Rockwood Classification Guides Treatment | CC Ligaments Key | Type III Controversial
- CC ligaments (conoid + trapezoid) provide vertical stability - torn in Type III+
- AC ligaments (superior most important) provide horizontal stability
- Type III is controversial - most now treated conservatively unless high-demand athlete/laborer
- Type IV posterior displacement may look like Type III on AP - need axillary view
- Hook plate requires removal at 3-4 months - mandatory second surgery
- “Rockwood classification expanded Tossy (I-III) to include Types IV-VI
- “CC distance greater than 13mm or greater than 50% increase compared to contralateral = Grade III+
- “AC ligament superior portion provides 56% of horizontal stability
- “Type VI inferior dislocation extremely rare - associated with severe trauma

Most examiners want conservative first for Type III. Consider surgery in: throwing athletes, heavy laborers, failed conservative 3-6 months. Don't reflexively operate!
Axillary view is MANDATORY - Type IV posterior displacement looks like Type III on AP. Weighted views controversial but may help quantify displacement.
CC ligaments = vertical stability (torn III+). AC ligaments = horizontal stability (superior portion 56%, posterior 25%). Know their anatomic insertions.
Hook plate: temporary fixation, MUST remove 3-4 months, acute only. CC reconstruction: anatomic (both ligaments) better than Weaver-Dunn. Know indications for each.
- CC Ligaments
- Intact (sprained)
- Displacement
- None - tenderness only
- Treatment
- Sling 1-2 weeks, ice, early ROM
- CC Ligaments
- Sprained (intact)
- Displacement
- AC widened, slight step
- Treatment
- Sling 2-4 weeks, conservative
- CC Ligaments
- TORN
- Displacement
- 25-100% superior
- Treatment
- CONTROVERSIAL - conservative first
- CC Ligaments
- Torn
- Displacement
- Posterior into trapezius
- Treatment
- Surgical - needs axillary view to diagnose
- CC Ligaments
- Torn + deltotrapezial
- Displacement
- Greater than 100-300% superior
- Treatment
- Surgical - severe soft tissue injury
- CC Ligaments
- Torn
- Displacement
- Inferior (subcoracoid)
- Treatment
- Surgical - extremely rare, high-energy
ROCKROCK - Rockwood Type III Decision
Hook:ROCK solid conservative management first for Type III
CCCC Ligaments - TACO
Hook:TACO - Trapezoid And Conoid On coracoid - Trapezoid lateral, Conoid medial
ACAC Ligaments - SAPI
Hook:SAPI - Superior and Posterior most Important for AP stability
HOOKHOOK - Hook Plate Rules
Hook:HOOK plate requires HOOK removal - plan the second surgery
Overview and Epidemiology
AC joint injuries are common shoulder injuries, particularly in young active males participating in contact sports. They result from disruption of the ligamentous structures stabilizing the acromioclavicular joint.
- Direct blow - fall onto point of shoulder with arm adducted (most common)
- Indirect - fall onto outstretched hand with transmitted force
- Contact sports - rugby, AFL, ice hockey, cycling crashes
- Contact sports participation
- Male gender
- High-velocity activities (cycling, motorcycling)
- Previous AC joint injury
Tossy classification (1963) described Types I-III. Rockwood expanded this to include Types IV-VI, recognizing different displacement patterns that require surgical intervention.
Anatomy and Biomechanics
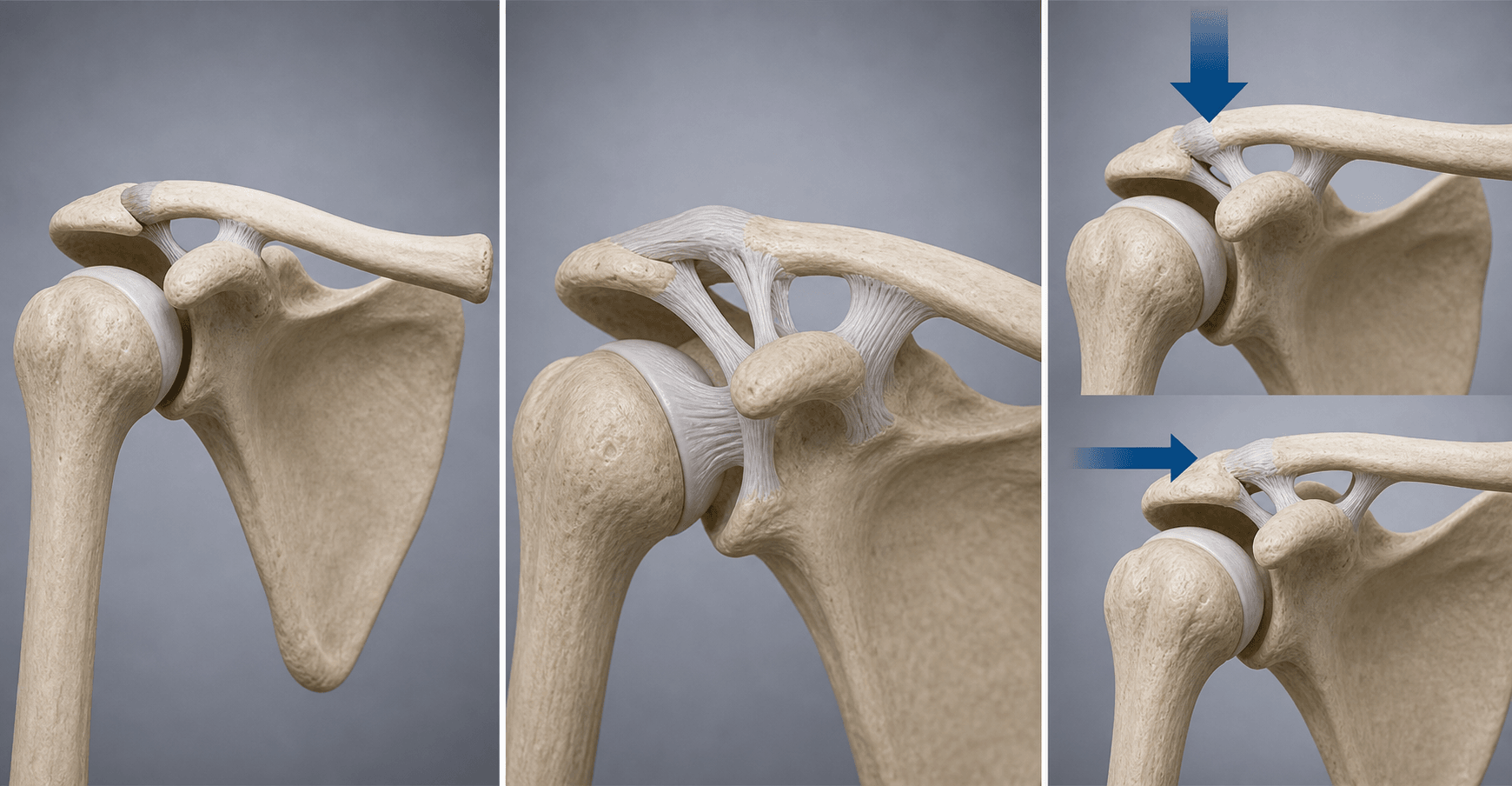

AC Joint anatomy:
- Synovial diarthrodial joint between lateral clavicle and medial acromion
- Contains fibrocartilaginous intra-articular disc (degenerates with age)
- Joint capsule reinforced by AC ligaments
- Small contact area with high stress concentration
AC Ligaments (horizontal stability):
- Contribution
- 56%
- Function
- Most important for AP stability
- Contribution
- 25%
- Function
- Second most important
- Contribution
- Minor
- Function
- Weak contribution
- Contribution
- Minor
- Function
- Least important
The superior AC ligament is the most important for horizontal (AP) stability, contributing 56%. It blends with the deltotrapezial fascia to form a strong superior stabilizer.
CC Ligaments (vertical stability):
- Position
- Lateral
- Distance from AC
- 20mm
- Shape
- Quadrilateral
- Strength
- Weaker
- Position
- Medial
- Distance from AC
- 45mm
- Shape
- Conical
- Strength
- Stronger
Trapezoid is LATERAL, Conoid is MEDIAL. The conoid is the stronger ligament. Both insert on the undersurface of the clavicle and the base of the coracoid process. Anatomic reconstruction must address BOTH ligaments.
- Deltoid - originates from lateral clavicle and acromion anteriorly
- Trapezius - inserts on clavicle and acromion posteriorly
- Deltotrapezial fascia - critical for stability and surgical repair
- CC distance: 11-13mm (normal)
- AC joint width: 1-3mm (normal)
- Side-to-side CC difference: less than 50% variation is normal
Classification Systems
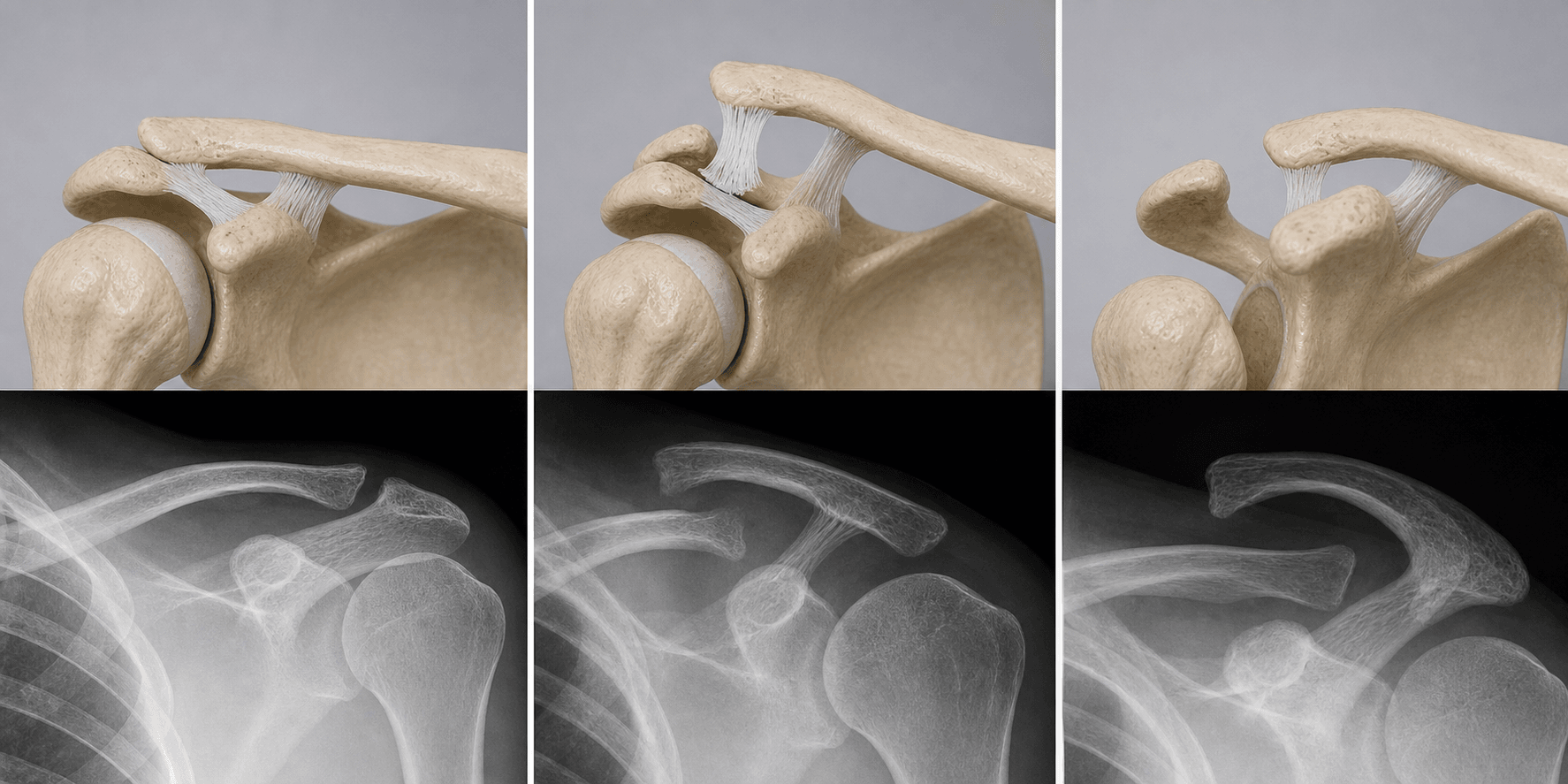
Type I - AC Ligament Sprain
- AC ligaments sprained but intact
- CC ligaments intact
- No displacement on X-ray
- Tenderness over AC joint only
Treatment: Sling 1-2 weeks, ice, early ROM Prognosis: Excellent - full recovery expected

- AC Ligaments
- Sprained
- CC Ligaments
- Intact
- Displacement
- None
- Surgery?
- No
- AC Ligaments
- Torn
- CC Ligaments
- Sprained
- Displacement
- Slight (AC widened)
- Surgery?
- No
- AC Ligaments
- Torn
- CC Ligaments
- TORN
- Displacement
- 25-100% superior
- Surgery?
- Controversial
- AC Ligaments
- Torn
- CC Ligaments
- Torn
- Displacement
- Posterior
- Surgery?
- Yes
- AC Ligaments
- Torn
- CC Ligaments
- Torn
- Displacement
- Over 100% superior
- Surgery?
- Yes
- AC Ligaments
- Torn
- CC Ligaments
- Torn
- Displacement
- Inferior
- Surgery?
- Yes
SPATIRockwood Classification
Hook:SPATIal orientation of the clavicle!
Clinical Presentation and Assessment
History:
- Mechanism: fall onto point of shoulder, direct blow
- Time since injury
- Sport/occupation
- Hand dominance
- Overhead requirements (throwing athlete, laborer)
- Previous AC joint problems
Physical examination:
- Type I
- Present
- Type II
- Present
- Type III+
- Present
- Significance
- Non-specific
- Type I
- None
- Type II
- Slight
- Type III+
- Obvious
- Significance
- Indicates severity
- Type I
- Negative
- Type II
- May be positive
- Type III+
- Positive
- Significance
- CC ligament integrity
- Type I
- Positive
- Type II
- Positive
- Type III+
- Positive
- Significance
- AC joint pathology
- Type I
- None
- Type II
- Present
- Type III+
- Present
- Significance
- AC ligament tear
- Patient reaches hand to opposite shoulder
- Positive: pain at AC joint
- Sensitive but not specific for AC injury
- Arm 90° flexion, 10° adduction, internally rotated (thumb down)
- Resist downward force
- Positive: pain at AC joint relieved with supination
- May also be positive for SLAP lesions
- Examiner presses lateral clavicle inferiorly
- Positive: clavicle depresses then springs back
- Indicates CC ligament compromise
- Stabilize acromion, translate clavicle AP
- Increased translation = AC ligament tear
Always examine for associated injuries: scapula fracture (floating shoulder), clavicle shaft fracture, rotator cuff pathology. Examine neurovascular status and check for skin tenting (relative surgical indication). High-grade dislocations carry an appreciable rate of occult intra-articular pathology - arthroscopy in surgically treated type III-V injuries found intra-articular lesions in 18.2%, including SLAP lesions in 14.3%.
Differential diagnosis of the painful/deformed superolateral shoulder:
- Distinguishing features
- Step-off at AC joint, point tenderness, positive cross-body adduction
- Key investigation
- Zanca + axillary view; CC distance
- Distinguishing features
- Tenderness medial to AC joint, crepitus; can mimic high-grade AC injury (Neer/Craig type II)
- Key investigation
- Plain radiograph; CT if comminuted
- Distinguishing features
- Medial-end pain/asymmetry; posterior type threatens mediastinal structures
- Key investigation
- Serendipity view / CT chest
- Distinguishing features
- Chronic, activity-related pain, no acute trauma; weightlifters (distal clavicle osteolysis)
- Key investigation
- Zanca view; MRI; diagnostic injection
- Distinguishing features
- Painful arc, weakness, Neer/Hawkins positive; cross-body test less localised
- Key investigation
- MRI / ultrasound
- Distinguishing features
- Deep shoulder pain, positive O'Brien relieved by supination; co-exists with high-grade AC injury
- Key investigation
- MR arthrography; arthroscopy
Investigations
Standard imaging:
AP Shoulder/Zanca View:
- Zanca view: 10-15° cephalic tilt, centered on AC joint
- Compare CC distance bilaterally
- Measure AC joint width
- Assess displacement percentage
The Zanca view (10-15° cephalic tilt) is optimal for AC joint assessment. It angles the beam perpendicular to the AC joint plane, reducing overlap from spine and scapula.
Axillary Lateral View (ESSENTIAL):
- MUST obtain in all AC joint injuries
- Only view to identify Type IV (posterior displacement)
- Shows hook of acromion, coracoid, glenoid
- Type IV: clavicle posterior to acromion
Never diagnose or treat an AC joint injury without an axillary view. Type IV posterior displacement looks identical to Type III on AP view. Missing Type IV leads to failed conservative treatment.
Stress Views (Controversial):
- Weighted views (5-10kg weights in hands)
- May help differentiate Type II from III
- Most centers no longer routinely use
- Pain limits utility in acute setting
Radiographic measurements:
- Normal
- 11-13mm
- Type III+
- Over 13mm or over 50% increase
- Normal
- 1-3mm
- Type III+
- Over 5mm widening
- Normal
- Under 50%
- Type III+
- Over 50%
- Suspected fracture (clavicle, acromion, coracoid)
- Failed conservative treatment (evaluate for occult fracture)
- Preoperative planning for complex reconstruction
- Suspected associated rotator cuff injury
- Chronic AC joint pain (evaluate disc, OA)
- Preoperative assessment in delayed reconstruction
Management
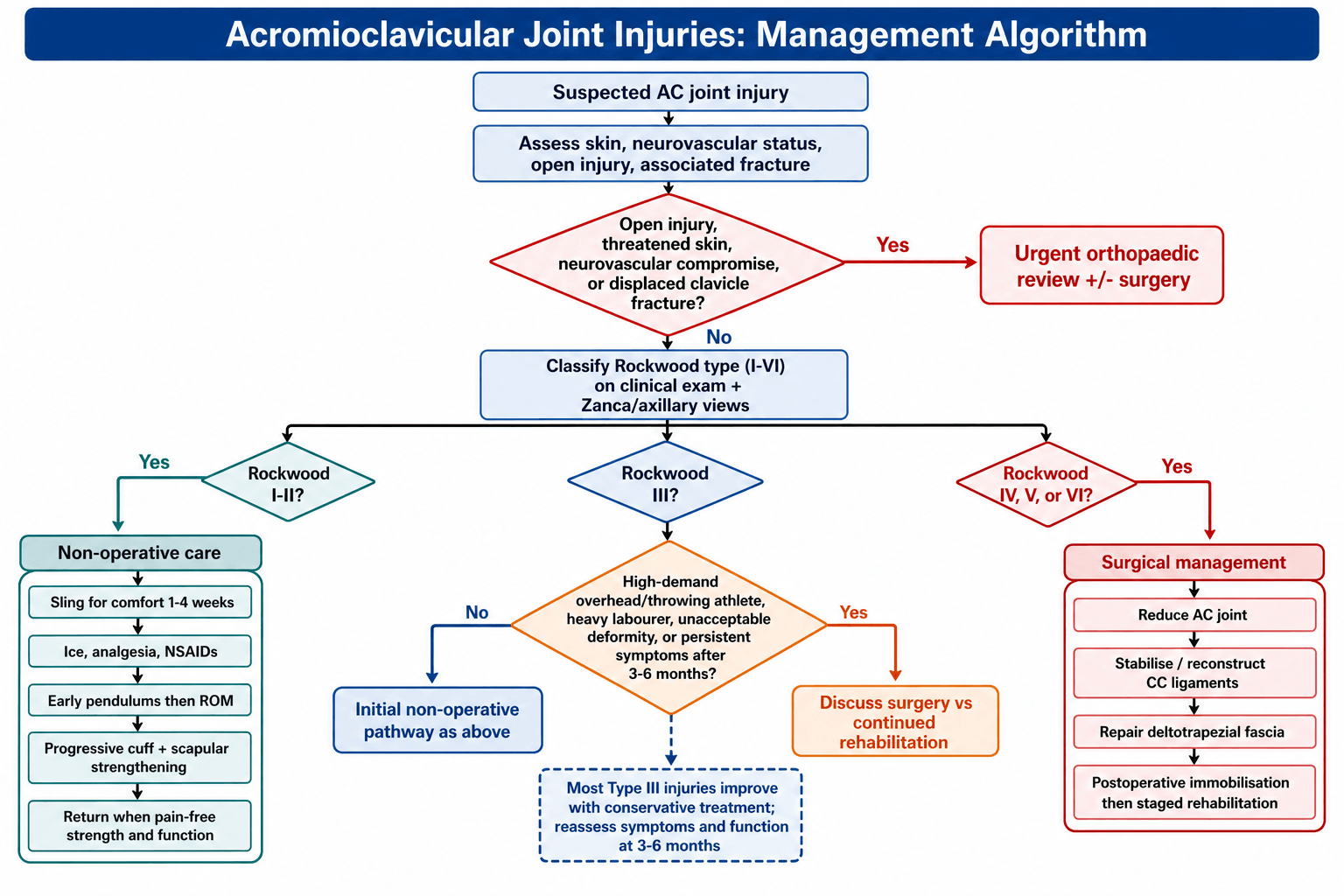
Conservative management (Types I-II, most Type III):
- Ice, analgesia, NSAIDs
- Sling for comfort
- Avoid aggravating activities
- Gentle pendulum exercises
- Wean sling as pain allows
- Active ROM exercises
- Avoid cross-body movements initially
- No heavy lifting
- Progressive strengthening
- Rotator cuff and scapular exercises
- Sport-specific rehabilitation
- Return to non-contact sport when pain-free
- Return to contact sport when full strength
- Some persistent cosmetic deformity acceptable
- Protective padding if returning to collision sports
80-90% of Type III injuries treated conservatively achieve satisfactory outcomes. Persistent symptoms at 3-6 months warrant reconsidering surgery, but this is uncommon.
A high-yield point that explains both missed injuries and failed surgery: the AC joint is stabilised in two planes, and the classification/imaging fixates on only one:
- Vertical stability is from the coracoclavicular (conoid + trapezoid) ligaments - lost in Type III+ and what the CC distance on the AP film measures.
- Horizontal (anteroposterior) stability is from the acromioclavicular capsule/ligaments (especially the superior and posterior AC ligament) - and this is routinely under-assessed.
Why it matters:
- Posterior/horizontal instability is easily missed (a Type IV looks like a Type III on the AP - you need the axillary/Alexander (cross-body) views and dynamic assessment with cross-body adduction to detect posterior translation of the clavicle).
- A reconstruction that only restores the CC (vertical) ligaments can still fail if horizontal instability is not addressed - persistent pain and a positive cross-body sign despite an "acceptable" CC distance. This is why modern anatomic reconstructions increasingly add an AC-joint/horizontal-plane stabilisation (AC cerclage/augmentation) on top of CC reconstruction.
Exam point: assess and treat both planes - CC ligaments (vertical, AP film) and the AC capsule (horizontal, axillary/cross-body views) - because unrecognised horizontal instability is a classic cause of a missed Type IV and of a symptomatic CC-only reconstruction.
Surgical Technique
Clavicle Hook Plate Fixation

Hook extends under acromion into subacromial space, plate secures to clavicle, pulls clavicle down to reduce AC joint
- Acute injuries only (less than 3 weeks)
- Type III-V where rapid rigid fixation desired
- Technically simpler
- Rigid fixation
- No graft harvest required
- MUST be removed at 3-4 months (mandatory second surgery)
- High complication rate if not removed (50% impingement)
- Subacromial impingement/rotator cuff irritation
- Acromion fracture or erosion (5-10%)
- Not suitable for chronic injuries
Hook plates MUST be removed at 3-4 months. Complications if left include: subacromial impingement (50%), acromion fracture, rotator cuff damage, plate breakage. Always plan the second surgery.

Complications
- Conservative
- 10-20%
- Hook Plate
- 10-20%
- CC Reconstruction
- 10-15%
- Conservative
- Common (accepted)
- Hook Plate
- Low (while in)
- CC Reconstruction
- Low
- Conservative
- N/A
- Hook Plate
- 10-15% (after removal)
- CC Reconstruction
- 10-15%
- Conservative
- N/A
- Hook Plate
- Up to 50% if not removed
- CC Reconstruction
- Rare
- Conservative
- N/A
- Hook Plate
- Common (requires removal)
- CC Reconstruction
- 5-10%
- Conservative
- N/A
- Hook Plate
- Acromion 5-10%
- CC Reconstruction
- Coracoid/clavicle 2-5%
- Conservative
- Rare (under 10%)
- Hook Plate
- 100% (mandatory)
- CC Reconstruction
- 10-20%
- Persistent pain (10-20% - usually mild)
- Cosmetic deformity (common - usually well-tolerated)
- AC joint arthritis (long-term)
- Failed conservative requiring delayed surgery (5-10%)
- Subacromial impingement (up to 50% if hook too long/medial)
- Acromion fracture or erosion (5-10%)
- Mandatory hardware removal (100% - second surgery)
- Recurrent instability after removal (10-15%)
- Rotator cuff irritation/damage
- Loss of reduction/failure (10-15%)
- Coracoid fracture (2-5%)
- Clavicle fracture through tunnels
- Graft site morbidity (if autograft)
- Infection (1-2%)
- Nerve injury (rare - musculocutaneous, suprascapular)
Distal clavicle excision (Mumford procedure) can address AC joint arthritis but does NOT treat instability. In chronic AC separations with arthritis, combine CC reconstruction with limited (5-7mm) distal clavicle excision if needed.
COFSurgical Complications
Hook:Watch out for the COF (Cough) when operating!
Postoperative Care and Rehabilitation
Post-operative protocol (CC reconstruction):
- Sling full time
- Pendulum exercises only
- Ice, wound care
- No active shoulder movement
- Sling when walking/out
- Passive ROM to 90° elevation, neutral rotation
- Active elbow and wrist ROM
- No lifting
- Wean sling
- Active-assisted then active ROM
- Progressive strengthening begins at 8 weeks
- No heavy lifting
- Full active ROM
- Progressive strengthening
- Sport-specific training
- Return to contact sport 6-9 months
Hook plate specific protocol:
- Similar early protocol to above
- Hardware removal at 3-4 months (mandatory)
- After removal: 2-4 weeks protected, then progressive activity
- Some loss of reduction after removal is normal (usually asymptomatic)
Robust deltotrapezial fascia repair is critical for success. This layer shares load with the CC reconstruction and prevents superior instability. Failure of this repair leads to persistent pain and weakness.
Outcomes and Prognosis
- Type I-II: Excellent outcomes, full recovery expected
- Type III: 80-90% satisfactory, may have cosmetic deformity
- Most patients return to full sport/activity
- Type IV-VI: Good outcomes with surgery (90% satisfaction)
- Type III (delayed surgery): Similar outcomes to early surgery
- Anatomic reconstruction superior to Weaver-Dunn
Cosmetic deformity (persistent bump) is common after conservative or surgical treatment. This is usually well-tolerated and does NOT correlate with functional outcome. Counsel patients preoperatively.
Factors affecting outcome:
- Accuracy of diagnosis (don't miss Type IV)
- Patient selection (appropriate conservative vs surgical)
- Surgical technique (anatomic reconstruction preferred)
- Rehabilitation compliance
- Associated injuries (rotator cuff, fractures)
Guidelines, Registries & Global Practice
Global epidemiology:
- In a population-based Scottish study, the acromioclavicular joint accounted for an incidence of 8.9 dislocations per 100,000 per year (Hindle et al., Injury 2013), making it one of the more frequently dislocated joints of the appendicular skeleton.
- Strongly male-predominant and concentrated in the young active population (mean age mid-30s in operative series), with a peak in the second-to-fourth decades.
- Mechanism is typically a direct blow to the point of the shoulder (contact and collision sports - rugby codes, American football, ice hockey, AFL) or a cycling/motorcycling fall; the same mechanism predominates internationally.
- Most injuries are low-grade (Rockwood I-II); complete (III-VI) dislocations are the minority but generate most of the surgical workload and controversy.
Side-by-side guideline and society positions:
- Position on Type III
- Non-operative first-line; surgery individualised for high-demand patients or failed conservative care
- Surgical types
- Type IV-VI (and selected V)
- Evidence level
- Level I RCT and meta-analysis
- Position on Type III
- Conservative initial management; shared decision-making, delayed reconstruction if symptomatic
- Surgical types
- Type IV-VI; selected high-grade III/V
- Evidence level
- Level I (ACORN, Cochrane)
- Position on Type III
- Acute complete injuries - anatomic CC/AC stabilisation when operative; reserves hook plate for selected acute cases
- Surgical types
- Type IV-VI; unstable V
- Evidence level
- Expert consensus + biomechanics
- Position on Type III
- Distinguishes stable vs unstable III (IIIa/IIIb); operative consideration for unstable IIIb and overhead athletes
- Surgical types
- Type IIIb-VI
- Evidence level
- Level II-III
Modern (ISAKOS-influenced) practice increasingly subdivides Rockwood III into IIIA (stable) - treated conservatively - and IIIB (unstable on dynamic/cross-body imaging, scapular dyskinesis, or overhead athlete**)** - where surgery is more readily considered. Quoting this nuance shows examiners you are current beyond the simple "III is controversial" line.
- There is no dedicated international AC-joint implant registry, but the pooled Level I evidence (COTS 2015, ACORN 2018, Cochrane 2010, Xie meta-analysis 2024) consistently shows no long-term functional advantage of surgery over conservative care for acute complete dislocations, with higher complication and reoperation rates in operative arms.
- Practice variation persists: surgeons in some European and North American centres favour early anatomic reconstruction (often arthroscopically assisted with suspensory devices) for high-grade injuries and athletes, whereas the default in the UK/Australasia remains conservative-first.
- Non-contact activity: ~6-8 weeks (conservative), ~12 weeks (after reconstruction).
- Contact/collision sport: 12+ weeks (conservative); ~6 months after reconstruction; protective padding for collision sports.
- Heavy manual/overhead work typically resumes ~12-16 weeks after reconstruction.
Be ready to summarise the Level I evidence (COTS, ACORN, Cochrane, Xie meta-analysis) showing equivalent long-term function for operative vs conservative care of complete dislocations, then nuance it with stable vs unstable type III and patient factors (overhead athlete, manual labourer). This combination of evidence plus individualised decision-making is what distinguishes a strong answer.
MCQ Practice Points
Q: Which AC ligament provides the majority of resistance to horizontal translation? A: Superior AC ligament (56%). The posterior AC ligament contributes 25%. The CC ligaments provide vertical (superior-inferior) stability, not horizontal.
Q: What distinguishes Type V from Type III AC joint separation? A: Deltotrapezial fascia detachment in Type V leads to greater than 100-300% superior displacement (vs 25-100% in Type III). Type V represents more severe soft tissue disruption.
Q: Which view is essential to differentiate Type III from Type IV AC separation? A: Axillary lateral view. Type IV has posterior clavicle displacement that cannot be seen on AP view. Missing Type IV leads to failed conservative treatment.
Q: What is the current consensus for treatment of Type III AC separations? A: Conservative management first for most patients. Surgery considered in: throwing athletes, heavy laborers, or after failed conservative treatment at 3-6 months. Multiple RCTs show no significant difference in outcomes.
Q: Why is the hook plate not suitable for chronic AC joint injuries? A: Hook plate provides temporary rigid fixation only (must be removed at 3-4 months). In chronic injuries, soft tissue healing has already occurred and anatomic CC ligament reconstruction is needed to address persistent instability.
Q: What is the anatomic position of the trapezoid vs conoid ligament? A: Trapezoid is LATERAL (20mm from AC joint), Conoid is MEDIAL (45mm from AC joint). Remember: TACO - Trapezoid And Conoid On coracoid, with Trapezoid lateral.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old rugby player presents after a tackle onto his right shoulder. X-rays show a Type III AC joint separation with CC distance 15mm (contralateral 11mm). He wants to return to professional rugby. How would you manage this patient?”
“A 40-year-old manual laborer presents 3 months after a cycling accident. He was treated conservatively for an AC joint injury but has persistent pain and cosmetic deformity. X-rays show 100% superior displacement with AC joint arthritis. What is your assessment and management?”
“A 30-year-old presents after a motorcycle accident with severe shoulder deformity. The AP X-ray shows what appears to be a Type III AC separation with significant superior displacement. On examination, the lateral clavicle cannot be palpated anteriorly and there is fullness posteriorly. What is your concern and management?”
ROCKWOOD CLASSIFICATION
- Type I: AC sprain, intact CC - conservative
- Type II: AC torn, CC sprain - conservative
- Type III: CC torn, 25-100% - CONTROVERSIAL (mostly conservative)
- Type IV: Posterior displacement - SURGICAL (need axillary view!)
- Type V: Over 100% superior, deltotrapezial detached - SURGICAL
- Type VI: Inferior (rare) - SURGICAL
KEY ANATOMY
- CC ligaments = VERTICAL stability (conoid medial, trapezoid lateral)
- AC ligaments = HORIZONTAL stability (superior 56%, posterior 25%)
- Normal CC distance: 11-13mm
- Trapezoid: 20mm from AC joint (lateral)
- Conoid: 45mm from AC joint (medial)
TYPE III CONTROVERSY
- Multiple RCTs show NO difference operative vs conservative
- Current consensus: CONSERVATIVE FIRST
- Consider surgery: throwing athletes, heavy laborers, failed conservative
- 80-90% satisfactory outcome with conservative treatment
IMAGING ESSENTIALS
- ALWAYS get AXILLARY VIEW (Type IV looks like III on AP)
- Zanca view: 10-15° cephalic tilt for AC joint
- CC distance increased over 50% or over 13mm = Type III+
- Weighted views controversial - rarely change management
SURGICAL OPTIONS
- Hook plate: ACUTE only, MUST remove at 3-4 months
- Anatomic CC reconstruction: Both ligaments, 10-15% failure
- Weaver-Dunn: Non-anatomic, 20-30% failure (historical)
- CC screw: Must remove 6-8 weeks (breakage risk)
TRAPS AND PEARLS
- Missing Type IV (no axillary view) = failed conservative
- Hook plate in chronic injury = wrong indication
- Forgetting hook plate mandatory removal = complications
- K-wire migration = unacceptable complication rate
- Cosmetic deformity doesn't predict function
Evidence Base
- Multicentre RCT of 83 patients with acute complete (Rockwood III-V) AC dislocations randomised to hook-plate fixation versus non-operative care. The non-operative group had significantly better DASH scores at 6 weeks and 3 months, with no significant difference at 6, 12 or 24 months (mean DASH 5-6 in both groups at 2 years). Hook-plate fixation gave superior radiographic alignment but a significantly higher reoperation rate.
- RCT of 60 patients (16-35 years) with acute type III/IV dislocations randomised to open reduction with tunnelled suspensory device versus non-operative care. Surgery markedly improved radiographic reduction (mean 1.75 mm vs 10.61 mm displacement) but gave no functional benefit at 1 year (DASH 5.63 vs 4.67) and cost over four times as much. However, 5 non-operative patients failed and required delayed reconstruction.
- Meta-analysis of 4 RCTs (244 patients) restricted to Rockwood type III. No significant difference in long-term Constant score (MD 4.82, 95% CI -6.42 to 16.06). Surgery gave better early pain relief and coracoclavicular distance but higher rates of post-traumatic osteoarthritis and hardware-related complications.
- Three trials (174 patients) of surgery (CC screws, AC pins/wires) versus sling. No significant difference in unsatisfactory shoulder function (RR 1.49, 95% CI 0.75-2.95) or treatment failure (RR 1.72, 95% CI 0.72-4.12). Fixation failures occurred in all trials (wire breakage 41%); surgery delayed return to work and routinely required implant removal.
- Controlled cadaveric study (42 shoulders) comparing anatomic CC reconstruction (free tendon graft reconstructing both conoid and trapezoid) with modified Weaver-Dunn and an arthroscopic technique. The modified Weaver-Dunn had significantly greater laxity than the anatomic reconstruction, which had significantly less anterior and posterior translation and more closely restored the intact state.
- Prospective sonographic study of 40 patients with an AO clavicular hook plate. Subacromial impingement developed in 37.5%, acromial bony erosion in 50%, and rotator cuff lesions in 6 patients; impingement correlated with poorer DASH and Constant scores.
- Cadaveric serial-sectioning study showing the superior and posterior AC capsular ligaments are the principal restraints to posterior clavicular translation, contributing 56% (+/-23%) and 25% (+/-16%) respectively; the anterior and inferior ligaments had no significant role.
- Universal force-moment sensor study of 10 cadaveric shoulders. The trapezoid ligament was the primary restraint to posterior clavicular displacement, providing 55.8% (+/-20.0%) of the resisting force, while the inferior AC capsule was the major restraint to anterior displacement.
- Arthroscopy in 77 surgically treated acute type III-V dislocations found intra-articular injuries in 18.2%, including SLAP lesions in 14.3% and supraspinatus tears in 3 patients. SLAP lesions were more common in type V (19%) than type IV (3.4%).