Posterolateral Most Common | LCL Always Injured | Early Motion Essential
- Posterolateral is the most common direction (90%)
- LCL complex always injured - primary lateral restraint
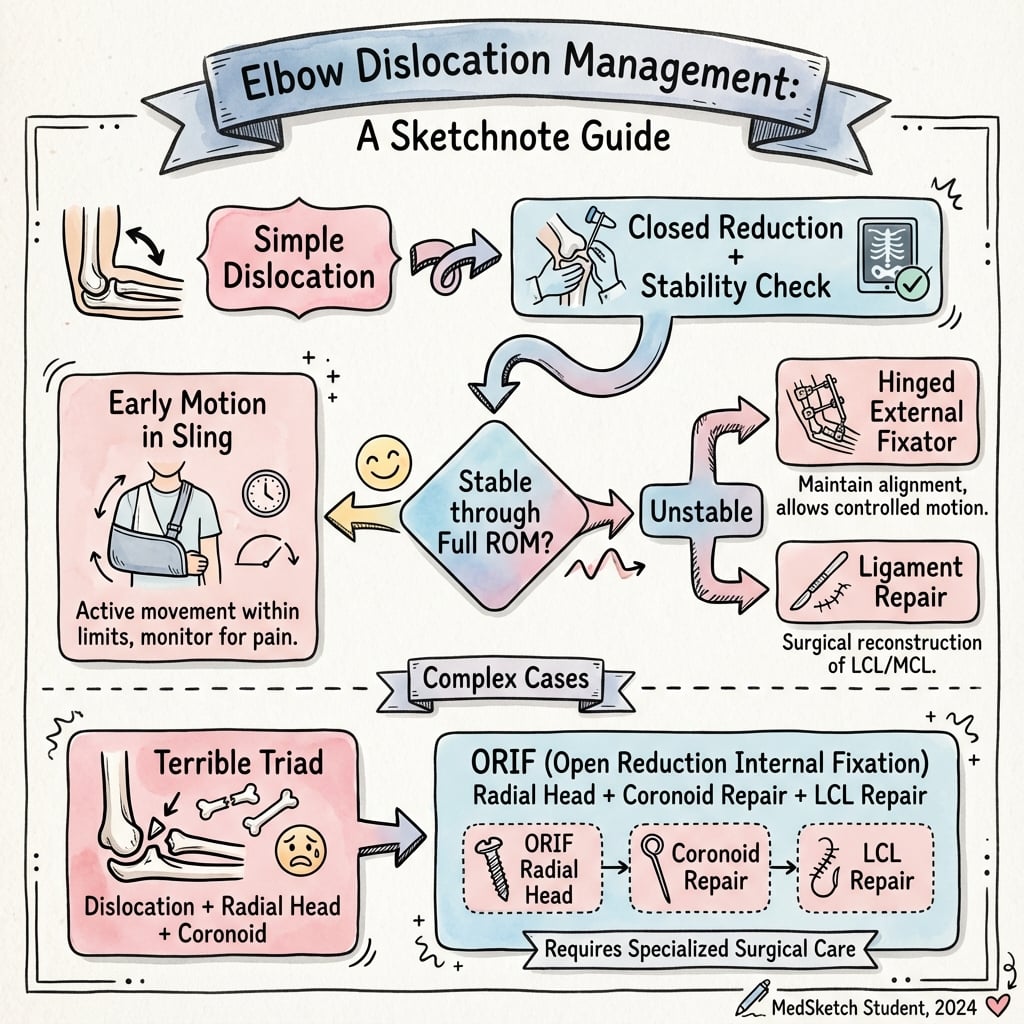
- Simple dislocations usually stable after reduction
- Complex patterns - terrible triad, coronoid, Monteggia variant
- Early motion is essential to prevent stiffness
- “LCL fails first, then anterior capsule, then MCL (outside-to-inside pattern)
- “Simple dislocations: if stable through 30-130° = non-operative
- “Check for associated fractures - radial head, coronoid are commonly missed
- “PLRI (posterolateral rotatory instability) is chronic sequela of LCL injury

Simple = no fracture, ligament injury only. Typically stable after reduction with early motion. Complex = with fracture(s), includes terrible triad, requires addressing all structures.
Soft tissue disruption pattern: LCL complex fails first (Stage 1), then anterior/posterior capsule (Stage 2), then MCL (Stage 3). Understanding this helps guide treatment.
After reduction, test stability under fluoro. Stable through 30-130° arc = non-operative. If redislocates before 60° extension = likely needs surgery.
Stiffness is the enemy. Start motion within 1 week for simple dislocations. Prolonged immobilization leads to contracture. Use hinged brace if stability concerns.
- Key Finding
- Stable after reduction (30-130°)
- Treatment
- Early ROM in hinged brace, non-operative
- Key Finding
- Unstable after reduction
- Treatment
- Consider operative LCL repair
- Key Finding
- Dislocation + radial head + coronoid
- Treatment
- Fix/replace RH, repair LCL, +/- coronoid
- Key Finding
- Mason IV
- Treatment
- Address radial head + ligaments
- Key Finding
- Olecranon impales trochlea
- Treatment
- Reduce carefully, assess for olecranon fracture
- Key Finding
- Radius and ulna separate
- Treatment
- Reduce, high likelihood of instability
- Key Finding
- Unreduced over 3 weeks
- Treatment
- Complex reconstruction required
HORIIHORII - Circle of Instability
Hook:HORII described the circle - injury moves from lateral (outside) to medial (inside)
REDUCEREDUCE - Reduction Steps
Hook:REDUCE the elbow with controlled technique

Overview and Epidemiology
Elbow dislocations are the second most common large joint dislocation after the shoulder. They range from simple ligamentous injuries to complex fracture-dislocations with significant instability.
Mechanism of injury:
- Fall on outstretched hand (FOOSH) - most common
- Axial load with elbow slightly flexed
- Valgus and supination moment
- Creates posterolateral dislocation
- Direct trauma - less common
- Sports injuries - common in young adults
- Motor vehicle accidents - often high-energy, complex patterns
The classic mechanism is a fall on outstretched hand with the elbow in slight flexion. The axial load creates a valgus and supination moment, driving the ulna posterolaterally relative to the humerus. This explains why posterolateral dislocation is most common.
Types:
- Simple (50-60%): No associated fracture, ligament injury only
- Complex (40-50%): With associated fracture(s)
- Terrible triad
- Radial head fracture-dislocation
- Coronoid fracture-dislocation
- Transolecranon fracture-dislocation
Anatomy and Biomechanics
- Ulnohumeral joint: primary elbow stability (hinge)
- Radiocapitellar joint: secondary stabilizer
- Coronoid: anterior buttress of ulnohumeral joint
- Olecranon: posterior buttress
- Trochlea: articulates with greater sigmoid notch
- Lateral ulnar collateral ligament (LUCL) - most important component
- Origin: lateral epicondyle
- Insertion: supinator crest of ulna
- Primary restraint to posterolateral rotatory instability (PLRI)
- Radial collateral ligament (RCL) - blends with annular ligament
- Annular ligament - stabilizes radial head to ulna
- Anterior bundle - most important
- Origin: medial epicondyle
- Insertion: sublime tubercle
- Primary valgus stabilizer
- Posterior bundle - tightens in flexion
- Transverse ligament - minimal contribution
The soft tissue injury in elbow dislocation follows a predictable pattern described by the Horii circle. Disruption proceeds from lateral to medial: Stage 1 (LCL), Stage 2 (anterior/posterior capsule), Stage 3 (MCL). The LCL complex is ALWAYS injured in posterolateral dislocation.
- Stage 1: PLRI - LCL disruption, elbow subluxes posterolaterally
- Stage 2: Incomplete dislocation - capsule disrupted, elbow perches
- Stage 3A: Complete dislocation - MCL posterior bundle torn
- Stage 3B: Gross instability - entire MCL torn (anterior bundle)
- Static: ligaments, bony congruity
- Dynamic: muscles crossing elbow (triceps, biceps, brachialis, flexors/extensors)
Classification Systems
Primary Classification
- Definition
- No fracture, ligament injury only
- Incidence
- 50-60%
- Definition
- With associated fracture(s)
- Incidence
- 40-50%
- Ligamentous injury only
- Usually stable after closed reduction
- Excellent prognosis with early motion
- Fracture + dislocation
- Includes terrible triad, radial head, coronoid patterns
- Usually requires operative treatment
- Higher complication rates
Classification into simple vs complex guides treatment approach and prognosis.
Clinical Presentation and Assessment
History:
- Mechanism of injury
- Any spontaneous reduction
- Previous elbow problems
- Time since injury
- Hand dominance, occupation
Physical examination:
- Significance
- Unreduced dislocation
- Action
- Assess NV, reduce urgently
- Significance
- Posterior dislocation
- Action
- Confirm with X-ray, reduce
- Significance
- Arterial injury/kinking
- Action
- Urgent reduction
- Significance
- Nerve injury/entrapment
- Action
- Document, usually resolves with reduction
- Significance
- Open dislocation
- Action
- Antibiotics, urgent OR
- Significance
- High energy, compartment risk
- Action
- Monitor compartments
Differential diagnosis:
- Discriminating feature
- Loss of normal three-point bony relationship; ulna posterior to trochlea, no fracture
- Key investigation
- AP and lateral radiograph
- Discriminating feature
- Dislocation PLUS radial head and/or coronoid and/or olecranon fracture
- Key investigation
- Radiograph + CT for fragment characterisation
- Discriminating feature
- Deformity with crepitus; intact ulnohumeral articulation on lateral film, fracture line proximal to joint
- Key investigation
- Radiograph (look for fat-pad sign, fracture proximal to joint)
- Discriminating feature
- Localised lateral tenderness, painful rotation, joint reduced and congruent
- Key investigation
- Radiograph; radiocapitellar (Greenspan) view
- Discriminating feature
- Arm held pronated and slightly flexed, refusal to use; normal radiograph
- Key investigation
- Clinical; radiograph usually normal
- Discriminating feature
- Fever or no clear trauma, global swelling, congruent joint on film
- Key investigation
- Aspiration, inflammatory markers
- Discriminating feature
- Recurrent clicking/giving way, positive pivot-shift, reduced at rest
- Key investigation
- Stress radiographs / examination under anaesthesia
Pre-reduction assessment:
- Neurovascular status - median, ulnar, radial nerves; brachial artery
- Skin integrity - open vs closed
- Associated injuries - ipsilateral limb
- Deformity pattern - helps predict direction
Document neurovascular status before and after reduction. The ulnar nerve is most commonly injured (transient paresthesias in 10-20%). Brachial artery injury is rare but can occur, especially with anterior dislocations or open injuries.
STABLESTABLE - Post-Reduction Assessment
Hook:Is the elbow STABLE? Test it thoroughly
Investigations
- AP elbow (or attempt)
- Lateral elbow
- Often difficult to obtain true views due to deformity
- Confirm dislocation and direction
- Look for associated fractures (radial head, coronoid)
- Assess any bony fragment position
Do not delay reduction waiting for imaging if neurovascular compromise is present. A single lateral view can confirm dislocation. Reduce urgently, then obtain post-reduction imaging.
- AP and lateral elbow - confirm concentric reduction
- Look carefully for:
- Radial head fracture (often subtle)
- Coronoid fracture (often seen on lateral)
- Any joint widening suggesting interposed fragments
- Concentric reduction (radiocapitellar alignment)
- Suspected associated fracture not clear on X-ray
- Complex dislocation patterns
- Surgical planning
- Any joint incongruency on plain films
- Fracture characterization (radial head, coronoid)
- Fragment count and size
- Associated injuries
Management
Reduction technique:
- Adequate analgesia/sedation (or general anesthesia)
- Assistant for counter-traction
- Fluoroscopy available if possible
- Document pre-reduction neurovascular status
- Patient supine, arm abducted
- Assistant holds upper arm for counter-traction
- Operator controls forearm
- Apply longitudinal traction along forearm
- Slight supination to correct rotational component
- Flex elbow while applying pressure to olecranon
- May need brief hyperextension to unlock coronoid
- Guide olecranon over trochlea into reduced position
- Palpable/audible clunk confirms reduction
- Confirm reduction with fluoroscopy/X-ray
- Test stability through ROM
- Document neurovascular status
- Splint in stable position
For posterolateral dislocation: Apply longitudinal traction with the forearm supinated (corrects the lateral rotation). Apply pressure to olecranon while flexing the elbow. The olecranon slides over the trochlea and reduces with a palpable clunk.
After reduction, assess stability under fluoroscopy:
-
Flexion-extension arc: Move through ROM
- Note angle at which elbow redislocates
- Stable if maintains reduction 30-130°
- Unstable if redislocates before 60° extension
-
Valgus stress test: Test MCL integrity
-
Varus stress test: Test LCL integrity
-
Lateral pivot shift (if awake): Tests for PLRI
If the elbow is stable through 30° extension, it can be managed non-operatively with early motion. If it redislocates before 60° extension, operative stabilization is usually needed.
TERRIBLETERRIBLE TRIAD - Components and Treatment
Hook:The TERRIBLE TRIAD requires systematic treatment of all components
Surgical Technique
Kocher (Lateral) Approach
- LCL repair
- Radial head fixation/replacement
- Lateral coronoid access
- Incision from lateral epicondyle to ulna
- Identify anconeus-ECU interval
- Elevate anconeus from posterior ulna
- Expose LCL complex (usually avulsed from lateral epicondyle)
- Address radial head
- Repair LCL with suture anchors
The lateral approach provides excellent access to the lateral stabilizers.
Complications
- Incidence
- 20-30%
- Management
- Early motion, physio, capsular release if severe
- Incidence
- 1-2% simple, higher complex
- Management
- LCL reconstruction, address all structures
- Incidence
- 5-10%
- Management
- Prophylaxis (indomethacin), excision if limiting
- Incidence
- 5-10%
- Management
- Activity modification, eventual arthroplasty
- Incidence
- Variable
- Management
- LCL reconstruction
- Incidence
- 10-20% transient
- Management
- Usually resolves, may need exploration
- Incidence
- Rare
- Management
- Urgent vascular repair
- Incidence
- Rare
- Management
- Emergency fasciotomy
- Most common complication
- Prevention is key - early motion
- Flexion contracture most common pattern
- Treatment: physiotherapy, dynamic splinting, surgical release
- Chronic sequela of untreated/inadequately healed LCL
- Patient has apprehension or frank instability
- Treatment: LCL reconstruction
The topic names the "lateral pivot shift" but a complete answer on chronic posterolateral rotatory instability (PLRI) - the late sequela of an incompetent LCL/LUCL - should give the full provocative battery, because the frank pivot-shift is often only positive under anaesthesia in a guarding patient:
- Lateral pivot-shift test (O'Driscoll): supine, arm overhead; apply supination, valgus and axial compression while flexing from extension - the radiohumeral joint subluxates then reduces with a clunk around 40 degrees of flexion. Often needs anaesthesia.
- Posterolateral rotatory drawer test: an antero-posterior "drawer" of the forearm on the humerus producing posterolateral rotation.
- Chair push-up (push-up) sign: pushing up from a chair with forearms supinated reproduces apprehension/subluxation.
- Active floor push-up (prone push-up) test: apprehension/subluxation pressing up from the floor with arms abducted and forearms supinated.
- Table-top relocation test: pain/apprehension leaning on the affected hand on a table in supination, relieved when the examiner supports (relocates) the radial head.
On imaging, the "drop sign" - ulnohumeral joint widening/incongruity (the trochlea "dropping" away from the olecranon) on a lateral radiograph - signals residual instability after reduction or surgery and mandates reassessment (often a hinged external fixator or further ligament work).
Exam point: PLRI is diagnosed by the lateral pivot-shift plus the awake-patient apprehension tests (chair push-up, floor push-up, table-top relocation), and a postreduction drop sign on the lateral film means the joint is not concentrically stable.
The elbow is prone to stiffness after injury. Most activities require 30-130° arc and 50° supination/pronation. Early motion within the first week significantly reduces stiffness risk. A functional arc for most activities is 30-130°.
Heterotopic ossification:
- Risk factors: head injury, burns, delayed surgery, aggressive physio
- Prophylaxis: indomethacin 25mg TDS x 3 weeks (or radiation)
- Excision if mature and limiting function
The adult medial epicondyle entrapment shown above has a paediatric counterpart, and the examinable framework is when to operate on the paediatric medial epicondyle avulsion (the apophysis to which the MCL and flexor-pronator origin attach, often avulsed during a paediatric elbow dislocation):
- Absolute (uncontested) operative indications: a fragment incarcerated within the joint (cannot be reduced closed - the classic "missed" cause of a blocked, unstable elbow), an open fracture, and ulnar nerve dysfunction that warrants exploration. Valgus instability in the high-demand throwing/overhead athlete is a strong relative indication.
- The displacement controversy: there is no agreed displacement threshold for fixing a non-incarcerated fragment - historical cut-offs of about two, five and up to fifteen millimetres are all quoted, displacement is notoriously hard to measure on plain films (the apophysis is posteromedial; oblique/distal-humerus views or CT improve accuracy), and several series show good results with non-operative management of even quite displaced fragments (fibrous union is often asymptomatic).
- Operative technique: open reduction and fixation (screw in the adolescent with a large fragment, or sutures/anchors in the very young), restoring the MCL/flexor-pronator origin; protect/identify the ulnar nerve.
Exam point: incarceration in the joint, an open injury, or ulnar nerve dysfunction mandate surgery (with valgus instability in the throwing athlete a strong relative indication); for the isolated displaced fragment the displacement threshold is genuinely controversial and measurement is unreliable, so decisions are individualised rather than driven by a single millimetre cut-off.
Postoperative Care and Rehabilitation
Simple dislocation (non-operative):
- Posterior splint at 90°
- Elevation, ice
- Finger motion
- Convert to hinged elbow brace
- Begin active ROM in brace
- Flexion-extension exercises
- Light supination/pronation
- Progressive ROM
- May wean from brace if stable
- Target functional ROM
- No valgus/varus stress
- Full ROM expected
- Begin strengthening
- Progressive activity
- May resume light sport
- Full activity
- Sports clearance
- Final outcome assessment
Post-operative (LCL repair/complex):
- More protected initially
- Hinged brace with extension block if needed
- Motion started early but within safe arc
- Progress based on stability and healing
Functional elbow ROM for most activities: 30-130° flexion-extension and 50° supination/pronation. Focus rehabilitation on achieving this functional arc. Some terminal limitation may be well-tolerated.
Outcomes and Prognosis
Outcomes by type:
- Good/Excellent
- 90-95%
- Key Factors
- Early motion critical
- Good/Excellent
- 85-90%
- Key Factors
- Quality of repair
- Good/Excellent
- 70-80%
- Key Factors
- Address all structures
- Good/Excellent
- 60-80%
- Key Factors
- Pattern-dependent
Prognostic factors:
- Simple vs complex (simple better)
- Time to reduction
- Time to motion initiation
- Quality of reduction
- Associated injuries
- Patient compliance
Simple elbow dislocations that are stable after reduction have excellent prognosis (over 90% good/excellent outcomes) with early motion protocol. The key is avoiding prolonged immobilization.
Guidelines, Registries & Global Practice
Global epidemiology
- Figure
- 5.21 per 100,000 person-years (US NEISS)
- Source
- Stoneback 2012 (PMID 22298056)
- Figure
- 10-19 years (6.87 per 100,000; 43.5% of cases)
- Source
- Stoneback 2012
- Figure
- Essentially equal (rate ratio 1.02)
- Source
- Stoneback 2012
- Figure
- 44.5% (football/wrestling in males; gymnastics/skating in females)
- Source
- Stoneback 2012
- Figure
- Roughly half of dislocations are simple (no fracture)
- Source
- Josefsson 1987 (PMID 3571318)
Elbow dislocation is the second most common large-joint dislocation after the shoulder and is predominantly an injury of active adolescents and young adults.
Guidance and evidence, side by side
There is no single dedicated international society guideline for elbow dislocation comparable with hip-fracture pathways; practice is driven by high-level trial and consensus evidence that is broadly concordant across regions.
- Position
- Closed reduction then early active mobilisation; avoid prolonged immobilisation
- Evidence basis
- Level I RCT (FuncSiE, PMID 26175020) and Level I (Josefsson, PMID 3571318) - no benefit from routine ligament repair or plaster
- Position
- As short as comfort allows (days, not weeks); immobilisation beyond ~1-2 weeks increases stiffness
- Evidence basis
- Level IV (Mehlhoff, PMID 3343270): immobilisation strongly linked to flexion contracture
- Position
- Systematic operative repair - radial head, coronoid, LCL +/- MCL/hinged fixator
- Evidence basis
- Level IV reference protocol (Pugh/King/McKee, PMID 15173283); endorsed by AO Foundation and elbow-surgeon consensus
- Position
- Lateral ligament reconstruction (tendon graft preferred over direct repair)
- Evidence basis
- Level IV (Sanchez-Sotelo, PMID 15686238)
- Position
- Emergent reduction and surgical management (general trauma/BOA-style principles)
- Evidence basis
- Open-fracture and limb-threatening-injury principles (BOAST, AO)
Registry evidence
Elbow dislocation is a soft-tissue / fracture-dislocation injury and is not tracked by the arthroplasty joint registries (NJR, AJRR, AOANJRR, SHAR, NZJR), which capture joint replacement rather than acute trauma. Epidemiology therefore derives from national injury-surveillance datasets (e.g. the US NEISS database) rather than implant registries.
Global practice variation
- High-resource settings: ready access to fluoroscopy, CT for complex patterns, radial head arthroplasty and hinged external fixators; early supervised hand-therapy-led mobilisation is standard.
- Limited-resource settings: reliance on plain radiographs and closed reduction; restricted access to radial head prostheses and hinged fixators may favour fixation or, where unavoidable, excision strategies and longer protected mobilisation.
- Convergent core: across all settings the principles are identical - reduce promptly, document neurovascular status before and after, classify simple versus complex, test the stable arc, and mobilise early.
Be prepared to discuss reduction technique, stability assessment, simple vs complex classification, and terrible triad management. Understanding the Horii circle, the FuncSiE early-mobilisation evidence, and when to operate are key viva topics across FRCS, FRACS, EBOT and ABOS.
MCQ Practice Points
Q: What is the most common direction of elbow dislocation? A: Posterolateral - accounts for approximately 90% of elbow dislocations. The mechanism (FOOSH with valgus and supination moment) drives the ulna posterior and lateral to the humerus.
Q: What differentiates simple from complex elbow dislocation? A: Simple = no fracture (ligament injury only). Complex = with associated fracture (radial head, coronoid, olecranon). Simple dislocations are usually stable after reduction with excellent prognosis.
Q: In what order do structures fail in posterolateral elbow dislocation? A: According to the Horii circle, injury progresses from lateral to medial: Stage 1 (LCL complex), Stage 2 (anterior/posterior capsule), Stage 3 (MCL). The LCL is always injured first.
Q: What is the threshold for stable vs unstable simple elbow dislocation? A: If the elbow maintains reduction through 30° extension to full flexion, it is considered stable for non-operative treatment. If it redislocates before 60° extension, operative stabilization is usually recommended.
Q: What is the most common complication of elbow dislocation? A: Stiffness - occurs in 20-30% to some degree. Prevention through early motion is key. Prolonged immobilization (greater than 3 weeks) significantly increases stiffness risk.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old man falls while skateboarding, landing on his outstretched hand. He presents with obvious elbow deformity. X-rays confirm a posterior elbow dislocation with no fracture. How do you manage this injury?”
“You reduce a simple posterior elbow dislocation in a 35-year-old woman. After reduction, under sedation, you assess stability. The elbow redislocates when you extend beyond 50 degrees. What is your management?”
“A 45-year-old woman falls down stairs. Her elbow was dislocated and has been reduced in the emergency department. CT shows a Mason Type III radial head fracture with 5 fragments and a small coronoid tip fracture. How do you approach this injury?”
CLASSIFICATION
- Simple = no fracture, ligament injury only
- Complex = with fracture(s)
- Posterolateral = 90% (most common)
- LCL always injured in posterolateral
HORII CIRCLE (INJURY PROGRESSION)
- Stage 1: LCL complex (lateral)
- Stage 2: Anterior/posterior capsule
- Stage 3A: Posterior MCL
- Stage 3B: Entire MCL (medial)
REDUCTION TECHNIQUE
- Document NV status before and after
- Adequate sedation essential
- Traction + supination + olecranon pressure + flex
- Confirm with X-ray
STABILITY ASSESSMENT
- Test ROM under sedation/anesthesia
- Stable if maintains reduction to 30° extension
- Unstable if redislocates before 60° extension
- Unstable = likely needs operative repair
SIMPLE DISLOCATION MANAGEMENT
- If stable: early motion, hinged brace
- Begin ROM within first week
- Avoid prolonged immobilization (greater than 3 weeks)
- If unstable: LCL repair
TERRIBLE TRIAD PROTOCOL
- Dislocation + radial head + coronoid + LCL
- 1. Fix/replace radial head
- 2. Repair LCL (always injured)
- 3. Fix coronoid if still unstable
- 4. Consider hinged fixator if needed
Evidence Base
- First description of posterolateral rotatory instability (PLRI) of the elbow in five patients. Identified laxity of the ulnar part of the lateral collateral ligament (LUCL) as the essential lesion, producing transient rotatory subluxation of the ulnohumeral joint with the annular ligament intact. Defined the pivot-shift (posterolateral rotatory-instability) test; operative repair of the LUCL eliminated instability in all five.
- Prospective randomised trial of 30 adults with simple elbow dislocation examined under anaesthesia, then randomised to surgical ligament repair versus non-operative care. All elbows had medial and most had combined medial and lateral collateral ligament rupture. At follow-up both groups had generally good results with no statistically significant difference - surgical repair conferred no advantage over closed treatment.
- Long-term review of 52 adults with simple elbow dislocation treated by closed reduction (mean follow-up 34 months). 60% reported residual symptoms; flexion contracture greater than 30 degrees in 15%, residual pain in 45%. Prolonged immobilisation was strongly associated with larger flexion contracture (p less than 0.001) and more severe pain.
- Defined the standard surgical protocol for the terrible triad in 36 consecutive elbows: radial head fixation or replacement, coronoid fixation where feasible, lateral collateral ligament repair, and selective MCL repair or hinged external fixation. At a mean of 34 months the mean Mayo Elbow Performance Score was 88; 28 of 36 (78%) were excellent or good and concentric stability was restored in 34 of 36. Eight patients required reoperation.
- 44 patients with posterolateral rotatory instability followed at a mean of six years after 12 direct LCL repairs or 33 tendon-graft reconstructions. Surgery restored stability in all but five; mean Mayo Elbow Performance Score 85, with 86% subjectively satisfied. Augmented tendon-graft reconstruction gave better and durable results compared with simple repair (p = 0.04), and outcomes did not deteriorate with time.
- Multicentre randomised trial of 100 adults with simple elbow dislocation comparing immediate active mobilisation with 3 weeks of plaster immobilisation. At 6 weeks the early-mobilisation group had less disability (DASH 12 vs 19) and a larger flexion-extension arc (121 vs 102 degrees) and returned to work sooner (10 vs 18 days). No recurrent dislocations occurred and the complication rate did not differ; 1-year DASH was equivalent.
- National (US) Electronic Injury Surveillance System analysis estimated an elbow dislocation incidence of 5.21 per 100,000 person-years. The highest rate (43.5% of cases) occurred in 10-19 year-olds (6.87 per 100,000); incidence was essentially equal between sexes. Nearly half (44.5%) of dislocations in those aged 10 or older were sports-related - football and wrestling in males, gymnastics and skating in females.