Return-to-Play Timing | Type III Controversy | Surgical Decision-Making in the Athlete
- Default to conservative even in elite athletes - the COTS RCT shows no clinical advantage to surgery at 2 years for high-grade injury
- Return-to-play differs sharply by treatment: 6-12 weeks conservative vs 6-9 months after surgery - decisive when counselling mid-season
- Type III is controversial - reserve surgery for failed conservative trial, throwing athletes, and high-demand cosmesis concerns
- Absolute surgical indications remain Type IV-VI (posterior, severe superior, inferior displacement)
- Hook plate requires removal at 3-4 months - a mandatory second surgery to factor into the athlete's season
- “COTS RCT: no clinical advantage to surgery at 2 years for high-grade (III-V) AC injury
- “15-20% re-injury rate in contact sport after conservative treatment; padding reduces but does not eliminate risk
- “Type IV posterior displacement may mimic Type III on AP - axillary view mandatory
- “Throwing mechanics load the AC joint in late cocking - overhead athletes may have persistent horizontal-adduction pain
Default to conservative even in athletes. Surgery offers NO clinical advantage at 2 years (COTS RCT). Consider surgery ONLY in: throwing athletes, failed conservative 3-6 months, cosmesis concerns in elite athletes.
Conservative: 6-12 weeks to contact sport. Surgical: 6-9 months minimum. This timeline difference is CRITICAL when counseling athletes mid-season.
Throwing mechanics affected by AC instability - late cocking phase stress on AC joint. Overhead athletes may have persistent pain with horizontal adduction. Consider sport demands when deciding treatment.
15-20% re-injury rate in contact sports after conservative treatment. Protective shoulder padding reduces risk. Surgical fixation does NOT eliminate re-injury risk (can fail).
ATHLETEATHLETE - RTP Decision Factors
Hook:ATHLETE framework guides sport-specific RTP decision-making
SPORTSPORT - Activity-Specific Concerns
Hook:SPORT-specific factors influence conservative vs surgical decision
Overview and Sports Epidemiology
AC joint injuries in athletes are among the most common shoulder injuries in contact and collision sports. The injury pattern, treatment considerations, and return to sport timeline differ significantly from non-athletic populations.
Sport-specific epidemiology:
- Injury Rate
- 8-12 per 1000 athlete-exposures
- Common Mechanism
- Direct tackle to shoulder
- Type Distribution
- Type II-III most common
- Injury Rate
- 6-10 per 1000 exposures
- Common Mechanism
- Board collision
- Type Distribution
- Type III-V higher rate
- Injury Rate
- 3-5 per 1000 exposures
- Common Mechanism
- Tackling, blocking
- Type Distribution
- Type II-III predominant
- Injury Rate
- 2-4 per 1000 exposures
- Common Mechanism
- Fall onto shoulder
- Type Distribution
- Type III-IV patterns
- Injury Rate
- 2-3 per 1000 exposures
- Common Mechanism
- Direct pressure
- Type Distribution
- Type II-III typical
Mechanism in athletes:
- Direct blow - fall onto point of shoulder with arm adducted (85% of cases)
- Axial loading - tackling with shoulder leading
- Indirect trauma - fall onto outstretched hand (rare, 15%)
- Chronic repetitive stress - throwing athletes (Type I-II sprains)
Athletes have higher rates of Type III-V injuries compared to general population (60% vs 40%) due to high-energy mechanisms. Re-injury rate is also higher in athletes returning to contact sports (15-20% vs under 10% general population).
Career impact considerations:
- Professional athletes: career implications, insurance, contract status
- College athletes: scholarship considerations, draft prospects
- Recreational athletes: quality of life, activity modification tolerance
- Timing: mid-season vs off-season affects surgical timing
Pathophysiology and Mechanisms
Functional anatomy in athletes:
The AC joint serves as the critical link between the axial skeleton (clavicle) and the appendicular skeleton (scapula). In athletes, this articulation is subjected to repetitive and high-magnitude forces.
AC Ligament Complex (horizontal stability):
- Function in Athletes
- 56% AP stability
- Sport-Specific Role
- Resists tackle/collision forces
- Function in Athletes
- 25% AP stability
- Sport-Specific Role
- Throwing follow-through stability
- Function in Athletes
- Proprioception
- Sport-Specific Role
- Neuromuscular control
- Function in Athletes
- Load sharing
- Sport-Specific Role
- Critical for overhead athletes
CC Ligament Complex (vertical stability):
The two coracoclavicular ligaments provide the vertical stability that fails in high-grade injury — the Conoid medially and the Trapezoid laterally.
- Position
- Medial (45mm from AC)
- Strength
- Stronger
- Athletic Function
- Primary vertical restraint
- Position
- Lateral (20mm from AC)
- Strength
- Secondary
- Athletic Function
- Rotational control
Throwing Athletes (Cricket, Baseball, Javelin):
Phase-specific AC joint stress:
- Wind-up: Minimal AC stress
- Early cocking: Scapular positioning, moderate AC load
- Late cocking: PEAK AC STRESS - horizontal abduction stretches posterior AC ligament
- Acceleration: Rapid scapular protraction, AC shear forces
- Deceleration: High eccentric load on deltotrapezial complex
- Follow-through: Horizontal adduction compresses AC joint
Key point: Late cocking and deceleration place maximum stress on AC joint. Instability affects throwing mechanics and velocity.
In throwing athletes, AC instability causes scapular dyskinesis leading to altered glenohumeral mechanics. This can reduce throwing velocity by 10-15% and increase risk of secondary rotator cuff or labral pathology.
Classification Systems
Rockwood classification — the one ladder. Grade is set by which ligaments fail and how far the clavicle displaces, and it drives the entire management decision. It is presented once, in full, here; later sections refer to a grade by name rather than re-listing the ladder.
The Type III controversy — the decision that matters


Historically (pre-2010) many throwing and contact athletes underwent surgery, on the belief that anatomic reduction improved outcomes and out of concern for cosmetic deformity in elite athletes. Current evidence (post-COTS RCT, 2015) overturned that default: there is no clinical difference in outcomes between operative (hook plate) and non-operative treatment at 2 years, 80–90%RTP of athletes succeed conservatively, cosmetic deformity does not correlate with performance, and surgery carries its own complications (infection, hardware problems, recurrence).
- 1Trial conservativeSling, analgesia, early ROM for 3–6 weeks — the default even in elite athletes.
- 2ReassessPain, strength and sport-specific testing; most athletes are progressing by now.
- 3Escalate selectivelyPersistent symptoms at 3–6 months, or a throwing athlete / off-season timing → reconsider surgery.
Type IV–VI are not part of the controversy — they are surgical. Type IV is buttonholed posteriorly and irreducible closed; Type V has the deltotrapezial fascia detached from a high-energy mechanism and mandates a robust deltotrapezial repair; Type VI is an inferior displacement from severe trauma and a surgical emergency in which multi-trauma (pneumothorax, rib fractures) must be excluded. None has any role for conservative management, and a high-grade injury can be career-threatening.
Clinical Assessment in Athletes
Sport-specific history:
Key questions:
- Sport and position played
- Level (professional, college, recreational)
- Hand dominance (critical in throwing sports)
- Time in season (pre-season, mid-season, playoffs, off-season)
- Mechanism (direct blow, fall, repetitive)
- Previous AC joint injuries (increased re-injury risk)
- Performance impact (pain with specific movements)
- Career implications (contract year, scholarship, draft)
Physical examination - Athlete-focused:
- Technique
- Arm across body to opposite shoulder
- Positive Finding
- AC joint pain
- Athletic Significance
- Predicts pain with tackling, blocking
- Technique
- 90° flexion, 10° adduction, IR, resist downward
- Positive Finding
- AC pain relieved with supination
- Athletic Significance
- Overhead/throwing mechanics affected
- Technique
- Depress lateral clavicle, observe recoil
- Positive Finding
- Clavicle depresses and springs back
- Athletic Significance
- CC ligament integrity - Type III+
- Technique
- Translate clavicle AP with acromion fixed
- Positive Finding
- Increased translation vs contralateral
- Athletic Significance
- AC ligament compromise - instability
- Technique
- Simulated throwing motion (late cocking)
- Positive Finding
- AC pain during late cocking phase
- Athletic Significance
- Throwing athletes - biomechanics affected
- Technique
- Full push-up position with scapular protraction
- Positive Finding
- AC pain or weakness
- Athletic Significance
- Contact athletes - blocking/tackling
Throwing athletes: Simulate late cocking position (horizontal abduction, external rotation) - reproduces AC stress. Contact athletes: Push-up test assesses scapular stability and deltotrapezial function. Overhead athletes: Cross-body adduction with resistance predicts pain during sport activities.
Functional assessment:
- Active ROM vs contralateral
- Strength testing (all shoulder movements)
- Scapular dyskinesis evaluation
- Sport-specific movement patterns
- Pain during athletic simulation
Differential diagnosis
The athlete who has fallen onto the point of the shoulder can have several injuries that mimic or coexist with AC separation. The cross-body adduction view, axillary view and focused examination distinguish them.
- Key distinguishing feature
- Bony tenderness, crepitus; deformity is fracture not joint
- Best test / imaging
- AP/Zanca radiograph shows fracture line, not joint widening
- Why it matters
- Neer IIB pattern is unstable and often needs fixation
- Key distinguishing feature
- Chronic, atraumatic or repetitive load; no acute displacement
- Best test / imaging
- MRI: distal clavicle bone marrow oedema and resorption
- Why it matters
- Managed with load modification, not acute injury pathway
- Key distinguishing feature
- Apprehension, deep joint pain, arm held in fixed position
- Best test / imaging
- Apprehension/relocation test; AP + axillary radiograph
- Why it matters
- Different reduction and rehabilitation pathway
- Key distinguishing feature
- Painful arc, weakness in abduction/ER, night pain
- Best test / imaging
- Jobe/Hawkins tests; ultrasound or MRI
- Why it matters
- Common coexisting pathology in overhead athletes
- Key distinguishing feature
- Pain with O'Brien deep in joint (not localised to AC)
- Best test / imaging
- O'Brien test, MR arthrography
- Why it matters
- O'Brien is positive in both AC and SLAP — localise the pain
- Key distinguishing feature
- Medial-end pain, possible dysphagia/venous congestion
- Best test / imaging
- Serendipity view, CT of SC joint
- Why it matters
- Posterior SC dislocation is a surgical emergency
Investigations in Athletes
- Zanca: 10-15° cephalic tilt
- Bilateral comparison (CC distance)
- Measure AC joint width
- Calculate displacement percentage
- ONLY view to diagnose Type IV posterior displacement
- Type IV looks identical to Type III on AP view
- Must obtain in all AC joint injuries
- Weighted views with 5-10kg weights
- May help differentiate Type II from III
- Most centers no longer use routinely
- Pain limits utility in acute setting
- Decision rarely changed by stress views
- Chronic AC joint pain (distal clavicle osteolysis)
- Suspected rotator cuff or labral pathology
- Pre-operative planning for chronic reconstruction
- Failed conservative treatment (assess for occult pathology)
Weightlifter's shoulder - chronic repetitive stress causes distal clavicle osteolysis. Seen on MRI as bone marrow edema and clavicle resorption. Different from acute AC separation. Treatment: activity modification, NSAIDs, consider distal clavicle excision if persistent.
- Suspected fracture (clavicle, acromion, coracoid)
- Pre-operative planning for complex reconstruction
- Failed surgery (assess hardware, bone quality)
- Dynamic assessment of AC stability
- CC distance measurement
- Operator-dependent
- Not standard of care currently
The Cross-Body Adduction View and Dynamic Horizontal-Instability Assessment (IIIA vs IIIB)
The single most useful refinement in the grade III controversy is to ask whether the joint is horizontally stable. The standard AP and Zanca films show vertical (superior) displacement, but they say nothing about horizontal (antero-posterior) stability — and it is horizontal instability, together with scapular dysfunction, that separates the athlete who may benefit from surgery from the one who will not. Horizontal stability is assessed dynamically, with the cross-body (modified Basamania) adduction view and a focused scapular examination, rather than from the static AP film.
Performing the cross-body adduction view
- The patient forward-flexes the arm to roughly 90 degrees and adducts it across the body toward the opposite shoulder (a cross-body / horizontal-adduction position); an AP radiograph of the AC joint is taken in that position.
- In a horizontally stable joint the distal clavicle stays reduced relative to the acromion. In a horizontally unstable joint the distal clavicle overrides the acromion — the dynamic shift that a static AP film misses.
- It is the radiographic counterpart of the clinical cross-body adduction (horizontal stress) test already described in the examination: pain plus a demonstrable override signals horizontal instability.
Using it to subdivide the controversial grade III (ISAKOS / Beitzel)
- Type IIIA (stable)
- No clavicular overriding — joint stays reduced
- Type IIIB (unstable)
- Overriding distal clavicle — dynamic horizontal instability
- Type IIIA (stable)
- No significant scapular dysfunction
- Type IIIB (unstable)
- Therapy-resistant scapular dyskinesis
- Type IIIA (stable)
- Favour non-operative — behaves like a stable injury
- Type IIIB (unstable)
- Consider operative stabilisation, especially in the overhead/throwing athlete
The practical sequence is therefore: confirm the grade on AP/Zanca, exclude a posterior Type IV with the axillary view, then use the cross-body adduction view plus a scapular assessment to decide whether a grade III is a IIIA (trial conservative, as the great majority of athletes are) or a IIIB (the small subgroup in whom early surgery is reasonable). A trial of structured physiotherapy is part of the definition — it is therapy-resistant scapular dysfunction, not dysfunction at presentation, that defines IIIB.
The axillary lateral answers "is this a posterior Type IV?" — a hard surgical indication. The cross-body adduction view answers "is this grade III horizontally stable (IIIA) or unstable (IIIB)?" — the question that actually triages the controversial grade III in the athlete. Vertical displacement on the AP film alone does not decide the operation.
Management Algorithm
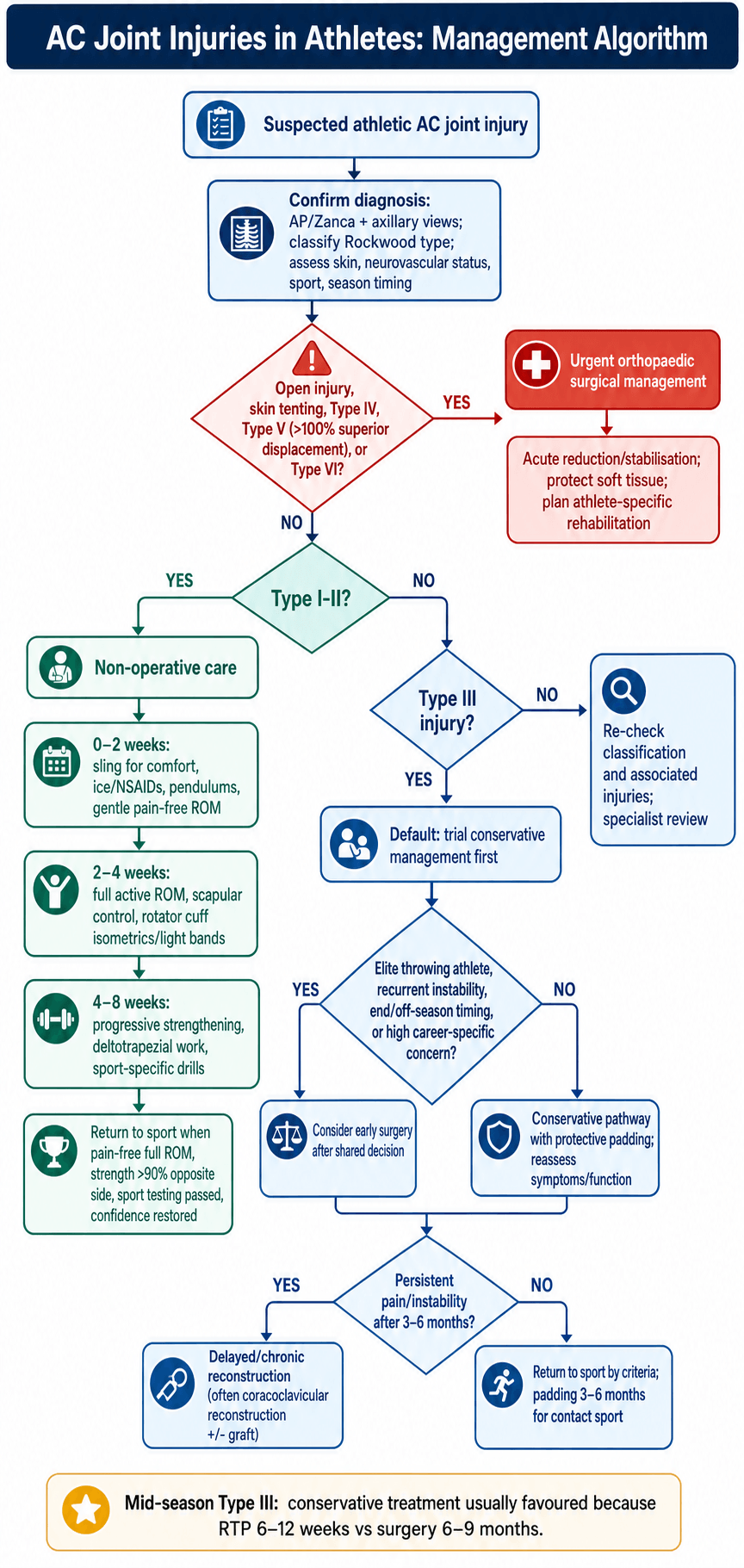
The management decision in the athlete turns on grade, sport demands, and timing in the season — weigh these factors together (the ATHLETE and SPORT frameworks at the top of this page capture them).
Conservative Management - Type I-III Athletes
Pain control, protect healing tissues
- Ice 20 minutes every 2-3 hours
- NSAIDs (ibuprofen 400mg TDS or naproxen 500mg BD)
- Sling for comfort (wean by day 3-5)
- Avoid provocative movements (cross-body, overhead)
- Pendulum exercises starting day 2-3
- Pain-free gentle ROM
Light cardio only if tolerated, no upper body
Restore ROM, begin strengthening
- Progress to full active ROM
- Scapular stabilization exercises
- Rotator cuff isometrics
- Light resistance band exercises
- Avoid heavy loading, cross-body movements
Upper body ergometer, light weights (under 5kg)
If pain-free ROM and strength over 80%, progress to Phase 3 sport-specific
Restore strength, begin sport-specific training
- Progressive resistance training
- Deltotrapezial strengthening (shrugs, rows)
- Sport-specific movement patterns
- Proprioceptive training
- Bench press, push-ups (if pain-free)
Isokinetic strength over 90% contralateral for all movements
Progress to Phase 4 if strength goals met
Safe return to full competition
- Full contact practice with protective padding
- Sport-specific drills at game intensity
- Psychological readiness assessment
- Maintenance strengthening program
- Full pain-free ROM
- Strength over 90% contralateral (all movements)
- Sport-specific testing passed
- Athlete confidence restored
AC joint padding for contact sports for 3-6 months
80-90% of athletes with Type III AC injuries return to sport successfully with conservative treatment. This includes contact and throwing athletes. Surgery should be reserved for the 10-20% who fail conservative treatment at 3-6 months.
In-Season Management: Playing Through an AC Injury
A question the previous sections answer only indirectly is the one the athlete and coach actually ask on the sideline: "Can I keep playing now?" The definitive treatment timeline (6–12 weeks conservative, 6–9 months surgical) is a separate question from the short-term in-season decision about returning to the same match or the same week.
Who can play through, and when
- Same-game / same-week return
- Often possible once pain is controlled and ROM/strength allow safe participation
- How it is managed in-season
- Analgesia, an AC-joint 'donut' pad or strapping, taping; symptom-limited return
- Same-game / same-week return
- Not same-game; default is a short protected period then a graded return within the season
- How it is managed in-season
- Sling for comfort, early ROM, protective padding; return only once pain settles and criteria are met
- Same-game / same-week return
- No — remove from play; these are surgical injuries
- How it is managed in-season
- Protect the limb and arrange surgical management; do not return to contact
Principles of playing through a low-grade injury
- Protect the joint mechanically. A purpose-made AC "donut" pad offloads a direct blow to the point of the shoulder; shoulder padding or strapping is the mainstay for the contact athlete who returns to play.
- Control pain — do not mask a dangerous injury. Simple analgesia and ice allow participation in a low-grade sprain, but pain control must never be used to push a high-grade or undiagnosed (potential Type IV) injury back onto the field.
- Re-examine and image before clearing for contact. Exclude a Type IV (axillary view) and a distal clavicle fracture before deciding an athlete can play on — the deformity of a high-grade separation can be mistaken for a "minor" one on the sideline.
- Shared decision and timing. The choice to play through — particularly mid-season or in playoffs — is made with the athlete after explaining that continued play carries a re-injury risk and that definitive treatment (almost always conservative) can usually wait for the off-season without compromising the eventual result.
Returning an athlete to play within days is reasonable for a Type I–II injury with controlled pain and protective padding. For a Type III the in-season goal is a short protected period and a graded, criteria-based return — not a same-game decision — while definitive (usually conservative) management proceeds. Type IV–VI come off the field for surgery.
Surgical Techniques for Athletes
Clavicle Hook Plate Fixation


- Acute injury (under 3 weeks)
- Type III-V where rapid rigid fixation desired
- Off-season timing (allows removal at 3-4 months before next season)
- Beach chair position, 30-45° upright
- Superior incision along Langer lines
- Identify and preserve lateral cutaneous nerve branches
- Reduce AC joint with manual pressure
- Hook placed 10-15mm medial to lateral clavicle edge
- Hook length: 15-18mm (avoid over-stuffing subacromial space)
- 3-4 cortical screws in clavicle
- Robust deltotrapezial fascia repair (critical for athletes)
- Deltotrapezial repair is CRITICAL - provides load sharing, allows earlier RTP
- Use non-absorbable suture (FiberWire, Ethibond) for fascia repair
- Rigid fixation allows earlier ROM compared to CC reconstruction
- Plan removal at 3-4 months (second surgery)
- Subacromial impingement if hook too long or medial (50% if not removed)
- Acromion fracture/erosion (5-10%)
- Loss of reduction after removal (10-15%)
- MUST remove at 3-4 months - non-negotiable
Athletes MUST have hook plate removed at 3-4 months. Plan this during off-season if possible. After removal, allow 4-6 weeks before contact sport return. Some loss of reduction after removal is normal but usually asymptomatic.

Complications in Athletes
- Incidence
- 15-20% conservative
- Impact on RTP
- Repeat time loss, may require surgery
- Prevention/Management
- Protective padding, strengthening, technique modification
- Incidence
- 10-20% both treatments
- Impact on RTP
- Limits performance, may end career
- Prevention/Management
- Adequate rehab, consider delayed surgery if conservative fails
- Incidence
- 5-10% (usually mild)
- Impact on RTP
- Reduces power in throws, tackles
- Prevention/Management
- Intensive strengthening, scapular stabilization
- Incidence
- 20-30% chronic instability
- Impact on RTP
- Secondary rotator cuff/labral issues
- Prevention/Management
- Scapular-focused rehab, periscapular strengthening
- Incidence
- 1-2% surgical cases
- Impact on RTP
- Delays RTP 3-6 months, may require hardware removal
- Prevention/Management
- Sterile technique, perioperative antibiotics
- Incidence
- 5-15% depending on technique
- Impact on RTP
- Requires revision surgery, extends RTP
- Prevention/Management
- Appropriate technique, adequate fixation, protect healing
- Incidence
- 2-5% CC reconstruction
- Impact on RTP
- Requires extended immobilization, delayed RTP
- Prevention/Management
- Avoid excessive tunnel size, adequate bone stock
Career-ending complications:
While rare, certain complications may end athletic careers:
- Chronic pain syndrome - failed conservative and surgical treatment
- Recurrent instability - multiple surgical failures
- Neurovascular injury - brachial plexus injury during surgery (very rare)
- Chronic shoulder dysfunction - secondary rotator cuff or labral pathology
Cosmetic deformity (visible bump) occurs in 80% of conservative Type III and 20% of surgical cases. This does NOT correlate with athletic performance or career longevity. Multiple studies show elite athletes perform at same level with cosmetic deformity. Counsel athletes appropriately.
Prevention of complications:
- Proper surgical technique
- Adequate rehabilitation compliance
- Protected return to sport
- Protective equipment for contact sports
- Monitoring for secondary pathology
Postoperative Care and Return to Play
Whether recovery has been conservative or surgical, return to play is gated by the same criteria — full ROM, strength greater than 90% of the contralateral side, and pain-free sport-specific testing — not by time alone.
Surgical rehabilitation protocol:
Protect repair, prevent stiffness
- Sling full time except exercises
- Pendulum exercises only
- Elbow/wrist/hand ROM
- No active shoulder motion
- Ice, wound care
- Sling when walking/sleeping
- Passive ROM to 90° elevation, neutral rotation
- Active-assisted ROM begins week 4
- Scapular retraction exercises (pain-free)
- No lifting, no resisted motion
Full passive ROM, pain under 3/10, wound healed
Full active ROM, begin strengthening
- Wean sling by week 6-8
- Progress to full active ROM
- Light resistance exercises (1-2kg)
- Scapular stabilization focus
- Rotator cuff strengthening
- Avoid heavy lifting, contact
- ROM: Should match contralateral
- Strength: 50-60% contralateral
- Pain: Under 2/10 with activities
Full pain-free active ROM, strength over 50%
Restore strength, begin sport-specific training
- Progressive resistance training
- Bench press, overhead press (light initially)
- Push-ups, pull-ups
- Plyometric exercises (late phase)
- Sport-specific movement patterns
- Proprioceptive training
- Strength: 80-90% contralateral
- Pain: Minimal (under 1/10)
- Functional testing passed
Strength over 85%, pain-free sport simulation
Safe return to full competition
4-5 months Contact sports: 6-9 months Throwing sports: 6-12 months (gradual throwing progression)
- Full pain-free ROM
- Strength over 90% contralateral (all movements)
- Isokinetic testing passed
- Sport-specific drills at game intensity
- Psychological readiness
- Clearance from surgeon and athletic trainer
AC joint padding for contact sports 6-12 months
- Type I: 2-4 weeks
- Type II: 4-6 weeks
- Type III: 6-12 weeks
- Hook plate: 6-9 months
- CC reconstruction: 6-9 months
- After hook plate removal: additional 4-6 weeks protected
- Contact practice without pain
- Tackling drills (for applicable positions)
- Strength over 95% (contact demands high)
- Protective AC joint padding
- AC joint-specific pad (donut design)
- Worn for 3-6 months after RTP
- May reduce re-injury risk by 30-40%
Collision positions (linebacker, prop forward, defenseman) may need longer RTP timeline and more extensive strengthening compared to skill positions (quarterback, backs, forwards). Assess demands individually.
Outcomes and Return to Performance
Conservative treatment outcomes:
- RTP Rate
- 95-100%
- Time to RTP
- 2-4 weeks
- Same Level Performance
- 95%
- Notes
- Excellent prognosis
- RTP Rate
- 90-95%
- Time to RTP
- 4-6 weeks
- Same Level Performance
- 90%
- Notes
- May have minor cosmetic deformity
- RTP Rate
- 80-90%
- Time to RTP
- 6-12 weeks
- Same Level Performance
- 85%
- Notes
- Cosmetic deformity common but functional
Surgical outcomes:
- Success Rate
- 80-85%
- RTP Contact Sport
- 6-9 months
- Same Level Performance
- 80-85%
- Complications
- Removal required, impingement risk
- Success Rate
- 85-90%
- RTP Contact Sport
- 6-9 months
- Same Level Performance
- 85-90%
- Complications
- Lower failure vs Weaver-Dunn
- Success Rate
- 80-85% (early data)
- RTP Contact Sport
- 4-6 months
- Same Level Performance
- 85%
- Complications
- Limited long-term data
Elite athlete performance data shows NO significant difference in career longevity, statistics, or performance metrics between athletes with conservative vs surgical treatment for Type III injuries. Cosmetic deformity does NOT predict performance.
- Young age (under 25 years)
- Type I-II injury
- Compliance with rehabilitation
- Access to specialized sports medicine care
- Off-season injury timing
- Non-throwing sport
- Type V injury (severe soft tissue disruption)
- Multiple re-injuries
- Associated pathology (rotator cuff, labrum)
- Poor rehabilitation compliance
- In-season injury with rushed return
- Throwing athlete with Type III
- 95% RTP after Type I-II
- 85% RTP after Type III (conservative)
- Same performance statistics pre vs post-injury
- Average time loss: 2-4 weeks Type I-II, 6-8 weeks Type III
- 90% RTP after conservative Type III
- Forwards (higher re-injury): 20% re-injury rate
- Backs (lower re-injury): 10% re-injury rate
- Protective padding reduces re-injury by 30-40%
- 80% RTP after Type III conservative
- Velocity loss under 5% (not significant)
- Surgery delays RTP but similar long-term outcomes
- Biomechanics normalize by 6-12 months
Guidelines, Registries & Global Practice
Global epidemiology
AC joint injury is one of the most common shoulder injuries in young, athletic populations, with a clear male predominance and a peak in the second and third decades of life. The highest rates occur in collision and contact sports (rugby, American football, ice hockey) and in cycling and skiing, typically from a direct fall onto the point of the shoulder. Low-grade injuries (Rockwood I-II) are substantially more frequent than high-grade injuries (III-VI). These patterns are consistent across the major systematic reviews and consensus statements cited below; OrthoVellum reports them as the global picture rather than any single nation's data.
Major guidelines and consensus statements — side by side
- Scope
- Classification of the grade III controversy
- Key position
- Subdivide grade III into stable IIIA (non-operative) and unstable IIIB (consider surgery), using the cross-body adduction view and scapular dysfunction
- Evidence basis
- Level V expert consensus
- Scope
- European diagnosis and treatment
- Key position
- True AP or bilateral Zanca sufficient for diagnosis; cross-body override test for horizontal instability; arthroscopically-assisted suspensory reconstruction without biological augmentation for acute injuries; tendon-graft biological reconstruction for chronic; 3-week acute/chronic cut-off
- Evidence basis
- Modified Delphi (greater than 66.7% agreement)
- Scope
- Grade I-II and most acute grade III
- Key position
- Non-operative first-line for I-III; surgery reserved for IV-VI and selected/failed III
- Evidence basis
- Supported by the COTS Level I RCT
- Scope
- Operative technique
- Key position
- Anatomic CC (and AC) reconstruction preferred over historic non-anatomic transfers; preserve coracoacromial ligament
- Evidence basis
- Expert/biomechanical
Registry note: AC joint injuries are soft-tissue ligamentous injuries treated by repair/reconstruction rather than arthroplasty, so they are not captured by the national joint replacement registries (NJR, AJRR, AOANJRR, SHAR, etc.). The best population-level evidence therefore comes from RCTs (COTS), systematic reviews (Kay, Gawel, Smith) and sports-injury surveillance datasets rather than implant registries.
Practice variation
- Grade III is the genuine area of global disagreement: most North American and UK practice favours an initial non-operative trial (COTS RCT), whereas some European/sports-medicine centres operate earlier on the unstable IIIB subtype, on high-demand throwing athletes, or where horizontal instability is demonstrated.
- Acute vs chronic threshold is set at roughly 3 weeks internationally (ESA-ESSKA): acute injuries are amenable to suspensory/hook fixation, chronic injuries generally require biological graft reconstruction.
- Resource setting: in lower-resource settings, simpler constructs (hook plate, K-wire historically) are used because graft and suspensory implants are costly; in well-resourced centres, arthroscopically-assisted anatomic reconstruction predominates.
- Return-to-play decisions remain mostly time-based (Gawel review) — typically around 6 months after surgery and 6-12 weeks after non-operative care — with a global shift toward criteria-based clearance (full pain-free ROM, strength greater than 90% contralateral, sport-specific testing).
MCQ Practice Points
Q: A 20-year-old college football linebacker sustains an acute Type III AC separation mid-season. What is the most appropriate initial management?
A: Conservative treatment with sling, ice, analgesia, and early ROM. Level I evidence (COTS RCT) shows no clinical difference in outcomes between operative and non-operative high-grade injuries at 2 years. 80-90% of athletes RTP successfully with conservative treatment. Surgery reserved for failed conservative at 3-6 months or specific indications (throwing athletes, off-season timing).
Q: An athlete with Type III AC separation asks about return to contact sport timeline. What is the expected RTP with conservative vs surgical treatment?
A: Conservative: 6-12 weeks. Surgical: 6-9 months. This timeline difference is CRITICAL when counseling athletes, especially mid-season. Surgical treatment commits to season-ending recovery, while conservative allows potential return same season.
Q: What imaging view is ESSENTIAL to differentiate Type III from Type IV AC joint separation?
A: Axillary lateral view. Type IV (posterior displacement) looks identical to Type III on AP view. Axillary view shows clavicle displaced posterior to acromion. Failing to obtain axillary view leads to missed Type IV diagnosis and failed conservative treatment.
Q: Why might throwing athletes have different outcomes with Type III AC separations compared to contact athletes?
A: Throwing biomechanics place high stress on AC joint during late cocking (horizontal abduction) and deceleration phases. AC instability can cause scapular dyskinesis, reduce throwing velocity by 10-15%, and increase risk of secondary rotator cuff or labral pathology. Some throwing athletes may benefit from early surgery, though evidence is mixed.
Q: Why is hook plate NOT suitable for chronic AC joint injuries (over 6 weeks)?
A: Hook plate provides temporary rigid fixation that requires removal at 3-4 months. It works in acute injuries where soft tissue healing is occurring. In chronic injuries, soft tissues have already healed in malaligned position and anatomic CC ligament reconstruction is needed to restore stability. Hook plate would fail in chronic setting.
Q: What Level I evidence exists regarding Type III AC separation management in athletes?
A: The Canadian Orthopaedic Trauma Society (COTS) RCT (2015, J Orthop Trauma) randomised 83 patients with acute complete (grade III-V) dislocations to hook plate vs non-operative treatment. No significant difference in DASH or Constant scores at 6 months, 1 year, or 2 years; the operative group had better radiographic alignment but a higher reoperation rate. Smith et al meta-analysis (2011, J Orthop Traumatol) pooled 6 case series and found no functional difference for grade III (better cosmesis but longer sick leave with surgery). Together these support conservative first-line treatment.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old professional cricket fast bowler sustained a Type III AC joint separation to his bowling arm 2 weeks ago during a match. X-rays show 80% superior displacement with CC distance 18mm (contralateral 12mm). He is currently mid-season with 6 weeks remaining. His team is in playoff contention and wants him to return ASAP. He asks about surgery. How would you manage this case?”
“A 19-year-old university rugby prop forward presents with recurrent right AC joint instability. He had a Type III AC separation 9 months ago treated conservatively. He returned to rugby at 10 weeks wearing protective padding but has had 3 episodes of the shoulder 'giving way' during scrums. X-rays show persistent 60% superior displacement. He is currently off-season with 4 months until pre-season training. What is your management?”
“A 24-year-old professional cyclist presents to you 3 weeks after a high-speed crash. He was diagnosed with a Type III AC separation at another hospital and treated with sling for 2 weeks. He has been trying to return to training but has severe pain and the shoulder 'doesn't feel right.' On examination the lateral clavicle is prominent posteriorly and difficult to palpate anteriorly. You review the images - there is an AP shoulder X-ray showing superior clavicle displacement but no axillary view was done. What is your concern and management?”
TYPE III CONTROVERSY IN ATHLETES
- COTS RCT (Level I): NO clinical difference operative vs conservative at 2 years
- 80-90% of athletes RTP successfully with conservative treatment
- Conservative RTP: 6-12 weeks vs Surgical RTP: 6-9 months
- Default to CONSERVATIVE even in elite athletes
- Consider surgery: throwing athletes, failed conservative 3-6 months, off-season
- Cosmetic deformity does NOT predict athletic performance
RETURN TO SPORT CRITERIA
- Full pain-free ROM (equal to contralateral)
- Strength over 90% contralateral (all movements, isokinetic testing)
- Sport-specific testing passed (throwing velocity, tackling drills, etc)
- Psychological readiness restored
- Protective AC joint padding for contact sports 3-6 months
SPORT-SPECIFIC TIMELINES
- Contact sports (AFL, rugby): 6-12 weeks conservative, 6-9 months surgical
- Throwing sports (cricket, baseball): 8-16 weeks conservative, 6-12 months surgical
- Overhead sports (swimming, tennis): 6-10 weeks conservative, 4-6 months surgical
- Cycling: 4-8 weeks conservative, 4-6 months surgical
- Re-injury rate contact sports: 15-20% (protective padding reduces by 30-40%)
IMAGING ESSENTIALS
- MANDATORY: AP + Zanca + AXILLARY view (all AC injuries)
- Axillary view ONLY way to diagnose Type IV (posterior displacement)
- Type IV looks IDENTICAL to Type III on AP view alone
- Stress views controversial, rarely change management
- MRI for chronic pain (distal clavicle osteolysis, cuff pathology)
SURGICAL DECISION-MAKING
- Absolute indications: Type IV, V, VI
- Relative indications athletes: throwing athletes, failed conservative 3-6 months
- Hook plate: acute only (under 3 weeks), MUST remove 3-4 months
- Anatomic CC reconstruction: chronic injuries, throwing athletes, permanent solution
- TightRope: minimally invasive, no removal, faster RTP, emerging technique
- CRITICAL: robust deltotrapezial fascia repair for all athletes
THROWING ATHLETE SPECIFICS
- Late cocking phase: peak AC joint stress (horizontal abduction)
- AC instability causes scapular dyskinesis, reduces velocity 10-15%
- May benefit from early surgery (controversial, no Level I evidence)
- Interval throwing program: 12 weeks gradual progression
- Monitor velocity, mechanics, pain throughout progression
CRITICAL EXAM TRAPS
- Don't reflexively operate on Type III athletes (80-90% conservative success)
- Don't miss Type IV (no axillary view = missed diagnosis)
- Don't use hook plate for chronic injuries (over 6 weeks)
- Don't forget deltotrapezial repair (critical for athletes)
- Don't rush return (re-injury risk 15-20% if premature)
- Don't ignore cosmetic deformity counseling (expected, doesn't affect function)
Evidence Base
- 83 patients with acute complete (Rockwood grade III, IV, V) AC dislocations randomised to hook plate fixation (n=40) vs non-operative treatment (n=43). The non-operative group had significantly better DASH scores at 6 weeks and 3 months, but there was NO significant difference at 6 months, 1 year, or 2 years (mean DASH 5-6, Constant 91-95 in both). Operative group had superior radiographic alignment but a significantly higher reoperation rate.
- Systematic review and meta-analysis of 6 eligible studies (all retrospective case series) on Rockwood grade III dislocation. Operative management gave a better cosmetic outcome (p less than 0.0001) but a longer duration of sick leave (p less than 0.001). There was NO difference in strength, pain, throwing ability, or rate of AC osteoarthritis. Authors concluded there is a lack of well-designed studies to define optimal treatment.
- ISAKOS Upper Extremity Committee consensus subdividing the controversial Rockwood grade III. Grade IIIA = stable AC joint with no clavicular overriding on cross-body adduction view and no significant scapular dysfunction (favour non-operative). Grade IIIB = therapy-resistant scapular dysfunction with an overriding clavicle on cross-body adduction view (consider operative). The cross-body (modified Basamania) view and dynamic assessment guide the operative decision.
- 12 studies (315 patients, mean age 33.8 years) on surgical management of AC dislocation. Return to any level of sport ranged 94-100%; return to pre-injury level ranged 62-100%. Pooled return to pre-injury level was 89.6% for type III/IV injuries and 86.2% for type V. Rates were comparable across injury types and surgical techniques.
- 63 studies reporting at least one explicit return-to-play criterion after AC joint surgery. Time from surgery was by far the most common criterion (95.2% of studies), with 6 months the most frequent timeline (37.8%); reported timelines ranged 2-12 months. Only 4 studies (6.3%) used conditional criteria (ROM, strength, clinical/radiographic stability, functional and safety testing, hardware removal).
- 35 patients with acute AC dislocation: minimally invasive single-TightRope CC fixation (n=16) vs clavicular hook plate (n=19), mean follow-up 27-30 months. No significant difference in VAS, UCLA, or Constant-Murley scores. Hook plate gave better reduction; TightRope tended toward less pain. Redislocation 1/16 (6.3%) in the TightRope group; acromial osteolysis 1/19 (5.3%) in the hook plate group. The hook plate requires a second operation for removal.