thresholds cold.
Microfracture produces fibrocartilage (Type I collagen) which is mechanically inferior to native hyaline cartilage (Type II collagen). This is why larger defects need better options.
Young, active, single contained defect = best candidates. Avoid in malalignment, instability, or meniscal deficiency - must address concomitant pathology.
Kissing lesions (bipolar defects), diffuse OA, inflammatory arthritis, BMI greater than 35, and uncorrected malalignment are relative contraindications. Address alignment first.
- Depth
- Any depth
- First-Line Treatment
- Debridement +/- microfracture
- Key Consideration
- May do well with debridement alone
- Depth
- Full thickness
- First-Line Treatment
- Microfracture
- Key Consideration
- Best for contained lesions
- Depth
- Full thickness
- First-Line Treatment
- OATS (mosaicplasty)
- Key Consideration
- Limited by donor availability
- Depth
- Full thickness
- First-Line Treatment
- ACI/MACI
- Key Consideration
- Two-stage, expensive
- Depth
- Into subchondral
- First-Line Treatment
- Osteochondral allograft
- Key Consideration
- Fresh allograft for viability
SLIMPrerequisites for Cartilage Surgery
Hook:Keep your cartilage patient SLIM (address all these first)!
DONOROATS Considerations
Hook:Get your DONOR site right for successful OATS!
Overview and Epidemiology
Articular cartilage is avascular, aneural, and alymphatic. It relies on diffusion from synovial fluid for nutrition. Without blood supply, there is no inflammatory healing response. This is why we must create a vascular channel (microfracture) or transplant cells (ACI) to achieve repair.
- 60% of knee arthroscopies show cartilage damage
- Peak incidence 10-50 years
- Sports injuries common cause
- Traumatic vs degenerative defects
- Males more commonly affected
- Full thickness defects do NOT heal
- Partial thickness may not progress
- Size correlates with symptoms
- Surrounding cartilage at risk
- Untreated leads to OA
Pathophysiology and Mechanisms
Hyaline Cartilage Zones
Type II collagen parallel to surface. Resists shear.
Oblique collagen. Resists compressive forces.
Perpendicular collagen. Anchors to tidemark.
Above subchondral bone. Tidemark separates from deep zone.
The calcified cartilage layer MUST be removed during microfracture. Leaving it in place prevents integration of repair tissue with subchondral bone and leads to delamination. Curette to bleeding bone, but preserve subchondral plate.
Classification Systems
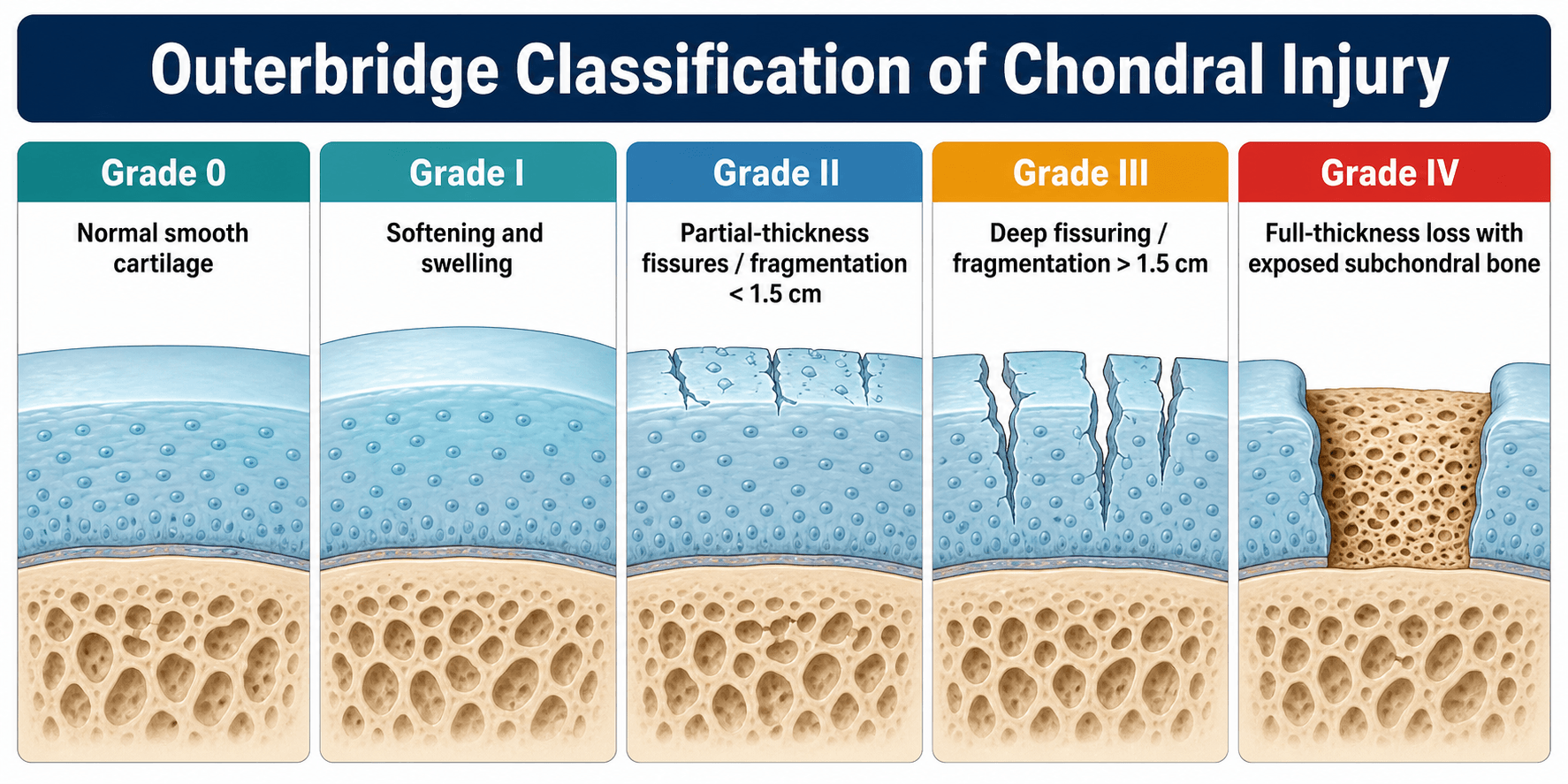
International Cartilage Repair Society
- Description
- Normal
- Depth
- Intact
- Treatment Implication
- No treatment
- Description
- Superficial
- Depth
- Softening/fibrillation
- Treatment Implication
- Conservative
- Description
- Less than 50%
- Depth
- Abnormal
- Treatment Implication
- Debridement/microfracture
- Description
- Greater than 50%
- Depth
- Not to calcified layer
- Treatment Implication
- Microfracture/OATS
- Description
- Greater than 50%
- Depth
- To calcified layer
- Treatment Implication
- Microfracture/OATS
- Description
- Greater than 50%
- Depth
- Through calcified layer
- Treatment Implication
- Restorative procedure
- Description
- Greater than 50%
- Depth
- Blistering
- Treatment Implication
- Restorative procedure
- Description
- Full thickness
- Depth
- To subchondral bone
- Treatment Implication
- Size-based algorithm
Clinical Assessment
- Mechanism: Acute trauma vs insidious
- Pain: Activity-related, mechanical symptoms
- Locking/catching: Loose body?
- Swelling: Effusion pattern
- Previous surgery: Failed treatment?
- Effusion: Common with acute injury
- Tenderness: Focal joint line
- ROM: Usually preserved unless OB/locking
- Alignment: Varus/valgus assessment
- Stability: ACL, meniscal tests
Cartilage procedures in isolation will fail if you do not address ACL insufficiency, meniscal deficiency, or malalignment. A comprehensive assessment is mandatory. Combined procedures (e.g., ACL + microfracture, HTO + cartilage procedure) may be needed.
Key Clinical Distinction
Single, contained, healthy surrounding cartilage. Good candidates for restorative procedures.
Multiple lesions, poor surrounding cartilage, kissing lesions common. Poor candidates for isolated cartilage surgery - consider arthroplasty or osteotomy.
Investigations
MRI Assessment
Gold standard for cartilage evaluation.
Proton density, T2 mapping, dGEMRIC.
Location, size, depth, bone edema.
Bipolar damage - worse prognosis.
Quality affects surgical planning.
Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) evaluates repair tissue quality after cartilage surgery. Assesses: fill, integration, surface, structure, signal intensity, subchondral bone, effusion.

Differential Diagnosis
- Key Distinguishing Feature
- Activity-related pain, mechanical symptoms, well-localized lesion
- Best Investigation
- MRI (T2 map) / arthroscopy
- Why It Matters
- Index diagnosis - size and depth drive treatment
- Key Distinguishing Feature
- Subchondral bone fragment, younger patient, often stable lesion
- Best Investigation
- MRI assesses fragment stability
- Why It Matters
- May be amenable to fixation rather than resurfacing
- Key Distinguishing Feature
- Joint space narrowing, osteophytes, bipolar/diffuse change
- Best Investigation
- Weight-bearing radiographs
- Why It Matters
- Contraindicates isolated cartilage repair
- Key Distinguishing Feature
- Joint-line tenderness, positive McMurray, no full-thickness cartilage loss
- Best Investigation
- MRI
- Why It Matters
- Often coexists - address concurrently
- Key Distinguishing Feature
- Older patient, acute pain, marked bone marrow oedema
- Best Investigation
- MRI
- Why It Matters
- Resurfacing inappropriate; treat the bone
- Key Distinguishing Feature
- Anterior pain, stairs/squatting, often no discrete defect
- Best Investigation
- Clinical + skyline view
- Why It Matters
- Address maltracking before any cartilage surgery
Management Algorithm
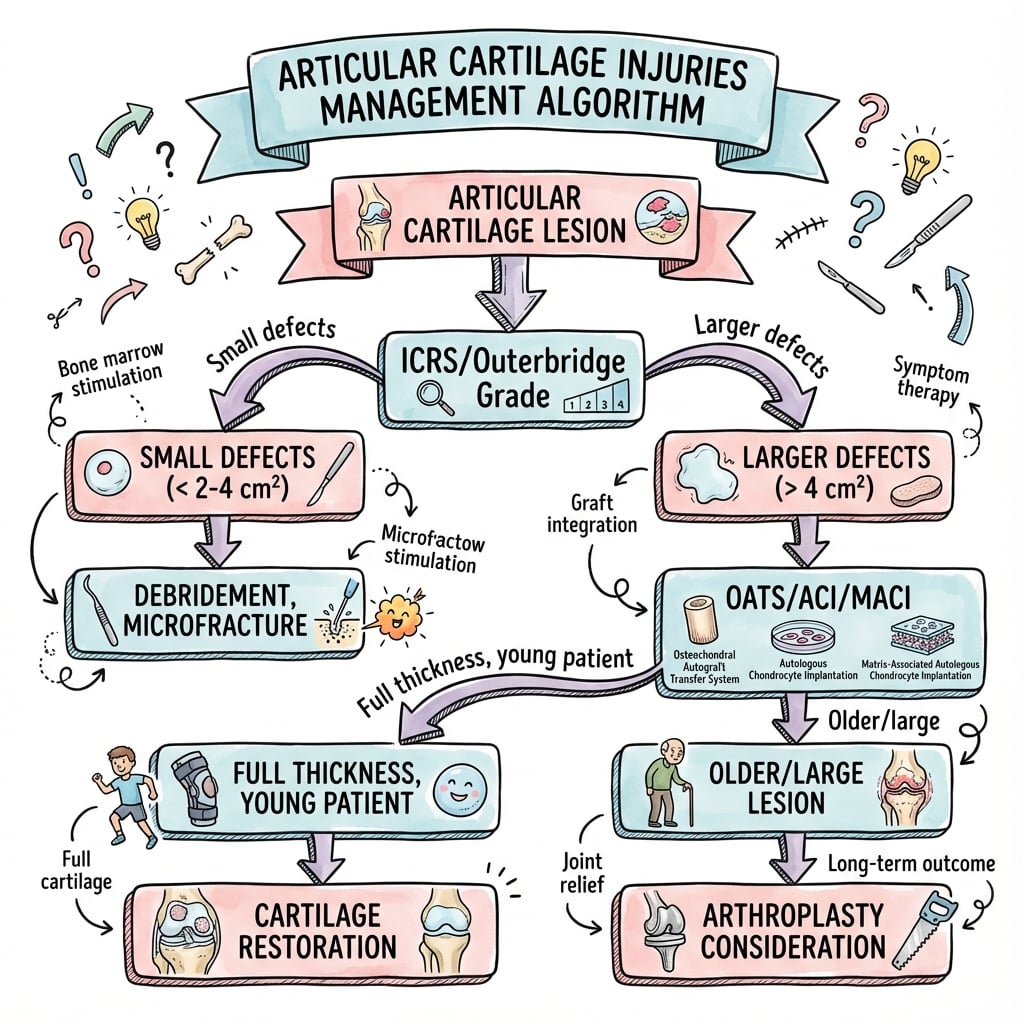
Treatment Selection by Defect Size
Decision Pathway
First-line for small lesions. Creates access to marrow elements. Forms fibrocartilage. Best for contained defects on femoral condyle.
Hyaline cartilage transfer. Autologous osteochondral plugs from non-weight-bearing area. Limited by donor availability and morbidity.
Cultured chondrocytes. Two-stage procedure. Expensive. Requires intact cartilage rim. Best long-term hyaline restoration.
Fresh allograft transfer. For lesions with subchondral bone involvement. Cell viability requires fresh tissue.
When you realign to protect a cartilage repair, the planned correction differs from a standard osteotomy for established OA. For a varus knee with a medial cartilage procedure, aim to bring the mechanical (weight-bearing) axis to neutral or only slightly into the lateral compartment to off-load the medial repair without overloading the healthy lateral side. The classic Fujisawa point (mechanical axis crossing the tibial plateau at roughly 62% of its width from medial, i.e. just lateral to the midline) is the target for osteotomy treating medial OA; for a focal cartilage repair many surgeons deliberately correct less (toward neutral) to avoid transferring load onto the opposite compartment. This is exactly why long-leg alignment films are mandatory before any cartilage surgery.
DMOACCartilage Treatment Ladder
Hook:Doctors Make Orthopaedic Algorithms Clear - size determines step!
Surgical Technique
Microfracture Technique (Steadman)
Surgical Steps
Debride unstable cartilage to stable vertical walls. Curette the calcified cartilage layer. Preserve subchondral plate.
Use curved arthroscopic awl. Create holes 3-4mm deep, 3-4mm apart. Start peripherally, work centrally. 3-4 holes per cm².
Reduce arthroscopic pressure. Observe fat droplets (marrow element) from holes. This is the "super clot" precursor.
CPM 6-8 hours/day for 6 weeks. NWB or TTWB 6-8 weeks. Avoid impact for 4-6 months.
Microfracture produces TYPE I collagen (fibrocartilage) which is mechanically inferior to native TYPE II collagen (hyaline cartilage). Fibrocartilage has only 25% of the stiffness and durability of hyaline. This is why larger defects need better solutions.
PADSMicrofracture Technique
Hook:PADS protect the healing fibrocartilage!
Complications
- Complication
- Intralesional osteophyte
- Incidence
- Common
- Management
- Revision restorative procedure
- Complication
- Fibrocartilage deterioration
- Incidence
- 5+ years
- Management
- Consider second-line procedures
- Complication
- Donor site morbidity
- Incidence
- 5-10%
- Management
- Limit harvest size and number
- Complication
- Plug subsidence
- Incidence
- 5%
- Management
- Proper depth preparation
- Complication
- Hypertrophy
- Incidence
- 15-30%
- Management
- Secondary debridement
- Complication
- Delamination
- Incidence
- 10%
- Management
- Proper rim preparation
- Complication
- Arthrofibrosis
- Incidence
- 5%
- Management
- Appropriate CPM and therapy
- Complication
- Failure
- Incidence
- Variable
- Management
- Address malalignment, revise to higher tier
Graft delamination and hypertrophy are the main ACI-specific complications. Delamination occurs when the calcified layer is not removed or when the surrounding cartilage rim is inadequate. Hypertrophy (overgrowth of repair tissue) may require debridement but is usually a sign of successful healing.
Postoperative Care
Rehabilitation Protocol
CPM 6-8 hours/day. NWB or TTWB with crutches. Avoid shear forces. Focus on ROM and quadriceps activation.
Gradual weight-bearing progression. PWB to FWB by 12 weeks. Pool exercises, stationary bike.
Full weight-bearing. Progressive strengthening. Low-impact activities (swimming, cycling). No impact sports.
Impact activities gradually introduced. Sport-specific training. Full return 9-12 months for high-level athletes.
Premature weight-bearing damages the immature repair tissue and leads to failure. Strict adherence to NWB/TTWB protocol is essential. CPM promotes nutrition diffusion and prevents adhesions.
Outcomes and Prognosis
Procedure-Specific Outcomes
70-80% good/excellent at 5 years. Durability limited - best as bridge procedure. Fibrocartilage degrades over time.
80-90% good outcomes. Limited by plug number. Donor site morbidity in 5-10%.
80-90% satisfaction at 10+ years. Best long-term hyaline restoration. Expensive, two-stage.
75-85% survival at 10 years. Best for large defects with bone loss.
Prognostic Factors
Young age, single defect, femoral condyle location, normal alignment, intact menisci, first-time procedure.
Age greater than 40, bipolar lesions, patellofemoral location, malalignment, revision surgery.
Osteochondral Lesions of the Talus (Site-Specific)
The knee dominates cartilage teaching, but the talar dome is the second most common site and behaves differently enough to be a favourite viva extension. The same biological ladder applies, but the thresholds, morphology and classification are talus-specific.
Posteromedial lesions are the commonest - typically deeper, cup-shaped, and often atraumatic/degenerative. Anterolateral lesions are usually shallower, wafer-shaped, and more clearly traumatic (inversion injury). This shapes both diagnosis and the choice of resurfacing.
MRI assesses cartilage, bone oedema and subchondral cysts; CT best defines bony geometry and cyst size for planning. Posteromedial lesions are hard to reach and may need a medial malleolar osteotomy for open grafting.
- Description
- Small area of subchondral compression (trabecular injury); cartilage intact
- Description
- Partially detached osteochondral fragment
- Description
- Completely detached fragment but undisplaced (remains in the crater)
- Description
- Detached and displaced fragment (loose body)
As at the knee, lesion size and subchondral bone quality decide treatment, but the talar cut-off is smaller. Small lesions (broadly under ~1.5 cm² / 150 mm²) without a large subchondral cyst do well with bone-marrow stimulation (microfracture/drilling). Larger lesions, or those with a significant subchondral cyst or after failed marrow stimulation, are better served by an osteochondral graft - autograft (OAT, e.g. from the knee) or allograft - because marrow stimulation does not reconstruct the bony defect. Symptomatic Berndt-Harty stage III-IV lesions generally need surgery; many stage I-II are trialled non-operatively first.
Guidelines, Registries & Global Practice
- Focal chondral lesions seen in roughly 60% of knee arthroscopies
- Full-thickness (ICRS 3 to 4) defects in around 5 to 11% of arthroscopies
- Peak presentation 30 to 50 years; sports and trauma common in younger patients
- Medial femoral condyle and patella most frequent sites
- Untreated full-thickness defects are a recognized precursor to osteoarthritis
- MACI (matrix-applied ACI) holds FDA approval (US, 2016) and EMA approval for symptomatic femoral condylar defects
- First-generation periosteal ACI largely abandoned for membrane/matrix techniques
- No single dominant cartilage-repair registry; data come mostly from RCTs and institutional series
- Fresh OCA depends on tissue-bank logistics and is concentrated in higher-resource centres
- Cell-therapy products vary widely in regulatory status by region
- Position on Microfracture
- Standard option for small defects
- Position on ACI/MACI
- ACI recommended option for defects over 2cm² with no prior repair and intact rim
- Emphasis
- Defect size and treatment-naive status drive ACI eligibility
- Position on Microfracture
- First-line for small contained lesions
- Position on ACI/MACI
- Preferred for larger lesions; correct alignment/stability first
- Emphasis
- Patient selection and concomitant pathology
- Position on Microfracture
- Acceptable for lesions under 2 to 2.5cm²
- Position on ACI/MACI
- Favoured for larger lesions and active patients
- Emphasis
- Lesion size threshold and activity demand
In high-resource settings the full ladder (microfracture, OATS, ACI/MACI, fresh OCA) is available, often combined with osteotomy or meniscal transplant. In limited-resource settings, debridement and microfracture predominate because they are single-stage, low-cost, and need no cell-culture facility or tissue bank. Cell-based therapy and fresh allograft are restricted by cost, cold-chain logistics, and regulatory approval rather than by clinical indication.
Cartilage surgery is a common viva topic. Know the size-based algorithm cold. Be prepared to discuss why you would choose one procedure over another, address concomitant pathology, and understand the biological differences between repair tissue types. A strong candidate also acknowledges that long-term RCT data (Knutsen) show no clear winner and that no procedure reliably prevents osteoarthritis.
Controversies and Areas of Uncertainty
Subchondral bone overgrowth (intralesional osteophyte) and subchondral cysts after microfracture may compromise later restorative surgery. Some surgeons now prefer marrow stimulation augmented with scaffolds (AMIC) or move straight to cell therapy in larger lesions.
Industry RCTs (SUMMIT, Saris) favour cell therapy for larger lesions, but independent long-term RCTs (Knutsen 5 and 15 year) show no clear advantage over microfracture and no protection against OA. Cost-effectiveness remains debated.
The 2cm² and 4cm² cut-offs are pragmatic teaching figures. Real decisions weigh location, depth, bone involvement, patient age, activity, and prior surgery - not size alone.
Minced/particulated cartilage, scaffold-based one-step techniques, BMAC and PRP augmentation, and allogeneic cell products are under active study but lack long-term high-level evidence.
MCQ Practice Points
Q: What is the upper size limit for microfracture? A: Less than 2cm². Beyond this, consider OATS (2-4cm²) or ACI/MACI (greater than 4cm²).
Q: What type of cartilage does microfracture produce? A: Fibrocartilage (Type I collagen). Native articular cartilage is hyaline (Type II collagen). Fibrocartilage is mechanically inferior.
Q: What is required for successful ACI? A: Intact surrounding cartilage rim (shoulders). This is needed to contain the implanted chondrocytes and prevent leakage.
Q: What limits the size of defects treatable with OATS? A: Donor site availability. Harvesting too many plugs causes donor site morbidity. Typically limited to 2-4cm² defects.
Q: Why must the calcified cartilage layer be removed in microfracture? A: Prevents integration of repair tissue with subchondral bone. Leaving it causes delamination of the fibrocartilage layer.
Q: Why must osteochondral allografts be fresh? A: Chondrocyte viability. Cells die with freezing - must implant within 28 days of harvest for living cartilage.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old soccer player presents with knee pain after a twisting injury. MRI shows a 1.5cm² ICRS Grade 4 chondral defect on the medial femoral condyle. The knee is otherwise normal. How would you manage this?”
“A 32-year-old woman has persistent medial knee pain. MRI shows a 4.5cm² full-thickness defect on the medial femoral condyle. Long leg films show 5° of varus. She has failed 6 months of conservative treatment. How would you proceed?”
“A 28-year-old returns 3 years after microfracture for a 2cm² medial femoral condyle defect. He has recurrent symptoms. MRI shows poor fill and subchondral cysts. Alignment is normal. What are your options?”
Size-Based Algorithm
- Less than 2cm² = Microfracture
- 2-4cm² = OATS/Mosaicplasty
- Greater than 4cm² = ACI/MACI
- Large + bone loss = OCA
Tissue Produced
- Microfracture = Fibrocartilage (Type I)
- OATS = Hyaline (transplanted)
- ACI = Hyaline-like (Type II)
- OCA = Hyaline (transplanted)
Prerequisites (SLIM)
- Stability (ligaments intact)
- Limb alignment (correct malalignment)
- Intact menisci
- Motivation for rehab
Microfracture Technique
- Debride to stable vertical walls
- Remove calcified cartilage layer
- Awl holes 3-4mm deep, 3-4mm apart
- Confirm fat droplets (marrow access)
Postoperative Protocol
- CPM 6-8 hours/day for 6 weeks
- NWB or TTWB 6-8 weeks
- No impact for 4-6 months
- Full return 9-12 months
Key Studies
- SUMMIT trial: MACI superior to microfracture
- Steadman: Microfracture 75% good at 11 years
- Hangody: OATS 92% good at 10 years
- Size matters for treatment selection
Evidence Base and Key Studies
Brittberg - First-in-Human Autologous Chondrocyte Implantation
- Landmark first clinical series of ACI in 23 patients (defects 1.6 to 6.5 cm²)
- Cultured autologous chondrocytes injected under a sutured periosteal flap
- 14 of 16 femoral condylar transplants good to excellent at 2 years
- Patellar lesions did markedly worse than femoral condylar lesions
- Biopsy showed hyaline-like cartilage in 11 of 15 femoral grafts
Steadman - Microfracture for Traumatic Chondral Defects (11-Year)
- 72 patients (75 knees), age 45 years and younger, isolated traumatic full-thickness defects
- Average 11.3-year follow-up (range 7 to 17 years), 95% retention
- Lysholm improved from 59 to 89, Tegner from 3 to 6
- 80% of patients rated themselves improved at 7 years
- Younger age predicted greater functional improvement
Knutsen - ACI vs Microfracture RCT (5-Year)
- 80 patients randomized to first-generation ACI (n=40) vs microfracture (n=40)
- Both groups improved significantly at 2 and 5 years
- No significant clinical or radiographic difference between groups at 5 years
- 9 failures (23%) in EACH group by 5 years
- No correlation between histological repair quality and clinical outcome
Knutsen - ACI vs Microfracture, 14 to 15-Year Follow-up
- Long-term follow-up of the original 80-patient RCT
- No significant difference between ACI and microfracture at 14 to 15 years
- 17 failures (ACI) vs 13 (microfracture); more TKAs in ACI group (6 vs 3)
- Around half of all patients had radiographic OA (Kellgren-Lawrence 2 or higher)
- Authors raise concern that neither procedure reliably prevents OA
Saris - Characterized Chondrocyte Implantation vs Microfracture (36-Month Clinical)
- 118 patients randomized to characterized chondrocyte implantation (n=57) vs microfracture (n=61)
- Significantly greater overall KOOS improvement with CCI at 36 months (P=0.048)
- More treatment responders with CCI (83% vs 62%)
- Benefit greatest when symptom onset was under 3 years
- Companion 2008 paper (PMID 18202295) showed superior structural/histological repair at 1 year
SUMMIT Trial - MACI vs Microfracture (2-Year RCT)
- 144 patients with symptomatic defects 3 cm² or larger (mean lesion 4.8 cm²)
- MACI significantly better than microfracture for co-primary KOOS pain and function at 2 years (P=0.001)
- Fewer treatment failures with MACI (12.5% vs 31.9%)
- Histology and MRI repair-tissue quality similar between groups
- No unexpected safety signals
Hangody - Autologous Osteochondral Mosaicplasty (10-Year Experience)
- 831 patients undergoing mosaicplasty over 10 years
- Good to excellent results in 92% of femoral condylar implantations
- Lower success at the patella/trochlea (79%) than femoral condyle
- Long-term donor-site morbidity only 3% (Bandi score)
- Arthroscopic biopsies confirmed survival of transplanted hyaline cartilage
Levy/Bugbee - Fresh Osteochondral Allograft of the Femoral Condyle
- 122 patients (129 knees), median 13.5-year follow-up
- Graft survivorship 82% at 10 years, 74% at 15 years, 66% at 20 years
- Durable improvement in pain and function scores
- Age over 30 years and 2 or more prior knee surgeries predicted failure
- 47% underwent a reoperation but most retained the graft
Mithoefer - Microfracture Evidence-Based Systematic Review
- Systematic review of 28 studies, 3122 patients
- Consistent functional improvement in the first 24 months
- Conflicting evidence on durability beyond 2 years
- Variable defect fill on MRI correlated with functional outcome
- Limited hyaline repair tissue and possible functional deterioration over time
ICRS Cartilage Injury Classification (Reference Standard)
- Standardized arthroscopic grading (0 to 4) of chondral lesions
- Grade-3 subdivided (3A to 3D) by depth into the calcified layer
- Includes ICRS Cartilage Repair Assessment (CRA) for repair tissue
- Globally adopted reporting standard for cartilage studies