Preserve When Possible | Repair Better Than Resect | Red-White-White Zones
- Meniscus transmits 70% of knee load - preservation critical to prevent OA
- Blood supply: Red-red (outer third), red-white (middle), white-white (inner) zones
- Repair indications: Peripheral tears under 3mm from rim, length over 10mm, stable rim
- McMurray test: Joint line pain/click with rotation plus flexion-extension
- MRI: Gold standard (90-95% sensitivity) for tear detection and characterization
- “Always try to repair peripheral tears - better long-term outcomes than resection
- “Root tears disrupt hoop stress - treat like complete meniscectomy functionally
- “Degenerative tears in older patients: conservative management first (FIDELITY and METEOR trials)
- “ACL-deficient knee with meniscus tear: stabilize ACL to protect meniscus repair
The meniscus is not just a vestigial structure - it transmits 70% of load, increases contact area by 50%, and is critical for joint health. Meniscectomy increases contact stress 200-300% and leads to early OA. Always try to repair when possible.
Red-red zone (0-3mm from periphery): excellent healing. Red-white (3-5mm): moderate. White-white (inner third): avascular, poor healing. This determines repair success and technique selection.
Repair indications: Peripheral tears under 3mm from rim, vertical pattern, length over 10mm, stable tissue. Repair preferred even if technically challenging - better 10-year outcomes. Young patient with repairable tear should get repair.
Meniscal root tears disrupt hoop stress mechanism - functionally equivalent to total meniscectomy. Posterior medial root most common. Must repair to restore function. Transtibial pullout technique is gold standard.
- Tear Pattern
- Vertical/longitudinal
- Location
- Red-red zone (under 3mm)
- Treatment
- Arthroscopic repair (inside-out or all-inside)
- Tear Pattern
- Peripheral tear
- Location
- Any repairable location
- Treatment
- ACL + meniscus repair (protect repair with stability)
- Tear Pattern
- Radial or root
- Location
- Posterior root
- Treatment
- Repair if symptomatic, preserve meniscus
- Tear Pattern
- Complex/degenerative
- Location
- White-white zone
- Treatment
- Conservative first (6 months), partial resection if fails
- Tear Pattern
- Degenerative
- Location
- Any location
- Treatment
- Conservative management first (FIDELITY/METEOR trials) - PT, injections
REDRED-WHITE Zones - Blood Supply
Hook:Think RED for the outer rim - rich blood supply, excellent healing, direct repair possible
BUCKETBUCKET - Bucket-Handle Tear Features
Hook:BUCKET describes the classic displaced longitudinal tear - needs urgent treatment
ROOTROOT - Meniscal Root Tear Significance
Hook:ROOT tears cut the anchor - functionally removes the whole meniscus stress function
Overview and Epidemiology
Meniscal tears are among the most common knee injuries, occurring across all age groups but with distinct patterns based on mechanism. The menisci are C-shaped fibrocartilaginous structures that play critical roles in load transmission, shock absorption, and joint stability.
Why meniscus preservation matters:
- Transmits 70% of knee load in extension, 50% in flexion
- Increases contact area by 50%, reducing peak stress
- Loss increases contact pressure 200-300%
- Meniscectomy accelerates osteoarthritis development (relative risk approximately 7 for radiographic and symptomatic OA after meniscectomy for a degenerative tear at 16 years; Englund 2003)
Historical approach: arthroscopic partial meniscectomy for all symptomatic tears. Modern approach: preserve meniscus tissue whenever possible. Two landmark randomised trials underpin this shift - the FIDELITY trial (Sihvonen et al, NEJM 2013) showed arthroscopic partial meniscectomy was no better than sham surgery for degenerative medial tears without OA, and the METEOR trial (Katz et al, NEJM 2013) showed surgery plus physiotherapy was no better than physiotherapy alone for degenerative tears with mild-to-moderate OA. Repair techniques have also improved, supporting meniscal preservation over resection.
Two distinct populations:
- Mechanism: Acute trauma (twisting, pivoting)
- Tear pattern: Vertical, longitudinal, bucket-handle
- Location: Often peripheral (red-red zone)
- Associated injuries: ACL tears (40% have meniscus injury)
- Treatment: Repair strongly preferred
- Mechanism: Minor trauma or spontaneous
- Tear pattern: Horizontal cleavage, complex
- Location: Often central (white-white zone)
- Associated findings: Early OA changes
- Treatment: Conservative first, selective resection
Pathophysiology and Mechanisms
Gross anatomy:
- Medial Meniscus
- C-shaped (covers 50-60% of plateau)
- Lateral Meniscus
- O-shaped (covers 70-80% of plateau)
- Medial Meniscus
- Less mobile (fixed to MCL)
- Lateral Meniscus
- More mobile (no MCL attachment)
- Medial Meniscus
- More common (60-70% of tears)
- Lateral Meniscus
- Less common (30-40% of tears)
- Medial Meniscus
- Attached to tibial plateau anterior
- Lateral Meniscus
- Attached near ACL
- Medial Meniscus
- Attached to PCL attachment area
- Lateral Meniscus
- Attached near PCL, popliteus hiatus
Microstructure:
- Fibrocartilage: Type I collagen (90%), proteoglycans, cells (fibrochondrocytes)
- Fiber orientation: Circumferential fibers (resist hoop stress) + radial tie fibers
- Zones: Superficial (contact with femur/tibia), deep (transitional), lamellar (central)
Load transmission creates circumferential hoop stress in meniscal fibers, like hoops on a barrel. This is why radial tears and root tears are so devastating - they disrupt the circumferential fibers and eliminate the hoop stress function. The meniscus then functions like a "washer with a cut" - it cannot resist extrusion and loses load-bearing capacity.
Blood supply:
The understanding of meniscal blood supply is critical for repair decisions:
- Distance from Periphery
- 0-3mm
- Vascularity
- Excellent (perimeniscal capillary plexus)
- Healing Potential
- Good
- Repair Success
- 80-90%
- Distance from Periphery
- 3-5mm
- Vascularity
- Moderate (some penetration)
- Healing Potential
- Variable
- Repair Success
- 60-70%
- Distance from Periphery
- over 5mm (inner 1/3)
- Vascularity
- Avascular
- Healing Potential
- Poor
- Repair Success
- 20-30%
Source of blood supply:
- Perimeniscal capillary plexus from superior and inferior geniculate arteries
- Penetrates radially from periphery
- Adult meniscus: outer 10-25% has blood supply (children have more)
Pediatric menisci have blood supply extending further toward the center (red-white zone may extend to 50% in young children). This is why meniscus tears in children have better healing potential and repair should be attempted even for more central tears.
Biomechanical functions:
- Load transmission - 70% of load in extension, 50% in flexion
- Shock absorption - Energy dissipation during loading
- Joint stability - Secondary stabilizer (especially lateral meniscus in ACL-deficient knee)
- Joint lubrication - Synovial fluid distribution
- Proprioception - Mechanoreceptors provide feedback
Classification Systems
International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS)
Most comprehensive and widely accepted classification:
- Description
- Parallel to circumferential fibers, longitudinal
- Mechanism
- Acute trauma, twisting
- Repairability
- Good if peripheral
- Description
- Cleavage tear, parallel to tibial plateau
- Mechanism
- Degenerative, chronic
- Repairability
- Poor - usually resect
- Description
- Perpendicular to circumferential fibers
- Mechanism
- Acute or chronic
- Repairability
- Difficult - consider if root
- Description
- Combination of patterns
- Mechanism
- Chronic, degenerative
- Repairability
- Variable, usually poor
ISAKOS also describes:
- Location: Anterior horn, body, posterior horn
- Depth: Partial (superior or inferior surface) vs full-thickness
- Length: Measured in mm
- Quality: Traumatic (good tissue) vs degenerative (poor tissue)
The ISAKOS classification is superior because it integrates pattern (determines load-bearing), location (determines vascularity), and tissue quality (determines healing) - all critical for surgical decision-making.
Parameniscal Cyst
The complications section notes a meniscal cyst only in passing, yet the parameniscal cyst is a recognised presentation in its own right and a recurring exam favourite because of how it must be treated.
A parameniscal cyst is a collection of synovial-like fluid adjacent to the meniscus that almost always communicates with a meniscal tear - characteristically a horizontal cleavage tear - through a one-way-valve mechanism that pumps fluid peripherally.
- Detail
- Usually arises from a horizontal cleavage tear; a one-way valve pushes synovial fluid peripherally to form the cyst
- Detail
- Lateral cysts are commoner and more often palpable; medial cysts tend to be larger and more posterior
- Detail
- Firm joint-line swelling, classically most prominent near extension and reducing with flexion (lateral cyst), with joint-line pain
- Detail
- MRI shows the cyst contiguous with the underlying (usually horizontal) meniscal tear
- Detail
- Treat the underlying tear arthroscopically (debride/partial meniscectomy, or repair if repairable) with cyst decompression; excising the cyst alone without treating the tear recurs
A parameniscal cyst is a fluid collection beside the meniscus that almost always communicates with a horizontal cleavage tear through a one-way-valve mechanism; lateral cysts are commoner and palpable as a firm joint-line swelling that is prominent in extension and shrinks with flexion. The key principle is that the cyst is SECONDARY to the tear - arthroscopic treatment of the tear with decompression of the cyst is durable, whereas excising the cyst alone (without addressing the tear) leads to recurrence.
Clinical Assessment
History:
- Mechanism: Twisting injury, pivoting, deep squat
- Onset: Immediate or within 24-48 hours
- Symptoms: Sharp pain, click, locking, swelling
- Age: Younger patients (under 40)
- Associated: ACL injury (screen carefully)
- Mechanism: Minor trauma or spontaneous
- Onset: Gradual (days to weeks)
- Symptoms: Aching, catching, intermittent swelling
- Age: Older patients (over 45)
- Associated: Early OA changes, activity-related pain
Key history questions:
- Locking vs pseudo-locking (true locking = inability to fully extend)
- Mechanical symptoms (catching, clicking with specific movements)
- Swelling pattern (immediate vs delayed)
- Previous knee injuries or surgery
- Activity level and goals
Physical examination:
- Technique
- Flex knee fully, rotate tibia, extend knee
- Positive Finding
- Pain or click at joint line
- Sensitivity/Specificity
- Sens 70%, Spec 71%
- Technique
- Patient stands on one leg, knee flexed ~20deg, rotates body
- Positive Finding
- Pain at joint line
- Sensitivity/Specificity
- Originally Sens 89%/Spec 97% (Karachalios); Sens ~0.62-0.66/Spec ~0.39-0.55 on independent validation (Blyth 2015)
- Technique
- Palpate medial/lateral joint line
- Positive Finding
- Point tenderness
- Sensitivity/Specificity
- Sens 83%, Spec 83%
- Technique
- Prone, flex knee 90deg, rotate with compression
- Positive Finding
- Pain with compression
- Sensitivity/Specificity
- Sens 61%, Spec 70%
The Thessaly test (patient stands on the affected leg with knee flexed about 20 degrees and rotates the body while held for balance) was originally described by Karachalios et al with very high reported accuracy (sensitivity 89%, specificity 97%). However, these figures have not been reproduced: the independent NIHR HTA prospective study (Blyth et al, 2015) found a sensitivity of only 0.62-0.66 and specificity of 0.39-0.55, no better than McMurray, Apley or joint-line tenderness. The exam-safe answer is that no single physical test reliably diagnoses a meniscal tear, and clinical assessment is combined with MRI.
Examination components:
- Inspection: Swelling (effusion), quadriceps wasting (chronic), alignment
- Palpation: Joint line tenderness (most sensitive single finding)
- Range of motion: Extension deficit (bucket-handle), painful arc
- Special tests: McMurray, Thessaly, Apley
- Stability: ACL (Lachman), MCL (valgus stress) - associated injuries
A substantial proportion of acute ACL tears have an associated meniscus injury, often the lateral meniscus at the time of injury. If clinical examination suggests a meniscus tear in a young patient with acute trauma, always assess ACL stability. Combined injuries need both addressed for optimal outcome.
Differential diagnosis of the painful or mechanical knee
The symptoms attributed to a meniscal tear (joint-line pain, catching, giving way, effusion) overlap with several other conditions, and a meniscal tear seen on MRI is frequently incidental in middle-aged and older patients (Englund, NEJM 2008). Consider the breadth of differentials before attributing symptoms to the meniscus.
- Discriminating features
- Older patient, diffuse rather than point joint-line pain, crepitus, morning stiffness, often coexists with degenerative tear
- Key investigation
- Weight-bearing radiographs; MRI cartilage
- Discriminating features
- True intermittent locking that resolves, mechanical catching, younger patient (OCD)
- Key investigation
- Radiographs, MRI (cartilage and subchondral bone)
- Discriminating features
- Acute pivot injury, haemarthrosis, instability/giving way, positive Lachman
- Key investigation
- Lachman/pivot-shift, MRI
- Discriminating features
- Valgus stress mechanism, tenderness over MCL rather than joint line, valgus laxity
- Key investigation
- Valgus stress test, MRI
- Discriminating features
- Anterior knee pain, pain on stairs and prolonged sitting, apprehension
- Key investigation
- Clinical, skyline radiograph
- Discriminating features
- Pain and tenderness 4-5 cm below medial joint line, no true mechanical symptoms
- Key investigation
- Clinical; ultrasound if unclear
- Discriminating features
- Sudden severe medial pain in older patient, often with a degenerative root tear, marked bone marrow oedema
- Key investigation
- MRI
- Discriminating features
- Hot swollen knee, fever, systemic upset, raised inflammatory markers
- Key investigation
- Joint aspiration, bloods
Investigations
Imaging protocol:
Investigation Pathway
Views: AP standing, lateral, skyline patella, long-leg alignment (if considering surgery)
Purpose: Exclude bony injury, assess OA degree, alignment assessment
Cannot diagnose meniscus tear but rules out differential diagnoses (fracture, OA, loose body)
Sensitivity 90-95%, Specificity 85-90% for meniscus tears
Findings:
- Increased signal intensity within meniscus on T2 (tear)
- Grade 0 = normal, Grade I = intrasubstance (no tear), Grade II = linear signal not reaching surface (no tear), Grade III = signal reaches articular surface (TEAR)
- Meniscus extrusion (over 3mm = root tear or severe degeneration)
- Associated findings (ACL, MCL, bone marrow edema)
True gold standard when performed, but invasive
Used therapeutically more than diagnostically with modern MRI
Only MRI Grade III signal (linear signal extending to articular surface) represents a true tear. Grade I and II are intrasubstance degeneration without tear - these are NOT surgical indications and are often seen in asymptomatic patients over 45 years old.
MRI interpretation for surgeons:
- Clinical Significance
- Repairable tear in vascular zone
- Action
- Arthroscopy for repair
- Clinical Significance
- Non-repairable, likely chronic
- Action
- Conservative first per FIDELITY/METEOR trials
- Clinical Significance
- Root tear with loss of hoop stress
- Action
- Urgent arthroscopy for root repair
- Clinical Significance
- Intrasubstance degeneration, NO tear
- Action
- Not surgical - manage symptoms
Additional investigations:
- Ultrasound: Operator-dependent, can identify peripheral tears
- Arthro-CT: Rarely used, for patients unable to have MRI
- Standing X-rays: Essential if considering meniscus transplant or realignment surgery

Management Algorithm

Non-Operative Treatment
Indications:
- Degenerative tears in patients over 45 years (FIDELITY and METEOR trials)
- Small stable tears without mechanical symptoms
- Grade I-II MRI signal (intrasubstance degeneration)
- Patient choice or medical comorbidities
Conservative Treatment Protocol
- Activity modification: Avoid aggravating activities (twisting, pivoting, squatting)
- Ice and NSAIDs: Symptom control
- Quadriceps strengthening: Straight leg raises, quad sets
- ROM exercises: Gentle flexion-extension
- Physiotherapy: Comprehensive program
- Strengthening: Progressive resistance (quadriceps, hamstrings)
- Proprioception training: Balance exercises
- Functional training: Sport-specific activities
- Continue strengthening
- Activity modification: Avoid deep squatting
- Weight management: Reduce knee load
- Consider injections: Corticosteroid or hyaluronic acid if persistent symptoms
Two NEJM 2013 randomised trials reshaped management of degenerative tears. FIDELITY (Sihvonen et al, n=146, age 35-65, no OA) found arthroscopic partial meniscectomy no better than sham surgery at 12 months. METEOR (Katz et al, n=351, age 45+, with mild-to-moderate OA) found surgery plus physiotherapy no better than physiotherapy alone at 6 and 12 months, though 30% of the physiotherapy-only group crossed over to surgery within 6 months. Together they support a trial of physiotherapy first for degenerative tears.
Surgical Technique - Arthroscopic Meniscectomy
When Meniscectomy is Necessary
- Irreparable tear (central location, degenerative tissue)
- Failed repair
- Unstable flap tear causing mechanical symptoms
- Complex tear with poor healing potential
- Preserve as much meniscus as possible
- Create smooth, stable rim
- Remove only unstable, damaged tissue
- Never perform total meniscectomy (increases OA risk dramatically)
- Review MRI for tear pattern and location
- Assess degree of OA (if advanced, surgery won't help)
- Counsel patient about preservation vs resection
- Discuss realistic outcomes
- Plan portal placement
- Arthroscopy tower and camera
- Arthroscopic instruments (probes, graspers, punches)
- Meniscal suture devices (if repair possible)
- Meniscal repair needles and sutures
- Basket forceps and shavers
Complications
- Incidence
- less than 1%
- Prevention/Management
- Safe portal placement, protect structures during inside-out repair
- Incidence
- less than 1%
- Prevention/Management
- Sterile technique, prophylactic antibiotics
- Incidence
- 0.1-0.5%
- Prevention/Management
- Early mobilization, thromboprophylaxis in high-risk patients
- Incidence
- 10-20%
- Prevention/Management
- Complete tear removal, assess for associated pathology
- Incidence
- 10-20%
- Prevention/Management
- Appropriate patient selection, protect repair with rehab protocol
- Incidence
- RR ~7 (degenerative tear, Englund 2003)
- Prevention/Management
- Preserve meniscus tissue, counsel patient about long-term risk
Nerve injuries (most significant risk with inside-out technique):
-
Medial meniscus repair:
- Saphenous nerve injury: 2-5% incidence
- Presents as numbness/paresthesia over posteromedial leg
- Prevention: Use retractor to protect neurovascular structures, make safe accessory incision
- Usually resolves over 6-12 months
-
Lateral meniscus repair:
- Peroneal nerve injury: Less than 1% (more serious)
- Risk of foot drop if nerve damaged
- Prevention: Keep knee flexed 90 degrees, use lateral safety incision
- May require nerve exploration if complete injury
Repair failure: 10-20% depending on location and technique
- Red-red zone: 10-15% failure
- Red-white zone: 20-30% failure
- Risk factors: White-white location, poor tissue quality, non-compliance with rehab
Other complications:
- Persistent pain: 5-10%
- Stiffness: 5% (usually responds to PT)
- Postoperative meniscal cyst: Rare
Always use a safety incision and protect neurovascular structures when tying inside-out sutures. The saphenous nerve (medial) and peroneal nerve (lateral) are at risk. Use a spoon retractor to displace neurovascular bundle away from the capsule.
Proper technique minimizes nerve injury risk while achieving optimal repair strength.
Postoperative Care and Rehabilitation
Partial Meniscectomy Rehabilitation
Meniscectomy Recovery Timeline
- Weight-bearing: As tolerated with crutches (if needed)
- ROM: Immediate mobilization
- Exercises: Quadriceps sets, ankle pumps, straight leg raises
- Ice and elevation
- Pain control: Acetaminophen, NSAIDs
- Mobilization: Full weight-bearing without aids
- ROM: Regain full flexion and extension
- Strengthening: Progressive quadriceps and hamstring strengthening
- Stationary bike: Low resistance
- Pool therapy: If available
- Advanced strengthening: Leg press, step-ups
- Proprioception: Balance board
- Light jogging: If no pain
- Sport-specific training: Begin transition
- Full ROM and strength
- Return to sports: Gradual progression
- Clearance: Pain-free full activity
Return to sport:
- Desk work: 1-2 weeks
- Manual labor: 4-6 weeks
- Non-contact sports: 6-8 weeks
- Contact sports: 8-12 weeks
Meniscectomy allows rapid return but with long-term OA risk trade-off.
Outcomes and Prognosis
Outcomes by treatment:
- Success Rate
- 80-90%
- Return to Sport
- 6-9 months
- Long-term OA Risk
- Low (preserved meniscus)
- Success Rate
- 60-70%
- Return to Sport
- 9-12 months
- Long-term OA Risk
- Low if successful
- Success Rate
- 85% (short term)
- Return to Sport
- 3-4 months
- Long-term OA Risk
- High (RR ~7 for OA, Englund 2003)
- Success Rate
- 70-85%
- Return to Sport
- 9-12 months
- Long-term OA Risk
- Moderate (better than no repair)
- Success Rate
- 60-70%
- Return to Sport
- Variable
- Long-term OA Risk
- Natural progression
Prognostic factors for repair success:
- Good Prognosis
- Peripheral (under 3mm)
- Poor Prognosis
- Central (white-white zone)
- Good Prognosis
- Vertical, longitudinal
- Poor Prognosis
- Horizontal, complex, radial
- Good Prognosis
- Young (under 30)
- Poor Prognosis
- Older (over 50)
- Good Prognosis
- Acute trauma
- Poor Prognosis
- Chronic degenerative
- Good Prognosis
- ACL intact or reconstructed
- Poor Prognosis
- ACL deficient
- Good Prognosis
- Healthy
- Poor Prognosis
- Degenerative, frayed
When meniscus repair is performed with concomitant ACL reconstruction, repair success rates are higher (85-90%) compared to isolated meniscus repair (70-80%). The ACL reconstruction restores knee stability and protects the meniscus repair during healing. Always address both injuries together.
Long-term implications:
-
After partial meniscectomy:
- Substantially higher risk of OA development (RR approximately 7 for combined radiographic and symptomatic OA after meniscectomy for a degenerative tear; Englund 2003)
- More extensive resection and degenerative (rather than traumatic) tear type are associated with worse radiographic and symptomatic outcomes
-
After successful repair:
- OA risk approaches normal knee
- Joint preservation maintained
- Better quality of life long-term
Lateral vs Medial Meniscus Loss
The topic compares medial and lateral meniscus anatomy and notes that meniscectomy accelerates osteoarthritis, and the Paxton review records a higher reoperation rate after lateral than medial partial meniscectomy. The corollary - that LOSS of the lateral meniscus is functionally worse - deserves to be stated explicitly, because it changes the threshold for preservation.
- Medial meniscectomy
- Relatively congruent (concave medial tibial plateau)
- Lateral meniscectomy
- Less congruent (convex/flat lateral plateau under a convex femoral condyle)
- Medial meniscectomy
- High, but loss is tolerated relatively better
- Lateral meniscectomy
- Greater - the lateral meniscus covers more plateau and carries more of the compartment load
- Medial meniscectomy
- Progressive medial-compartment OA over years
- Lateral meniscectomy
- Faster, more severe chondral loss (rapid chondrolysis) and OA, especially in young active patients
- Medial meniscectomy
- Varus
- Lateral meniscectomy
- Valgus
- Medial meniscectomy
- Preserve where possible
- Lateral meniscectomy
- Even stronger imperative to preserve or repair
Although the medial meniscus is torn more often, LOSS of the lateral meniscus is functionally worse. The lateral compartment is less congruent (a convex femoral condyle on a convex/flat lateral plateau) and the lateral meniscus carries a greater share of compartment load, so lateral meniscectomy raises peak contact stress more and is associated with faster, more severe chondral loss - rapid chondrolysis and post-meniscectomy lateral-compartment OA - particularly in young active patients and those with valgus alignment (consistent with the higher lateral reoperation rate in the Paxton review). The practical message: the threshold to preserve or repair is even lower for the lateral meniscus.
REPAIRREPAIR - Indications for Meniscus Repair
Hook:REPAIR guides you to save the meniscus - check all criteria before deciding
Guidelines, Registries & Global Practice
Global epidemiology
Meniscal tears are among the most common knee injuries worldwide and arthroscopic partial meniscectomy has historically been one of the highest-volume orthopaedic procedures in many health systems. The population burden is dominated by degenerative tears in middle-aged and older adults: in the population-based Framingham MRI study (Englund et al, NEJM 2008; PMID 18784100), the prevalence of a meniscal tear or destruction rose from 19% in women aged 50-59 to 56% in men aged 70-90, and 61% of those with a tear were asymptomatic in the preceding month. Traumatic tears predominate in younger, athletic populations and are commonly associated with ACL rupture.
Guidelines side-by-side
International guidance has converged against routine arthroscopy for degenerative tears since the FIDELITY and METEOR trials, although surgery retains a clear role for true mechanical locking, repairable traumatic tears and root tears.
- Position on degenerative tears
- Strong recommendation AGAINST arthroscopy for nearly all degenerative knee disease, including degenerative meniscal tears
- Evidence basis
- Linked systematic review of RCTs (incl. FIDELITY, METEOR)
- Position on degenerative tears
- Non-operative care first for degenerative meniscal lesions; arthroscopy only after a failed structured programme and selected indications
- Evidence basis
- Formal European consensus on degenerative meniscus
- Position on degenerative tears
- Management of OA of the knee guideline discourages arthroscopic lavage/debridement for primary OA; meniscectomy reserved for mechanical symptoms
- Evidence basis
- AAOS clinical practice guideline
- Position on degenerative tears
- Arthroscopic lavage and debridement not recommended for knee OA unless clear history of mechanical locking
- Evidence basis
- NICE osteoarthritis guidance
- Position on degenerative tears
- Do not perform arthroscopy with partial meniscectomy for degenerative tears without mechanical locking
- Evidence basis
- Specialty-society low-value-care lists
- Position on degenerative tears
- Preserve the meniscus - repair peripheral vertical tears; repair root tears via transtibial pull-out
- Evidence basis
- FIDELITY/METEOR do not apply; supported by preservation and biomechanical evidence
Registry and practice variation
There is no dedicated international meniscus registry comparable to arthroplasty registries (e.g. AOANJRR, NJR), so population-level evidence comes from administrative datasets and RCTs rather than implant-style registry survival data. Despite consistent guidance, large practice variation persists: arthroscopic partial meniscectomy rates differ several-fold between and within countries, and uptake of the FIDELITY/METEOR evidence into routine practice has been slow. This gap between evidence and practice is a recognised low-value-care target and a common exam discussion point.
- Re-tear / repair failure: long-term reoperation after repair around 20% versus around 4% after partial meniscectomy (Paxton 2011)
- Infection (less than 1%), DVT/PE (low), and neurovascular injury specific to inside-out repair (saphenous medially, common peroneal laterally)
- Long-term OA risk after meniscectomy (relative risk approximately 7 for degenerative tears; Englund 2003) versus tissue preservation with repair
- Alternatives: for degenerative tears, a structured non-operative programme first, per the FIDELITY and METEOR trials
meniscectomy for a degenerative tear without a documented non-operative trial; failure to offer repair for a repairable tear in a young patient; undocumented nerve protection during inside-out repair; and missed associated ACL injury leading to repair failure. Document the repair-versus-resection rationale, tear characteristics, pre- and post-operative neurovascular status, and the rehabilitation plan provided.
MCQ Practice Points
Q: What is the blood supply to the meniscus and which zone has the best healing potential? A: The perimeniscal capillary plexus from the geniculate arteries supplies the outer 10-25% of the meniscus. The red-red zone (0-3mm from periphery) has excellent blood supply and 80-90% repair success. The white-white zone (inner third) is avascular with poor healing potential (20-30% success).
Q: What is the biomechanical consequence of a meniscal root tear? A: A meniscal root tear disrupts the circumferential collagen fibers and eliminates the hoop stress mechanism, leading to meniscal extrusion. This is functionally equivalent to a total meniscectomy in terms of contact stress distribution. Root tears require repair via transtibial pullout technique to restore function.
Q: According to the ISAKOS classification, which meniscus tear pattern has the best repairability? A: Vertical longitudinal tears in the peripheral (red-red) zone have the best repairability. These tears run parallel to the circumferential fibers and can be sutured effectively. Horizontal cleavage tears and complex tears typically have poor healing potential.
Q: How accurate are clinical tests for meniscus tears? A: No single physical test is reliable in isolation. The Thessaly test was originally reported with sensitivity 89% and specificity 97% (Karachalios), but the independent NIHR HTA validation study (Blyth et al, 2015) found it no better than McMurray, Apley or joint-line tenderness (sensitivity ~0.62-0.66, specificity ~0.39-0.55). Diagnosis combines history, examination and MRI; joint-line tenderness remains a useful single finding.
Q: What did the landmark 2013 NEJM trials demonstrate about degenerative meniscus tears? A: The FIDELITY trial (Sihvonen et al, NEJM 2013) showed arthroscopic partial meniscectomy was no better than sham surgery at 12 months for degenerative medial tears without OA. The METEOR trial (Katz et al, NEJM 2013) showed surgery plus physiotherapy was no better than physiotherapy alone for degenerative tears with mild-to-moderate OA. Together they support conservative management first for degenerative tears without true mechanical locking.
Q: What are the long-term consequences of partial meniscectomy? A: Meniscectomy substantially increases the long-term risk of knee osteoarthritis. In Englund's 16-year matched cohort (2003), the relative risk of combined radiographic and symptomatic OA was approximately 7 after meniscectomy for a degenerative tear (and ~2.7 after a traumatic tear). Risk rises with the amount of meniscus removed, because resection reduces contact area and increases peak contact stress. This is why meniscus preservation is critical.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old footballer presents with acute knee pain after a twisting injury 3 days ago. He describes a popping sensation and immediate swelling. Examination shows joint line tenderness and positive McMurray test. MRI shows a vertical longitudinal tear of the posterior horn of the medial meniscus, 2cm in length, located 2mm from the meniscocapsular junction. What is your assessment and management?”
“A 52-year-old office worker presents with 3 months of medial knee pain. No specific injury - started after gardening. Examination shows joint line tenderness and positive Thessaly test. MRI shows Grade III signal in the posterior horn of the medial meniscus, horizontal cleavage tear pattern, with underlying Grade 2 chondral changes. How do you manage this patient?”
“A 45-year-old female presents with 6 months of medial knee pain and swelling. She describes a twisting injury at onset. MRI shows discontinuity of the posterior medial meniscus root with 5mm of meniscal extrusion. No significant chondral loss yet. She has failed 3 months of physiotherapy. How do you manage this?”
Key Anatomy and Function
- Transmits 70% of knee load in extension, 50% in flexion
- Blood supply: Red-red (0-3mm), red-white (3-5mm), white-white (inner third - avascular)
- Medial: C-shaped, less mobile, attached to MCL, more commonly torn
- Lateral: O-shaped, more mobile, no MCL attachment
- Hoop stress mechanism: circumferential fibers resist extrusion
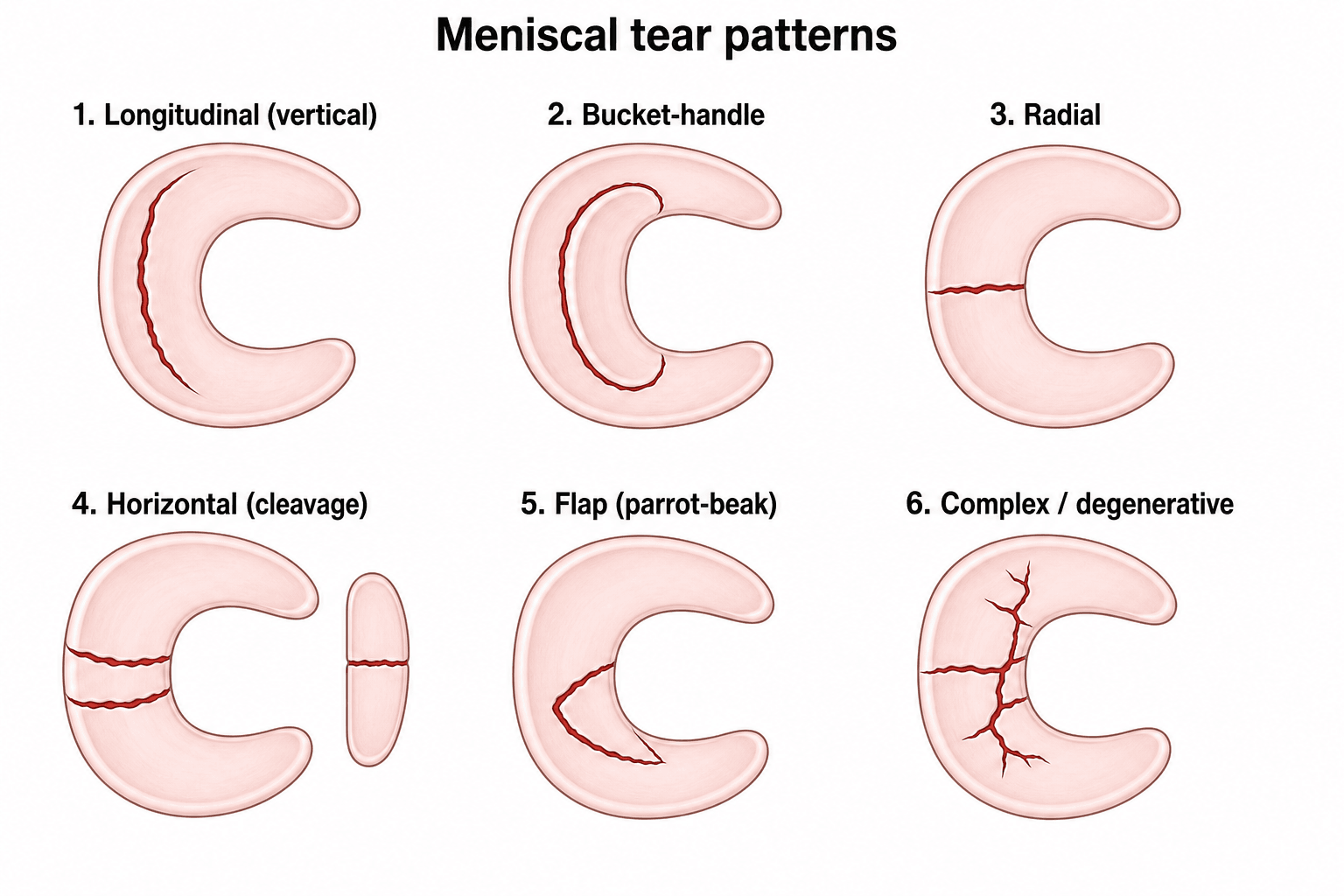
Classification (ISAKOS)
- Vertical: longitudinal/bucket-handle - repairable if peripheral
- Horizontal: cleavage tear - usually resect
- Radial: perpendicular to fibers - repair if root
- Complex: multiple patterns - assess repairability
- Root tear: disrupts hoop stress = functional total meniscectomy
Clinical Assessment
- McMurray test: pain/click with rotation + flexion-extension (Sens 70%, Spec 71%)
- Thessaly test: stand on one leg, rotate body - originally Sens 89%/Spec 97%, but only ~0.62/~0.45 on independent validation (Blyth 2015)
- Joint line tenderness: 83% sensitive
- MRI: Grade III signal = tear (Sens 90-95%)
- Root tear: MRI shows extrusion over 3mm
Treatment Algorithm
- Young traumatic peripheral tear: REPAIR (inside-out or all-inside)
- Degenerative tear over 45: CONSERVATIVE first (FIDELITY/METEOR trials)
- Bucket-handle with locking: URGENT arthroscopy, repair if possible
- Root tear: Transtibial pullout repair
- Central white-white tear: Partial meniscectomy if conservative fails
Surgical Pearls
- Preserve every millimeter possible - even 10% more preservation reduces OA risk
- Inside-out: gold standard for posterior horn, protect saphenous (medial) or peroneal (lateral)
- All-inside: faster but watch neurovascular structures
- Root repair: tunnel at 7mm anterior to PCL, tie over button
- Protected WB for 6 weeks after repair, 4 weeks non-WB for root
Key Evidence and Outcomes
- FIDELITY (APM vs sham) and METEOR (surgery+PT vs PT): no benefit of surgery for degenerative tears
- Meniscectomy for degenerative tear: OA relative risk ~7 at 16 years (Englund 2003)
- Repair success: 80-90% (red-red), 60-70% (red-white), 20-30% (white-white)
- Repair with ACL reconstruction: 85-90% success (ACL protects repair)
- Root repair: 70-85% success, reduces extrusion, slows OA
Evidence Base and Key Trials
FIDELITY Trial - Arthroscopic Partial Meniscectomy vs Sham Surgery
- Multicentre, double-blind, sham-controlled RCT of 146 patients aged 35-65 with a degenerative medial meniscus tear and NO knee osteoarthritis
- Arthroscopic partial meniscectomy versus sham (diagnostic) arthroscopy
- No significant between-group difference in Lysholm, WOMET or post-exercise pain at 12 months
- Subsequent knee surgery: 2 in the meniscectomy group versus 5 in the sham group
METEOR Trial - Surgery plus Physiotherapy vs Physiotherapy Alone
- Multicentre RCT of 351 patients aged 45+ with a meniscal tear and mild-to-moderate OA on imaging
- Arthroscopic partial meniscectomy plus physiotherapy versus standardised physiotherapy (with optional crossover)
- Mean WOMAC improvement at 6 months similar between groups (difference 2.4 points, 95% CI -1.8 to 6.5)
- 30% of the physiotherapy-only group crossed over to surgery within 6 months
Incidental Meniscal Tears in the General Population (Framingham)
- Population-based MRI study of 991 subjects aged 50-90 (Framingham)
- Prevalence of meniscal tear/destruction rose from 19% (women 50-59) to 56% (men 70-90)
- 61% of subjects with a meniscal tear had no knee pain, aching or stiffness in the prior month
- Tear prevalence was similar in symptomatic and asymptomatic knees with radiographic OA
According to PubMed, the evidence above is drawn from FIDELITY (DOI), METEOR (DOI), Englund 2008 (DOI), Englund 2003 (DOI), Paxton 2011 (DOI), LaPrade root classification 2014 (DOI) and LaPrade root biomechanics 2015 (DOI).