Pivot Shift | Graft Selection | Tunnel Placement | Return to Sport
- ACL is PRIMARY restraint to anterior tibial translation
- Pivot shift is most specific clinical test
- Wait 3+ weeks post-injury to reduce arthrofibrosis risk
- Anatomic tunnel placement critical - avoid high noon position
- BTB autograft remains gold standard for young athletes
- “Segond fracture = pathognomonic for ACL tear
- “Associated meniscal tears in 50%+ of acute injuries
- “Allograft failure 4x higher in patients under 25
- “STABILITY trial: LET reduces graft failure in high-risk
Pivot shift test is most specific for ACL deficiency. Demonstrates rotational instability. Grade correlates with functional disability.
Anatomic femoral tunnel at center of native footprint. Old high noon position is NON-ANATOMIC. Use anteromedial portal technique.
BTB autograft = gold standard for young athletes. Fastest bone-to-bone healing. Avoid allograft in under 25 years old.
Wait 3+ weeks before surgery. Regain full ROM first. Early surgery = arthrofibrosis risk.
- Advantages
- Fastest integration
- Disadvantages
- Anterior knee pain
- Best For
- Young athletes, contact sports
- Advantages
- Less knee pain
- Disadvantages
- Slower integration
- Best For
- Non-contact sports
- Advantages
- Strong graft
- Disadvantages
- Quad weakness
- Best For
- Revision surgery
- Advantages
- No donor morbidity
- Disadvantages
- 4x failure in young
- Best For
- Low-demand older than 35
GRAFTACL Reconstruction Principles
Hook:Get the GRAFT right for successful reconstruction!
Overview and Epidemiology
Females have 2-8x higher ACL injury rate than males in same sports. Factors: narrower notch, hormonal, neuromuscular patterns. Prevention programs reduce risk by 50%.
- ACLR incidence ~46/100,000/year (German registry data)
- Peak age: 15-25 years
- Female greater than male (same sport)
- High-risk: soccer, basketball, skiing
- 70% non-contact injuries
- Meniscal tears: 50%+ acute
- MCL injury: contact mechanism
- Bone bruise pattern: posterolateral tibia
- Segond fracture: pathognomonic
- Lateral meniscus root tears
Pathophysiology and Mechanisms
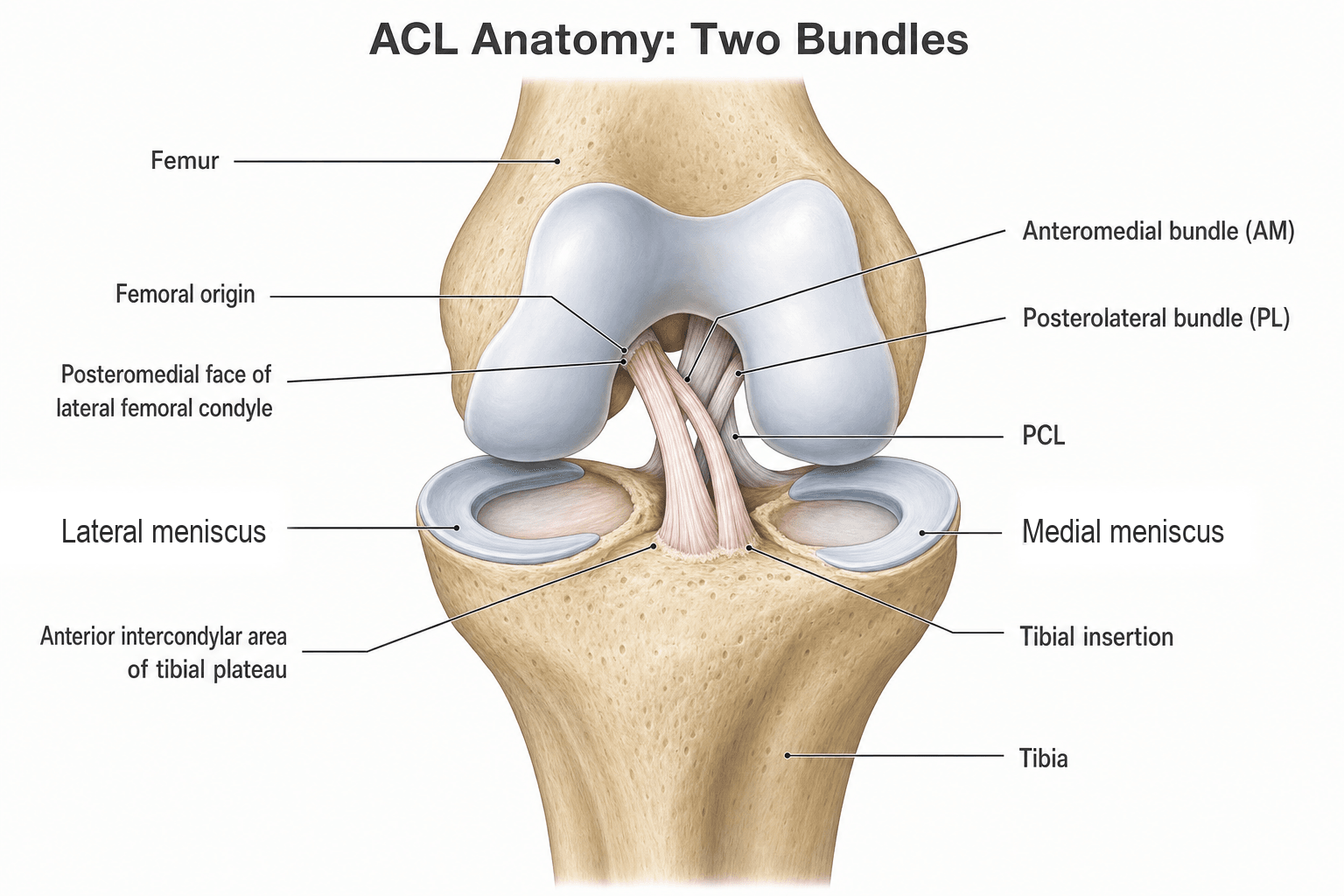
ACL Anatomy
Posteromedial lateral femoral condyle in intercondylar notch.
Anterior intercondylar tibia, anterolateral to medial tibial spine.
- Anteromedial (AM): tight in flexion
- Posterolateral (PL): tight in extension
Middle genicular artery. Poor vascularity limits healing.
30-35mm. Width: 10-12mm.
Understanding AM and PL bundles is important for anatomic reconstruction. Aim to recreate center of native footprint - double-bundle reconstruction has not shown superiority in most studies.
Classification Systems
ACL Injury Grading
- Pathology
- Microscopic tears
- Clinical Finding
- Firm endpoint
- Treatment
- Conservative
- Pathology
- Partial macroscopic
- Clinical Finding
- Endpoint present
- Treatment
- Variable
- Pathology
- Complete rupture
- Clinical Finding
- No endpoint, positive pivot
- Treatment
- Reconstruction
Most presentations are Grade III (complete tears).
Clinical Assessment
- Mechanism: Non-contact pivot, pop heard
- Immediate swelling: Hemarthrosis
- Instability: Giving way with pivoting
- Sport level: Determines treatment
- Previous injuries: Contralateral ACL
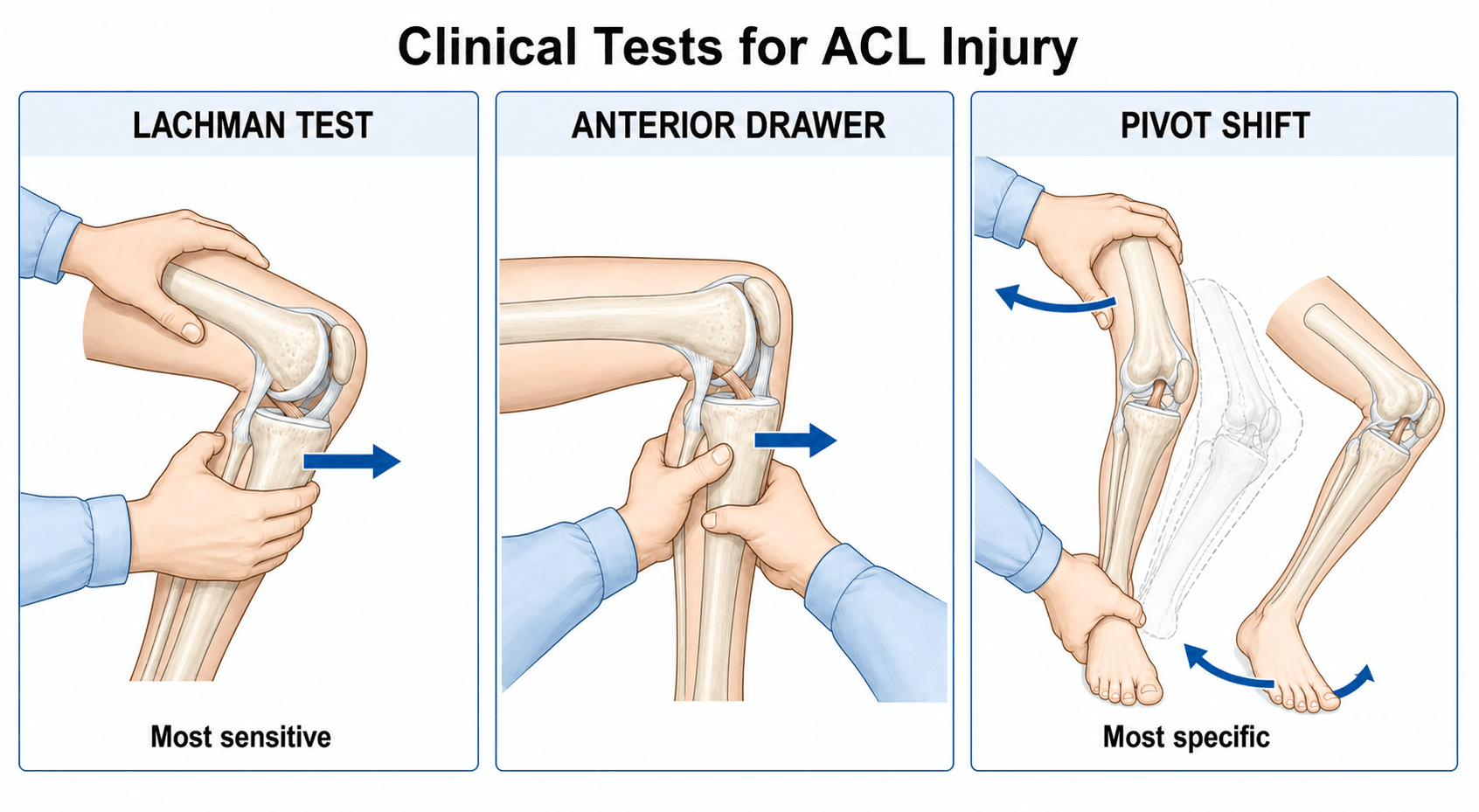
- Lachman test: Most sensitive (85-95%)
- Anterior drawer: Less sensitive
- Pivot shift: Most specific
- Associated injuries: MCL, meniscus
- Effusion: Hemarthrosis acute
Knee 20-30 degrees flexion. Stabilize femur. Translate tibia anteriorly. Positive: Increased translation AND soft/absent endpoint. Compare to contralateral side.
Key Clinical Pearls
Best with patient relaxed (EUA). Demonstrates functional rotational instability causing giving way.
Always check MCL, menisci, posterolateral corner.
Differential Diagnosis of the Acute Haemarthrotic Knee
- Distinguishing Feature
- Non-contact pivot, pop, rapid effusion, positive Lachman/pivot shift
- Confirming Test
- MRI; EUA
- Distinguishing Feature
- Lateral patellar apprehension, medial tenderness (MPFL)
- Confirming Test
- MRI - MPFL tear, lateral femoral/medial patellar bone bruise
- Distinguishing Feature
- True locking, joint-line tenderness, slower effusion
- Confirming Test
- MRI
- Distinguishing Feature
- Dashboard/hyperflexion mechanism, positive posterior drawer/sag
- Confirming Test
- Posterior drawer, MRI
- Distinguishing Feature
- Haemarthrosis with fat globules on aspiration
- Confirming Test
- Radiograph/CT
- Distinguishing Feature
- Gross instability in multiple planes, vascular concern
- Confirming Test
- Vascular assessment, MRI
A tense haemarthrosis after a twisting injury is ACL rupture until proven otherwise, but patellar dislocation and peripheral meniscal tears are the commonest mimics. Always exclude a spontaneously reduced knee dislocation when more than one ligament is involved.
LAPClinical Tests for ACL
Hook:LAP up the ACL tests!
Investigations
Standard Views
Alignment, fractures.
Segond fracture, tibial plateau.
- Segond fracture: Pathognomonic for ACL tear
- Tibial spine fracture: Common in children
- Deep lateral notch sign: Greater than 1.5mm
These radiographic signs should prompt further evaluation with MRI.

Segond fracture = small avulsion lateral tibial plateau = anterolateral ligament avulsion. Pathognomonic for ACL injury. Associated with high-grade pivot shift.

Management Algorithm
Management Pathway
ACL Injury Management
RICE, aspiration for comfort, brace, physiotherapy for ROM.
Consider: age, activity, sports demands, instability, associated injuries.
Low-demand, willing to avoid pivoting, no giving way, older patient.
Young active, pivoting sports, recurrent instability, repairable meniscus.
Surgical Technique
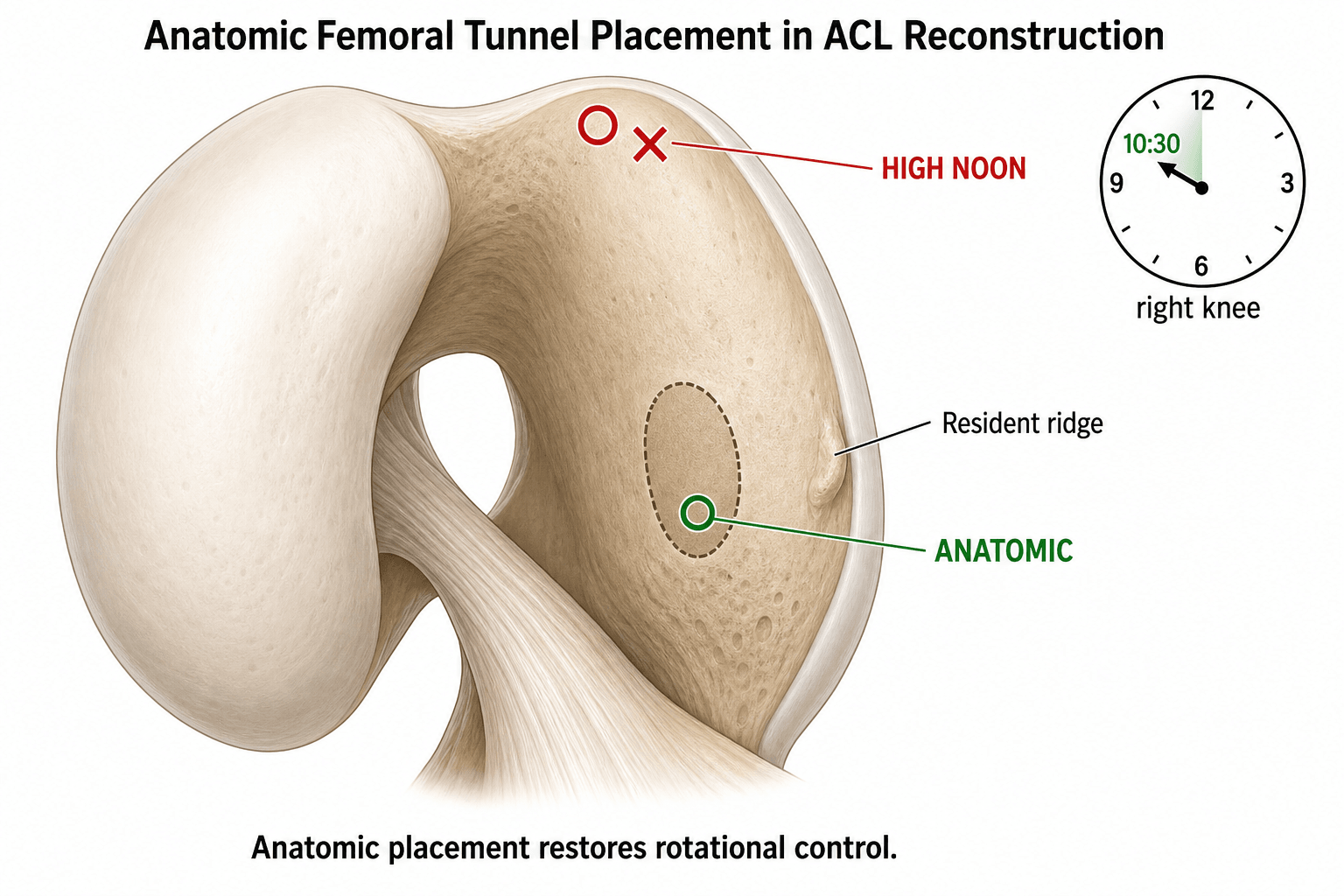
Anatomic Tunnel Position
- Center of native ACL footprint
- NOT high noon (non-anatomic)
- Use anteromedial portal technique
- Resident ridge as posterior landmark
- Anterolateral to medial tibial spine
- 1:30 (right) or 10:30 (left) position
Anatomic placement is essential for restoring rotational stability.
Old transtibial technique placed femoral tunnel too vertically. This is non-anatomic with poor rotational control. Use anteromedial portal for anatomic placement (10:30 right knee).
The Anterolateral Complex and Lateral Extra-Articular Tenodesis (LET)
The topic mentions LET and the STABILITY trial repeatedly - the examiner will expect you to explain what the anterolateral structures are and what the operation does.
The anterolateral complex is a secondary restraint to internal rotation (the pivot shift) and comprises:
- The anterolateral ligament (ALL) - from the lateral femoral epicondyle to the anterolateral tibia between Gerdy's tubercle and the fibular head (its bony avulsion is the Segond fracture).
- The iliotibial band with its deep Kaplan fibres and the anterolateral capsule.
Lateral extra-articular tenodesis (LET) is an extra-articular augment - classically a strip of iliotibial band (modified Lemaire or MacIntosh technique) left attached distally at Gerdy's tubercle, routed deep to the LCL and fixed to the lateral femur - that reduces anterolateral rotatory instability and offloads the intra-articular graft. Anatomic ALL reconstruction with a free graft is an alternative.
- Why
- Highest re-rupture risk group (STABILITY population)
- Why
- Residual rotatory laxity not controlled by the intra-articular graft alone
- Why
- Greater rotatory load on the graft
- Why
- Protects the revision graft and addresses persistent rotatory instability
- Why
- A recognised driver of graft failure that adds anterior load
In the STABILITY RCT, adding a lateral extra-articular tenodesis to a hamstring ACL reconstruction in young high-risk pivoting patients cut graft rupture from about 11% to 4%. Reserve LET (or anatomic ALL reconstruction) for the high-risk knee: young, pivoting sport, high-grade pivot shift, hyperlaxity, revision, or high posterior tibial slope - it controls the rotatory instability the intra-articular graft alone may not.
Complications
- Risk Factors
- Early surgery, poor ROM
- Prevention
- Wait 3+ weeks, restore ROM
- Management
- Aggressive PT, lysis
- Risk Factors
- Allograft young, malposition
- Prevention
- Autograft, anatomic tunnels
- Management
- Revision ACLR
- Risk Factors
- BTB graft
- Prevention
- Hamstring/quad graft
- Management
- Usually settles
- Risk Factors
- Any surgery
- Prevention
- Aseptic technique
- Management
- Washout, antibiotics
Highest failure risk: Allograft in under 25 (4x), RTS before 9 months, non-anatomic tunnels. BTB autograft + anatomic tunnels + delayed RTS minimizes failure.
ACL Injury in the Skeletally Immature
ACL reconstruction in a child with open physes is a distinct problem because tunnels can injure the growth plate. The distal femoral physis contributes the majority of lower-limb growth, so a misplaced tunnel, a bone block, or hardware across it risks growth arrest, limb-length discrepancy or angular deformity.
Assess skeletal maturity, not just age (bone age and Tanner stage) and match the technique to it:
- Preferred technique
- Physeal-sparing (all-epiphyseal, or combined intra/extra-articular iliotibial band - Micheli-Kocher)
- Principle
- Avoid crossing the physis entirely
- Preferred technique
- Transphyseal with SOFT-TISSUE graft
- Principle
- Vertical central tunnels, no bone block or fixation across the physis, smaller tunnels
- Preferred technique
- Standard adult reconstruction
- Principle
- Physeal risk negligible
Crucially, do not simply wait for maturity in an unstable knee: a complete tear left unreconstructed in an active child leads to recurrent giving way and progressive, often irreparable, meniscal and chondral damage. The displaced tibial eminence (spine) avulsion is the paediatric bony equivalent of a mid-substance tear and is fixed (arthroscopic suture or screw).
In the skeletally immature knee, judge by bone age and Tanner stage: physeal-sparing reconstruction for the prepubescent child, transphyseal soft-tissue graft (no bone block or hardware across the physis) for the adolescent, standard reconstruction near maturity. Tunnels across an open physis risk growth arrest and deformity - but leaving an unstable knee unreconstructed risks irreversible meniscal/chondral damage, so age-appropriate reconstruction is favoured over watchful waiting.
PIVOTACL Injury Mechanism
Hook:PIVOT mechanism causes ACL tears - pivot shift tests for it!
Postoperative Care
Rehabilitation Protocol
Brace locked extension. WBAT with crutches. ROM 0-90 degrees. Quad sets, SLR.
Unlock brace. Progressive ROM. Stationary bike. Patellar mobilization.
Wean crutches. Pool running. Closed chain exercises. Proprioception.
Running program (straight). Progressive resistance. Late agility.
Cutting/pivoting. Sport drills. Psychological readiness.
Full competition after functional tests. Hop tests, strength greater than 90%.
Before RTS: Hop test LSI greater than 90%, quad strength greater than 90%, no effusion, full ROM, ACL-RSI passed, minimum 9 months. Each month delay reduces re-injury risk.
Outcomes and Prognosis
Outcome Factors
Anatomic reconstruction, appropriate graft, compliant rehab, adequate time, isolated injury.
Malposition, early RTS, cartilage injury, meniscectomy, non-compliance.
Long-Term
50% develop radiographic OA by 10-15 years regardless of treatment. Higher if meniscectomy.
10-25% lifetime risk, especially young females.
Guidelines, Registries & Global Practice
Global Epidemiology
- ACLR incidence ~46/100,000/year (German inpatient data, Domnick 2017)
- Peak age: 15-25 years; second mid-life peak in women
- Males higher absolute volume; females higher per-exposure risk
- Highest-risk sports: football/soccer, basketball, skiing, handball
- ~70% of injuries are non-contact (cutting/landing)
- Female sex (per-exposure), narrow intercondylar notch
- Increased posterior tibial slope
- Generalised ligamentous laxity
- Neuromuscular control (dynamic valgus on landing)
- Prior ACL injury (ipsi- or contralateral)
Major Guidelines, Side by Side
- AAOS CPG 2023
- Reconstruction improves activity/stability in active patients; rehab reasonable in lower-demand
- NICE / UK practice
- Trial of rehab acceptable; reconstruct if instability persists or high demand
- Evidence
- Moderate (KANON, AAOS systematic review)
- AAOS CPG 2023
- Autograft (BTB or hamstring) over allograft, especially in young/active
- NICE / UK practice
- Autograft preferred in young; allograft reserved for selected older/low-demand
- Evidence
- Strong for autograft in young (MOON/MARS)
- AAOS CPG 2023
- Option in high-risk revision/young pivoting patients
- NICE / UK practice
- Increasingly offered to high-risk young pivoting patients
- Evidence
- Level 1 (STABILITY)
- AAOS CPG 2023
- Delay and use objective criteria, not time alone
- NICE / UK practice
- Criteria-based RTS, typically not before 9 months
- Evidence
- Level 3 (Grindem/Delaware-Oslo)
The AAOS 2023 ACL Clinical Practice Guideline (Brophy & Lowry, J Am Acad Orthop Surg) gives 8 recommendations plus 7 options: autograft over allograft in young/active patients, anatomic single-bundle reconstruction, and criteria-based (not purely time-based) return to sport.
Landmark Trials That Shape Practice
- Design
- RCT 121 acute tears
- Take-home
- Rehab + optional delayed ACLR equals early ACLR at 2-5y; many avoid surgery
- Design
- RCT 618, ACLR +/- LET
- Take-home
- LET cut graft rupture 11% to 4% in high-risk young patients
- Design
- Prospective cohort
- Take-home
- Allograft 4x failure vs autograft in young patients
- Design
- 1205 revision ACLRs
- Take-home
- Autograft 2.78x lower re-rupture than allograft at revision
- Design
- Prospective cohort
- Take-home
- Each month RTS delay to 9 months cut re-injury 51%
Global Practice Variation
- Graft default: hamstring dominant in Europe/Scandinavia (~90% in German data); BTB/quadriceps more favoured for high-demand contact athletes elsewhere
- Timing: early reconstruction common in athlete-focused systems; rehab-first with optional delayed ACLR (KANON model) used widely in Scandinavia
- LET use: rising globally after STABILITY, fastest in young pivoting and revision cases
- Surgeon training and registry feedback (e.g. Scandinavian, NZ knee-ligament registries)
- Patient demand profile and sport culture
- Access, theatre capacity and rehab resourcing
- Interpretation of equivalence trials (KANON) vs failure-reduction trials (STABILITY)
ACL injuries are an extremely common viva topic across FRCS (Tr & Orth), FRACS, EBOT and ABOS. Know graft selection, the rehab-vs-reconstruct debate (KANON), surgical timing, anatomic tunnel placement, LET indications (STABILITY) and criteria-based RTS (Grindem).
MCQ Practice Points
Q: Primary function of ACL? A: Restraint to anterior tibial translation - 85% of restraint at 30 degrees. Also resists internal rotation and hyperextension.
Q: Most sensitive clinical test for ACL? A: Lachman test (85-95% sensitive). At 20-30 degrees flexion. Assess translation AND endpoint quality.
Q: Most specific clinical test for ACL? A: Pivot shift test. Demonstrates rotational instability causing functional giving way.
Q: What does Segond fracture indicate? A: ACL rupture (pathognomonic). Avulsion lateral tibial plateau. Associated high-grade pivot shift.
Q: Why avoid allograft in young athletes? A: 4x higher failure rate in under 25. Slower incorporation, remodeling issues.
Q: Primary risk of ACL surgery within 3 weeks? A: Arthrofibrosis. Wait for ROM recovery. Optimal timing 4-12 weeks.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 20-year-old male soccer player presents 2 weeks after a non-contact pivoting injury. He heard a pop and had immediate swelling. Examination shows positive Lachman and pivot shift. MRI confirms complete ACL tear without meniscal injury. How would you manage this?”
“A 30-year-old female recreational skier needs ACL reconstruction but is concerned about anterior knee pain as she kneels frequently for work. She asks about graft options. What would you discuss?”
“A 23-year-old presents 18 months after hamstring ACL reconstruction. He returned to soccer at 7 months and now has recurrent instability. MRI shows graft rupture. CT shows vertical femoral tunnel. How would you approach this?”
Clinical Tests (LAP)
- Lachman: Most sensitive 85-95%
- Anterior drawer: Less sensitive
- Pivot shift: Most specific
- Compare endpoint quality
Graft Selection
- BTB: Gold standard young athletes
- Hamstring: Less anterior knee pain
- Quad: Growing popularity
- Allograft: Over 35 only (4x failure young)
Surgical Timing
- Wait 3+ weeks post-injury
- Regain full ROM extension
- Early surgery = arthrofibrosis
- Optimal: 4-12 weeks
Tunnel Placement
- Anatomic = center of footprint
- Avoid high noon non-anatomic
- Use anteromedial portal
- 10:30 right or 1:30 left
Return to Sport
- Minimum 9 months post-op
- Hop test LSI greater than 90%
- Quad strength greater than 90%
- Each month delay = 51% less re-injury
Evidence Base and Key Studies
KANON Trial - Early ACLR vs Rehab + Optional Delayed
- RCT, 121 young active adults with acute ACL tear
- Early ACLR + rehab vs rehab + optional delayed ACLR
- No difference in 2-year KOOS (between-group 0.2 points)
- 61% of the optional-delayed group avoided surgery
MARS Cohort - Graft Choice in Revision ACLR
- 1205 revision ACLRs, 83 surgeons, 52 sites
- Autograft predicted better 2-year IKDC and KOOS sport/QoL
- Graft re-rupture 3.3% at 2 years
- Autograft 2.78x less likely to re-rupture vs allograft
Timing of ACL Reconstruction (Hamstring)
- RCT, 69 patients, early (within 21 days) vs delayed (beyond 6 weeks)
- Hamstring autograft, identical extension-focused rehab in both arms
- No difference in postoperative range of motion lost
- No difference in KT-1000 stability or subjective scores
STABILITY Trial - LET
- RCT ACLR +/- lateral extra-articular tenodesis
- 618 patients randomized
- ACLR + LET: 4% graft rupture
- ACLR alone: 11% graft rupture
Return to Sport Timing
- 106 pivoting-sport athletes, prospective 2-year cohort (Delaware-Oslo)
- Reinjury rate reduced 51% for each month RTS was delayed up to 9 months (no further reduction after 9 months)
- Returning to level I sport gave a 4.3x higher reinjury rate; failing RTS criteria 38.2% reinjured vs 5.6% who passed
- More symmetrical quadriceps strength before return was protective
Allograft Failure in Young
- MOON prospective longitudinal cohort (model built on 281 ACLRs, validated on a further 645)
- Allograft reconstruction carried ~4x the odds of graft rupture versus autograft
- Age was an independent predictor: odds of rupture rose ~2.3x for each 10-year decrease in age, highest in the 10-19 age group
- Graft type and patient age were the significant predictors of failure