O'Driscoll Classification | Elbow Stability Keystone | Terrible Triad Component
- Coronoid is the anterior buttress - prevents posterior subluxation
- Over 50% height = unstable - requires operative fixation
- Terrible triad component - dislocation + radial head + coronoid
- Anteromedial facet fractures are often varus-posteromedial pattern
- Never ignore - instability leads to poor outcomes
- “Anteromedial facet fractures have different mechanism - varus stress, not dislocation
- “Coronoid tip fractures in terrible triad may need fixation despite small size
- “Basal fractures always unstable - include brachialis insertion
- “Sublime tubercle involvement means MCL attachment disrupted
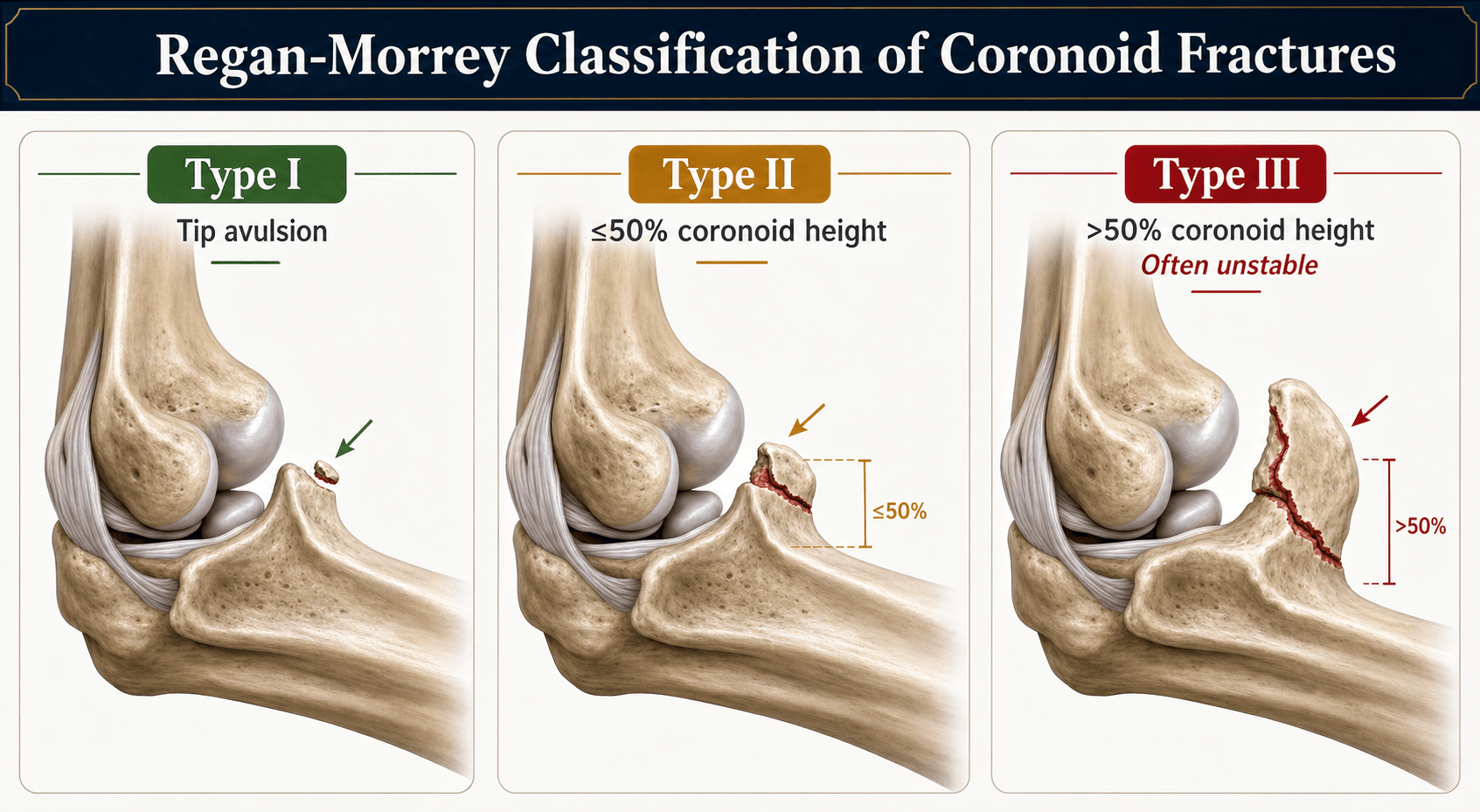
Coronoid is the anterior buttress of the elbow. It resists posterior displacement of the ulna. Loss of over 50% height = elbow instability. Must reconstruct for stability.
Tip fractures (Type I) often with posterolateral dislocation. Anteromedial facet (Type II) with varus-posteromedial instability. Basal (Type III) always unstable.
75%+ occur with elbow dislocation. Part of terrible triad (with radial head fracture, LCL). May have isolated anteromedial pattern with MCL injury.
Fix coronoid to restore stability. Options include suture lasso, screw fixation, or plate buttress. Approach depends on pattern - lateral vs medial.
- Key Finding
- Elbow stable after reduction
- Treatment
- Treat associated injuries, no coronoid fixation
- Key Finding
- Part of terrible triad, persistent instability
- Treatment
- Consider suture lasso fixation
- Key Finding
- Subtype 1, less than 50% of facet
- Treatment
- May be stable - assess carefully
- Key Finding
- Subtype 2-3, medial instability
- Treatment
- Buttress plate via medial approach
- Key Finding
- Always unstable, over 50% height
- Treatment
- Plate fixation mandatory
- Key Finding
- MCL attachment involved
- Treatment
- Fix fragment = fixes MCL insertion
Overview and Epidemiology
Coronoid fractures are typically associated with elbow instability. Isolated coronoid fractures are rare; most occur with elbow dislocation or other fracture patterns. The coronoid is a critical structure for elbow stability.
Mechanism of injury:
- Posterolateral dislocation - most common (Type I tip fractures)
- Elbow dislocates, shearing off the coronoid tip
- Part of terrible triad pattern
- Varus-posteromedial rotational instability (Type II anteromedial)
- Axial load with varus stress
- Different mechanism from posterolateral dislocation
- High-energy direct trauma (Type III basal)
- Significant force through ulnohumeral joint
Tip fractures occur with posterolateral dislocation - the coronoid is sheared off as the elbow dislocates. Anteromedial facet fractures occur with varus stress without dislocation - a distinct mechanism and injury pattern requiring different treatment approach.
Associated injuries:
- Elbow dislocation (75%+)
- Radial head fracture (terrible triad)
- LCL complex rupture (always with dislocation)
- MCL rupture (with anteromedial facet fractures)
- Olecranon fracture (transolecranon pattern)
Anatomy and Biomechanics
Coronoid anatomy:
- Anterior projection of the proximal ulna
- Forms anterior buttress of the greater sigmoid notch
- Tip is attachment of anterior capsule
- Sublime tubercle - medial aspect, MCL (anterior bundle) attachment
- Brachialis insertion - on anterior surface of coronoid base
Key anatomical relationships:
- Anterior capsule attaches to tip
- MCL anterior bundle attaches to sublime tubercle
- Brachialis attaches across base
- Lateral facet articulates with radial head via radioulnar joint
Biomechanical function:
The coronoid provides the primary anterior buttress against posterior subluxation. Loss of more than 50% of coronoid height results in significant elbow instability. Even smaller fractures can contribute to instability in the presence of ligamentous injury.
- Primary constraint to posterior translation (with olecranon)
- Secondary valgus stabilizer (with MCL and radial head)
- Works with radial head to resist axial loading
- Loss of over 50% of coronoid height = unstable elbow
- Applies to sagittal plane (anterior-posterior height)
- Even smaller fractures may be unstable with ligament injuries
Classification Systems
O'Driscoll Classification (most commonly used)
- Subtype
- Tip
- Description
- Tip fracture (less than 2mm)
- Mechanism
- Posterolateral dislocation
- Subtype
- 1
- Description
- Sublime tubercle (medial)
- Mechanism
- Varus-posteromedial
- Subtype
- 2
- Description
- Anteromedial rim
- Mechanism
- Varus-posteromedial
- Subtype
- 3
- Description
- Anteromedial rim + tip
- Mechanism
- Varus-posteromedial
- Subtype
- 1
- Description
- Basal - less than 50%
- Mechanism
- High energy
- Subtype
- 2
- Description
- Basal - more than 50%
- Mechanism
- High energy
Type II anteromedial facet fractures have a different mechanism than Type I tip fractures. They result from varus-posteromedial rotational instability, not posterolateral dislocation. This affects both approach and treatment strategy.
The "Associated Patterns" above list terrible triad, varus posteromedial rotatory instability and transolecranon fracture-dislocation - but a coronoid fracture is also a hallmark of the posterior Monteggia lesion (Bado type II), and missing this changes the whole reconstruction:
- Pattern: a proximal ulna fracture with posterior dislocation of the radial head, frequently accompanied by a coronoid fracture and a radial head fracture. In Jupiter's sub-classification of Bado II, the type IIA lesion is defined by a fracture at the level of the coronoid/distal trochlear notch - so the coronoid is integral to this pattern, not incidental.
- Why it matters: unlike the terrible triad (a pure dislocation pattern) or varus PMRI (a coronoid + LCL pattern), the posterior Monteggia is fundamentally a proximal-ulna malalignment problem. The priority is anatomical reconstruction of the proximal ulna (restoring length, alignment and the trochlear notch with a contoured dorsal plate); the coronoid fragment must be captured as part of that construct, and only then is the radiocapitellar joint reduced.
- The trap: treating an apparent isolated "coronoid + radial head fracture" as a terrible triad and approaching it from the lateral side alone will miss the posterior ulnar malalignment and lead to recurrent posterior instability and arthrosis. Older patients with osteoporotic comminution at the notch do worst.
Exam point: a coronoid fracture with a posteriorly dislocated radial head and a proximal ulna fracture is a posterior Monteggia (Bado II/Jupiter IIA), not a terrible triad - reconstruct the proximal ulna first, then the radiocapitellar joint.
Clinical Assessment
History:
- Mechanism (fall, direction of force)
- Any sense of instability or dislocation
- Whether elbow was relocated (self-reduced or reduced)
- Previous elbow problems
- Hand dominance, occupation
Physical examination:
- Significance
- Intra-articular injury
- Action
- X-ray, CT if fracture suspected
- Significance
- Coronoid/anteromedial facet
- Action
- CT for classification
- Significance
- MCL injury
- Action
- Consider sublime tubercle involvement
- Significance
- LCL injury
- Action
- May have anteromedial facet pattern
- Significance
- PLRI pattern
- Action
- Likely had posterolateral dislocation
- Significance
- Multiple structure involvement
- Action
- Urgent surgical planning
Stability testing:
Posterolateral rotational instability (PLRI): Elbow subluxes posterolaterally - associated with tip fractures. Varus-posteromedial instability: Ulna rotates posteromedially - associated with anteromedial facet fractures. Different patterns require different approaches.
Key examination points:
- Range of motion - assess for mechanical block
- Valgus stress test - MCL integrity
- Varus stress test - LCL integrity
- Posterolateral rotatory instability test - pivot shift
- Neurovascular status - especially ulnar nerve
Differential diagnosis:
- Distinguishing features
- Anterior elbow pain, effusion, often part of dislocation; subtle on plain films
- Key discriminator
- Loss of triangular coronoid projection on lateral X-ray; confirm and type on CT
- Distinguishing features
- History of dislocation, gross instability, radial head fracture
- Key discriminator
- All three components present - LCL ruptured by definition
- Distinguishing features
- Lateral pain, painful rotation, no posteromedial tenderness
- Key discriminator
- Coronoid intact on CT; elbow stable through arc
- Distinguishing features
- Posterior wound/pain, large coronoid fragment, dorsal ulna disrupted
- Key discriminator
- Trochlear notch incongruity; ulnohumeral relationship lost through fracture
- Distinguishing features
- Dislocation that reduces and stays stable, no fracture
- Key discriminator
- No bony fragment on CT - purely capsuloligamentous injury
- Distinguishing features
- Fall onto varus-loaded arm, no frank dislocation, medial joint pain
- Key discriminator
- Anteromedial facet fracture plus LCL avulsion - typically no radial head fracture
- Distinguishing features
- Valgus laxity, medial pain, often in throwing athlete
- Key discriminator
- Bony avulsion at MCL anterior bundle insertion on CT/MRI
Investigations
Radiographic assessment:
Radiographic assessment:
Standard views:
- AP elbow - may see coronoid fracture
- Lateral elbow - best view for coronoid height
- Oblique views - anteromedial facet visualization
On the lateral X-ray, assess coronoid height - the anterior projection of the ulna. Compare to the opposite side if needed. Loss of the normal triangular projection suggests coronoid fracture.
- All suspected coronoid fractures
- Classification (O'Driscoll typing)
- Fragment size and displacement assessment
- Surgical planning
- Associated injuries (radial head, olecranon)
- Fragment size (% of coronoid height)
- Fragment location (tip vs anteromedial vs basal)
- Sublime tubercle involvement
- Associated radial head fracture
- Articular step-off
- Helpful for complex patterns
- Surgical planning
- Understanding fragment geometry
- Rarely indicated acutely
- May assess ligamentous structures
- Consider for chronic instability evaluation
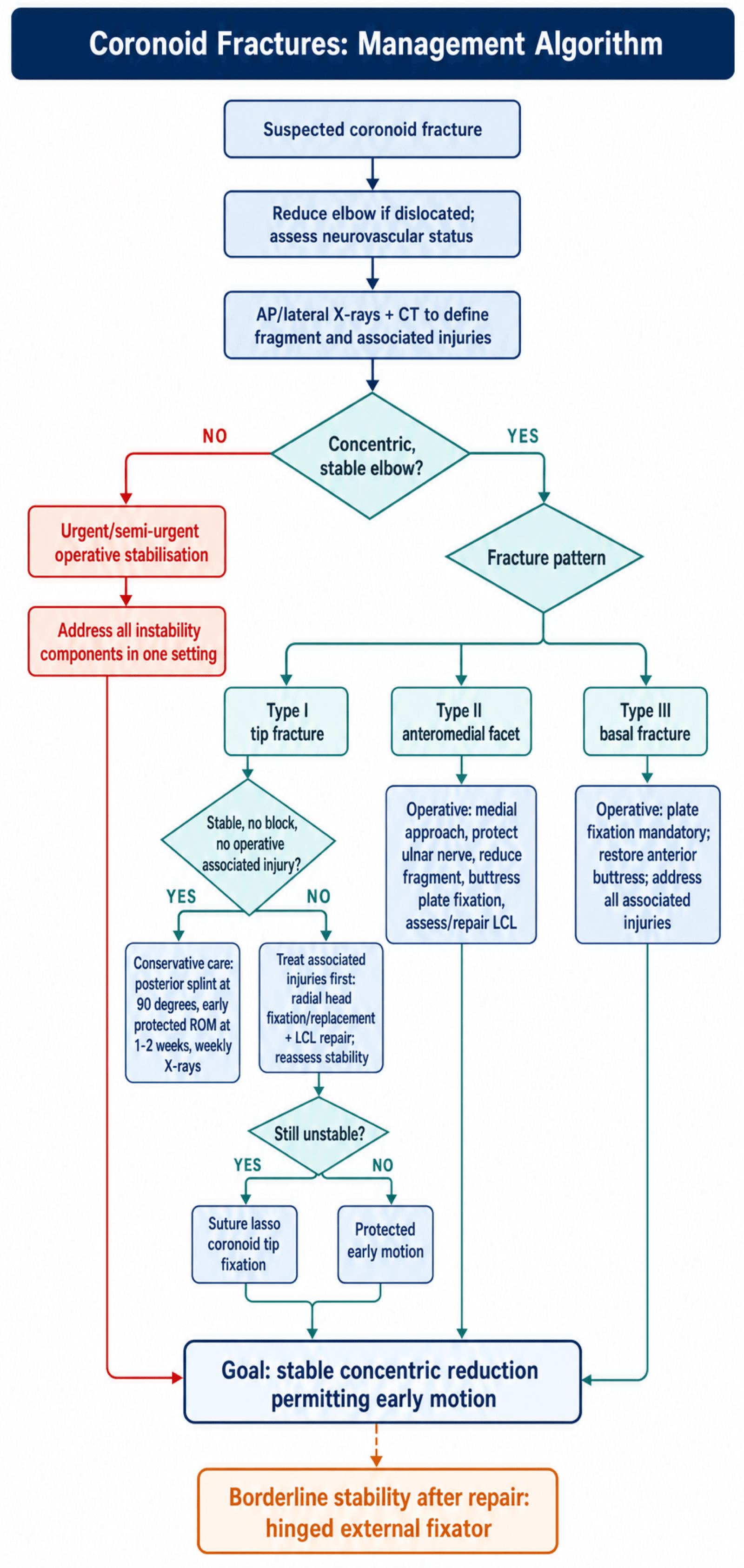
Management Algorithm
Conservative management:
- Type I tip fracture with stable elbow
- Concentric reduction maintained
- No mechanical block
- No associated operative injuries
- Posterior splint at 90 degrees initially
- Begin motion at 1-2 weeks if stable
- Active ROM in flexion-extension arc
- Avoid terminal extension initially
- Progressive motion over 6 weeks
- Weekly X-rays initially
- Assess for subluxation
- Progress motion if maintaining reduction
Conservative management only appropriate for Type I tip fractures with a stable, concentrically reduced elbow. Any instability, incongruency, or associated injuries requiring surgery = fix the coronoid.
Surgical Technique
- Kocher or lateral column approach
- Addresses radial head and LCL
- Can reach coronoid from lateral (over-the-top)
- Suture lasso technique for tip fractures
- FCU splitting or over-the-top of flexor mass
- Identify and protect ulnar nerve
- Direct access to anteromedial facet
- Can also assess/repair MCL
- For transolecranon fracture-dislocations
- Direct visualization through olecranon fracture
- Fix coronoid from posterior
Approach selection depends on fracture pattern and associated injuries.
A favourite viva follow-up is "what if the coronoid is comminuted/non-reconstructable, or the patient presents late with chronic coronoid insufficiency?" Plate/screw/suture-lasso fixation assumes a fixable fragment; when there is no fragment to fix, you reconstruct the anterior buttress:
- Olecranon tip osteoarticular autograft: the most popular reconstruction - the tip of the olecranon is harvested (it is largely expendable for stability) and fixed to the coronoid base with a screw/plate to rebuild the anterior buttress and the trochlear-notch contour.
- Radial head fragment as a graft: when the radial head is being excised/replaced anyway, a suitably sized osteoarticular fragment from the resected head can be repurposed to reconstruct the coronoid - "spare-part" surgery.
- Iliac crest tricortical graft: a structural autograft contoured to the coronoid base, fixed with a screw - useful when no local articular graft is available.
- Other described options: rib osteochondral graft, coronoid prosthesis (rare, salvage), and in chronic cases an allograft proximal ulna for major bone loss.
Indications are an acute unreconstructable (highly comminuted) coronoid and, more often, chronic posttraumatic coronoid insufficiency presenting with persistent or recurrent instability. The goal is always the same: restore enough anterior height to prevent posterior subluxation, then assess stability and add a hinged fixator if borderline.
Exam point: a non-reconstructable or chronically deficient coronoid is reconstructed - olecranon tip osteoarticular autograft is the workhorse, with a resected radial-head fragment or iliac crest as alternatives.
Complications
- Incidence
- 5-15%
- Management
- Revision fixation, ligament repair, hinged fixator
- Incidence
- 20-30%
- Management
- Early motion, physio, capsular release if severe
- Incidence
- 15-25%
- Management
- Activity modification, eventual arthroplasty
- Incidence
- 5-15%
- Management
- Prophylaxis, excision if limiting
- Incidence
- 5-10%
- Management
- Often transient, protect during medial approach
- Incidence
- Variable
- Management
- Hardware removal if symptomatic
- Incidence
- Rare
- Management
- Revision fixation, bone graft
- Most significant complication
- Usually due to inadequate coronoid reconstruction
- Or missed associated injuries
- May require revision surgery, hinged external fixator
- Common with complex elbow trauma
- Prevention: stable fixation, early motion
- Treatment: physiotherapy, dynamic splinting, capsular release
The ulnar nerve is at risk during the medial approach. Options include in-situ protection (preferred for brief procedures) or anterior transposition (for prolonged retraction or if nerve subluxing). Always identify and protect before deep dissection.
Postoperative Care and Rehabilitation
Postoperative protocol:
- Posterior splint at 90 degrees
- Elevation, ice
- Finger motion
- Wound check at 5-7 days
- Begin active ROM if stable fixation
- May use hinged brace if borderline stable
- Focus on flexion-extension
- Avoid varus/valgus stress
- Progressive active ROM
- Target functional ROM by 6 weeks
- No resistance until 6 weeks
- Dynamic splinting if stiff
- Begin gentle strengthening
- Progressive loading
- Return to light activities
- Full strengthening
- Return to sport/work
- Final outcome assessment
Key rehabilitation principles:
- Early motion critical to prevent stiffness
- Stable fixation allows early motion
- If stability borderline - hinged external fixator
- Avoid varus/valgus stress early
- May need extension block initially
If the elbow remains borderline unstable after addressing all injured structures, a hinged external fixator allows early motion while protecting the repair. It centers rotation at the elbow axis and prevents subluxation during rehabilitation.
Outcomes and Prognosis
Outcomes by pattern:
- Good/Excellent
- 80-90%
- Key Factors
- Stable reduction critical
- Good/Excellent
- 70-80%
- Key Factors
- Address all components
- Good/Excellent
- 70-80%
- Key Factors
- Adequate buttress fixation
- Good/Excellent
- 60-75%
- Key Factors
- High energy, complex
Prognostic factors:
- Associated injuries (worse with complex patterns)
- Quality of reconstruction
- Time to surgery
- Patient compliance
- Pre-existing elbow conditions
Terrible triad injuries have worse outcomes than isolated coronoid fractures. Despite addressing all three components (radial head, coronoid, LCL), expect higher rates of stiffness and residual instability. Counsel patients about guarded prognosis.
Guidelines, Registries & Global Practice
Global epidemiology. Isolated coronoid fractures are rare; the coronoid is fractured almost exclusively as part of a complex injury pattern. Across consecutive surgical series, the fragment morphology tracks the instability pattern — small transverse tip fractures with terrible-triad injuries, larger fractures with olecranon fracture-dislocations, and anteromedial facet fractures with varus posteromedial rotational instability (Doornberg & Ring, J Hand Surg Am 2006; PMID 16443103). The anteromedial facet is anatomically vulnerable: 3D-CT analysis shows that on average 58% of the facet (range 26-82%) is unsupported by the proximal ulnar metaphysis, explaining why it so often shears off as a discrete fragment (Doornberg et al., J Shoulder Elbow Surg 2007; PMID 17512221). High-energy mechanisms (motorcycle and vehicle trauma, falls from height, occupational falls) predominate for basal patterns, whereas low-energy varus-loading falls produce anteromedial facet injuries.
Guideline & society position (side-by-side). No registry tracks coronoid fractures specifically, and there is no randomised-trial-level guideline; practice is governed by classification-led expert consensus and instructional teaching from the major societies.
- Region
- USA / global
- Position on coronoid fractures
- Pattern-based fixation; restore the anterior buttress; fix coronoid within the terrible-triad sequence after radial head and LCL
- Evidence level
- Expert consensus (Level V)
- Region
- UK
- Position on coronoid fractures
- Complex fracture-dislocations to be managed at units with elbow/upper-limb expertise; early definitive surgery, early mobilisation
- Evidence level
- Consensus standard
- Region
- Europe
- Position on coronoid fractures
- Endorse O'Driscoll typing; anteromedial facet via medial approach with buttress plate; hinged fixator for residual instability
- Evidence level
- Expert consensus (Level V)
- Region
- UK
- Position on coronoid fractures
- Covered under general non-complex/complex fracture pathways; no disease-specific recommendation
- Evidence level
- Not addressed
Registry evidence. Coronoid fractures are not separately captured in arthroplasty or trauma registries (AOANJRR, NJR, AJRR record joint replacement, not elbow fracture fixation), so the evidence base is series- and meta-analysis-driven rather than registry-driven. The best pooled data come from systematic reviews of the terrible triad: comparable functional scores for radial head repair versus replacement (mean MEPS ~88), with an overall complication rate near 65% and reoperation rates of roughly 18% in both groups (Kyriacou et al., Arch Orthop Trauma Surg 2019; PMID 30656475).
Practice variation. Surgical approach is the main area of genuine variation. A meta-analysis found that a combined lateral and anteromedial approach gave significantly greater elbow and forearm motion and a higher MEPS than a lateral-only approach for the terrible triad, at the cost of longer operative time (Meena et al., Bull Emerg Trauma 2020; PMID 32201696). Choice of radial head reconstruction versus replacement, routine versus selective coronoid fixation in tip fractures, and threshold for hinged external fixation differ between centres and surgeon experience.
Be prepared to discuss coronoid classification, recognise the difference between tip and anteromedial facet patterns, understand the sublime tubercle anatomy, and know when plate fixation versus suture lasso is appropriate. Examiners also probe why there is no registry or RCT-level guidance and how you reconcile the high complication rates reported in meta-analyses with the need for early motion. These are common viva topics.
Key Mnemonics for Exam Recall
DRISCOLLO'DRISCOLL - Classification Framework
Hook:O'Driscoll described it - Types go from tip to base with increasing instability
BUTTRESSBUTTRESS - Coronoid Function
Hook:The coronoid BUTTRESS prevents posterior subluxation
SUBLIMESUBLIME - Tubercle Anatomy
Hook:SUBLIME tubercle = MCL insertion - fixing it = fixing the MCL
TRIADTRIAD - Terrible Triad Management
Hook:The TERRIBLE TRIAD requires addressing all three components systematically
MCQ Practice Points
Q: What defines an O'Driscoll Type II coronoid fracture? A: Anteromedial facet fracture - includes subtypes involving the sublime tubercle (MCL insertion), anteromedial rim, or combination. This pattern results from varus-posteromedial rotational instability, not posterolateral dislocation.
Q: What percentage of coronoid height loss results in elbow instability? A: Greater than 50%. Basal fractures (O'Driscoll Type III) involving more than 50% of coronoid height are always unstable and require operative fixation.
Q: What structure attaches to the sublime tubercle? A: The MCL (specifically the anterior bundle). The sublime tubercle is the ulnar insertion of the most important stabilizing bundle of the MCL. Fractures involving this area are essentially bony MCL avulsions.
Q: What is the mechanism of anteromedial facet fractures? A: Varus-posteromedial rotational instability - an axial load with varus stress, NOT posterolateral dislocation. This is distinct from tip fractures which occur with posterolateral dislocation.
Q: What approach is required for anteromedial facet fracture fixation? A: Medial approach (FCU splitting or over-the-top). These fractures cannot be adequately visualized or fixed from a lateral approach. Must protect the ulnar nerve.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old woman falls from a ladder. Her elbow was dislocated and has been reduced. CT shows a comminuted radial head fracture with more than 4 fragments and a small coronoid tip fracture. How do you approach this injury?”
“A 38-year-old man presents after a fall onto his arm. He has no history of dislocation. CT shows an anteromedial facet fracture involving approximately 40% of the coronoid with the sublime tubercle involved. What is your diagnosis and management approach?”
“A 52-year-old man involved in a motorcycle accident has a complex elbow injury. CT shows a basal coronoid fracture involving approximately 60% of the coronoid height. The elbow is grossly unstable. What are your key considerations?”
O'DRISCOLL CLASSIFICATION
- Type I: Tip fracture - posterolateral dislocation mechanism
- Type II: Anteromedial facet - varus-posteromedial mechanism
- Type III: Basal - over 50% height, always unstable
- Subtypes: I.1/I.2, II.1/II.2/II.3, III.1/III.2 by fragment size
KEY ANATOMY
- Coronoid = anterior buttress of elbow
- Sublime tubercle = MCL (anterior bundle) insertion
- Brachialis inserts on coronoid base
- Over 50% height loss = unstable
PATTERN RECOGNITION
- Type I tip - part of terrible triad (posterolateral dislocation)
- Type II anteromedial - varus stress mechanism, different approach needed
- Type III basal - always operative, plate fixation
- Isolated Type I can be treated conservatively if elbow stable
SURGICAL APPROACHES
- Tip fractures - lateral approach, suture lasso
- Anteromedial facet - MEDIAL approach, buttress plate
- Basal - medial or posterior, plate fixation
- Protect ulnar nerve on medial approach
FIXATION TECHNIQUES
- Suture lasso - for tip fractures (Type I)
- Screws - for larger single fragments
- Buttress plate - for anteromedial facet (Type II)
- Plate - mandatory for basal (Type III)
TERRIBLE TRIAD PROTOCOL
- 1. Fix/replace radial head
- 2. Repair LCL
- 3. Assess stability - fix coronoid if unstable
- 4. Consider hinged fixator if still borderline
Evidence Base
- Defined the coronoid classification by fracture location — tip, anteromedial facet, and basal (body) — and recognised anteromedial facet fractures as varus posteromedial rotatory fracture-subluxations rather than dislocation-driven injuries. These patterns predict associated injuries, instability and surgical approach.
- In 67 surgically treated coronoid fractures, fracture morphology was strongly associated with the instability pattern: large coronoid fractures with olecranon fracture-dislocations, small transverse tip fractures with terrible-triad injuries, and anteromedial facet fractures with varus posteromedial rotational instability (statistically significant for both classification systems).
- 18 anteromedial facet fractures: all but three had avulsion of the LCL complex from the lateral epicondyle. Six elbows in which the facet was not specifically treated (or lost fixation) developed varus subluxation and arthrosis with fair/poor results; secure medial buttress fixation restored good or excellent function in the remainder.
- 42 terrible-triad elbows treated by a modified Pugh standard protocol (radial head fixation/replacement, LCL repair, coronoid fixation when indicated) achieved a mean Mayo Elbow Performance Score of 88, mean flexion-extension arc of 107 degrees, and 24 excellent plus 16 good results; complications included heterotopic ossification (n=5) and transient nerve palsies, with four reoperations.
- 13 patients with persistent ulnohumeral instability after elbow fracture-dislocation treated with a protocol of coronoid and radiocapitellar restoration, LCL repair/reconstruction and temporary hinged external fixation regained stability in every case (mean Mayo score 84, mean motion arc 99 degrees), though arthrosis was common.
- 9 studies, 210 patients: no significant difference in mean MEPS (replacement 88.6 vs reconstruction 88.5) or range of motion. The overall complication rate was 65% and reoperation rates were high in both groups (replacement 18.4%, reconstruction 17.9%).