Biceps Femoris Most Common | Grading I-III | Proximal Repair if Greater Than 2cm Retraction
- Biceps femoris long head (BFlh) most commonly injured - eccentric loading at late swing phase
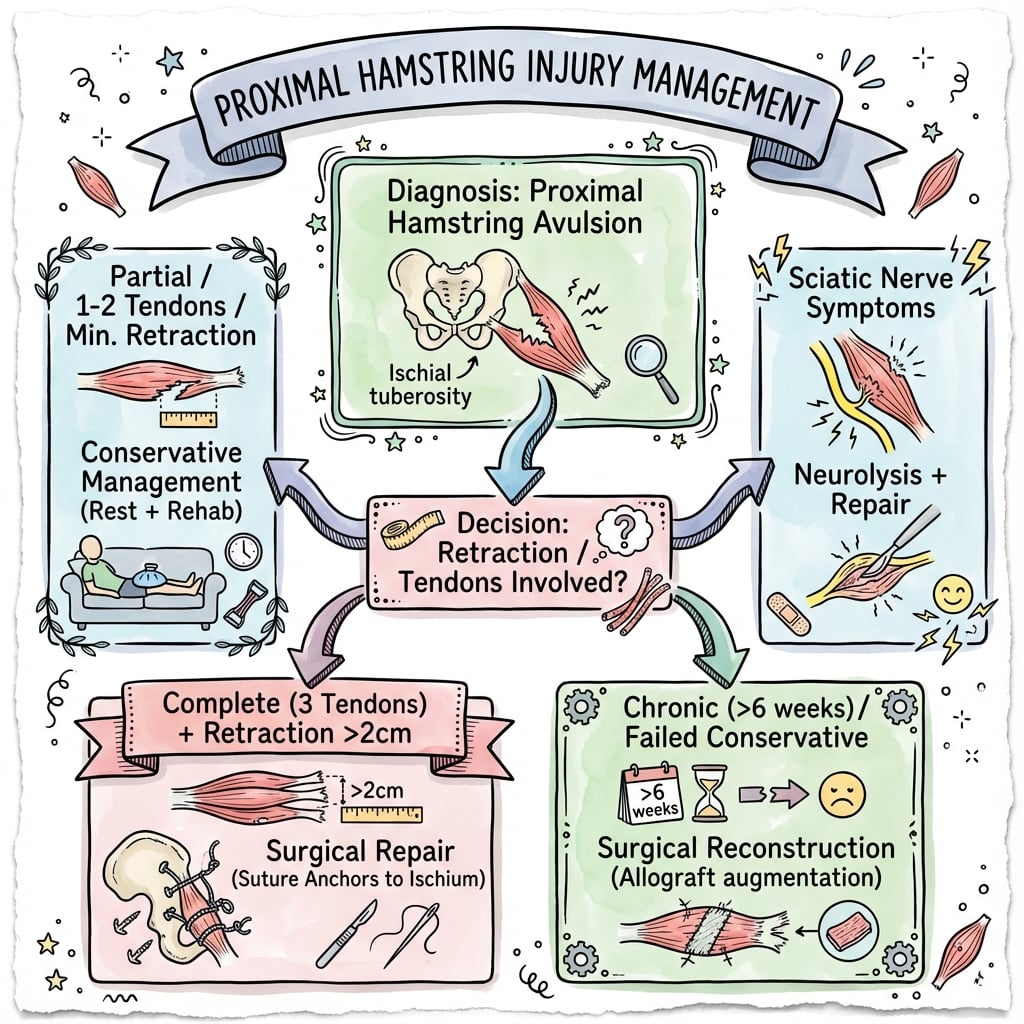
- Proximal hamstring avulsion requires surgical repair if greater than 2cm retraction or more than 2 tendons
- MRI essential for surgical planning - measure retraction distance and number of tendons involved
- Nordic hamstring exercises are evidence-based for prevention and rehabilitation
- Return to sport requires hamstring:quadriceps ratio greater than 0.8 and Askling H-test negative
- “Hamstring injuries peak at late swing phase (eccentric contraction during deceleration)
- “Proximal avulsion off ischial tuberosity more common in water-skiing, splits injuries
- “Mid-substance tears (myotendinous junction) more common in sprinting, kicking sports
- “Bent-knee stretch test distinguishes proximal (positive) from mid-substance (negative) tears
Three muscles: semimembranosus (SM), semitendinosus (ST), biceps femoris long head (BFlh). BFlh most commonly injured (80%) due to dual innervation (tibial + peroneal) causing uncoordinated contraction. Eccentric load during late swing phase of running.
Grade I: Mild strain, less than 10% fibres disrupted. Grade II: Moderate partial tear, 10-50% disruption. Grade III: Complete tear or proximal avulsion. MRI confirms grading - Grade II shows feathery oedema, Grade III shows gap and retraction.
Proximal hamstring avulsion: Surgery if retraction greater than 2cm OR more than 2 tendons avulsed OR failure of conservative management. Acute repair (within 4 weeks) has better outcomes than delayed. Use suture anchors to ischial tuberosity.
Functional criteria mandatory: H:Q ratio greater than 0.8, Askling H-test negative, pain-free sprinting, return to sport-specific drills. Premature return (within 3 weeks for Grade II) leads to 34% re-injury rate. Minimum 6 weeks for Grade II, 12 weeks post-op for Grade III.
- Clinical Features
- Mild pain, minimal loss of motion, able to walk normally
- Treatment
- RICE, gentle stretching, progressive loading
- Return Timeline
- 2-3 weeks (when Askling test negative)
- Clinical Features
- Moderate pain, palpable defect, limp, reduced ROM
- Treatment
- Conservative: progressive eccentric exercises, Nordic hamstrings
- Return Timeline
- 4-8 weeks (functional criteria essential)
- Clinical Features
- Severe pain, bruising, weakness, positive bent-knee test
- Treatment
- Conservative trial (non-operative) with close monitoring
- Return Timeline
- 12-16 weeks (may need surgery if fails)
- Clinical Features
- Complete loss of hamstring contour, palpable gap, severe weakness
- Treatment
- URGENT surgical repair (within 4 weeks optimal)
- Return Timeline
- 12 weeks minimum post-op (functional testing required)
- Clinical Features
- Persistent weakness, sitting pain (ischial), functional limitation
- Treatment
- Delayed surgical reconstruction (may need graft augmentation)
- Return Timeline
- 16-24 weeks post-op (lower success than acute)
BICEPSBICEPS - The Most Injured Hamstring
Hook:BICEPS is the muscle that gets injured when you sprint - think of the biceps femoris as the sprint muscle with dual innervation making it vulnerable!
NORDICNORDIC - Evidence-Based Prevention and Rehab
Hook:NORDIC exercises are the gold standard for both preventing and rehabilitating hamstring injuries - remember the H:Q ratio of 0.8!
Overview and Epidemiology
Hamstring injuries are among the most common muscle injuries in sport, particularly affecting sprinters, footballers (AFL, soccer, rugby), and track athletes. The injury spectrum ranges from mild muscle strains to complete proximal avulsions requiring surgical repair.
- Incidence: 12-16% of all sports injuries in running-based sports
- Peak age: 20-40 years (peak athletic participation)
- Gender: Male to female ratio approximately 2:1 (higher male participation in sprinting sports)
- Location:
- Biceps femoris long head: 80% of injuries
- Semimembranosus: 15%
- Semitendinosus: 5%
- Eccentric overload: Late swing phase of sprinting (muscle lengthening under load)
- Sudden acceleration/deceleration: Change of direction, explosive sprinting
- Proximal avulsion: Extreme hip flexion with knee extension (splits, water-skiing)
- Chronic overuse: Accumulation of microtears in high-volume training
The biceps femoris long head has dual innervation (tibial nerve to medial portion, common peroneal nerve to lateral portion), leading to uncoordinated muscle activation. It also has the longest fascicle length and greatest excursion during running, making it most susceptible to eccentric injury at the myotendinous junction.
Sport-specific burden:
- Football codes: Hamstring injuries account for approximately 15-20% of all injuries in elite running-and-kicking sport (e.g. AFL, soccer, rugby)
- Time loss: Average 3-4 weeks missed playing time for a Grade II injury
- Re-injury burden: 34% re-injury rate if returned within 3 weeks (premature return)
Pathophysiology and Mechanisms
Hamstring muscle group:
The posterior thigh muscles consist of three distinct muscles:
- Origin
- Ischial tuberosity (medial facet)
- Insertion
- Fibular head
- Innervation
- Tibial nerve (medial) + Common peroneal (lateral)
- Function
- Knee flexion, hip extension
- Origin
- Ischial tuberosity (medial facet)
- Insertion
- Proximal medial tibia (pes anserinus)
- Innervation
- Tibial nerve
- Function
- Knee flexion, hip extension, tibial internal rotation
- Origin
- Ischial tuberosity (lateral facet)
- Insertion
- Posterior medial tibial condyle
- Innervation
- Tibial nerve
- Function
- Knee flexion, hip extension
The biceps femoris long head (BFlh) has dual innervation from both the tibial nerve (L5, S1, S2) and the common peroneal nerve (L4, L5, S1), creating a neuromuscular coordination challenge. The medial and lateral portions contract with slightly different timing, predisposing to microtears at the myotendinous junction during high-speed eccentric loading.
Biomechanics of injury:
Late swing phase of running (70-80% of gait cycle): hamstring muscle lengthens while contracting to decelerate the leg. Peak force occurs just before foot strike. This eccentric load (up to 2.5x body weight) exceeds muscle capacity in fatigue.
Most common tear location (Grade I-II): junction between muscle belly and proximal tendon. This zone has poorest blood supply and highest mechanical stress concentration during eccentric loading.
Ischial tuberosity avulsion (Grade III): occurs with extreme hip flexion + knee extension (splits, water-skiing, martial arts kicks). Complete separation of one or more tendons from bony insertion. Requires surgical repair if greater than 2cm retraction.
Modifiable: Inadequate warm-up, previous hamstring injury (greatest risk factor), hamstring weakness (H:Q ratio less than 0.6), fatigue, limited flexibility. Non-modifiable: Age greater than 30, previous injury, BFlh anatomy (long fascicles).
Blood supply:
- Perforating branches of profunda femoris artery
- Inferior gluteal artery (proximal portion)
- Myotendinous junction has relatively poor vascularity (watershed zone)
Phase of running cycle:
- Hamstring Activity
- Minimal activity
- Risk
- Low risk
- Hamstring Activity
- Concentric contraction (hip extension)
- Risk
- Low risk
- Hamstring Activity
- Eccentric contraction (deceleration)
- Risk
- HIGH RISK - peak injury phase
- Hamstring Activity
- Isometric contraction
- Risk
- Low risk
Classification Systems
British Athletics Muscle Injury Classification (BAMIC)
The standard grading system for hamstring muscle injuries:
- MRI Findings
- Normal MRI, no oedema
- Clinical Features
- Hamstring tightness, no structural injury
- Return Time
- 1-3 days
- MRI Findings
- Less than 10% cross-sectional area, feathery oedema
- Clinical Features
- Mild pain, minimal strength loss, able to continue activity
- Return Time
- 2-3 weeks
- MRI Findings
- 10-50% cross-sectional area, visible fibre disruption
- Clinical Features
- Moderate pain, palpable defect, significant strength loss, limp
- Return Time
- 4-8 weeks
- MRI Findings
- Greater than 50% or complete tear, gap visible
- Clinical Features
- Severe pain, visible deformity, complete loss of function
- Return Time
- 12+ weeks or surgery
MRI is mandatory for accurate grading and surgical planning. T2-weighted sequences show muscle oedema (bright signal). Measure: (1) Cross-sectional area involved (percentage), (2) Longitudinal length of injury, (3) Retraction distance (for Grade III). These measurements predict return-to-sport timeline.
The Actual BAMIC Grading (Grades 0-4 with Site Suffix)
The table above is the traditional three-grade strain model. The British Athletics Muscle Injury Classification (Pollock 2014), in this topic's evidence base, is the contemporary MRI-based system examiners now expect, because it adds prognostic resolution the old model lacks: it grades injuries 0-4 and appends a site suffix (a/b/c) to grades 1-4 indicating where in the muscle-tendon unit the injury sits.
- MRI extent
- 0a: MRI normal / 0b: oedema only, no architectural disruption
- Site suffix (grades 1-4)
- No suffix
- MRI extent
- Small injury
- Site suffix (grades 1-4)
- a / b / c
- MRI extent
- Moderate injury
- Site suffix (grades 1-4)
- a / b / c
- MRI extent
- Extensive injury
- Site suffix (grades 1-4)
- a / b / c
- MRI extent
- Complete tear (muscle or tendon)
- Site suffix (grades 1-4)
- a / b / c
The suffix is the key prognostic refinement:
- a (myofascial): at the muscle periphery/fascia - generally the shortest recovery.
- b (musculo-tendinous): at the myotendinous junction - intermediate.
- c (intratendinous): involves the central/intramuscular tendon - the longest recovery and a higher re-injury risk, even at the same grade.
For a given grade, an intratendinous ('c') injury - one involving the central tendon - takes substantially longer to return and carries a higher re-injury risk than a myofascial ('a') injury of the same grade. Reporting the BAMIC site suffix, not just the grade, is the modern, examinable refinement over the traditional Grade I-III strain model.
MPCGRADING - Muscle Strain Classification
Hook:MPC = Mild, Partial, Complete - the three grades you MUST know for hamstring classification!
Clinical Presentation and Assessment
History:
- Sprinting/acceleration: Mid-substance or proximal MTJ tear
- Sudden deceleration/change direction: Eccentric overload
- Extreme hip flexion + knee extension: Proximal avulsion (splits, water-skiing)
- Acute pop or tear sensation: Suggests Grade II-III
- Pain location: Posterior thigh (mid-substance) vs ischial/buttock (proximal)
- Severity: Mild (continue playing) vs severe (immediate cessation)
- Functional loss: Inability to sprint, kick, or accelerate
- Previous injury: Most significant risk factor for re-injury
Physical examination:
- Grade I
- Normal or minimal limp
- Grade II
- Antalgic gait, avoids heel strike
- Grade III/Avulsion
- Severe limp, unable to bear weight
- Grade I
- Minimal swelling
- Grade II
- Swelling, bruising appears 24-48h
- Grade III/Avulsion
- Visible deformity, loss of hamstring contour, extensive bruising
- Grade I
- Tender but no defect
- Grade II
- Palpable defect, tender area
- Grade III/Avulsion
- Large palpable gap, ischial tenderness
- Grade I
- Minimal limitation, pain at end range
- Grade II
- Limited active knee flexion, painful passive stretch
- Grade III/Avulsion
- Severe limitation, unable to flex knee against gravity
- Grade I
- 4 out of 5 (mild weakness)
- Grade II
- 3 out of 5 (moderate weakness)
- Grade III/Avulsion
- 1-2 out of 5 or complete loss of function
Askling H-Test (Return to Sport Clearance)
Purpose: Functional assessment for return-to-sport readiness
- Patient standing, hip neutral
- Actively flex knee maximally (heel to buttock)
- Extend hip while maintaining knee flexion
- Hold position for 5 seconds
- Pain or discomfort during test
- Unable to complete full range
- Apprehension or fear of injury
- Negative test (pain-free): Safe to return to sport
- Positive test: Continue rehabilitation, re-test weekly
The Askling H-test is the gold standard functional test. Athletes must pass (pain-free) before returning to sprinting or sport. Sensitivity 80%, specificity 85% for predicting safe return. Combine with H:Q strength ratio greater than 0.8 for optimal decision-making.
Chronic sitting pain (ischial discomfort) is pathognomonic for proximal hamstring pathology. If a patient reports pain sitting on hard surfaces, especially weeks after injury, think proximal avulsion or incomplete healing. This indicates surgical consultation is warranted.
Differential diagnosis of posterior thigh / ischial pain:
- Distinguishing Features
- Acute sprinting/eccentric mechanism, mid-posterior thigh pain, palpable defect, pain on resisted knee flexion
- Key Investigation
- MRI (feathery oedema, cross-sectional area)
- Distinguishing Features
- Pop with hip flexion/knee extension, ischial bruising, weakness, chronic sitting pain, bowstring sign
- Key Investigation
- MRI (retraction distance, number of tendons)
- Distinguishing Features
- Insidious deep buttock pain at the ischium, worse with sitting and sprinting, no acute tear; overuse
- Key Investigation
- MRI/ultrasound (tendinosis, no discontinuity)
- Distinguishing Features
- Skeletally immature athlete, sudden pain with sprint/kick, bony fragment off ischium
- Key Investigation
- Plain radiograph (displaced apophysis)
- Distinguishing Features
- Back pain, dermatomal radiation below knee, positive straight-leg raise, neurological signs, no localised tenderness
- Key Investigation
- MRI lumbar spine
- Distinguishing Features
- Buttock pain with neuropathic quality, no true weakness on isolated knee flexion, provocative sciatic tests
- Key Investigation
- MRI, dynamic ultrasound, diagnostic injection
- Distinguishing Features
- Posterior hip/buttock pain in adduction/extension, narrowed ischiofemoral space, quadratus femoris oedema
- Key Investigation
- MRI (ischiofemoral and quadratus femoris space)
- Distinguishing Features
- Calf/thigh swelling, no clear injury, risk factors; must not be missed
- Key Investigation
- Doppler ultrasound
Investigations
Imaging protocol:
Hamstring Injury Imaging Pathway
Initial assessment based on history and physical examination. Determine severity clinically. Imaging not required for Grade 0-I if diagnosis clear.
Indications: Grade II or suspected Grade III, surgical planning needed, elite athlete. Sequences: T2-weighted (shows oedema), T1-weighted (shows anatomy), coronal and axial views. Measure: Cross-sectional area involved, longitudinal extent, retraction distance (if Grade III).
Dynamic assessment: Real-time imaging, operator-dependent. Can assess tendon retraction, haematoma. Less sensitive than MRI for muscle oedema. Useful for serial monitoring of healing.
If not progressing: Reassess with MRI to check healing. Persistent oedema or enlarging gap suggests need for intervention. Serial ultrasound for monitoring rehabilitation progress.
MRI findings by grade:
- T2 Signal
- Feathery high signal, less than 10% area
- Muscle Architecture
- Muscle fibres intact
- Measurements Required
- Note location, no measurement needed
- T2 Signal
- High signal, 10-50% area, partial fibre disruption
- Muscle Architecture
- Partial gap, some fibres torn
- Measurements Required
- Measure cross-sectional area percentage, length
- T2 Signal
- Complete gap, retracted tendon, haematoma
- Muscle Architecture
- Complete disruption, visible retraction
- Measurements Required
- Measure retraction distance from ischial tuberosity, count tendons involved
For proximal avulsion, MRI must document: (1) Number of tendons avulsed (ST, SM, BFlh), (2) Retraction distance (measure from ischial tuberosity to proximal tendon edge on coronal view), (3) Muscle quality (fatty infiltration suggests chronic injury), (4) Haematoma size. These factors guide surgical approach and prognosis.
Other investigations:
- X-ray: Only if concern for ischial tuberosity avulsion fracture (rare, adolescents)
- CT: Not routinely indicated
- Diagnostic ultrasound: Useful for serial monitoring, less detailed than MRI
Management Algorithm
Non-Operative Management (Grade I-II)
Goal: Progressive loading to restore strength and prevent re-injury
Rehabilitation Timeline
RICE protocol: Rest from aggravating activities, Ice 15-20 minutes every 2-3 hours, Compression bandage, Elevation. Pain management: NSAIDs (ibuprofen 400mg TDS) for 3-5 days. Gentle ROM: Pain-free knee flexion/extension, avoid stretching. Crutches if needed: For Grade II with significant limp.
Isometric exercises: Pain-free hamstring contractions (seated knee flexion against resistance). Gentle stretching: Pain-free range, no aggressive stretching (delays healing). Progressive walking: Increase distance and speed as tolerated. Pool exercises: Aqua jogging (unloaded).
Nordic hamstring curls: 3 sets of 5-8 reps, 3x per week (EVIDENCE-BASED). Single-leg deadlifts: Eccentric loading with control. Progressive resistance: Increase load as strength improves. Avoid explosive movements: No sprinting or kicking yet.
Running progression: Light jogging → straight-line sprinting → change of direction. Plyometrics: Hopping, bounding (when Askling test negative). Sport drills: Kicking, acceleration (sport-specific). Strength testing: H:Q ratio must be greater than 0.8.
Criteria for return: (1) Askling H-test negative, (2) H:Q ratio greater than 0.8, (3) Pain-free full sprinting, (4) Completed sport-specific drills without symptoms. Minimum time: 2-3 weeks (Grade I), 4-8 weeks (Grade II). Re-injury prevention: Continue Nordic hamstrings 2x per week indefinitely.
Premature return (within 3 weeks for Grade II) leads to 34% re-injury rate. Athletes who complete full rehabilitation (including eccentric strengthening) have re-injury rate of only 12%. The key is achieving functional criteria (strength, Askling test, pain-free sprinting), NOT just time-based clearance.

Surgical Technique - Proximal Repair Detail
Pre-operative planning:
- Sciatic nerve injury: 1-3% (numbness, weakness, permanent risk)
- Infection: 2-5% (superficial wound infection most common)
- Re-rupture: 5-10% (if non-compliant with post-op protocol)
- Persistent weakness: 10-20% (especially chronic repairs)
- Sitting discomfort: May persist for 6-12 months
- Failure to return to sport: 10-20%
- Suture anchors: 5.5mm x 3-5 anchors (plan for ischial tuberosity)
- Sutures: No.2 non-absorbable (Fiberwire or Ethibond)
- Retractors: Deep retractors for gluteus maximus and sciatic nerve
- Imaging: C-arm for anchor placement (lateral view confirms depth)
- Hip brace: Post-operative brace limiting flexion to 60 degrees
Detailed operative steps:
Step-by-Step Proximal Hamstring Repair
- Prone position on radiolucent table (allows C-arm access)
- Chest padding: Reduce pressure on chest and abdomen
- Pelvic bolsters: Support pelvis, allow hip mobility
- Knees padded: Protect patellae
- Arms: Positioned on arm boards or alongside body
- Wide prep from lumbar spine to mid-thigh bilaterally
- Include perineum in field (ischial access)
- Transparent adhesive drape for visualization
- Palpate ischial tuberosity (bony prominence inferior to gluteal fold)
- Transverse incision (preferred) or longitudinal
- Centered over ischial tuberosity, 8-12cm length
- Deepen through subcutaneous fat
- Split gluteus maximus longitudinally along fibre direction
- Blunt dissection to avoid bleeding
- Identify sciatic nerve (lateral border of incision, deep to glut max)
- Place deep retractor to protect nerve (retract laterally)
Proper positioning and surgical approach are critical for safe access to the ischial tuberosity while protecting neurovascular structures.
Intraoperative troubleshooting:
- Cause
- Extensive retraction (greater than 10cm)
- Solution
- Extend incision distally, palpate along posterior thigh
- Cause
- Chronic retraction, scarring
- Solution
- Consider allograft augmentation or accept tension
- Cause
- Nerve adherent to scar or stretched
- Solution
- Mobilize nerve carefully, may need external neurolysis
- Cause
- Poor bone quality or incorrect angle
- Solution
- Re-drill, use larger anchor, or add additional anchor
SURGICALSURGICAL - Indications for Proximal Repair
Hook:SURGICAL criteria for proximal hamstring avulsion - greater than 2cm retraction is the key threshold!
Complications
- Incidence
- 12-34%
- Risk Factors
- Premature return, inadequate rehab, previous injury
- Management
- Prevention: Nordic hamstrings, functional criteria, minimum 6 weeks
- Incidence
- 5-15%
- Risk Factors
- Incomplete healing, inadequate rehab
- Management
- Extended physiotherapy, consider PRP injection, surgical consultation
- Incidence
- 1-3%
- Risk Factors
- Intraoperative traction, anchor malposition
- Management
- Observation (most resolve), EMG at 6 weeks, neurosurgery if persistent
- Incidence
- 2-5%
- Risk Factors
- Deep dissection, haematoma
- Management
- Antibiotics, drainage if collection, debridement if deep
- Incidence
- 5-10%
- Risk Factors
- Non-compliance with brace, premature loading
- Management
- Prevention: strict brace protocol 6 weeks, controlled rehab
- Incidence
- 10-15%
- Risk Factors
- Incomplete haemostasis
- Management
- Observation if small, aspiration if large, drain if recurrent
- Incidence
- 20-40% (6-12 months)
- Risk Factors
- Ischial tuberosity sensitivity, hardware prominence
- Management
- Cushioned seating, time (resolves in 80%), hardware removal if persistent
Re-injury risk remains elevated for approximately 15 weeks after return to play (Orchard 2020), and a recent prior hamstring injury is by far the strongest risk factor (adjusted OR 13.1). The key prevention strategies: (1) Nordic hamstring exercises (approximately 70% reduction in overall injury and approximately 85% reduction in recurrence, Petersen 2011), (2) Functional testing before clearance (Askling test, H:Q ratio), (3) Continued eccentric loading and load monitoring well beyond clearance (4-8 weeks Grade II, 12+ weeks post-op).
Platelet-Rich Plasma and Biologic Injections
PRP appears repeatedly in this topic as an "option" (the complications table, the recurrent-injury scenario, the alternative-treatments list), so the evidence deserves to be stated plainly rather than left as a question.
What the evidence shows. For acute hamstring muscle injury, placebo-controlled randomised trials and subsequent meta-analyses have not shown that PRP shortens return-to-play time or reduces re-injury compared with a structured rehabilitation programme (with or without a blinded placebo injection). The early enthusiasm was not borne out once PRP was tested against blinded saline controls.
Practical position. PRP is therefore not recommended as routine treatment for acute hamstring strain; the intervention with robust (Level 1) evidence remains progressive eccentric loading (the Nordic programme), supported by criterion-based return to play. PRP and other biologics may still be discussed with elite athletes under shared decision-making, but without an evidence-based expectation of faster or safer return.
The high-yield answer to "what is the evidence for PRP in hamstring injury?" is that blinded, placebo-controlled trials have not shown a benefit in return-to-play or re-injury for acute hamstring strain. Do not offer it as standard care - anchor management on eccentric rehabilitation and functional return criteria.
Postoperative Care and Rehabilitation
Post-Surgical Protocol (Proximal Hamstring Repair)
- Brace: Hip brace limiting flexion to 60 degrees (worn at all times except exercises)
- Weight-bearing: Toe-touch weight-bearing with crutches for 2 weeks
- ROM: Passive knee flexion/extension (no hip flexion beyond 60 degrees)
- Wound care: Keep dry, staples removed at 14 days
- Pain management: Paracetamol + tramadol (avoid NSAIDs - may impair healing)
- DVT prophylaxis: Enoxaparin 40mg daily for 14 days (extended if high risk)
- Brace: Continue hip brace (flexion limit 60 degrees)
- Weight-bearing: Progress to full weight-bearing as tolerated
- ROM: Gradually increase hip flexion (10 degrees per week target)
- Exercises: Isometric hamstring contractions (seated), quadriceps strengthening
- Pool therapy: Aqua walking (week 4+) for unloaded ROM
- No stretching: Avoid aggressive hamstring stretching (delays healing)
- Brace: Wean off brace at 6 weeks (if ROM adequate)
- ROM: Full hip flexion goal by 8 weeks
- Strengthening: Begin Nordic hamstring curls (3x per week)
- Progressive resistance: Single-leg deadlifts, hamstring curls
- Cycling: Stationary bike for endurance (low resistance)
- Avoid: Running, jumping, explosive movements
- Running progression: Light jogging on treadmill, progress to outdoor
- Eccentric focus: Continue Nordic hamstrings (key to success)
- Strength testing: H:Q ratio should be greater than 0.7 by 16 weeks
- Plyometrics: Hopping, bounding (if Askling test negative)
- Functional drills: Sport-specific movements
- Criteria for return:
- Askling H-test negative (pain-free)
- H:Q ratio greater than 0.8 (isokinetic testing)
- Pain-free full sprinting
- Completed sport-specific drills without symptoms
- Minimum time: 4-6 months post-surgery for high-demand athletes
- Ongoing: Continue Nordic hamstrings 2x per week indefinitely
Key rehabilitation principles:
- Strict brace compliance for 6 weeks (prevents re-rupture)
- Nordic hamstring curls from week 6 onwards (evidence-based)
- Progressive loading - increase gradually, monitor symptoms
- Functional testing before return (objective criteria)
- NO aggressive stretching first 12 weeks (delays healing)
- NO premature return (minimum 4 months for athletes)
- NO running before 12 weeks post-op
- DO NOT ignore pain - pain indicates excessive loading
Outcomes and Prognosis
Outcomes of conservative management (Grade I-II):
- Return to Sport
- 95-100% at 2-3 weeks
- Re-injury Risk
- 10-15%
- Key Prognostic Factor
- Compliance with Nordic exercises
- Return to Sport
- 85-95% at 6-8 weeks
- Re-injury Risk
- 20-34%
- Key Prognostic Factor
- Time to return (longer is better)
Athletes who return after 6 weeks for Grade II injuries have 12% re-injury rate, compared to 34% re-injury if returned within 3 weeks. Every additional week of rehabilitation reduces re-injury risk by approximately 5%. Functional criteria (H:Q ratio, Askling test) are more important than time alone.
Outcomes of surgical repair (proximal avulsion):
- Return to Sport
- 90-95%
- Strength Recovery
- 90-100% (isokinetic testing)
- Patient Satisfaction
- Excellent (90%)
- Return to Sport
- 80-90%
- Strength Recovery
- 80-90%
- Patient Satisfaction
- Good (80%)
- Return to Sport
- 65-80%
- Strength Recovery
- 70-80%
- Patient Satisfaction
- Fair (70%)
Prognostic factors for good outcome:
- Acute repair (within 4 weeks of injury)
- 2 or fewer tendons involved (vs complete 3-tendon)
- No muscle atrophy or fatty infiltration on MRI
- Young patient (less than 40 years)
- Compliant with post-op protocol (brace, restricted ROM)
- Nordic hamstring exercise program maintained
- Delayed repair (greater than 12 weeks)
- Complete 3-tendon avulsion with extensive retraction
- Chronic muscle changes (atrophy, fatty infiltration)
- Older patient (greater than 50 years)
- Non-compliance with rehabilitation
- Premature return to high-demand activities
Long-term outcomes:
- Sitting discomfort: Resolves in 80% by 12 months, 20% have persistent mild discomfort
- Strength: 90-95% recovery in acute repairs, 70-80% in chronic
- Return to pre-injury level: 85-90% in acute repairs
Guidelines, Registries & Global Practice
Global epidemiology (PubMed-backed):
- Figure
- Most frequent and most prevalent injury
- Source population / evidence
- AFL surveillance 1992-2012 (Orchard 2013, PMID 23460329)
- Figure
- Approximately 26% (historically up to 25-26% before modern prevention)
- Source population / evidence
- AFL surveillance (Orchard 2013)
- Figure
- Elevated for approximately 15 weeks; approximately 9% in first match back
- Source population / evidence
- AFL cohort 1992-2014 (Orchard 2020, PMID 32024646)
- Figure
- Recent (8 weeks or less) prior hamstring injury, adjusted OR 13.1
- Source population / evidence
- Orchard 2020
- Figure
- Approximately 70% reduction overall, approximately 85% reduction in recurrence
- Source population / evidence
- Petersen 2011 RCT (PMID 21825112)
Hamstring strain injury is consistently the single most common time-loss injury across football codes worldwide (soccer, rugby, AFL, American football, Gaelic football), so the principles below are examinable on any board.
Major guidance and consensus, side by side:
- Position
- Use MRI grade 0-4 with myofascial/musculotendinous/intratendinous suffix for prognosis; intratendinous injuries take longest
- Evidence level
- Expert/classification (Level 5), validation ongoing
- Position
- Criterion-based return to play (clinical, strength symmetry, Askling H-test); MRI normalisation NOT required before return
- Evidence level
- Level 2 (systematic reviews, Reurink 2014 / Hickey 2017)
- Position
- Eccentric Nordic hamstring loading recommended for primary and secondary prevention in high-risk sport
- Evidence level
- Level 1 (cluster RCT, Petersen 2011)
- Position
- Repair complete/displaced avulsions (commonly cited greater than 2cm retraction or 2-3 tendons); acute repair superior to delayed
- Evidence level
- Level 3 (meta-analysis, Bodendorfer 2018)
The widely quoted "greater than 2cm retraction / more than 2 tendons" surgical threshold is a pragmatic consensus, not a randomised finding - no high-quality RCT compares operative with nonoperative treatment of proximal avulsion. The robust evidence is that (1) Nordic eccentric training prevents injury (Level 1), and (2) acute repair outperforms delayed repair (Level 3 meta-analysis).
Registry / surveillance evidence:
Hamstring injury has no implant registry; the equivalent high-volume datasets are prospective sports-injury surveillance systems - the AFL injury surveillance database (Orchard, 20+ seasons), UEFA Elite Club Injury Study (European soccer), and various national rugby and athletics audits. These consistently identify hamstring strain as the dominant time-loss injury and a high-recurrence problem, which is what drives the global emphasis on eccentric prevention and criterion-based return.
Global practice variation:
- Imaging access: MRI grading (BAMIC) is routine in elite/high-resource settings; in limited-resource settings, clinical grading and ultrasound guide management, with similar core rehabilitation principles.
- Return-to-play culture: Professional codes increasingly mandate objective functional clearance (strength symmetry, Askling H-test) rather than fixed time, whereas amateur practice still leans on symptom resolution alone.
- Surgery for proximal avulsion: Performed selectively worldwide for complete/displaced avulsions; thresholds and timing differ by surgeon and access, but acute referral is universally favoured because outcomes deteriorate with delay.
Medicolegal and consent considerations (universal):
Key documentation for hamstring surgery (applicable in any jurisdiction):
- Detailed informed consent including sciatic nerve injury risk (1-3%)
- MRI measurements documenting retraction distance and number of tendons avulsed
- Explanation of conservative alternatives and expected outcomes, including the approximately 23% overall complication rate after repair (Bodendorfer 2018)
- Clear documentation of functional deficit (strength testing, gait assessment)
- Post-operative protocol explained (brace compliance, weight-bearing restrictions)
- Common litigation themes: sciatic nerve palsy (inadequate warning), re-rupture (premature loading), persistent weakness (unrealistic expectations)
MCQ Practice Points
Q: Which hamstring muscle is most commonly injured and why? A: Biceps femoris long head (80% of injuries) due to: (1) Dual innervation (tibial + common peroneal nerves) causing uncoordinated contraction, (2) Longest fascicle length and greatest excursion during running, (3) Most eccentric loading at late swing phase. Injury typically occurs at the proximal myotendinous junction.
Q: What are the criteria for Grade II hamstring muscle strain? A: Grade II: (1) 10-50% cross-sectional area involvement on MRI, (2) Partial muscle fibre disruption with visible gap, (3) Feathery high signal on T2 MRI, (4) Clinical: Moderate pain, palpable defect, strength 3 out of 5, limp present. Return time: 4-8 weeks with appropriate rehabilitation.
Q: What are the indications for surgical repair of proximal hamstring avulsion? A: (1) Retraction greater than 2cm measured on MRI, (2) More than 2 tendons completely avulsed, (3) Complete 3-tendon avulsion (regardless of retraction), (4) Failed conservative trial (3 months) with persistent functional deficit, (5) Elite athlete with high functional demands. Acute repair (within 4 weeks) has better outcomes than chronic reconstruction.
Q: What MRI findings predict longer return-to-sport time after hamstring injury? A: (1) Greater cross-sectional area involvement (greater than 25% = longer return), (2) Longitudinal extent greater than 10cm, (3) Proximal MTJ location (vs distal MTJ), (4) Complete tear with retraction (Grade III). MRI performed within 5 days accurately predicts timeline: less than 10% area = 17 days, 10-50% = 42 days, greater than 50% = 73+ days.
Q: What is the evidence for Nordic hamstring exercises in injury prevention? A: Petersen et al (2011) cluster RCT showed: (1) overall acute hamstring injury rate fell from 13.1 to 3.8 per 100 player-seasons (adjusted rate ratio 0.29, approximately 70% reduction), (2) recurrent injury rate fell from 45.8 to 7.1 per 100 player-seasons (rate ratio 0.14, approximately 85% reduction), (3) number needed to treat 13 overall and 3 to prevent one recurrence, (4) progressive eccentric Nordic loading programme. This is the gold standard evidence-based prevention and rehabilitation exercise.
Q: What are the functional criteria for return to sport after Grade II hamstring strain? A: (1) Askling H-test negative (pain-free active knee flexion with hip extension), (2) H:Q ratio greater than 0.8 (isokinetic testing - hamstring:quadriceps strength ratio), (3) Pain-free full sprinting at match speed, (4) Completed sport-specific drills without symptoms, (5) Minimum time: 4-8 weeks for Grade II (NOT 3 weeks). Premature return (within 3 weeks) leads to 34% re-injury vs 12% with adequate rehabilitation.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 26-year-old professional AFL footballer presents 24 hours after experiencing sudden posterior thigh pain while sprinting during a match. He felt a 'pop' and was unable to continue. On examination, he has a palpable defect in the mid-posterior thigh, tenderness over the biceps femoris, and reduced strength (3 out of 5) on resisted knee flexion. He can walk with a limp. What is your assessment and initial management?”
“A 35-year-old recreational water skier presents 1 week after sustaining an injury during a fall. He felt severe pain in the buttock and posterior thigh, heard a 'pop', and had immediate loss of function. MRI shows complete avulsion of all three hamstring tendons from the ischial tuberosity with 4cm of retraction. He is currently unable to flex his knee against gravity and has severe weakness. Walk me through your surgical planning and technique.”
“A 28-year-old semi-professional soccer player presents with his third hamstring injury in 12 months, all to the same leg (left biceps femoris). He returned to sport 3 weeks after the previous injury. MRI shows Grade II strain with 25% cross-sectional area involvement at the proximal MTJ. He is frustrated and wants to 'just get surgery to fix it once and for all'. How do you manage this complex situation?”
Key Anatomy
- Biceps femoris long head (BFlh) = 80% of injuries (dual innervation: tibial + peroneal)
- Three muscles: ST (most medial), BFlh (lateral), SM (deep)
- Injury site: Proximal myotendinous junction (most common) or ischial avulsion
- Eccentric injury at late swing phase (70-80% of gait cycle)
Grading Classification
- Grade I: Less than 10% cross-sectional area, 2-3 weeks return
- Grade II: 10-50% area, 4-8 weeks return (functional criteria essential)
- Grade III: Greater than 50% or complete avulsion, surgery if greater than 2cm retraction
- MRI essential for grading and surgical planning
Treatment Algorithm
- Grade I-II: Conservative (RICE, Nordic hamstrings, functional criteria for return)
- Grade III with less than 2cm: Conservative trial (may heal)
- Grade III with greater than 2cm retraction: URGENT surgical repair (within 4 weeks)
- Complete 3-tendon avulsion: Surgical repair regardless of retraction
Surgical Pearls
- Prone position, transverse incision over ischial tuberosity
- PROTECT SCIATIC NERVE (lateral border, identify early, retract laterally)
- Horseshoe anchor pattern (5 anchors), angle medially away from nerve
- Tension repair: Hip neutral, knee 45 degrees flexion
- Post-op: Hip brace 60 degrees limit for 6 weeks, toe-touch 2 weeks
Complications and Prevention
- Re-injury: 34% if returned within 3 weeks, 12% with adequate rehab
- Sciatic nerve injury: 1-3% (post-op), most resolve spontaneously
- Nordic hamstring exercises: approximately 70% reduction in overall injury, approximately 85% in recurrence (Petersen 2011, EVIDENCE-BASED)
- Return criteria: Askling test negative, H:Q ratio greater than 0.8, pain-free sprinting
- Sitting pain post-op: 20-40% at 6 months (resolves in 80% by 12 months)
Evidence Base and Key Trials
Nordic Hamstring Exercise Prevention - Petersen et al (Landmark RCT)
- Cluster-randomised controlled trial of 50 Danish soccer teams (942 players) over one season
- 10-week progressive Nordic hamstring eccentric programme plus weekly maintenance vs usual training
- Overall acute hamstring injury rate 3.8 vs 13.1 per 100 player-seasons (adjusted rate ratio 0.29, 95% CI 0.15-0.57) - approximately 70% reduction
- Recurrent injury rate 7.1 vs 45.8 per 100 player-seasons (rate ratio 0.14) - approximately 85% reduction
- Number needed to treat: 13 to prevent any injury, 3 to prevent one recurrence
British Athletics Muscle Injury Classification (BAMIC) - Pollock et al (Defining Classification)
- Proposed an MRI-based grading system (grades 0-4) to replace the diagnostically limited 3-grade strain model
- Each grade 1-4 carries a suffix a/b/c denoting myofascial, musculotendinous or intratendinous site of injury
- Intratendinous (c) injuries (tendon involvement) carry a worse prognosis and longer return time
- Designed to improve prognostication and therapeutic decision-making over traditional grading
Operative vs Nonoperative Proximal Hamstring Avulsion - Bodendorfer et al (Meta-analysis)
- Systematic review and meta-analysis: 24 studies, 795 proximal hamstring avulsions
- Repair gave higher patient satisfaction (90.8% vs 52.9%) and hamstring strength (85.0% vs 64.0%) than nonoperative care (all P less than 0.001)
- Acute repair outperformed chronic repair (satisfaction 95.5% vs 83.8%; less pain; greater strength)
- Overall complication rate after repair 23.2%; complete-avulsion repair complication rate 29.4% vs 11.3% for partial
- Nonoperative comparison group was small, limiting the strength of the direct comparison
Functional Outcome After Proximal Hamstring Repair - Birmingham et al
- Retrospective series of 34 complete proximal hamstring avulsions (9 acute, 14 chronic repairs); 23 patients evaluated
- 21 of 23 returned to activity at a mean 95% of pre-injury level, at a mean of 9.8 months
- 18 excellent, 4 good, 1 fair subjective result
- Isokinetic hamstring strength averaged 90-93% of the uninvolved limb
- Minimal postoperative complications reported
Return-to-Play Criteria and Re-injury - Hickey et al (Systematic Review)
- Systematic review of 9 studies (601 acute hamstring strain injuries) on rehabilitation progression and return-to-play criteria
- Pain perception was used to guide rehabilitation progression across all studies
- Protocols using isokinetic dynamometry had the shortest return times (12-25 days)
- Protocols incorporating the Askling H-test had the lowest re-injury rates (1.3-3.6%)
- Called for more objective, criterion-based return-to-play decision-making
MRI at Return to Play of Recovered Hamstring Injuries - Reurink et al
- 53 athletes imaged within 5 days of injury and again within 3 days of return to play (51% grade 1, 49% grade 2)
- Median time to return to play was 28 days (range 12-76)
- 89% of clinically recovered athletes still showed increased intramuscular signal on fluid-sensitive MRI at return
- Normalisation of MRI signal is NOT required before safe return to play
- New low-signal (fibrous) tissue was seen in one-third at return; clinical significance uncertain
Two Decades of AFL Injury Surveillance - Orchard et al (Registry-scale epidemiology)
- Australian Football League injury surveillance 1992-2012 (4492 players, 13,606 new injuries)
- Hamstring strain was the most frequent and most prevalent injury (mean 6 per club per season; 20 missed matches per club per season)
- Hamstring strain recurrence rate averaged 26%
- Overall injury recurrence fell from 25% (1992) to 9% (2012) with surveillance and rule changes
- Public release of injury data supported rule changes targeting player safety
Fifteen-Week Recurrence Window - Orchard et al
- Prospective cohort: 3647 muscle strains (1932 hamstring) over 23 AFL seasons
- Recent (8 weeks or less) hamstring injury was by far the strongest risk factor for recurrence (adjusted OR 13.1, 95% CI 11.5-14.9)
- Non-recent prior hamstring injury still raised risk (adjusted OR 3.5)
- Recurrence risk was approximately 9% in the first match back and stayed elevated for 15 weeks after return
- Recent hamstring injury also raised the risk of subsequent quadriceps and calf strains