ECRB Origin Pathology | 80-90% Respond to Conservative | 6-12 Months Before Surgery
- ECRB origin is the primary pathology - angiofibroblastic degeneration, not inflammation
- 80-90% respond to conservative management - physiotherapy, eccentric exercises, bracing
- Surgery only after 6-12 months of failed conservative treatment
- Open vs arthroscopic debridement - both effective, similar outcomes
- PRP superior to corticosteroid (durable to 2 years) but benefit over an active needling control is modest and delayed
- “Lateral epicondylitis is tendinosis (degeneration), not tendinitis (inflammation)
- “Cozen's test and Mill's test are provocative tests for diagnosis
- “ECRB origin at lateral epicondyle is most commonly affected structure
- “Natural history is self-limiting - most resolve within 12-18 months
Angiofibroblastic degeneration of the ECRB origin - this is tendinosis, not tendinitis. No significant inflammatory cells on histology. Failed healing response with disorganized collagen and neovascularization.
Extensor Carpi Radialis Brevis origin at the lateral epicondyle is the primary pathology in 90% of cases. The underside of ECRB at its origin shows characteristic grey, friable angiofibroblastic tissue (Nirschl lesion).
80-90% respond to non-operative management including physiotherapy, eccentric exercises, counterforce bracing, and activity modification. Surgery is reserved for those who fail 6-12 months of conservative treatment.
PRP is superior to corticosteroid for long-term outcomes, durable to 2 years (Peerbooms/Gosens RCT). Much of the early effect of PRP is shared with needling/fenestration, so its benefit over an active needling control is modest and delayed (Mishra). Corticosteroid gives short-term relief but worsens long-term outcomes and increases recurrence.
- Symptoms
- Mild pain, provocable only
- Treatment
- Rest, activity modification, ice
- Key Pearl
- Avoid cortisone - may worsen long-term outcome
- Symptoms
- Moderate pain, functional limitation
- Treatment
- Physiotherapy, eccentric exercises, brace
- Key Pearl
- 80% will improve with structured rehabilitation
- Symptoms
- Failed conservative, persistent symptoms
- Treatment
- Consider PRP, GTN patches
- Key Pearl
- Surgery only if truly failed all conservative options
- Symptoms
- Failed all conservative, affecting work/life
- Treatment
- Surgical debridement (open or arthroscopic)
- Key Pearl
- 90% success with surgery after appropriate conservative trial
ECRBECRB - The Culprit Tendon
Hook:ECRB is the Culprit - 90% of lateral epicondylitis involves this tendon
Overview and Epidemiology
Lateral epicondylitis, commonly known as "tennis elbow," is a degenerative condition of the common extensor origin at the lateral epicondyle of the humerus. Despite the name, only 5-10% of patients with this condition actually play tennis.
Key epidemiological features:
- Incidence: 1-3% of the general population annually
- Peak age: 35-50 years (working age population)
- Dominant arm: 75% of cases
- Occupation: Manual laborers, computer workers, racquet sports athletes
- Natural history: Self-limiting in most cases, resolves within 12-18 months
The term "tendinitis" implies inflammation, but lateral epicondylitis is actually angiofibroblastic tendinosis - a failed healing response with degenerative changes rather than acute inflammation. Histology shows disorganized collagen, fibroblast proliferation, and neovascularization without significant inflammatory cells.
- Repetitive wrist extension and supination activities
- Age 35-50 years (peak occupational demands)
- Manual labor (mechanics, carpenters, painters)
- Computer work with poor ergonomics
- Racquet sports (especially poor technique)
- Smoking (impairs tendon healing)
- Diabetes (tendinopathy association)
- Affects work productivity (manual workers particularly affected)
- Causes significant pain with daily activities (lifting, gripping)
- Economic burden from lost work days and treatment costs
- Most resolve spontaneously but can become chronic in 10-20%
Pathophysiology and Mechanisms
Common extensor origin anatomy:
The lateral epicondyle serves as the attachment point for the common extensor origin, comprising four muscles:
- Function
- Wrist extension, radial deviation
- Involvement in LE
- 90% - primary pathology
- Clinical Significance
- Deep surface at origin most affected
- Function
- Wrist extension, radial deviation
- Involvement in LE
- Sometimes involved
- Clinical Significance
- Superficial to ECRB, may need reflection
- Function
- Finger extension
- Involvement in LE
- Rarely involved
- Clinical Significance
- Posterior aspect of origin
- Function
- Wrist extension, ulnar deviation
- Involvement in LE
- Rarely involved
- Clinical Significance
- Ulnar aspect of origin
Biomechanics of injury:
- ECRB origin experiences peak stress during wrist extension with elbow extension
- Pronation increases tension on ECRB
- Eccentric loading during deceleration phase (tennis backhand, hammering)
- Repetitive microtrauma leads to cumulative damage
- Failed healing response due to poor vascularity at tendon-bone interface
The undersurface of the ECRB at its origin is the primary site of pathology (Nirschl's original observation). This area is subjected to maximum tensile stress and has relatively poor blood supply. The pathological tissue is grey, friable, and lacks normal tendon architecture - termed "angiofibroblastic hyperplasia" or the "Nirschl lesion."
Pathophysiology - The Degenerative Cascade:
Tendinosis Progression
Organized type I collagen fibers, minimal vascularity, tenocytes aligned with load direction.
Tenocyte activation, increased proteoglycan and water content, reversible thickening. This is NOT lateral epicondylitis yet.
Angiofibroblastic degeneration: disorganized collagen (type III), increased cellularity, neovascularization with nerve ingrowth. This is lateral epicondylitis.
Collagen fiber disruption, partial tears, fibrosis, calcification. May progress to complete tendon failure in severe cases.
Histological features:
- Increased fibroblasts (not inflammatory cells)
- Disorganized type III collagen (instead of normal type I)
- Neovascularization with accompanying nerve ingrowth
- Absence of prostaglandins (explains poor response to NSAIDs)
- Increased substance P and glutamate (pain mediators)
Angio = new blood vessels (neovascularization), fibroblastic = increased fibroblast activity, degeneration = breakdown of normal tendon structure. This term accurately describes the pathology and explains why anti-inflammatory treatments (cortisone, NSAIDs) provide only temporary relief - there's no inflammation to suppress.
Nerve involvement:
- Posterior interosseous nerve (PIN) lies deep to common extensor origin
- PIN compression can coexist with lateral epicondylitis (radial tunnel syndrome)
- Differentiating between lateral epicondylitis and PIN compression is critical
- PIN syndrome: pain over radial tunnel (4cm distal to lateral epicondyle), weakness of finger/thumb extension
Classification Systems
Nirschl Staging of Tendinosis (most widely used)
This classification describes the pathological progression from acute inflammation through chronic degeneration.
- Pathology
- Mild inflammation, edema, reversible
- Clinical Features
- Pain after activity, resolves with rest
- Management
- Rest, ice, activity modification
- Pathology
- Angiofibroblastic degeneration
- Clinical Features
- Pain during and after activity
- Management
- Physiotherapy, eccentric exercises
- Pathology
- Structural failure, partial tearing
- Clinical Features
- Pain during activity, limits performance
- Management
- Consider injection therapy, surgery if refractory
- Pathology
- Fibrosis, calcification, chronic
- Clinical Features
- Pain at rest and with activity
- Management
- Surgical debridement often required
Nirschl was the first to recognize that lateral epicondylitis is not an inflammatory condition but rather a degenerative tendinosis. His classification emphasizes the progression from reversible changes (Phase 1) to irreversible structural damage (Phase 4), guiding treatment decisions.
Clinical Presentation and Assessment
History:
- Pain: Lateral elbow, radiates to forearm
- Onset: Gradual (overuse) or acute (single event rare)
- Aggravating factors: Gripping, lifting, wrist extension
- Relieving factors: Rest, avoiding provocative activities
- Functional impact: Difficulty with cup/kettle, handshake, turning doorknob
- Occupation: Manual labor, computer work, typing
- Sports: Tennis, golf, racquet sports (technique issues)
- Dominant hand: 75% affect dominant side
- Duration: Acute (weeks) vs chronic (months)
- Previous treatment: What has been tried, any injections
- Red flags: Severe pain at rest, night pain (exclude other pathology)
Physical examination:
- Key Findings
- Usually normal, no swelling/deformity
- Clinical Significance
- Massive swelling suggests other pathology (septic arthritis, fracture)
- Key Findings
- Tenderness 1cm distal/anterior to lateral epicondyle (ECRB origin)
- Clinical Significance
- This is the most reliable clinical finding
- Key Findings
- Full elbow flexion/extension, pronation/supination
- Clinical Significance
- Reduced ROM suggests intra-articular pathology
- Key Findings
- Pain with resisted wrist extension (elbow extended, wrist radially deviated)
- Clinical Significance
- High sensitivity for lateral epicondylitis
- Key Findings
- Pain with passive wrist flexion (elbow extended, forearm pronated)
- Clinical Significance
- Stretches ECRB, reproduces pain
- Key Findings
- Pain suggests radial tunnel syndrome (PIN compression)
- Clinical Significance
- Helps differentiate from pure lateral epicondylitis
Cozen's Test - The Gold Standard
Technique:
- Patient seated, elbow extended
- Forearm pronated, wrist in slight radial deviation
- Examiner resists wrist extension (patient makes a fist and extends wrist)
- Pain at lateral epicondyle is positive
Sensitivity: 80-90% Specificity: 70-80%
Resisted wrist extension loads the ECRB maximally, reproducing the pain at its origin. The test is most sensitive when performed with the elbow fully extended (increases tension on ECRB) and wrist radially deviated (ECRB's primary action).
Radial tunnel syndrome (PIN compression) can mimic lateral epicondylitis but has different treatment. Key distinguishing features:
- Pain is 4-5cm distal to lateral epicondyle (over radial tunnel)
- Weakness of finger/thumb extension (PIN motor function)
- Positive middle finger extension test (Maudsley's)
- No relief with lateral epicondyle cortisone injection
If suspected, consider EMG/NCS and surgical exploration of PIN.
COZENCOZEN - Clinical Tests
Hook:COZEN test is the classic provocative test - resisted wrist extension reproduces lateral epicondyle pain
The Radiocapitellar (Posterolateral) Synovial Plica
The differential-diagnosis table lists synovial plica as a mimic, and the arthroscopic sections note that arthroscopy lets you "assess joint, plica, instability". This deserves development, because a symptomatic radiocapitellar plica is a recognised cause of recalcitrant or "failed" tennis elbow.
A synovial plica is a normal fold of the joint lining at the posterolateral or posterior radiocapitellar joint. With repetitive pronation-supination it can thicken, become fibrotic and impinge between the radial head and capitellum.
- Radiocapitellar plica
- Over the radiocapitellar joint, slightly POSTERIOR to the lateral epicondyle
- Lateral epicondylitis (ECRB)
- 1 cm distal and anterior to the lateral epicondyle (ECRB origin)
- Radiocapitellar plica
- Painful clicking, snapping or catching with pronation-supination and flexion-extension; a painful arc
- Lateral epicondylitis (ECRB)
- Pain on gripping and resisted wrist extension (Cozen, Mill)
- Radiocapitellar plica
- MRI may show a thickened plica (more than 3 mm) abutting the radiocapitellar joint; definitive at arthroscopy
- Lateral epicondylitis (ECRB)
- ECRB tendinosis signal; plica usually absent
- Radiocapitellar plica
- Arthroscopic resection of the symptomatic plica
- Lateral epicondylitis (ECRB)
- ECRB debridement and repair
Suspect a radiocapitellar synovial plica when lateral elbow pain is accompanied by clicking, snapping or catching with rotation, when tenderness is over the radiocapitellar joint (slightly posterior to the epicondyle) rather than at the ECRB origin, or when an apparent tennis elbow fails to settle. It is a recognised cause of "failed lateral epicondylitis", which is why the arthroscopic approach is valued for letting the surgeon inspect and resect a symptomatic plica at the same sitting. Distinguish it from radial tunnel syndrome (pain further distal, finger-extension weakness) and posterolateral rotatory instability (a history of giving way), which have their own pathways.
Investigations
Radiographic assessment:
Imaging Protocol
AP and lateral elbow: Usually normal in lateral epicondylitis. Rarely shows calcification in chronic cases.
Purpose: Exclude other pathology (arthritis, loose bodies, fracture, osteochondritis dissecans).
Dynamic assessment: Can visualize tendon thickening, hypoechoic areas (degeneration), neovascularization on Doppler.
Advantages: Cost-effective, dynamic examination, guide injections.
Limitations: Operator-dependent, cannot assess intra-articular pathology.
T1 and T2 sequences: Shows increased signal in ECRB origin (tendinosis), partial tears, bone marrow edema.
Indications: Failed conservative treatment, planning surgery, exclude other causes (radiocapitellar arthritis, osteochondral lesion).
Not routinely required for diagnosis - lateral epicondylitis is a clinical diagnosis.
Electromyography/Nerve Conduction Studies: Used to diagnose radial tunnel syndrome (PIN compression) or cervical radiculopathy.
Indications: Weakness of finger/thumb extension, pain distal to lateral epicondyle, atypical symptoms.
Imaging is NOT required to diagnose lateral epicondylitis. The diagnosis is based on history (overuse, gradual onset) and examination (lateral epicondyle tenderness, positive Cozen's/Mill's test). Imaging is used to exclude other pathology or for pre-operative planning in surgical candidates.
Typical imaging findings:
- Typical Findings
- Usually normal; occasionally calcification
- Clinical Use
- Exclude arthritis, loose bodies, fracture
- Typical Findings
- ECRB thickening, hypoechoic areas, Doppler flow
- Clinical Use
- Confirm diagnosis, guide injections
- Typical Findings
- High T2 signal in ECRB, partial tears, bone edema
- Clinical Use
- Pre-operative assessment, exclude other causes


Management Algorithm
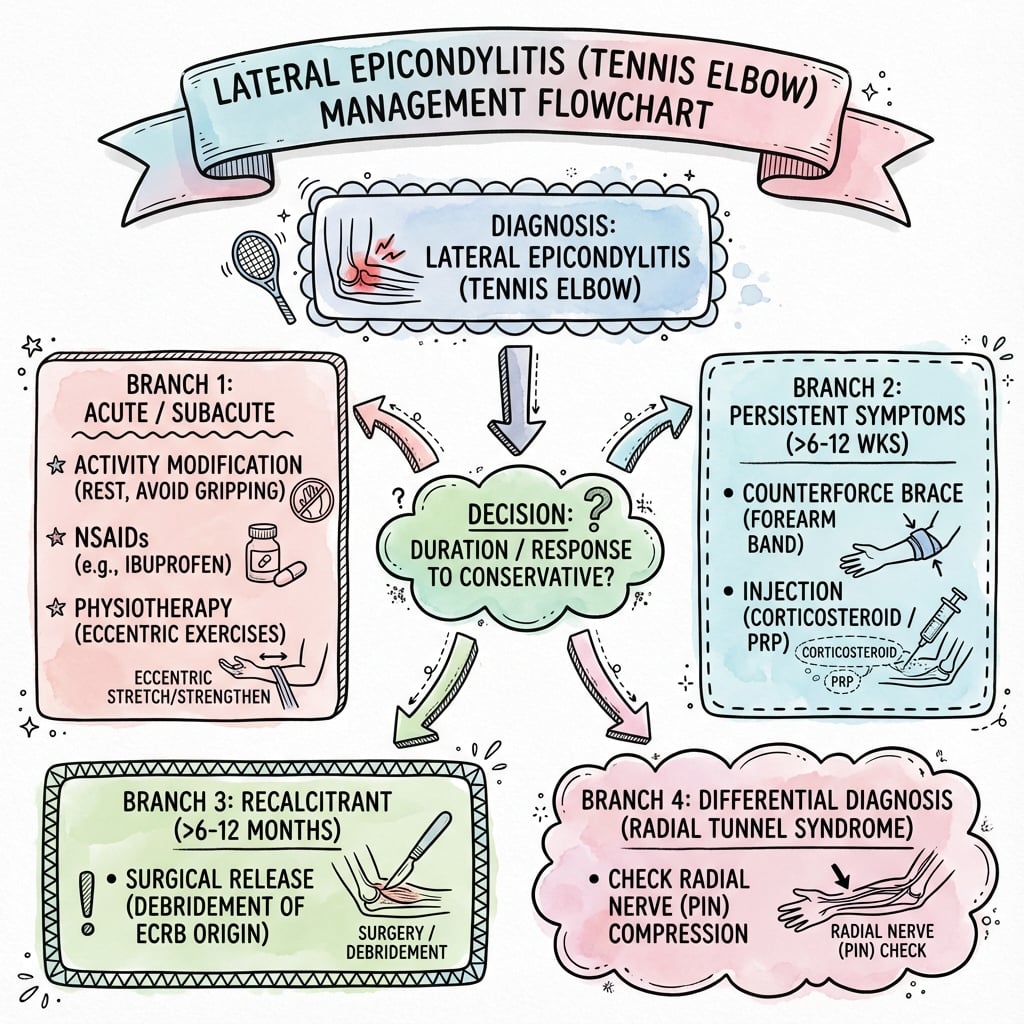
Conservative treatment is first-line for ALL patients
Success rate: 80-90% improve with non-operative management
Structured Conservative Protocol
Goals: Reduce pain, protect healing
- Activity modification: Avoid provocative activities (heavy lifting, gripping)
- Ice: 15-20 minutes several times daily
- NSAIDs: Short course (1-2 weeks) for symptom relief only
- Counterforce brace: Worn 2cm distal to lateral epicondyle during activities
- Wrist extension splint: Night splint to rest ECRB
Avoid cortisone injection at this stage - may worsen long-term outcome.
Goals: Restore tendon strength and endurance
Eccentric exercises (Tyler twist protocol):
- Wrist extension with resistance bar
- Slow eccentric lowering (3-5 seconds)
- 3 sets of 15 repetitions, daily
- Progress load as tolerated
Additional physiotherapy:
- Stretching of wrist extensors
- Ultrasound/laser therapy
- Manual therapy/soft tissue massage
- Gradual return to activities
If inadequate response to Phase 1-2:
- GTN (glyceryl trinitrate) patches: Applied to lateral epicondyle, may promote tendon healing
- Topical NSAIDs: Diclofenac gel, safer than oral NSAIDs
- Counterforce bracing: Continue during activities
- Ergonomic assessment: Work/sport modification
Consider injection therapy if still symptomatic at 3 months.
Only after failed structured rehabilitation:
PRP (Platelet-Rich Plasma):
- May be superior to cortisone for long-term outcomes
- NOT superior to placebo in RCTs
- Consider if patient wants to avoid surgery
Cortisone injection:
- Effective short-term relief (4-8 weeks)
- Worse long-term outcomes than PRP or placebo
- Maximum 2-3 injections
- Avoid in younger athletes
Autologous blood injection / dry needling:
- Similar efficacy to PRP
- Stimulates healing response
- Cheaper alternative to PRP
Surgery should only be considered after 6-12 months of failed conservative treatment. This includes:
- Structured eccentric exercise program (minimum 3 months)
- Counterforce bracing
- Activity modification
- At least one trial of injection therapy (PRP or cortisone)
Patients who proceed to surgery without adequate conservative trial have worse outcomes.
TENNISTENNIS - Conservative Management
Hook:TENNIS elbow needs TIME - 80-90% improve without surgery
Eccentric Loading and the Tyler Twist Protocol
The conservative sections repeatedly name "eccentric exercises (Tyler twist protocol)" as the core of rehabilitation, but never explain the technique or why eccentric loading works. Because this is the single most important evidence-based conservative measure, it is worth setting out.
Why eccentric loading? Lateral epicondylitis is a failed-healing tendinosis, not inflammation, so anti-inflammatory measures only mask symptoms. Controlled eccentric (lengthening-under-load) exercise applies a mechanotransduction stimulus that drives tenocyte collagen synthesis, remodels the disorganised type III collagen toward organised type I, reduces neovascularity and the accompanying nerve ingrowth, and progressively restores the tendon's load capacity - treating the actual pathology.
The Tyler twist (FlexBar) technique:
Tyler Twist - Step by Step
Hold a flexible resistance bar vertically in the affected hand with the wrist in FULL extension; grasp the top of the bar with the unaffected hand.
Twist the bar by flexing the unaffected (top) wrist while the affected wrist stays extended - this winds tension into the bar (the concentric phase is done by the healthy side).
Move both arms forward to horizontal with the elbows straight, keeping the bar twisted and the affected wrist extended.
SLOWLY allow the affected wrist to move from extension into flexion against the bar's recoil over 3-4 seconds - this controlled lowering is the eccentric load on the wrist extensors and ECRB. Typically 3 sets of 15 repetitions once daily, progressing bar stiffness as tolerated; mild discomfort during the exercise is acceptable.
The Tyler twist delivers an isolated eccentric load to the wrist extensors using a rubber FlexBar: the healthy wrist winds the bar, and the affected wrist then controls the slow untwist from extension into flexion. It matters because eccentric loading is mechanotransductive - it stimulates collagen remodelling and reduces neovascular/neural ingrowth, directly addressing the failed-healing tendinosis that anti-inflammatories cannot. Eccentric protocols outperform standard concentric exercise for lateral epicondylosis and are the backbone of the 6-12 month conservative trial that must be completed before surgery is considered.
Surgical Technique
The Gold Standard Open Technique
Patient Positioning
Setup Checklist
Supine on operating table with arm board.
- Shoulder abducted 90 degrees
- Elbow flexed 90 degrees on arm board
- Forearm supinated for lateral approach
- General anesthesia OR regional block (interscalene or axillary)
- Local anesthetic infiltration of surgical site
- Consider tourniquet for bloodless field (not essential)
- Standard limb drape
- Lateral epicondyle palpated and marked
- Radial head palpated (surgical landmark)
Surgical Approach
Step-by-Step Open Technique
Kaplan approach (modified lateral):
- 4-5cm longitudinal incision centered over lateral epicondyle
- Extends from 2cm proximal to 2cm distal to epicondyle
- Subcutaneous dissection, protect lateral cutaneous nerve of forearm
Identify ECRL (Extensor Carpi Radialis Longus):
- Most anterior muscle of common extensor origin
- Split ECRL longitudinally in line with fibers
- Retract ECRL anteriorly to expose ECRB beneath
ECRB examination:
- Underside of ECRB at origin typically shows grey, friable tissue
- Contrast with normal white, glistening tendon
- Palpate for tears or detachment
Remove pathological tissue:
- Excise grey angiofibroblastic tissue from undersurface of ECRB
- Preserve normal tendon (anterior and posterior margins)
- Extend debridement until normal tendon visualized
- Send specimen for histology (confirm diagnosis)
Prepare lateral epicondyle:
- Lightly decorticate lateral epicondyle with curette or burr
- Create bleeding bone surface for healing
- Drill 2-3 small holes in epicondyle (optional - for anchor if needed)
Reconstruct common extensor origin:
- Repair ECRB to lateral epicondyle with non-absorbable suture
- Side-to-side repair to adjacent normal tendon
- Avoid excessive tension (wrist in neutral position)
Layer closure:
- Close ECRL split with absorbable suture
- Subcutaneous layer with absorbable suture
- Skin with subcuticular or interrupted sutures
- Apply sterile dressing and hinged elbow brace
Nirschl described the pathological tissue as "grey, friable, edematous tissue resembling crabmeat". This tissue contrasts sharply with normal white, glistening tendon and is the target for surgical debridement. Complete removal of this tissue is essential for surgical success.
Technical Pearls
- Identify ECRB carefully: Split ECRL to expose ECRB beneath
- Complete debridement: Remove all grey, friable tissue until normal tendon seen
- Decorticate epicondyle: Create bleeding bone for healing
- Repair securely: ECRB to bone or side-to-side to adjacent tendon
- Protect PIN: Keep deep to supinator, forearm supinated
- Don't detach entire origin: Preserve normal tendon anterior/posterior
- Don't release LCL: Posterior to ECRB, essential for elbow stability
- Don't debride too deep: Risk to joint capsule and PIN
- Don't tension repair: Wrist neutral position to avoid re-rupture
- Don't immobilize long-term: Early motion prevents stiffness
SURGICALSURGICAL - Operative Indications and Technique
Hook:SURGICAL treatment only after failed conservative - debride ECRB, protect PIN
Complications
- Incidence
- 10-20% at 1 year
- Risk Factors
- Poor rehabilitation compliance, return to activity too soon
- Management
- Repeat physiotherapy, consider injection or surgery
- Incidence
- 5-10% (skin atrophy, depigmentation)
- Risk Factors
- Superficial injection, multiple injections
- Management
- Usually cosmetic only, counsel patient pre-injection
- Incidence
- 5-15%
- Risk Factors
- Inadequate debridement, incomplete conservative trial
- Management
- Revision surgery, assess for other pathology (PIN, LCL)
- Incidence
- Less than 5% (temporary), less than 1% (permanent)
- Risk Factors
- Deep dissection, arthroscopic technique, forearm pronation
- Management
- Most resolve spontaneously in 3-6 months; permanent injury rare
- Incidence
- 5-10%
- Risk Factors
- Prolonged immobilization, extensive dissection
- Management
- Early motion protocol, physiotherapy, manipulation if severe
- Incidence
- Less than 5%
- Risk Factors
- Excessive debridement, LCL damage
- Management
- Rare; may require LCL reconstruction
- Incidence
- Less than 1%
- Risk Factors
- Standard surgical risk
- Management
- Antibiotics; rarely requires debridement
Key complications in detail:
1. Recurrent symptoms after surgery (5-15%)
Causes:
- Inadequate debridement of pathological tissue
- Failure to address coexisting pathology (PIN, radial tunnel, plica)
- Poor rehabilitation compliance
- Return to provocative activities too soon
Management:
- Reassess diagnosis (MRI, EMG if suspect PIN)
- Trial of injection therapy
- Revision surgery if clear residual ECRB pathology
2. PIN injury
The posterior interosseous nerve is at risk during:
- Deep dissection through supinator
- Arthroscopic debridement (especially mid-anterolateral portal)
- Excessive retraction with forearm pronated
- Keep forearm supinated during dissection
- Limit depth of dissection (stay superficial to joint capsule)
- Identify and protect PIN if encountered
- Weakness of finger/thumb extension (no sensory loss)
- Usually temporary (neuropraxia)
- Permanent injury rare (less than 1%)
3. Elbow stiffness
Risk factors:
- Prolonged immobilization (more than 2 weeks)
- Extensive capsular damage
- Heterotopic ossification (rare)
Prevention:
- Early motion protocol (begin at 5-7 days)
- Hinged elbow brace allowing motion
- Avoid rigid splinting
With appropriate patient selection (failed adequate conservative trial, ECRB pathology confirmed), surgical debridement has 85-95% success rate. The key to success is:
- Adequate conservative trial (6-12 months)
- Complete removal of pathological tissue
- Secure repair of ECRB origin
- Early motion rehabilitation
- Gradual return to activities
Postoperative Care and Rehabilitation
Rehabilitation Timeline
- Dressing: Bulky dressing, remove at 48 hours
- Hinged brace: Apply at 90 degrees, allow 90-120 degrees ROM
- Gentle active motion: Elbow flexion/extension, pronation/supination
- No gripping or wrist exercises yet
- Ice and elevation: Control swelling
- Wound check: Remove sutures at 10-14 days
- Increase ROM: Progress to full extension/flexion
- Gentle strengthening: Begin light grip exercises (putty, stress ball)
- Wrist exercises: Active range of motion only, no resistance
- Continue brace: During activities, wean at 6 weeks
- Avoid: Heavy lifting, forceful gripping
- Wean brace: Discontinue at 6-8 weeks
- Eccentric exercises: Wrist extension with resistance (Tyler twist)
- Progressive loading: Gradually increase resistance
- Light work tasks: Office work, light manual labor
- Goal: Full ROM, 70% strength by 12 weeks
- Full strengthening: Continue progressive resistance
- Sport-specific training: Tennis players - gradual return to play
- Return to work: Manual labor at 3-4 months
- Return to sport: Racquet sports at 4-6 months
- Expect: 90% of final result by 6 months
Begin gentle active motion within first week to prevent stiffness. The repaired ECRB is secure enough to tolerate motion (no gripping yet). Prolonged immobilization leads to stiffness, which is harder to treat than the original condition.
Key rehabilitation principles:
- Begin within first week
- Prevents elbow stiffness
- Does not compromise repair
- Full ROM by 6 weeks
- Eccentric exercises from week 6
- Progressive resistance
- Tyler twist protocol
- Avoid pain with exercises
- Realistic expectations (3-6 months full recovery)
- Avoid premature return to sport
- Gradual return to work/activities
- 85-95% good-excellent outcomes
- Increasing pain (infection, re-injury)
- Weakness (PIN injury)
- Severe stiffness (needs aggressive therapy)
- No improvement by 3 months (consider revision)
Outcomes and Prognosis
Conservative treatment outcomes:
With structured rehabilitation (eccentric exercises, bracing, activity modification):
- 80-90% improve within 12 months
- Natural history is self-limiting - most resolve by 12-18 months regardless of treatment
- Recurrence rate: 10-20% at 1 year
Surgical treatment outcomes:
- Open Release
- 85-95%
- Arthroscopic Release
- 85-95%
- Notes
- No significant difference between techniques
- Open Release
- 2-3 weeks
- Arthroscopic Release
- 1-2 weeks
- Notes
- Arthroscopic slightly faster
- Open Release
- 3-4 months
- Arthroscopic Release
- 6-8 weeks
- Notes
- Significant difference favoring arthroscopic
- Open Release
- 4-6 months
- Arthroscopic Release
- 3-4 months
- Notes
- Gradual return important for both
- Open Release
- 10-15%
- Arthroscopic Release
- 10-15%
- Notes
- Mostly minor (stiffness, recurrence)
Predictors of poor outcome:
- Short conservative trial (less than 6 months)
- Workers' compensation claim
- Secondary gain issues
- Poor rehabilitation compliance
- Smoking (impairs healing)
- Inadequate debridement (grey tissue left behind)
- Damage to LCL (instability)
- PIN injury (weakness)
- Prolonged immobilization (stiffness)
- Early return to activity (re-injury)
Patients who undergo surgery after less than 6 months of conservative treatment have worse outcomes than those who complete an adequate trial. The reasons are multifactorial:
- Natural history of condition (many would have improved anyway)
- Psychological factors (patient not fully committed to recovery)
- Inadequate rehabilitation attempt
- Selection bias (more demanding patients)
Always complete 6-12 months of conservative treatment before considering surgery.
Guidelines, Registries & Global Practice
Global epidemiology (source-cited):
- Figure
- 1.3%
- Source population
- Finnish general population aged 30-64 (n=4783)
- Reference
- Shiri, Am J Epidemiol 2006 (PMID 16968862)
- Figure
- 45-54 years; no sex difference
- Source population
- Same Finnish population study
- Reference
- Shiri 2006 (PMID 16968862)
- Figure
- 4.9% new LE in symptom-free workers
- Source population
- US multi-industry worker cohort (n=699 followed)
- Reference
- Descatha, Occup Environ Med 2013 (PMID 23825198)
- Figure
- Current OR 3.4; former OR 3.0
- Source population
- Finnish population study
- Reference
- Shiri 2006 (PMID 16968862)
The often-quoted "1-3% annual" figure is a range across studies. The best population estimate of definite lateral epicondylitis is 1.3% point prevalence, peaking at 45-54 years with no sex difference (Shiri 2006). Repetitive/forceful wrist and forearm activity, smoking and obesity are the strongest determinants.
Major guidelines and evidence syntheses, side by side:
- Core recommendation
- Reassure (self-limiting), analgesia/topical NSAIDs, activity modification; corticosteroid injection only for short-term relief and not routinely; consider physiotherapy if not settling
- Evidence level / basis
- Guideline summary of RCT evidence
- Core recommendation
- Avoid corticosteroid injection: worse 1-year recovery (83% vs 96%) and higher recurrence (54% vs 12%) vs placebo
- Evidence level / basis
- Level I RCT (PMID 23385272)
- Core recommendation
- PRP superior to corticosteroid at 1 and 2 years for chronic LE
- Evidence level / basis
- Level I RCT (PMID 20448192, 21422467)
- Core recommendation
- No single modality clearly best for refractory disease; combine evidence-based and patient-centred care across PRP, tenotomy, open and arthroscopic options
- Evidence level / basis
- Level IV systematic review (PMID 39106325)
- Core recommendation
- Open, percutaneous and arthroscopic release give comparable results; choose by surgeon experience and concomitant pathology
- Evidence level / basis
- Level III systematic review (PMID 17632419)
Across UK, European and North American sources the message is consistent: lateral epicondylitis is largely self-limiting, corticosteroid injection harms long-term outcomes, and no surgical technique is proven superior. Differences are mainly in how readily PRP and surgery are offered, not in the underlying evidence.
Practice variation by setting:
- Ready access to ultrasound, PRP and arthroscopic facilities
- Greater use of PRP despite cost, given Level I support over corticosteroid
- Both open and arthroscopic release available; choice driven by surgeon preference
- Emphasis on reassurance, activity modification, counterforce bracing and eccentric loading (low-cost, evidence-based)
- Corticosteroid still widely used for short-term relief despite long-term harm
- Open release favoured where arthroscopy and PRP are unavailable
Key medicolegal points for lateral epicondylitis (applicable to any health system):
- Adequate conservative trial: Document structured physiotherapy, eccentric exercises, bracing and injection therapy
- Timing: Minimum 6-12 months before surgery
- Surgical consent: Inform about PIN injury risk (less than 5%), recurrence (5-15%) and stiffness (5-10%)
- Compensable injury / secondary gain: A recognised poor prognostic factor - document carefully
- Realistic expectations: Surgery is not 100% successful; 3-6 months recovery
Common litigation themes: surgery without adequate conservative trial, unrecognised or undocumented PIN injury, failure to warn about recurrence, and unrealistic expectations.
Return-to-work principles (any setting):
- Manual workers often need extended time off (3-4 months after open release)
- Ergonomic assessment and graduated return with modified duties
- Occupational therapy input where available
MCQ Practice Points
Q: What is the characteristic histological finding in lateral epicondylitis? A: Angiofibroblastic degeneration (or angiofibroblastic hyperplasia) - disorganized type III collagen, increased fibroblasts, neovascularization, and absence of inflammatory cells. This is tendinosis, not tendinitis.
Q: Which tendon is most commonly affected in lateral epicondylitis? A: Extensor Carpi Radialis Brevis (ECRB) - the undersurface of the ECRB at its origin on the lateral epicondyle is the site of pathology in 90% of cases. The grey, friable tissue described by Nirschl is found at this location.
Q: What is Cozen's test and what does a positive test indicate? A: Resisted wrist extension with the elbow extended and forearm pronated. A positive test (pain at lateral epicondyle) indicates lateral epicondylitis. High sensitivity (80-90%) for the diagnosis.
Q: What percentage of patients with lateral epicondylitis respond to conservative management? A: 80-90% of patients improve with conservative treatment including activity modification, physiotherapy, eccentric exercises, and bracing. Natural history is self-limiting with resolution in 12-18 months in most cases.
Q: What does the evidence show regarding PRP injection for lateral epicondylitis? A: PRP is superior to corticosteroid for long-term outcomes, durable to 2 years (Peerbooms 2010 / Gosens 2011). Against an active needling control, PRP showed no benefit at 12 weeks but was superior by 24 weeks (Mishra 2014) - much of the early effect comes from needling/fenestration itself. Corticosteroid provides short-term relief but worsens long-term outcomes and increases recurrence (Coombes 2013).
Q: What is the minimum duration of conservative treatment before considering surgery for lateral epicondylitis? A: 6-12 months of failed conservative treatment including structured physiotherapy with eccentric exercises, bracing, activity modification, and at least one trial of injection therapy. Surgery without adequate conservative trial leads to worse outcomes.
Q: What nerve is at risk during surgical release for lateral epicondylitis and where is it located? A: Posterior interosseous nerve (PIN) - a purely motor branch of the radial nerve located approximately 4-5cm distal to the lateral epicondyle, deep to the supinator muscle at the level of the radial neck. Injury causes finger/thumb extension weakness without sensory loss.
Q: What is the 'Nirschl lesion' and what should be done with it? A: The grey, friable angiofibroblastic tissue at the undersurface of the ECRB origin, described by Nirschl as resembling "crabmeat." This pathological tissue should be completely excised during surgical debridement until normal white, glistening tendon is visualized.
Q: What is the success rate of surgical debridement for lateral epicondylitis after failed conservative treatment? A: 85-95% good-to-excellent results with open or arthroscopic release in appropriately selected patients (those who have failed adequate conservative trial). Recurrence/failure rate is 5-15%.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old carpenter presents with 3 months of lateral elbow pain. It started gradually, worsened with work (hammering, gripping), and now affects his ability to work. He has been taking ibuprofen with minimal relief. On examination, he has tenderness 1cm distal to the lateral epicondyle and a positive Cozen's test. What is your assessment and management?”
“A 38-year-old tennis coach has had lateral elbow pain for 14 months. She has completed 6 months of structured physiotherapy with eccentric exercises, tried a counterforce brace, had two PRP injections (at 6 and 9 months), and modified her coaching activities. Despite this, she continues to have significant pain affecting her ability to coach and play. MRI shows ECRB tendinosis with partial-thickness tearing. She is requesting surgical intervention. Walk me through your surgical planning and technique.”
“You are performing an open release for lateral epicondylitis. During debridement of the ECRB, you notice the patient develops weakness of finger extension in recovery. The anesthesiologist mentions they saw some twitching of the fingers during your dissection. What has happened and how do you manage this?”
Key Anatomy
- ECRB origin at lateral epicondyle = primary pathology (90%)
- Undersurface of ECRB shows grey, friable tissue (Nirschl lesion)
- PIN located 4-5cm distal to lateral epicondyle (surgical danger)
- Common extensor origin = ECRB, ECRL, EDC, ECU
Pathophysiology
- Angiofibroblastic degeneration = tendinosis (NOT tendinitis)
- Disorganized type III collagen, neovascularization, increased fibroblasts
- No significant inflammatory cells (poor response to NSAIDs/cortisone)
- Failed healing response to repetitive microtrauma
Clinical Diagnosis
- Tenderness 1cm distal/anterior to lateral epicondyle
- Cozen's test = resisted wrist extension (high sensitivity)
- Mill's test = passive wrist flexion with forearm pronated
- Imaging NOT required (clinical diagnosis)
Conservative Management (80-90% Success)
- Activity modification + counterforce brace + ice
- Eccentric exercises (Tyler twist protocol) from 6 weeks
- Avoid cortisone early (worsens long-term outcomes)
- PRP at 3-6 months if refractory (superior to corticosteroid, durable to 2 years)
- 6-12 months trial mandatory before surgery
Surgical Technique
- Open Nirschl = split ECRL, debride ECRB (remove grey tissue), repair to bone
- Arthroscopic = portals, debride ECRB, faster recovery (same success rate)
- Protect PIN = forearm supinated, superficial dissection
- Early motion at 5-7 days, eccentric exercises at 6 weeks
- 85-95% success with appropriate patient selection
Evidence Base and Key Studies
- Double-blind RCT of 100 patients with chronic lateral epicondylitis (PRP n=51 vs corticosteroid n=49)
- Both injected via a peppering needling technique into the ECRB origin
- At 1 year, 73% of the PRP group were successful (greater than 25% reduction in VAS/DASH) versus 49% with corticosteroid (P less than 0.001)
- Corticosteroid improved early then declined, whereas PRP progressively improved
- Double-blind, multicentre RCT of 230 patients with chronic tennis elbow failing conservative therapy
- Leukocyte-enriched PRP needling versus active control (needling with local anaesthetic alone)
- No significant difference at 12 weeks (success 75.2% PRP vs 65.9% control, P=0.10)
- At 24 weeks PRP was superior (success 83.9% vs 68.3%, P=0.037; less residual tenderness, P=0.009)
- Landmark case series: 88 elbows in 82 patients undergoing open ECRB debridement and repair
- Consistently identified immature fibroblastic and vascular infiltration of the ECRB origin
- Results rated excellent in 66, good in 9, fair in 11, failed in 2 (overall 97.7% improvement)
- 85.2% of patients returned to full activity including rigorous sport
- Systematic review grouping surgery into open, percutaneous and arthroscopic techniques
- No single technique was superior for pain relief, strength restoration or return to work
- Insufficient controlled trials to perform a meta-analysis (2002 Cochrane review reached the same conclusion)
- Each approach has distinct advantages and disadvantages
- Two-year follow-up of the same 100-patient double-blind RCT (PRP vs corticosteroid)
- PRP group significantly more often successfully treated than corticosteroid (P less than 0.0001)
- Corticosteroid DASH scores returned to baseline; PRP scores continued to improve
- No complications related to PRP
- 2x2 factorial, placebo-controlled RCT of 165 patients with unilateral lateral epicondylalgia
- At 1 year, corticosteroid gave LOWER complete recovery/much improvement than placebo injection (83% vs 96%, RR 0.86)
- Corticosteroid markedly increased 1-year recurrence (54% vs 12% with placebo, RR 0.23)
- Adding physiotherapy gave no significant 1-year benefit over no physiotherapy