Extracapsular | Stable vs Unstable | SHS vs CMN | TAD under 25mm
- Extracapsular - blood supply preserved, low AVN risk
- Stability = posteromedial cortex - determines implant choice
- TAD under 25mm - prevents lag screw cutout
- Center-inferior screw position - optimal biomechanics
- Early surgery - within 24-48 hours reduces mortality
- “CMN for reverse oblique and unstable patterns
- “SHS requires intact lateral wall for stability
- “Lateral wall thickness greater than 20.5mm = stable
- “Shortened and externally rotated leg on presentation

Posteromedial cortex is KEY. Loss of lesser trochanter, reverse obliquity, or subtrochanteric extension = unstable = CMN.
Tip-Apex Distance under 25mm. Sum of AP + lateral distances. Center-inferior position optimal. TAD greater than 25mm = cutout.
SHS for stable patterns (intact medial buttress). CMN for unstable patterns (load-bearing independent of cortex).
Surgery within 24-48 hours. Delay greater than 48 hours increases mortality, pneumonia, pressure sores.
- Stability
- Stable
- Implant
- SHS or CMN
- Key Point
- Either acceptable, SHS cost-effective
- Stability
- Unstable
- Implant
- CMN
- Key Point
- Load-bearing fixation required
- Stability
- Unstable
- Implant
- CMN mandatory
- Key Point
- SHS causes medialization
- Stability
- Unstable
- Implant
- Long CMN
- Key Point
- Short nail = stress riser
STABLEStable Fracture Patterns
Hook:STABLE patterns = SHS is safe. If any letter is violated, use a CMN!
TADTAD Rule
Hook:Keep TAD under 25 to keep the screw alive!
REVERSECMN Indications
Hook:REVERSE the decision to use a plate - use a nail instead!
CCILag Screw Position
Hook:CCI - Center-Center or Center-Inferior. Superior = Cutout!
Overview and Epidemiology
Intertrochanteric fractures are extremely common and represent a major public health burden. Unlike femoral neck fractures, they are extracapsular so blood supply is preserved and AVN is rare. The key exam focus is stability assessment and implant selection.
- Elderly: Mean age 80+ years
- Female predominance: 3:1 ratio
- Osteoporosis: Primary risk factor
- Falls from standing: Most common mechanism
- 20-30% 1-year mortality
- Only 40-60% return to pre-fracture function
- Second hip fracture risk elevated
- Major global healthcare burden: ~1.6 million hip fractures/year worldwide, rising with population ageing
Bimodal Distribution
- Elderly (90%): Low-energy falls, osteoporotic bone
- Young (10%): High-energy trauma (MVA, fall from height)
Anatomy and Biomechanics
Key Anatomical Points

- Location
- Lateral, posterosuperior
- Clinical Significance
- Gluteus medius/minimus insertion, abductor function
- Location
- Medial, inferior
- Clinical Significance
- Iliopsoas insertion, medial buttress, stability marker
- Location
- Posteromedial cortex
- Clinical Significance
- Dense bone, resists compressive forces
- Location
- Anterior
- Clinical Significance
- Capsule insertion, extracapsular location
- Location
- Posterior
- Clinical Significance
- Quadratus femoris insertion
Unlike femoral neck fractures, intertrochanteric fractures are extracapsular. The blood supply from the medial femoral circumflex artery is NOT disrupted. AVN is extremely rare. Union rates exceed 95%.
Biomechanics
- Hip joint reaction force: 2.5-3x body weight walking
- Bending moment: On proximal femur
- Compression medially: Calcar resists
- Tension laterally: Lateral wall important
- Posteromedial cortex: KEY stability indicator
- Lesser trochanter: Medial buttress
- Lateral wall thickness: Greater than 20.5mm = stable
- Fracture obliquity: Reverse = unstable
Implant Biomechanics
- SHS (Sliding Hip Screw): Load-sharing device. Requires intact medial buttress to share load. Controlled collapse with healing. Fails if no medial support.
- CMN (Cephalomedullary Nail): Load-bearing device. Carries load independent of cortical integrity. Works even with comminution.
Classification Systems
Evans/Jensen Classification
- Pattern
- 2-part, undisplaced
- Stability
- Stable
- Treatment
- SHS or CMN
- Pattern
- 2-part, displaced
- Stability
- Stable
- Treatment
- SHS or CMN
- Pattern
- 3-part, greater trochanter
- Stability
- Unstable
- Treatment
- CMN preferred
- Pattern
- 3-part, lesser trochanter
- Stability
- Unstable
- Treatment
- CMN preferred
- Pattern
- 4-part, comminuted
- Stability
- Unstable
- Treatment
- CMN
- Pattern
- Fracture from medial proximal to lateral distal
- Stability
- Very unstable
- Treatment
- CMN mandatory
Can the fracture be anatomically reduced and provide a stable medial buttress? If NO (comminution, loss of lesser trochanter, reverse oblique) = Unstable = CMN.
Clinical Assessment
- Mechanism: Fall from standing (elderly), high-energy (young)
- Symptoms: Hip/groin pain, inability to weight-bear
- Pre-injury function: CRITICAL for surgical planning
- Comorbidities: Cardiac, respiratory, anticoagulation
- Look: Shortened (2-3cm), externally rotated leg
- Feel: Tenderness over greater trochanter
- Move: Unable to lift leg, pain with logroll
- NV: Distal pulses (rare injury to vessels)
Classic Presentation
Shortened and externally rotated leg - caused by unopposed pull of iliopsoas (flexion, external rotation) and gluteus medius (abduction). The leg appears 2-3cm shorter with 30-60° external rotation.
Important History Points
- Walking aids: Used prior to injury?
- Living situation: Independent, with family, nursing home?
- Cognitive status: Dementia increases mortality
- Anticoagulation: Warfarin, DOACs - reversal needed?
Differential Diagnosis
- Key Distinguishing Feature
- Shortened, externally rotated; extracapsular
- Imaging Clue
- Fracture line between trochanters, lesser trochanter fragment
- Why It Matters
- SHS vs CMN decision; AVN rare
- Key Distinguishing Feature
- Shortened, externally rotated; intracapsular
- Imaging Clue
- Fracture line within capsule, above intertrochanteric line
- Why It Matters
- AVN/non-union risk; arthroplasty often chosen in displaced fractures
- Key Distinguishing Feature
- Thigh deformity, proximal fragment flexed/abducted
- Imaging Clue
- Fracture within 5cm distal to lesser trochanter
- Why It Matters
- Long cephalomedullary nail; high stress zone
- Key Distinguishing Feature
- Pain on weight-bearing, normal initial X-ray
- Imaging Clue
- MRI (or CT) shows fracture not seen on plain film
- Why It Matters
- Missed diagnosis leads to displacement; image if clinical suspicion high
- Key Distinguishing Feature
- Low/no trauma, prior pain, known malignancy
- Imaging Clue
- Lytic lesion, cortical destruction at fracture site
- Why It Matters
- Staging, biopsy considerations, reconstruction nail
- Key Distinguishing Feature
- Localised tenderness, able to weight-bear partially
- Imaging Clue
- Isolated GT fragment, no intertrochanteric line
- Why It Matters
- Usually managed non-operatively
- Key Distinguishing Feature
- Pre-existing groin pain, no true deformity
- Imaging Clue
- Joint-space loss, no fracture line
- Why It Matters
- Avoid over-treatment; confirm no occult fracture
A patient with hip pain and inability to weight-bear after a fall, but a normal X-ray, may have an occult fracture. Plain radiographs miss up to 2-10% of hip fractures. If clinical suspicion persists, obtain an MRI (most sensitive) or CT before discharge. Missing it risks displacement and conversion of a simple fixation into an arthroplasty.
Investigations
Imaging Protocol
Both hips for comparison. AP pelvis plus cross-table lateral of affected hip. Assess fracture pattern, classification, and stability features.
Under sedation/analgesia to reduce fracture for better visualization of pattern and displacement.
For surgical planning in complex patterns, assessment of posterior comminution, or suspected pathological fracture.
Radiographic Assessment
- Significance
- Standard vs reverse oblique
- Implication
- Reverse = CMN mandatory
- Significance
- Attached vs separate fragment
- Implication
- Separate = loss of medial buttress
- Significance
- Intact vs comminuted
- Implication
- Comminuted = unstable
- Significance
- Greater or less than 20.5mm
- Implication
- Thin = CMN preferred
- Significance
- Present or absent
- Implication
- Present = long CMN needed
Preoperative Workup
- FBC: Baseline Hb (expect occult blood loss 500-1500ml)
- UEC: Renal function
- Coagulation: INR if on warfarin
- Group and Hold: 2 units PRBC
- ECG: Baseline cardiac status
- Cognitive screening: AMT, 4AT for delirium
- Nutritional status: Albumin, weight
- Medications review: Anticoagulation, polypharmacy
- ASA status: Anesthetic risk assessment
Management Algorithm
Surgery within 24-48 hours from admission. Delays beyond 48 hours associated with:
- Increased mortality
- Higher pneumonia rates
- More pressure sores
- Longer hospital stay
Medical optimization should NOT delay surgery beyond this window.
Implant Selection Decision Tree
Stable Fractures (Evans 1A/1B, AO 31-A1)
- 2-part fracture
- Intact posteromedial cortex
- Lesser trochanter attached
- Adequate lateral wall (greater than 20.5mm)
- Standard obliquity
- SHS or CMN - both acceptable
- SHS may be preferred (cost, simplicity, no shaft fracture risk)
- CMN acceptable if surgeon preference
Cochrane Review 2022: No difference in mortality or function between SHS and CMN for stable patterns. CMN has slightly higher reoperation rate for stable fractures (femoral shaft fracture risk).
Summary Table
- SHS Indicated
- Stable patterns
- CMN Indicated
- Unstable patterns
- SHS Indicated
- Intact
- CMN Indicated
- Comminuted
- SHS Indicated
- Attached
- CMN Indicated
- Detached
- SHS Indicated
- Standard
- CMN Indicated
- Reverse oblique
- SHS Indicated
- Greater than 20.5mm
- CMN Indicated
- Less than 20.5mm
- SHS Indicated
- No
- CMN Indicated
- Yes (long nail)
Surgical Technique
Patient Positioning
Setup Checklist
Supine on fracture table. Well-padded perineal post (avoid pudendal nerve injury). Contralateral leg in lithotomy holder or extended.
Apply traction and internal rotation to reduce fracture. Aim for slight valgus (5-10°) - do NOT accept varus. Confirm reduction on AP and lateral fluoroscopy.
Ensure adequate access for AP and lateral views. The lateral view is critical for screw placement and TAD measurement.
- Valgus acceptable: 5-10° reduces strain on fixation
- Varus NOT acceptable: Increases failure rate significantly
- Anatomic reduction: Ideal but not always achievable
- Slight valgus preferable to varus malreduction
Varus/valgus is only half of reduction quality. The modern, highly examinable concept (Chang and colleagues) is the anteromedial cortical apposition between the head-neck fragment and the femoral shaft, graded on the immediate post-reduction films as positive, neutral, or negative:
- Positive medial cortical support: the medial cortex of the head-neck fragment sits superomedial to (resting on) the medial cortex of the shaft. As the fracture slides under load, the cortices impact and lock, limiting further collapse - this is the desired reduction.
- Neutral (anatomic): cortices are flush end-to-end - acceptable.
- Negative: the head-neck medial cortex lies medial to and unsupported by the shaft cortex - it will slide off, predicting excessive collapse, loss of reduction, varus and lag-screw cutout. Negative apposition should be corrected at the time of surgery.
Why it matters: with a load-sharing or even a load-bearing implant, a fracture that cannot rest on its anteromedial cortex keeps sliding - so achieving positive or at least neutral anteromedial cortical contact is as important as TAD and valgus alignment for preventing mechanical failure. Quote it as: accept positive or neutral anteromedial cortical support; a negative medial buttress predicts collapse and cutout and should be re-reduced.


Alternative Fixation: External Fixation in High-Risk Patients
Very limited indications for external fixation in IT fractures:
- Medically unstable patient who cannot tolerate standard surgery
- Severe cardiac comorbidity with limited anesthesia tolerance
- Active infection precluding internal fixation
- Palliative care setting with limited mobility goals
- NOT recommended as routine treatment - higher complication rates, worse functional outcomes compared to internal fixation
Complications
- Incidence
- 1-5%
- Risk Factors
- TAD greater than 25mm, superior position, varus
- Management
- Revision to CMN or arthroplasty
- Incidence
- Under 5%
- Risk Factors
- Instability, inadequate fixation
- Management
- Revision fixation or arthroplasty
- Incidence
- Variable
- Risk Factors
- Poor reduction, unstable pattern
- Management
- Observation or corrective osteotomy
- Incidence
- 2-5%
- Risk Factors
- Diabetes, open fracture
- Management
- Debridement, antibiotics, revision
- Incidence
- 10-15%
- Risk Factors
- Immobility, elderly
- Management
- Prophylaxis, anticoagulation
- Incidence
- 30-50%
- Risk Factors
- Age, dementia, drugs
- Management
- Prevention, geriatric co-care
- Incidence
- 1-2%
- Risk Factors
- Osteoporosis, stress riser
- Management
- Long nail, plate
Lag Screw Cutout
Lag screw cutout is the most common reason for reoperation. Risk factors:
- TAD greater than 25mm (SINGLE MOST IMPORTANT)
- Superior screw position
- Varus malreduction
- Unstable fracture pattern
- Osteoporosis
Medical Complications
- Delirium: 30-50% in elderly - prevention is key
- Pneumonia: Increases with delay greater than 48 hours
- UTI: Common, catheter-associated
- Pressure injuries: Early mobilization essential
- 1-year mortality: 20-30% - related to frailty, not surgery
Postoperative Care
Postoperative Protocol
DVT prophylaxis (mechanical + LMWH). Pain management (multimodal, minimize opioids). Urinary catheter out early.
Weight-bear as tolerated (WBAT) for stable fixation. Physiotherapy. Sit out of bed. Delirium prevention.
Progressive mobilization. Transfer training. Falls risk assessment. Discharge planning.
Wound check, suture/staple removal. Check X-rays. Assess mobility.
Repeat X-rays. Continue weight-bearing. PT continuation.
Confirm union. Bone health assessment. Osteoporosis treatment initiation. Falls prevention program.
Weight-Bearing
WBAT (Weight-Bear As Tolerated) for stable internal fixation. SHS and CMN both allow immediate full weight-bearing. Restricted weight-bearing is:
- Difficult for elderly to comply with
- Associated with worse outcomes
- Not necessary with modern fixation
Orthogeriatric Care
- Shared care model (ortho + geriatrics)
- Delirium prevention and management
- Medication review
- Multimodal analgesia
- Early mobilization
- Reduced length of stay
- Lower mortality
- Better functional outcomes
- Fewer complications
- Cost-effective
Outcomes and Prognosis
Mortality
- Rate
- 5-10%
- Key Factors
- Cardiopulmonary complications, infection
- Rate
- 8-12%
- Key Factors
- Pre-existing comorbidities, age
- Rate
- 20-30%
- Key Factors
- Frailty, mobility loss, second hip fracture
- Rate
- 50-60%
- Key Factors
- Return to baseline mortality after year 1
Functional Outcomes
- 40-60% return to pre-injury walking level
- 25-30% require walking aids long-term
- 10-15% become non-ambulatory
- Better outcomes with stable fixation and early mobilization
- 50-70% return to previous residence
- 20-30% require increased care level
- 10-20% require nursing home placement
- Cognitive status major predictor
Prognostic Factors
- Pre-fracture independent mobility
- Stable fracture pattern
- Surgery within 48 hours
- Normal cognitive function
- Younger age (relative)
- Pre-existing dementia
- Multiple comorbidities (ASA III-IV)
- Delayed surgery (greater than 48 hours)
- Unstable fracture pattern
- Non-ambulatory pre-injury
Registry Benchmarks (Global)
Pooled from national hip-fracture registries (e.g. NHFD UK, ANZHFR Australia/NZ, European audits):
- Median hospital stay: 7-10 days
- 30-day mortality: 7-10%
- Surgery within 48 hours: target 80% or more
- Reoperation rate: 3-5% at 1 year
Guidelines, Registries & Global Practice
Global Epidemiology
- Worldwide burden: Hip fractures are projected to rise from roughly 1.6 million per year (2000) toward an estimated 4.5-6 million per year by 2050, driven by population ageing, with the largest absolute increases expected in Asia.
- Intertrochanteric share: Extracapsular fractures account for roughly half of all hip fractures; the proportion of unstable patterns rises with age and bone fragility.
- Demographics: Mean age in the ninth decade, female predominance approximately 3:1, the great majority following a low-energy fall in osteoporotic bone.
Side-by-Side Guideline Comparison
- Timing
- Surgery on day of, or day after, admission
- Implant Guidance
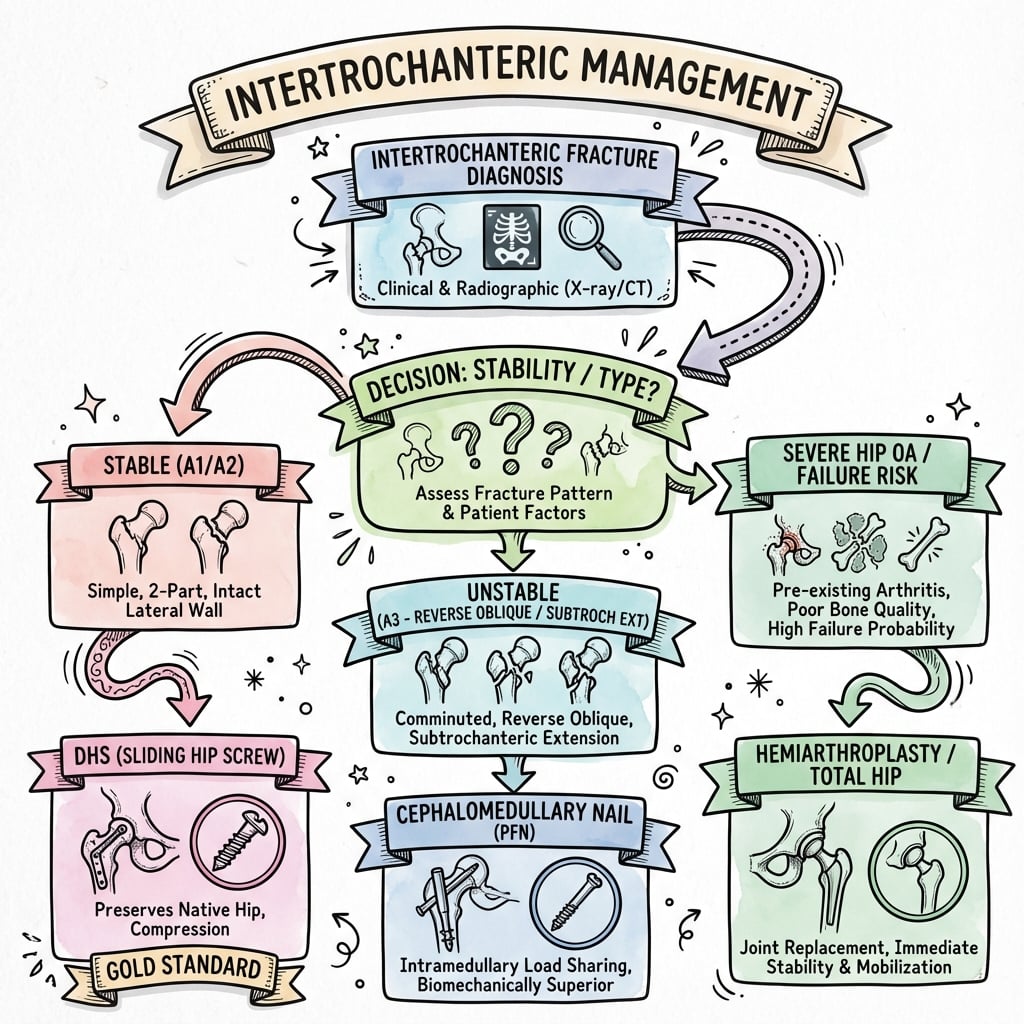
- SHS for trochanteric A1/A2; intramedullary nail for reverse-oblique/subtrochanteric (A3)
- System of Care
- Orthogeriatric co-management, early mobilisation, fascia iliaca block
- Timing
- Surgery within 24-48h improves outcomes
- Implant Guidance
- Strong evidence supports both constructs; nail favoured for unstable patterns
- System of Care
- Multidisciplinary care, VTE and delirium protocols
- Timing
- Early stable fixation
- Implant Guidance
- Stability-based: load-sharing SHS if medial buttress intact, load-bearing nail if not
- System of Care
- Emphasis on reduction quality, TAD, lateral wall
- Timing
- Within 48h
- Implant Guidance
- Nail increasingly default for unstable and reverse-oblique patterns
- System of Care
- Fragility-fracture liaison and secondary prevention
Universal agreement: extracapsular A3 reverse-oblique and subtrochanteric-extension patterns need a long cephalomedullary nail, NOT an SHS; surgery within 24-48h; orthogeriatric co-management; and routine bone-health / secondary-prevention follow-up. The main practice variation is in stable A1 patterns - the UK (NICE/BOA) still recommends the cheaper SHS as default, whereas many US and European units use a nail for almost all patterns.
Registry Evidence
- Major registries (NHFD UK, ANZHFR Australia/NZ, others across Europe and Asia) benchmark time-to-surgery, orthogeriatric review, mobilisation day 1, and 30-day mortality.
- Typical reported 30-day mortality 7-10% and 1-year mortality 20-30% across high-income settings.
- Registry feedback loops have driven measurable falls in time-to-surgery and mortality.
- Where care is linked to audited standards (surgery within 36-48h, orthogeriatric review, falls and bone-health assessment), registries show improved process compliance and lower mortality.
- Standardised pathways, not a single implant choice, are the dominant driver of outcome.
High- vs Limited-Resource Practice Variation
- High-Resource Setting
- Within 24-48h, dedicated trauma lists
- Limited-Resource Setting
- Often delayed by theatre access, blood, anaesthetic capacity
- High-Resource Setting
- SHS or CMN per stability; helical blades, InterTAN available
- Limited-Resource Setting
- Implant availability may dictate choice; SHS more widely stocked
- High-Resource Setting
- Orthogeriatric co-management, regional blocks
- Limited-Resource Setting
- Limited geriatric input; conservative (non-operative) care still used for very frail
- High-Resource Setting
- Fracture liaison services, anti-osteoporosis therapy
- Limited-Resource Setting
- Limited DXA and drug access; emphasis on falls counselling
Conservative (non-operative) treatment of an intertrochanteric fracture carries high rates of malunion, pressure injury, pneumonia and death from immobility. It is reserved for the rare patient who is unfit for any anaesthetic or in a palliative setting, and is more frequently encountered where surgical resources are constrained.
Controversies and Areas of Uncertainty
Some units now nail virtually every trochanteric fracture, arguing for a single reproducible technique and earlier full weight-bearing. The Cochrane data show equivalent function but a real, design-independent increase in implant-related femoral fracture with nails, plus higher implant cost. For truly stable A1 patterns the SHS remains defensible and cheaper.
Helical blades compact rather than ream the head, theoretically improving purchase in osteoporotic bone. However, medial migration / central perforation ("cut-through") is a recognised failure mode. Evidence has not shown clear superiority of blade over screw; TAD and reduction quality matter more than the device.
Integrated dual-screw designs (InterTAN) provide linear compression and rotational control and may reduce cutout and femoral neck shortening, but at higher cost and a more demanding technique. Benefit over standard single-screw nails remains debated.
Primary arthroplasty is occasionally proposed for severely comminuted unstable fractures or in pre-existing arthritis, but it is technically demanding (calcar deficiency), carries higher early morbidity, and is not standard. Internal fixation remains first-line; arthroplasty is mainly a salvage option after failed fixation.
State the mainstream position first (stability-based implant choice, TAD under 25mm, surgery within 48h), then acknowledge the controversy and justify a balanced, evidence-anchored stance. Examiners reward candidates who can defend a position with data rather than dogma.
MCQ Practice Points
Q: Which fracture pattern requires cephalomedullary nailing (CMN mandatory)?
A: Reverse oblique - the fracture line runs from medial proximal to lateral distal. SHS causes medialization of the shaft with this pattern, leading to malunion and failure.
Q: What is the threshold Tip-Apex Distance (TAD) for acceptable lag screw positioning?
A: Under 25mm - TAD greater than 25mm is associated with cutout rates exceeding 15%, compared to under 1% when TAD is under 25mm.
Q: Why is AVN rare in intertrochanteric fractures?
A: Extracapsular location - the fracture occurs outside the hip capsule, preserving the blood supply from the medial femoral circumflex artery which enters the femoral head via the retinacular vessels.
Q: What lateral wall thickness indicates stable fracture pattern suitable for SHS?
A: Greater than 20.5mm - lateral wall thickness under 20.5mm predicts risk of iatrogenic lateral wall fracture during SHS insertion and should be treated with CMN.
Q: What is the recommended timeframe for surgery in hip fracture?
A: Within 24-48 hours - delays beyond 48 hours increase mortality, pneumonia, and pressure sore rates. Medical optimization should not delay surgery beyond this window.
Q: What is the optimal position for lag screw in the femoral head?
A: Center-inferior quadrant - superior position has the highest cutout risk. The screw should be within 10mm of subchondral bone while maintaining TAD under 25mm.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“82-year-old woman presents after a fall at home. X-rays show a displaced intertrochanteric fracture with loss of the posteromedial buttress and the lesser trochanter is a separate fragment. She is on warfarin for AF with INR 2.8.”
“78-year-old man with a stable 2-part intertrochanteric fracture (Evans Type 1B). The registrar has listed him for a CMN. The consultant asks your opinion on implant choice.”
“You are reviewing a postoperative X-ray of a patient who had sliding hip screw fixation for an intertrochanteric fracture. The measured TAD is 32mm and the screw appears to be in the superior quadrant of the femoral head.”
Classification
- Evans/Jensen: Type 1 stable, Type 2-3 unstable
- AO 31-A1 stable, A2 unstable, A3 reverse oblique
- Stability = intact posteromedial cortex
- Reverse oblique = CMN mandatory
Implant Selection
- Stable: SHS or CMN (either acceptable)
- Unstable: CMN (load-bearing required)
- Reverse oblique: CMN mandatory
- Subtrochanteric extension: Long CMN
TAD Rule
- TAD = AP + Lateral tip-apex distance
- Under 25mm = cutout under 1%
- Greater than 25mm = cutout greater than 15%
- Target center-inferior position
Lateral Wall
- Greater than 20.5mm = SHS safe
- Less than 20.5mm = Use CMN
- Measure 3cm below innominate tubercle
Postoperative
- WBAT from day 1
- DVT prophylaxis essential
- Orthogeriatric co-management
- Start osteoporosis treatment
Evidence Base
These are the landmark papers an examiner expects you to be able to cite by name. Each card links to the original PubMed record for independent verification. Quote the headline number (TAD 25mm, lateral wall 20.5mm, surgery within 48h) rather than vague statements.
Cochrane Review: Cephalomedullary Nails vs Extramedullary Implants
- 76 studies, 10,979 participants. Probably little or no difference between CMN and extramedullary devices (mainly SHS) in mortality at 4 months (RR 0.96) or 12 months (RR 0.99).
- CMN reduced superficial infection (RR 0.71) and non-union (RR 0.55), but increased intraoperative implant-related fracture (RR 2.94) and later periprosthetic fracture (RR 3.62) - a risk NOT abolished by newer nail designs.
- No difference seen between stability subgroups, nail length, or nail generation.
HIP ATTACK: Accelerated vs Standard Surgery
- International RCT, 2970 patients, 17 countries. Median time to surgery 6h (accelerated) vs 24h (standard).
- No significant reduction in 90-day mortality (HR 0.91, 95% CI 0.72-1.14) or composite of major complications (HR 0.97).
Timing of Surgery and Mortality
- 35 studies, over 190,000 patients. Surgery within 48 hours associated with lower risk of death (pooled OR 0.74, 95% CI 0.67-0.81) and fewer pressure sores (OR 0.48).
- Effect persisted in adjusted prospective studies; conservative delay strategies should be avoided.