Surgical Emergency | Four-Compartment Fasciotomy | Time-Critical | Clinical Diagnosis
- Clinical diagnosis - pain out of proportion, pain on passive stretch, tense compartments
- Delta P less than 30mmHg = surgical indication (diastolic BP - compartment pressure)
- Two-incision, four-compartment release - lateral and medial approaches
- Do NOT wait for pulselessness - this is a late, irreversible sign
- Remove all circumferential dressings - may reduce pressure by 30-65%
- “The 6 P's are LATE signs - pain and pressure are early
- “Deep peroneal nerve (anterior compartment) - first web space sensation
- “Superficial peroneal nerve (lateral compartment) - dorsum of foot sensation
- “Document pre-op neurovascular status meticulously for medicolegal protection
- “Delayed primary closure at 3-5 days or STSG if unable to close
Post-Nail Pain: Escalating opioid doses. Conscious but Painful: Don't trust pulses. Obtunded Polytrauma: High suspicion → Measure pressures.
6-8 Hours: Irreversible necrosis. Delta P less than 30: Surgical threshold.
Release ALL Four: Local/Partial release = Negligence. 2 incisions required.
NEVER Say: "Wait and see", "Pulses are normal so it's fine", or "Just release anterior".
Overview and Epidemiology
Acute compartment syndrome (ACS) is a surgical emergency where elevated pressure within a closed fascial compartment compromises tissue perfusion. In the leg, untreated ACS leads to irreversible muscle necrosis within 6-8 hours and potential limb loss. The leg has four compartments, and tibial shaft fractures are the most common cause. Diagnosis is primarily clinical, but pressure measurement confirms equivocal cases. Emergent two-incision four-compartment fasciotomy is the treatment.
Irreversible muscle necrosis begins at 6-8 hours of ischemia.
The sequence of deterioration:
- 2-4 hours: Nerve dysfunction begins (paresthesia, weakness)
- 4-6 hours: Ongoing nerve and muscle damage
- 6-8 hours: Irreversible myonecrosis
- Beyond 8 hours: Volkmann's contracture, rhabdomyolysis, limb loss
If clinical suspicion is high, proceed to fasciotomy - do NOT wait for pressure confirmation.
Etiology and Risk Factors
- Examples
- Tibial shaft (most common), forearm, femoral shaft
- Risk Level
- High
- Examples
- Crush injuries, muscle contusions
- Risk Level
- High
- Examples
- Ischemia-reperfusion after revascularization
- Risk Level
- High
- Examples
- Tight casts, circumferential dressings, positioning
- Risk Level
- Moderate
- Examples
- Anticoagulation, coagulopathy, vascular injury
- Risk Level
- Moderate
- Examples
- Circumferential burns, escharotomy needed
- Risk Level
- Moderate
- Examples
- Snake bites, injection injuries, nephrotic syndrome
- Risk Level
- Lower
A distinct, frequently-litigated leg-specific entity absent from most candidates' answers: acute compartment syndrome of the well (non-operated, dependent) leg after prolonged surgery in the lithotomy or hemilithotomy position - "well-leg compartment syndrome" (WLCS).
- Mechanism: the elevated leg has reduced arterial perfusion pressure (limb elevation lowers local perfusion), compounded by external compression from the leg-holder/calf supports, intra-operative hypotension, and long operative duration - producing ischaemia in a leg that was never injured.
- At-risk operations: femoral or tibial nailing on a fracture/traction table (the contralateral "well" leg in hemilithotomy), and prolonged lithotomy for urological, colorectal and gynaecological surgery.
- Prevention (the examinable list): keep continuous lithotomy/elevation time short (lower the legs intermittently, roughly every 2 hours for long high-risk cases), use well-padded supports avoiding direct calf pressure, avoid sustained intra-operative hypotension, and be cautious with calf compression devices in steep head-down/elevated positions.
- Recognition: maintain a high index of suspicion for pain and tense compartments in the dependent leg in recovery after a long positioning case - and manage exactly as any ACS (urgent fasciotomy).
Exam point: the "well leg" can develop compartment syndrome from prolonged lithotomy positioning - elevation plus leg-holder compression plus hypotension plus time - so prevent it by limiting continuous elevation time and padding the supports.
Anatomy and Pathophysiology
The leg has four fascial compartments, each with specific contents:
- Anterior: Tibialis anterior, EHL, EDL, peroneus tertius, deep peroneal nerve, anterior tibial artery
- Lateral: Peroneus longus, peroneus brevis, superficial peroneal nerve
- Superficial Posterior: Gastrocnemius, soleus, plantaris, sural nerve
- Deep Posterior: Tibialis posterior, FDL, FHL, posterior tibial artery, tibial nerve
The anterior compartment is most commonly affected, but all four must be released.
- Tibialis anterior (foot dorsiflexion)
- Extensor hallucis longus
- Extensor digitorum longus
- Peroneus tertius
- Deep peroneal nerve (first web space)
- Anterior tibial artery
Lateral incision, 2cm lateral to tibial crest
- Peroneus longus
- Peroneus brevis
- Superficial peroneal nerve (foot dorsum)
Lateral incision, same as anterior, posterior incision in fascia
- Gastrocnemius
- Soleus
- Plantaris
- Sural nerve
Medial incision, 2cm posterior to medial tibial border
- Tibialis posterior
- Flexor digitorum longus
- Flexor hallucis longus
- Posterior tibial artery
- Tibial nerve
Detach soleus from tibia to access
Classification Systems
Classification by Clinical Severity:
- Clinical Features
- Pain with stretch, borderline Delta P 25-35
- Management
- Close monitoring, serial assessment every 1-2 hours
- Clinical Features
- Pain out of proportion, tense compartments, Delta P less than 30
- Management
- Immediate fasciotomy within 30-60 minutes
- Clinical Features
- Paralysis, paresthesia, pressure less than 30 Delta P
- Management
- Urgent fasciotomy, consider outcomes discussion
- Clinical Features
- Pulselessness, fixed contracture, sensory loss complete
- Management
- Amputation may be required, fasciotomy contraindicated
The severity grading helps guide urgency and prognosis discussions with patients.
Clinical Assessment
History and Examination
- Mechanism: Tibial fracture, crush, prolonged limb compression
- Time since injury - critical for prognosis
- Pain character: Constant, severe, not relieved by analgesia
- Symptoms: Numbness, tingling, weakness
- Anticoagulation status
- Polytrauma - altered consciousness masks symptoms
- Pain on passive stretch - most sensitive early sign
- Tense, woody compartments on palpation
- Pain out of proportion to injury
- Sensory deficit (first web space = deep peroneal)
- Motor weakness (foot drop = anterior compartment)
- Pulses typically present - don't be reassured
Passive Stretch Testing
- Passive Stretch Test
- Plantarflex foot and toes
- What Worsens Pain
- Stretches tibialis anterior, EDL, EHL
- Passive Stretch Test
- Invert foot
- What Worsens Pain
- Stretches peroneus longus and brevis
- Passive Stretch Test
- Dorsiflex foot
- What Worsens Pain
- Stretches gastrosoleus complex
- Passive Stretch Test
- Extend toes + dorsiflex foot
- What Worsens Pain
- Stretches FDL, FHL, tibialis posterior
Compartment Pressure Measurement
- Equivocal clinical findings
- Unconscious/sedated patient
- Unable to assess clinically (intubated, regional block)
- Borderline symptoms with need for documentation
- Use Stryker device or arterial line transducer
- Measure within 5cm of fracture site (highest pressure zone)
- Measure all four compartments - don't assume which is affected
- Compare to diastolic blood pressure
- Absolute pressure greater than 30mmHg: Traditional threshold
- Delta P less than 30mmHg: More reliable, especially in hypotensive patients
- Absolute greater than 45mmHg: Universally indicates fasciotomy needed
- Pulses - present in most cases of compartment syndrome
- Capillary refill - maintained until very late
- Single pressure reading - may need serial measurements
- "Soft" compartments - deeper compartments may be tense while superficial feels soft
- Obtunded/intubated patients
- Regional anesthesia (masks pain)
- Young males with high pain tolerance
- Those on anticoagulants
- After revascularization
Differential Diagnosis
- Key Distinguishing Features
- Pain out of proportion, pain on passive stretch, tense compartments, pulses usually present
- Discriminator
- Delta P less than 30mmHg; clinical picture
- Key Distinguishing Features
- Absent pulses early, pallor, poikilothermia, paralysis from outset
- Discriminator
- Absent pulses early (vs present in ACS); CT angiography
- Key Distinguishing Features
- Diffuse calf swelling, tenderness, no passive-stretch pain, gradual onset
- Discriminator
- Doppler ultrasound; absence of woody compartments
- Key Distinguishing Features
- Erythema, warmth, fever, systemic upset, no passive-stretch pain
- Discriminator
- Skin changes; inflammatory markers
- Key Distinguishing Features
- Pain out of proportion PLUS systemic sepsis, crepitus, skin necrosis, bullae
- Discriminator
- Systemic toxicity, LRINEC score, surgical exploration
- Key Distinguishing Features
- Pain localised to fracture, relieved by analgesia, soft compartments
- Discriminator
- Pain controlled by opioids; non-tense compartments
Acute limb ischaemia and necrotising fasciitis both share "pain out of proportion." Early absent pulses point to ischaemia (pulses are typically preserved in ACS until very late), while systemic sepsis, crepitus and skin necrosis point to necrotising fasciitis - which mandates urgent surgical debridement, not just fasciotomy.
Investigations
- FBC, UEC, coagulation
- CK (creatine kinase) - rhabdomyolysis
- Lactate
- Group and screen
- ECG (hyperkalemia risk)
- Serial CK post-fasciotomy
- Monitor urine output (myoglobinuria)
- Stryker intracompartmental monitor
- Or arterial line transducer + needle
- Insert perpendicular to compartment
- Within 5cm of fracture site
- Measure all 4 compartments
- Zero at level of compartment
- Delta P = DBP - compartment pressure
- CK (creatine kinase): Often greater than 10,000 U/L (can exceed 100,000)
- Myoglobin: Causes myoglobinuria (cola-colored urine)
- Potassium: Hyperkalemia - cardiac risk
- Creatinine: Rising indicates acute kidney injury
- Lactate: Elevated with tissue ischemia
- Phosphate: Elevated from muscle breakdown
- Aggressive IV fluids (target urine output 200-300mL/hr)
- Monitor for hyperkalemia
- Consider urinary alkalinization
- Avoid nephrotoxins
Management Algorithm
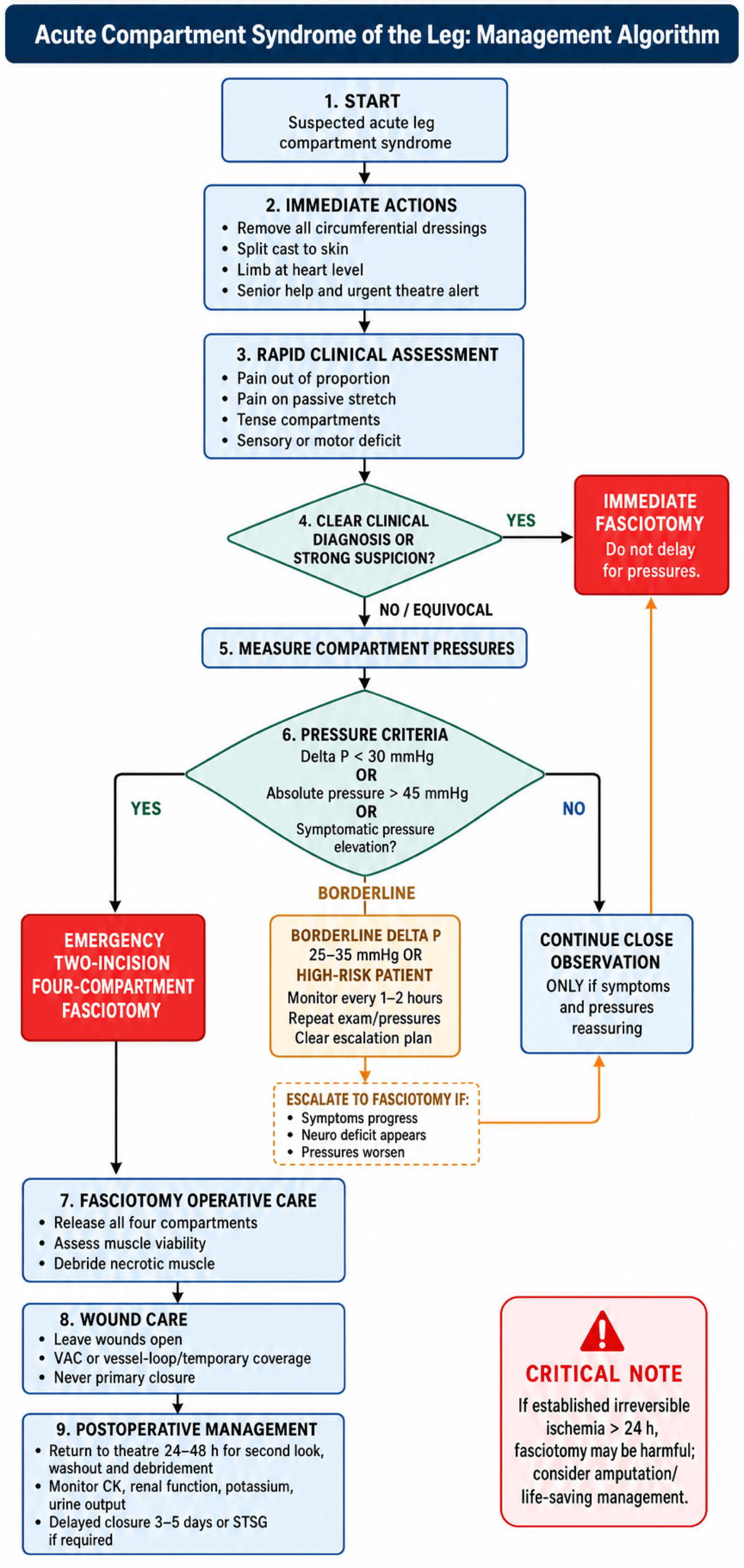
Management
Initial Non-Operative Management:
- Remove ALL circumferential dressings (can reduce pressure 30-65%)
- Split cast to skin
- Keep limb at heart level (elevation may reduce perfusion)
- Call for senior help immediately
- Rapid clinical assessment (pain, passive stretch, sensation)
- If clinical diagnosis clear: proceed directly to theatre
- If equivocal: measure compartment pressures
- Consent for fasciotomy
- Organize theatre urgently
Conservative measures (cast splitting, elevation) are only temporizing while organizing theatre. If compartment syndrome is diagnosed or strongly suspected, fasciotomy is mandatory. Do not rely on conservative measures alone.
Conservative management truly only applies for impending compartment syndrome with borderline Delta P (25-35mmHg). Close monitoring every 1-2 hours with clear escalation plan is essential.
Surgical Technique


Releases: Anterior + Lateral Compartments
- Supine with bump under ipsilateral hip
- Lateral incision 2cm anterior to fibula
- Full length from fibular head to lateral malleolus
- Find intermuscular septum between anterior and lateral compartments
- Identify superficial peroneal nerve in distal third (protect it)
- Incise fascia longitudinally posterior to septum
- Peroneal muscles should bulge
- Pass anterior to intermuscular septum
- Incise anterior compartment fascia longitudinally
- Tibialis anterior and EDL should bulge
- Make incision FULL LENGTH - don't be conservative
- Protect superficial peroneal nerve (crosses in distal third)
- Both compartments released through single incision
- Muscles should bulge and appear pink (viable)
FASCIOTOMY
Two-Incision Four-Compartment Release
Hook:FASCIOTOMY - complete release of all four compartments through two incisions
The two-incision technique above is standard, but the single-incision (lateral parafibular) four-compartment fasciotomy is an examinable alternative.
- Technique: a single long lateral incision over the fibula gives direct access to the anterior and lateral compartments (as in the two-incision lateral approach); the superficial and deep posterior compartments are then reached by developing the plane posterior to the fibula / along the posterior intermuscular septum, releasing them from the lateral side. (The historical fibulectomy fasciotomy - resecting the fibula to decompress all four - is now rarely used.)
- Indications: compromised or unusable medial skin/soft tissue, the need to preserve medial access for vascular reconstruction or a planned free flap, or a single-incision preference to reduce wound burden.
- Caveats: it is technically more demanding and carries a higher risk of incomplete deep posterior release (the most commonly missed compartment) and of injury to the peroneal vessels and superficial peroneal nerve.
Exam point: the single-incision parafibular fasciotomy releases all four compartments from the lateral side and is useful when the medial skin must be preserved, but the two-incision technique remains the standard because complete deep posterior release is more reliably achieved.
Complications
VOLKMANN
Complications of Compartment Syndrome
Hook:VOLKMANN - the devastating consequences of missed compartment syndrome
- Complication
- Rhabdomyolysis
- Prevention/Management
- Aggressive fluids, monitor CK, urine output
- Complication
- Hyperkalemia
- Prevention/Management
- ECG monitoring, calcium gluconate, insulin/dextrose
- Complication
- Acute kidney injury
- Prevention/Management
- IV fluids, avoid nephrotoxins, may need dialysis
- Complication
- Wound infection
- Prevention/Management
- Antibiotics, debridement, VAC therapy
- Complication
- Ongoing muscle necrosis
- Prevention/Management
- Serial debridement until viable tissue
- Complication
- Volkmann's contracture
- Prevention/Management
- Requires tendon lengthening, releases
- Complication
- Permanent nerve damage
- Prevention/Management
- May need tendon transfers
- Complication
- Amputation
- Prevention/Management
- May be required for unsalvageable limb
Definition: Fixed flexion contracture of forearm/leg muscles due to ischemic fibrosis.
- Affected muscles: Deep posterior compartment (FDL, FHL, tibialis posterior)
- Clinical appearance: Claw toes, equinovarus foot
- Pathology: Muscle replaced by fibrous tissue, shortened and contracted
- Mild: Stretching, splinting, physiotherapy
- Moderate: Muscle slide procedures
- Severe: Tendon lengthening, releases
- Very severe: May require amputation
Prevention: Early recognition and fasciotomy - this is the key message.
Medicolegal Considerations
Compartment syndrome is one of the most litigated conditions in orthopaedics. Protect yourself:
- Document baseline neurovascular status - sensation, motor, pulses
- Time-stamp all assessments - shows vigilant monitoring
- Document clinical findings - "pain with passive stretch," "tense compartments"
- Record all interventions - cast splitting, elevation, pressure measurements
- Document discussions with patient/family about risks
- If pressures measured - record actual values and Delta P calculation
- If proceeding to surgery - document indication clearly
- Consent: Include amputation as a possible outcome if delayed presentation
Postoperative Care
First 48 Hours Post-Fasciotomy:
- Serial CK levels (every 6-12 hours)
- Urine output monitoring (target greater than 1mL/kg/hr)
- Renal function (creatinine, urea)
- Potassium levels (hyperkalemia risk)
- ECG monitoring if hyperkalemia concerns
- Limb neurovascular checks
- Aggressive IV fluids - aim for urine output 200-300mL/hr
- Consider urinary alkalinization (target urine pH greater than 6.5)
- Avoid nephrotoxic medications
- DVT prophylaxis
- Analgesia optimization
- Consider ICU admission if significant rhabdomyolysis
Return to Theatre at 24-48 Hours:
- Mandatory second look
- Debride any further necrotic muscle
- Assess wound for closure readiness
- Washout
Adequate systemic resuscitation is critical to prevent acute kidney injury from rhabdomyolysis.
Outcomes and Prognosis
- Expected Outcome
- Full recovery expected
- Prognosis
- Excellent - near-normal function
- Expected Outcome
- Variable - some deficit possible
- Prognosis
- Good - most regain function with some residual
- Expected Outcome
- Significant deficit likely
- Prognosis
- Fair - permanent weakness/sensory loss common
- Expected Outcome
- Poor - Volkmann's/amputation
- Prognosis
- Poor - limb salvage may not be possible
Prognostic Factors
- Early diagnosis (less than 6 hours)
- Prompt complete fasciotomy
- Single compartment involvement
- Young, healthy patient
- Isolated injury
- Good systemic perfusion
- Delayed diagnosis (greater than 12 hours)
- Incomplete fasciotomy
- Multiple compartment involvement
- Associated vascular injury
- Polytrauma/hypotension
- Significant rhabdomyolysis
- Deep posterior compartment involvement
- 80-90% achieve satisfactory functional outcome
- Chronic pain in 10-15%
- Sensory disturbance in 15-20%
- Motor weakness in 10-15%
- Cosmetic concerns from scars in 20-30%
- 50% or more have significant functional limitation
- High rate of chronic pain
- Volkmann's contracture in 10-30%
- Amputation rate increases significantly
Guidelines, Registries & Global Practice
Global Epidemiology
- Overall annual incidence approximately 7.3/100,000 (males) and 0.7/100,000 (females)
- 2-11.5% of tibial diaphyseal fractures develop ACS (11.5% in the large Edinburgh cohort)
- Youth is the strongest risk factor - peak in the 12-29 year age range
- Male predominance roughly 10:1
- High-energy mechanisms (road traffic, sport, crush) dominate worldwide
- Rural / remote settings: longer transfer times mean fasciotomy may need to be performed locally before transfer rather than awaiting referral
- Limited-resource settings: pressure-monitoring devices (Stryker) may be unavailable - reliance on serial clinical assessment and arterial-line transduction
- Later presentation in regions with restricted access increases rates of established necrosis and amputation
Guidelines Compared Side by Side
- Diagnosis
- Primarily clinical; document serial neurovascular obs; high index of suspicion
- Threshold / Emphasis
- Delta P less than 30mmHg supports decompression; fasciotomy without delay
- Diagnosis
- Clinical assessment plus Delta P; continuous monitoring in unassessable patients
- Threshold / Emphasis
- Two-incision four-compartment release; wounds left open
- Diagnosis
- Clinical signs unreliable in isolation; consider monitoring in at-risk/obtunded
- Threshold / Emphasis
- Delta P less than 30mmHg; do not delay for confirmatory tests
- Diagnosis
- Clinical diagnosis remains gold standard; pressure adjunctive
- Threshold / Emphasis
- Emphasis on time-to-fasciotomy as the key modifiable outcome driver
There is broad international convergence: diagnosis is clinical, Delta P less than 30mmHg is the favoured objective threshold, and the decisive variable is time to decompression. No major society endorses an absolute-pressure-only rule.
Registry and System-Level Notes
- ACS is a recognised never-event / serious-incident trigger in many national systems; missed or delayed cases are commonly audited.
- Unlike arthroplasty, there is no dedicated international ACS registry; outcome data come from trauma databases (e.g. large single-unit cohorts such as Edinburgh) rather than implant registries.
- Health systems increasingly mandate structured neurovascular observation charts with explicit escalation triggers for at-risk limbs.
Antibiotic and Supportive Care (Principles, not Brands)
- Open fasciotomy / open fracture wounds: first-generation cephalosporin (e.g. cefazolin) as per local antimicrobial guidance; add gram-negative/anaerobic cover for heavily contaminated wounds; clindamycin if penicillin-allergic.
- Rhabdomyolysis: aggressive crystalloid resuscitation, monitor potassium and creatine kinase, treat hyperkalaemia (calcium, insulin-dextrose, salbutamol).
- Always follow local/national antimicrobial stewardship guidelines - agents and durations vary by region and resistance patterns.
Controversies and Areas of Uncertainty
Delta P (less than 30mmHg) is the most widely endorsed threshold, but the supporting evidence (McQueen 1996) is observational with very few true ACS cases. Some still use absolute thresholds (over 30 or over 45mmHg). No randomised trial defines the optimal cut-off.
Continuous Delta P monitoring shortens delay to fasciotomy but may also drive unnecessary fasciotomies in patients whose pressures would have settled. Whether to monitor all high-risk tibial fractures or only the unassessable is debated.
A single pressure measurement can be falsely low or high (wrong compartment, distance from fracture, technique). Many advocate trend-based or continuous data rather than acting on one number.
Near-infrared spectroscopy and serum biomarkers (e.g. CK trends) are investigational. None has replaced clinical assessment plus Delta P, and they are not standard of care globally.
State the mainstream position first (clinical diagnosis; Delta P less than 30mmHg drives the decision; if in doubt, decompress), then acknowledge the uncertainty (weak evidence base, risk of over-treatment with continuous monitoring). Examiners reward a safe default with awareness of nuance, not dogmatism.
MCQ Practice Points
- 6-8 hours: Window before irreversible necrosis
- Delta P less than 30mmHg: Threshold for fasciotomy
- 45 mmHg absolute: Universal indication for surgery
- 2-9%: Incidence with tibial fractures
- 4: Number of leg compartments
- 2: Number of incisions needed
- 30-65%: Pressure reduction with cast splitting
- 3-5 days: Delayed closure timing
- 10:1: Male:female ratio
- 36%: Missed in polytrauma patients
- Pulses present - doesn't exclude compartment syndrome
- Pain is the earliest sign - not paralysis or pulselessness
- All 4 compartments - must release all, not just anterior
- Delta P not absolute pressure - use perfusion-based threshold
- Don't close wounds - leave open for 3-5 days
- Passive stretch - most sensitive clinical test
- Anterior compartment - most commonly affected
- Deep peroneal nerve - first web space sensation
Q: What is the Delta P threshold for fasciotomy in compartment syndrome?
A: Delta P less than 30mmHg (diastolic BP minus compartment pressure). This is more reliable than absolute thresholds (30-40mmHg) as it accounts for patient's perfusion pressure.
Q: What are the early vs late clinical features of compartment syndrome?
A: Early (6 Ps in order): Pain out of proportion, Pressure (tense compartments), Pain with passive stretch, Paresthesia. Late (irreversible): Paralysis, Pulselessness. The key is that pulses are preserved until very late - don't wait for pulselessness!
Q: How many incisions are required for complete four-compartment fasciotomy of the leg?
A: Two incisions: (1) Lateral incision 2cm anterior to fibula for anterior and lateral compartments; (2) Medial incision 2cm posterior to tibial border for superficial and deep posterior compartments. Wounds are left open with delayed closure at 3-5 days.
Q: How do you access the deep posterior compartment during medial fasciotomy?
A: Detach the soleus muscle origin from the posterior tibial border. This exposes the fascia of the deep posterior compartment, which contains tibialis posterior, FDL, FHL, and the posterior tibial neurovascular bundle.
Q: Which nerve territories should be tested to assess compartment involvement?
A: First web space (deep peroneal nerve - anterior compartment), dorsum of foot (superficial peroneal nerve - lateral compartment), plantar foot (tibial nerve - deep posterior compartment), and lateral foot (sural nerve - superficial posterior).
At a Glance
- Key Information
- Elevated pressure in closed fascial space compromising tissue perfusion
- Key Information
- 2-9% of tibial fractures; 7.3/100,000 annual
- Key Information
- Male:Female 10:1; Peak age 20-35 years
- Key Information
- Tibial shaft fractures
- Key Information
- 6-8 hours of ischemia = irreversible
- Key Information
- CLINICAL - pain on passive stretch, tense compartments
- Key Information
- Delta P less than 30mmHg (DBP - compartment pressure)
- Key Information
- Emergent two-incision, four-compartment fasciotomy
- Key Information
- Delayed primary closure at 3-5 days or STSG
- Tibial fractures - 2-9% incidence
- Male: Female = 10:1
- Peak age: 20-35 years
- 36% missed in polytrauma patients
- Annual incidence: 7.3/100,000
- Tibial shaft fractures - most common
- High-energy trauma
- Crush injuries
- Ischemia-reperfusion after revascularization
- Tight casts/dressings
- Anticoagulation - lowers threshold
- Clinical diagnosis - don't delay for pressures
- Pain with passive stretch - most sensitive
- Pulses present in most cases
- Time is muscle - fascia always wins
- Document neurological status pre-op
- Delayed closure or STSG at 3-5 days
PPPPPP6 P's
Classic Signs (LATE findings)
Hook:Pain and Pressure are early - the other 4 P's mean you're too late!
COMPARTMENTS
Four Leg Compartments and Contents
Hook:COMPARTMENTS - remember all four need release through two incisions
STRETCH
Clinical Assessment Approach
Hook:STRETCH the muscles to test for compartment syndrome
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old male has a tibial shaft fracture from a motorcycle accident. Six hours post-nailing, the nurse calls you because he's requiring increasing morphine and complaining of severe leg pain.”
“You're performing a fasciotomy for compartment syndrome.”
“A patient presents 24 hours after a tibial fracture with an obviously dead limb - no pulses, fixed claw toes, insensate. The registrar asks whether to do a fasciotomy.”
“You're discussing compartment syndrome risk with a junior registrar.”
Evidence Base
McQueen et al. (1996) - Continuous Pressure Monitoring
- Continuous pressure monitoring in 116 tibial fractures.
- Delta P less than 30mmHg was the optimal threshold for fasciotomy indication.
- Absolute pressure greater than 30mmHg or greater than 45mmHg led to unnecessary fasciotomies.
Whitesides et al. (1975) - Tissue Perfusion
- Tissue pressure measurements as a determinant for the need of fasciotomy.
- Perfusion pressure = DBP - Intracompartmental Pressure.
- Recommended fasciotomy when tissue pressure rose to within 10-30 mmHg of DBP.
Ulmer (2002) - Clinical Findings Predictive Value
- Sens (13-19%) and PPV (11-15%) of clinical signs are POOR.
- Possibility of ACS increases with number of signs present.
- Pain on passive stretch is the most sensitive clinical finding.
McQueen (1998) - Continuous Monitoring Halves Delay
- Largest causal group is tibial diaphyseal fracture, then soft-tissue injury, crush, distal radius and forearm fractures.
- Clinical signs (pain, stretch pain, neurology) are inconstant; continuous monitoring is recommended in at-risk patients.
- Using a Delta P less than 30mmHg threshold with monitoring halved the delay to fasciotomy and reduced late complications.