Both-Bone Fractures, Greenstick, and Monteggia-Galeazzi
- Younger children remodel more (under 10 years: 20° acceptable)
- Sagittal plane remodels better than coronal
- Rotational deformity does NOT remodel - must reduce
- Always obtain true elbow views to exclude Monteggia
- Greenstick fractures may need completion plus overcorrection
- “Check radiocapitellar line on all forearm fractures
- “10° residual angulation is maximum in children over 10
- “Pronation-supination measured clinically, not on X-ray
- “ESIN preferred over plating in pediatric fractures
ALWAYS check the radiocapitellar line on any forearm fracture. Miss a Monteggia = medicolegal disaster. Radial head points to capitellum in all views.
Rotational malunion is permanent. Unlike angular deformity, rotational deformity cannot remodel. Clinically assess pronation-supination after reduction.
Younger = more acceptable. Under 10: up to 20°. Over 10: maximum 10°. Near physis: more forgiving. Mid-shaft: less forgiving.
Complete the fracture to prevent re-angulation. Greensticks with significant angulation should be completed during reduction to allow full correction and prevent cast loosening as swelling subsides.
- Stability
- Stable
- Treatment
- Splint or removable cast 3-4 weeks
- Key Pearl
- Parent-directed removal possible
- Stability
- Relatively stable
- Treatment
- Below elbow cast 4-6 weeks
- Key Pearl
- Watch for re-angulation
- Stability
- Unstable when completed
- Treatment
- Complete, reduce, above elbow cast
- Key Pearl
- 3-point mold essential
- Stability
- Unstable
- Treatment
- Closed reduction, above elbow cast
- Key Pearl
- Consider ESIN if unstable
- Stability
- Unstable
- Treatment
- Reduce ulna, check radial head
- Key Pearl
- Closed vs open reduction of ulna
- Stability
- Unstable
- Treatment
- Reduce radius, DRUJ usually stable
- Key Pearl
- Less common than in adults
RUGSRadiocapitellar Line Check
Hook:Check RUGS under the carpet - never miss a Monteggia hidden under an ulna fracture!
10-20Acceptable Angulation
Hook:10 and 20: Under 10 years accepts 20°, over 10 years accepts only 10°
SPARForearm Remodeling Rules
Hook:SPAR with rotational malunion - it's the one thing that will never get better!
Overview and Epidemiology
Forearm fractures are the most common pediatric fractures, accounting for up to 45% of all childhood fractures. The distal third is most frequently affected, but mid-shaft both-bone fractures are most concerning due to loss of forearm rotation.
- Peak age 4-14 years
- More common in boys (playground, sports)
- Distal third most common location
- Both-bone more common than single bone
- Incidence increasing (more active play)
- Fall from height (playground equipment)
- Sports injuries
- Direct trauma (less common)
- Cycling accidents
- Consider NAI in unusual patterns
Anatomy and Biomechanics
The radius and ulna function as a unit linked by the interosseous membrane. Any injury to one bone can affect the other or the proximal/distal radioulnar joints. This is why Monteggia and Galeazzi injuries occur.
Structural Considerations
- Radius and ulna connected by proximal and distal radioulnar joints
- Interosseous membrane provides stability
- Rotation occurs through supination/pronation
- Neutral rotation: thumb up, radial bow lateral
The natural radial bow allows clearance for muscle bellies and is essential for full pronation-supination. Loss of radial bow restricts rotation.
Classification Systems
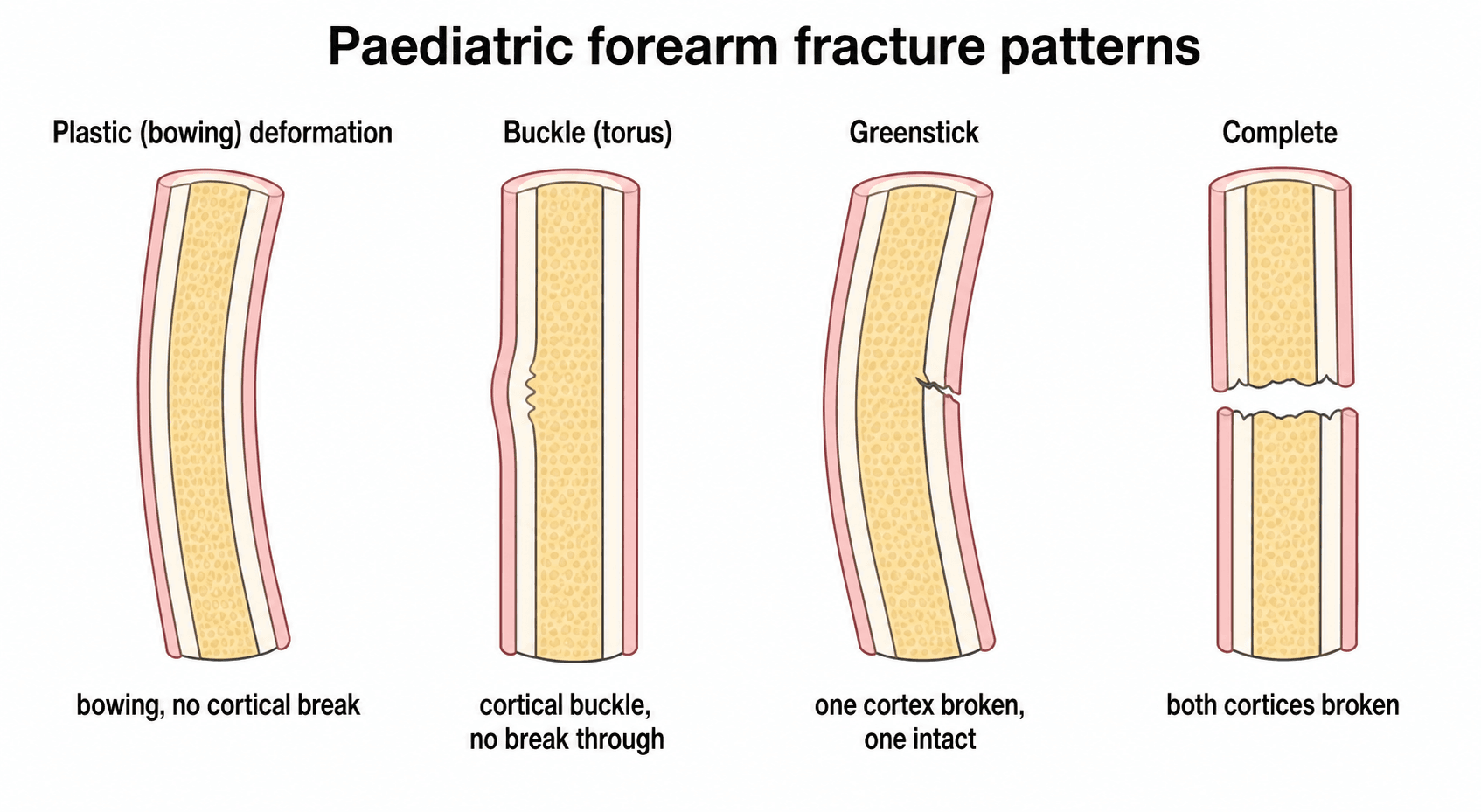
Pediatric Forearm Fracture Patterns
- Description
- Bowing without fracture line
- Stability
- Stable if less than 20°
- Treatment
- Reduction if greater than 20°
- Description
- Cortical compression, no displacement
- Stability
- Stable
- Treatment
- Splint 3-4 weeks
- Description
- One cortex complete, other intact
- Stability
- Variable
- Treatment
- Complete if angulated
- Description
- Both cortices disrupted
- Stability
- Unstable
- Treatment
- Closed reduction, cast/ESIN
Clinical Assessment
- Mechanism of injury
- Hand dominance
- Sports involvement
- Time since injury
- Previous fractures
- Any numbness or tingling
- Deformity and swelling
- Open wound (even needle-prick)
- Neurovascular status (median, ulnar, radial nerves)
- Compartment syndrome signs
- Check elbow and wrist for tenderness
- Assess rotational alignment (hard in acute setting)
Check the elbow on EVERY forearm fracture. Examine for elbow tenderness and get proper elbow X-rays. If the ulna is fractured, the radial head MUST be checked. A missed Monteggia leads to chronic radial head dislocation and functional impairment.
Rotation cannot be assessed on X-ray. Clinically compare pronation-supination to the opposite side. After reduction, the hand should lie flat with forearm supinated. Any rotational malunion is permanent.
Differential Diagnosis
A child with a painful, swollen forearm after a fall is not always a simple shaft fracture. Distinguishing these patterns changes management entirely - the most dangerous error is treating an isolated bone fracture and missing the associated joint injury.
- Key Distinguishing Feature
- Both radius and ulna fractured at similar level
- Pitfall if Missed
- Loss of forearm rotation if malreduced
- Key Distinguishing Feature
- Isolated ulna fracture/plastic bow PLUS broken radiocapitellar line
- Pitfall if Missed
- Chronic radial head dislocation, fixed pronation loss
- Key Distinguishing Feature
- Distal radius fracture PLUS widened or incongruent DRUJ
- Pitfall if Missed
- DRUJ instability, painful rotation
- Key Distinguishing Feature
- Single cortical wrinkle, no second-bone or joint injury
- Pitfall if Missed
- Overtreatment with rigid cast and follow-up
- Key Distinguishing Feature
- Tenderness/widening at the physis, not the shaft
- Pitfall if Missed
- Growth arrest if reduction forced repeatedly
- Key Distinguishing Feature
- Bowing with NO visible cortical break
- Pitfall if Missed
- Persistent rotational block; underestimated as 'no fracture'
- Key Distinguishing Feature
- Mechanism inconsistent with injury, multiple ages of injury, delayed presentation
- Pitfall if Missed
- Repeat injury or fatality if safeguarding missed
Investigations
Radiological Investigations
- What to Check
- Fracture pattern, displacement, angulation
- Don't Miss
- Both bone involvement
- What to Check
- Sagittal angulation, radial bow
- Don't Miss
- Bayonet apposition
- What to Check
- Radiocapitellar alignment
- Don't Miss
- Monteggia - radial head dislocation
- What to Check
- Radiocapitellar line
- Don't Miss
- Posterior fat pad (effusion)
- What to Check
- DRUJ congruence
- Don't Miss
- Galeazzi - DRUJ subluxation
Key principle: The joint above and below a forearm fracture must be imaged.

Management
Under 10 years: Accept up to 15-20° in sagittal plane, 10-15° in coronal plane. Over 10 years: Maximum 10° in either plane. Rotation: ZERO tolerance - must be anatomically reduced. Mid-shaft: Less forgiving than metaphyseal.
Buckle (Torus) Fracture Management
Stable cortical compression injury without displacement.
Splint or removable cast for 3-4 weeks. Parent-directed removal is safe. No follow-up X-rays usually needed.
These are inherently stable. Do not overtreat them with above elbow casts. Early mobilization is safe.
A proper 3-point mold is essential for maintaining reduction in cast. The interosseous mold is key. Pad bony prominences. The cast should be well-fitted but allow for swelling. Weekly X-rays for first 2-3 weeks to detect loss of reduction.
Cast Quality and the Cast Index
The management section stresses a well-moulded three-point cast, and the evidence (Bowman) shows that loss of reduction is common and happens early. The quality of the mould can be measured objectively rather than judged by eye, and these indices are increasingly examined as the radiographic answer to "how do you know the cast is good?".
- What It Measures
- Internal cast width on the LATERAL view divided by the internal width on the AP view, at the fracture level
- Threshold / Meaning
- About 0.7 or less indicates good oval moulding; a value above 0.8 (a round cast) predicts loss of reduction
- What It Measures
- Quantifies the three-point mould relative to the fracture displacement
- Threshold / Meaning
- Higher values predict redisplacement of completely displaced distal radius fractures
- What It Measures
- Padding thickness relative to bone width at the apex of deformity
- Threshold / Meaning
- Excess padding lets the fracture move and the position slip
- What It Measures
- Space between the cast and the limb
- Threshold / Meaning
- A loose cast (large gap) permits redisplacement as swelling settles
A well-moulded forearm cast is OVAL in cross-section - flattened over the volar and dorsal surfaces to create the three-point mould - giving a cast index of about 0.7 or less. A round, over-padded cast (cast index above 0.8) is the commonest technical reason for loss of reduction, which usually occurs within the first three weeks (Bowman). If the cast index looks poor on the check radiograph, re-mould or re-cast rather than waiting for the fracture to slip.
Surgical Technique Considerations
ESIN for Pediatric Forearm Fractures
- Dorsal entry just proximal to Lister's tubercle OR
- Lateral entry above distal radial physis
- Avoid palmar entry (flexor tendons)
- Proximal/antegrade entry at olecranon or proximal metadiaphysis
- Avoid distal ulnar physis (small, subcutaneous)
Pre-bend nails for radial bow. Seat nails well to avoid irritation and protrusion. Both bones should ideally be nailed. Use 2-2.5mm nails typically.
ESIN: Complications and Pitfalls
The topic covers when and how to use elastic stable intramedullary nailing and that nails are usually removed at 6-12 months, but the complication profile of ESIN is itself high-yield - especially as the child approaches skeletal maturity.
- Mechanism
- Prominent or long nail ends, especially over the subcutaneous distal ulna
- Avoidance / Management
- Trim and bury the nail ends; bursitis may settle or prompt earlier removal
- Mechanism
- Lateral/dorsal radial entry lies near the superficial radial nerve and the EPL tendon at Lister's tubercle
- Avoidance / Management
- Open entry with nerve protection; EPL can be irritated or, rarely, rupture
- Mechanism
- Open reduction or proximal radial manipulation
- Avoidance / Management
- Recognise the at-risk approach; usually a recovering neurapraxia
- Mechanism
- Closed passage fails to cross the fracture, common in adolescents
- Avoidance / Management
- Up to around 76% of nailed adolescents need open reduction of at least one bone (Freese)
- Mechanism
- A straight elastic nail fails to recreate the radial bow, especially near maturity
- Avoidance / Management
- Pre-bend the nails; consider plating in older adolescents (Freese)
- Mechanism
- Excess soft-tissue stripping, a single incision for both bones, or multiple passes
- Avoidance / Management
- Minimise passes and stripping; use separate incisions for the two bones
- Mechanism
- Stress riser through the healing bone and entry site
- Avoidance / Management
- Protect after removal and time removal appropriately (6-12 months)
- Mechanism
- Multiple forceful reduction and nailing passes with soft-tissue swelling
- Avoidance / Management
- Limit the number of passes; monitor closely with a low threshold for fasciotomy
ESIN is elegant in younger children, but its problems cluster in adolescents near skeletal maturity, where a straight elastic nail struggles to restore the radial bow and often forces an open reduction. Freese et al. found major complications in 55% of nailed adolescents versus none after plating, with around 76% needing open reduction and 91% a second operation. This is why plating is increasingly chosen as the child approaches maturity (see Areas of Uncertainty and Debate).
Complications
Complications of Pediatric Forearm Fractures
- Incidence
- Up to 20%
- Cause
- Poor mold, swelling resolution
- Management
- Re-manipulate or ESIN
- Incidence
- Varies
- Cause
- Missed re-displacement
- Management
- Remodel if young, osteotomy if old
- Incidence
- Permanent
- Cause
- Inadequate reduction
- Management
- Osteotomy if symptomatic
- Incidence
- Rare but serious
- Cause
- Tight cast, soft tissue swelling
- Management
- Fasciotomy urgently
- Incidence
- 5-10%
- Cause
- Early return to activity
- Management
- Cast longer, protect 6+ months
- Incidence
- Rare
- Cause
- High-energy, single-incision for both bones
- Management
- Excision if symptomatic
- Incidence
- Rare
- Cause
- Incomplete imaging
- Management
- Late reconstruction
Refracture occurs in 5-10% of forearm fractures. Protect for 6 months after healing with avoidance of high-risk activities. Some surgeons recommend a splint for sport during this period.
Postoperative Care
Post-Treatment Protocol
Elevate limb. Check neurovascular status. Watch for compartment syndrome. Above elbow cast (if closed treatment).
Weekly X-rays to check for re-displacement. Cast check for tightness or looseness. Finger exercises.
X-ray at 4 weeks to assess union. May convert to below elbow cast or removable brace in mid-treatment.
Remove cast once clinical and radiological healing. X-ray out of cast. Commence ROM exercises.
Avoid contact sports and high-risk activities. Refracture risk during this period. Full activities at 6 months.
Outcomes and Prognosis
Excellent Prognosis with Proper Treatment
- Rotation anatomically reduced
- Angular malunion within acceptable limits
- Monteggia and Galeazzi identified and treated
- Adequate protection from refracture
- Rotational malunion
- Missed Monteggia (chronic radial head dislocation)
- Late diagnosis of compartment syndrome
Guidelines, Registries & Global Practice
- Forearm fractures are among the most common childhood fractures worldwide, with the distal radius the single most frequent site
- Peak incidence in the pre-pubertal growth spurt (boys ~12-14, girls ~10-12 years)
- Incidence has risen over recent decades in several high-income populations, linked to activity, body mass and reduced bone density
- Boys affected more than girls overall; trampolines, playground falls and contact sport dominate mechanisms
- No implant registry tracks paediatric forearm fixation the way arthroplasty registries do; evidence comes from RCTs and large cohorts
- The UK FORCE trial (965 children) is the landmark dataset for torus fractures, driving de-implementation of casting and follow-up
- Cohort data (Bowman) quantify that ~half of displaced both-bone fractures lose acceptable position, mostly within 3 weeks
Side-by-Side Guideline and Society Positions
- Torus (buckle)
- Removable support, discharge, no routine follow-up (post-FORCE)
- Displaced shaft
- Reduction; surgery if unstable or unacceptable position
- Emphasis
- Minimising overtreatment and radiation
- Torus (buckle)
- Splint or short-arm cast, minimal imaging
- Displaced shaft
- Closed reduction; ESIN/plate for failed or unstable
- Emphasis
- Shared decision-making, function
- Torus (buckle)
- Stable - immobilise symptomatically
- Displaced shaft
- PDFC algorithm: cast vs ESIN vs external fixation by pattern
- Emphasis
- Pattern-based fixation, preserve periosteum
- Torus (buckle)
- Removable splint increasingly standard
- Displaced shaft
- ESIN favoured for unstable diaphyseal fractures
- Emphasis
- Less invasive surgery, early function
High-Resource vs Limited-Resource Practice
- Image intensifier and procedural sedation/GA readily available for closed reduction
- ESIN and locking plates stocked; theatre access within hours to days
- Trend toward de-implementation: fewer casts, fewer follow-up radiographs for stable patterns
- Closed reduction and well-moulded casting remain the mainstay and give excellent results in growing bone
- Implants and intra-operative imaging may be scarce; emphasis on getting the first cast right and on clinical rotation assessment
- Strong reliance on remodelling means angular deformity is more often accepted; rotational reduction and exclusion of Monteggia remain non-negotiable everywhere
Special Considerations
Monteggia Fracture-Dislocation
Ulna fracture + radial head dislocation + disrupted annular ligament.
Apex anterior ulna angulation, anterior radial head dislocation. Extension injury mechanism.
Closed reduction of ulna usually reduces radial head. Above elbow cast in flexion and supination. If radial head remains dislocated, open reduction may be needed (annular ligament may be entrapped). Check radiocapitellar line post-reduction.
MCQ Practice Points
Q: Which type of deformity in pediatric forearm fractures does NOT remodel? A: Rotational deformity. Angular deformity remodels well, especially in the sagittal plane and in younger children. Rotational malunion is permanent and must be anatomically reduced.
Q: What is a Bado Type I Monteggia lesion? A: Ulna fracture with apex anterior angulation and anterior dislocation of the radial head. This is the most common type in children (70%).
Q: How much angulation is acceptable in a forearm fracture in a 12-year-old child? A: Maximum 10 degrees. Over 10 years of age, remodeling potential is limited. Under 10 years, up to 15-20 degrees may be accepted.
Q: Why should a significantly angulated greenstick fracture be 'completed' during reduction? A: To prevent spring-back re-angulation. The intact cortex acts as a spring. Completing the fracture allows full correction and prevents cast loosening and re-angulation.
Q: What does the radiocapitellar line assess? A: Position of the radial head relative to the capitellum. A line through the radial shaft should pass through the capitellum center on all views. Deviation indicates radial head dislocation (Monteggia).
Q: What is the main indication for ESIN in pediatric forearm fractures? A: Unstable fractures that cannot be maintained in cast, including failed closed reduction, re-displacement in cast, open fractures, and polytrauma.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 7-year-old boy fell off playground equipment. X-rays show complete both-bone forearm fractures at the mid-shaft with 25 degrees of angulation on both AP and lateral views and 100% displacement. Neurovascular exam is normal. How would you manage this?”
“A 5-year-old girl presents after a fall with a displaced ulna fracture with apex anterior angulation. She has pain and limited motion at the elbow. How would you assess and manage this?”
“A 9-year-old presents with a greenstick fracture of the distal radius with 20 degrees of apex volar angulation on the lateral view. The intact cortex is on the volar (palmar) side. How would you manage this?”
Key Facts
- Most common pediatric fracture (45%)
- Rotation does NOT remodel
- Sagittal plane remodels better than coronal
- Always check radiocapitellar line
Acceptable Angulation
- Under 10 years: 15-20°
- Over 10 years: maximum 10°
- Mid-shaft less forgiving than metaphyseal
- Rotation: ZERO tolerance
Fracture Patterns
- Buckle: Splint 3-4 weeks
- Greenstick: Complete if angulated greater than 15-20°
- Complete: Closed reduction, above elbow cast
- Monteggia: Ulna + radial head dislocation
ESIN Indications
- Failed closed reduction
- Re-displacement in cast
- Open fracture
- Polytrauma, older child
Monteggia Bado Types
- Type I: Anterior radial head (70%)
- Type II: Posterior radial head
- Type III: Lateral radial head
- Type IV: Anterior + radial fracture
Evidence Base and Key Studies
FORCE Trial - Torus (Buckle) Fracture Immobilisation
- Multicentre randomised equivalence trial across 23 UK emergency departments, 965 children aged 4-15 years
- Offer of a soft bandage with immediate discharge was equivalent to rigid immobilisation for pain at 3 days (adjusted difference -0.10, 95% CI -0.37 to 0.17)
- No between-group difference in function or quality of life over 6 weeks
- Complication rates very low and similar (offer-of-bandage 1.0% vs rigid immobilisation 0.6%)
Davidson et al. - Simple Treatment of Distal Radius Torus Fractures
- Prospective randomised trial of 201 children comparing plaster cast vs a removable Futura-type wrist splint for 3 weeks
- No difference in outcome between groups; all patients achieved a good result
- Only 1 child did not tolerate the splint
- No evidence that follow-up beyond the day after diagnosis was required
Bowman et al. - Predictors of Failure of Nonoperative Both-Bone Fractures
- 321 children with complete both-bone shaft fractures; 282 treated by closed reduction and casting
- 51% exceeded acceptable angulation thresholds within follow-up; of these, 55% failed by the end of week 1 and 95% by week 3
- Highest odds of failure: age 10 years or older (OR 2.79), proximal-third radius fractures (OR 6.81), and initial ulnar angulation under 15 degrees (OR 2.94)
- Thresholds used: 10 degrees proximal, 15 degrees middle, 20 degrees distal in younger children; 10 degrees at all levels in older children
Schmittenbecher - State-of-the-Art Forearm Shaft Fracture Treatment
- Synthesis of a single-institution series since 1976; before ESIN, 95.9% of fractures were treated conservatively and a significant proportion healed with malalignment and poor function
- Introduction of elastic-stable intramedullary nailing (ESIN) produced very satisfactory functional results for unstable fractures
- External fixation reserved for open, comminuted or distal dia-metaphyseal fractures in older children/adolescents
- Proposes a 'primary definitive fracture care' algorithm matching method to fracture pattern
Freese et al. - Plate vs Intramedullary Fixation in Adolescents
- 102 adolescents (10-16 years) with diaphyseal both-bone fractures: 32 plated, 70 nailed
- Major complications in 55% of the intramedullary group vs none in the plate group
- 76% of nailed patients required open reduction of at least one bone; radial bow was smaller and more distal after nailing
- Second operation needed in 91% of nailed vs 3% of plated patients (mostly planned implant removal)
Price et al. - Outcome of Malunited Forearm Fractures in Children
- 39 skeletally immature children with malunited diaphyseal both-bone fractures followed a mean of 5 years 9 months (Monteggia/Galeazzi/greenstick excluded)
- 92% had good or excellent results despite residual angulation, complete displacement or loss of radial bow
- Only 9 of 39 had any loss of motion; age at injury did not correlate with recovery of rotation
- Distal fractures had a better prognosis than proximal fractures
Ko et al. - Predictors of Outcome After Chronic Monteggia Reconstruction
- 28 children reconstructed for chronic (missed) Monteggia with radial-head open reduction, ulnar osteotomy and annular ligament reconstruction
- Shorter interval from injury and lower skeletal maturity (Sauvegrain score) predicted better outcomes
- With low skeletal maturity and an interval of 7 months or less, ideal outcomes were achieved in 85.7% with no redislocation or arthritis
- Above skeletal ages of ~14 years (boys)/11.5 years (girls), reconstruction should be approached with great caution