Extensor Mechanism Disruption | Tension Band Principle | Articular Involvement
- Triceps insertion - olecranon fractures disrupt the extensor mechanism
- Articular fracture - olecranon forms proximal ulnohumeral articulation
- Tension band principle - converts tensile forces to compressive forces at articular surface
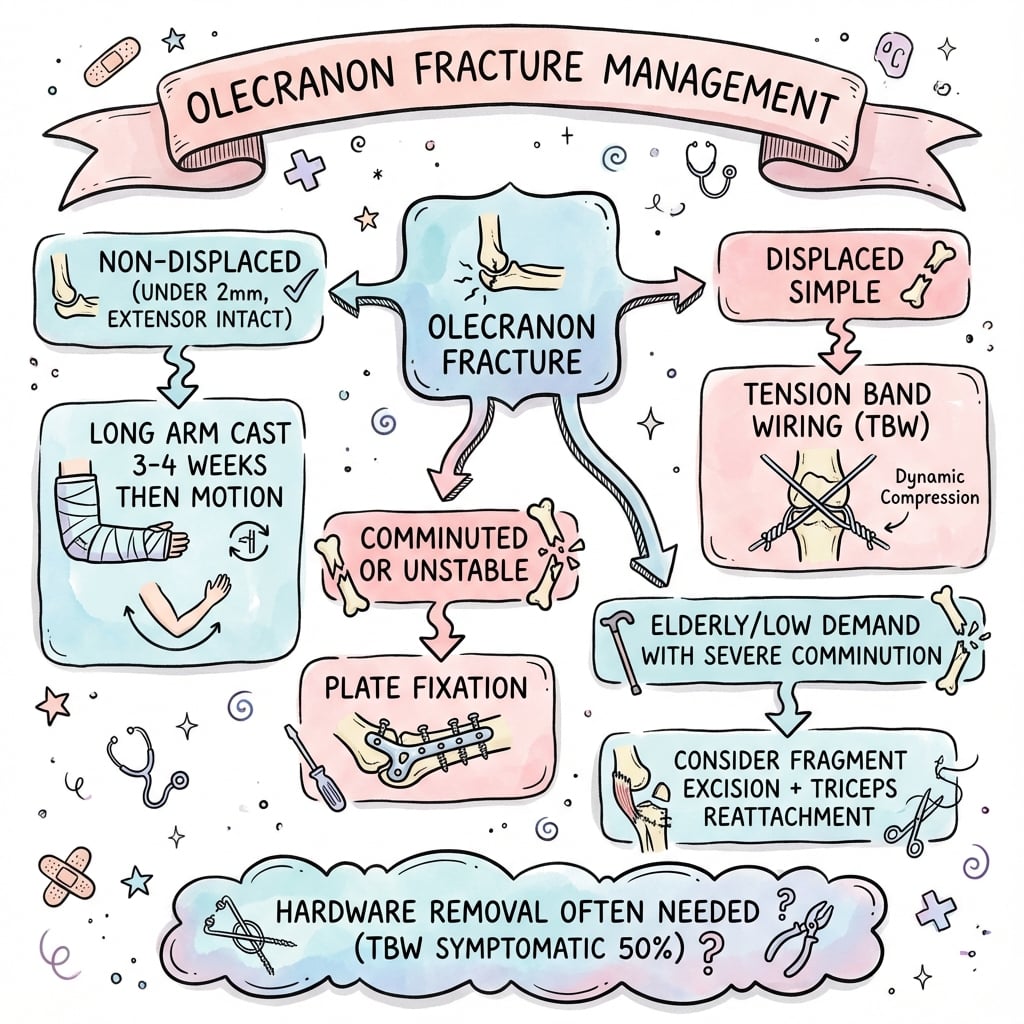
- Plate fixation preferred for comminuted and unstable patterns
- Symptomatic hardware is common (about half of TBW patients in RCT) - discuss removal with patients
- “Tension band only works for simple transverse or oblique fractures
- “Comminution or oblique patterns require plate fixation
- “Mayo Type III indicates elbow instability - more complex treatment
- “Check for associated coronoid and radial head fractures (terrible triad)
The olecranon is the triceps insertion. Fractures disrupt active elbow extension. Patient cannot extend against gravity = functional test for complete disruption.
Figure-of-8 wire converts tensile forces to compression at the articular surface. Only works for simple transverse/short oblique fractures. Comminution requires plate.
Plate fixation preferred for: oblique fracture (greater than 30 degrees), comminuted, Monteggia variant, Mayo Type III, osteoporotic bone, trans-olecranon fracture-dislocations.
Symptomatic implant removal affects roughly half of TBW patients in randomised data (50% vs 22% for plates). Pre-operative counselling is essential. Plate fixation has lower removal rates but carries the more serious risks of infection and revision.
- Mayo Type
- Type I
- Treatment
- Conservative - cast/splint, early motion
- Mayo Type
- Type IIA
- Treatment
- Tension band wiring (TBW)
- Mayo Type
- Type IIB
- Treatment
- Plate fixation
- Mayo Type
- Type III
- Treatment
- Plate fixation + address instability
- Mayo Type
- Complex
- Treatment
- Plate fixation + restore ulnohumeral joint
- Mayo Type
- Variable
- Treatment
- Consider plate or fragment excision + triceps repair

PLATEPLATE - When to Use Plate Fixation
Hook:PLATE fixation for these specific indications
302-30-50 Rule
Hook:2mm triggers surgery, 30 degrees triggers plate, ~50% of TBW need hardware out
Overview and Epidemiology
Olecranon fractures are common elbow injuries that disrupt the extensor mechanism and the ulnohumeral articulation. Understanding the biomechanics is essential for appropriate management.
- Young adults (20-40): High-energy trauma (MVA, sports, falls from height)
- Elderly (60+): Low-energy falls, osteoporotic bone
- Direct blow - fall onto point of elbow (most common)
- Indirect - fall on outstretched hand with triceps contraction (avulsion)
- Combined - direct blow + muscle contraction
The olecranon is the insertion of the triceps and forms the proximal ulnohumeral articulation. Fractures cause loss of active extension (extensor mechanism disruption) and articular incongruity (affecting elbow function).
Olecranon fractures in children behave differently from the adult injury and are a recognised exam point:
- They are frequently NOT isolated - the olecranon rarely breaks alone, so always screen for an associated injury: a radial neck fracture, a Monteggia lesion (radial head dislocation with the proximal ulna fracture), or a lateral condyle fracture. Missing the associated injury is the classic error.
- The proximal olecranon ossifies from a secondary centre (apophysis appearing about age 8-10, fusing in the mid-teens), so a normal apophysis or a persistent/sclerotic physis can mimic a fracture - compare with the other side.
- Most minimally displaced fractures are treated non-operatively in a cast, because children have thick periosteum and excellent remodelling; displaced or intra-articular fractures (and those with extensor lag) are fixed, usually with tension-band wiring or screws, on the same biomechanical principles as in adults.
- Consider an underlying bone fragility (e.g. osteogenesis imperfecta) when an olecranon fracture follows trivial trauma or is bilateral.
Anatomy and Biomechanics
- Olecranon process - proximal ulna, forms posterior elbow prominence
- Greater sigmoid notch (trochlear notch) - articular surface for trochlea
- Coronoid process - anterior buttress, critical for stability
- Subcutaneous position - minimal soft tissue coverage
- Triceps brachii - inserts on posterior olecranon tip
- Anconeus - lateral to olecranon, dynamic stabilizer
The triceps generates tensile forces on the posterior olecranon. The tension band (figure-of-8 wire) converts these to compressive forces at the articular surface. This requires intact anterior cortex to work as a compression hinge.
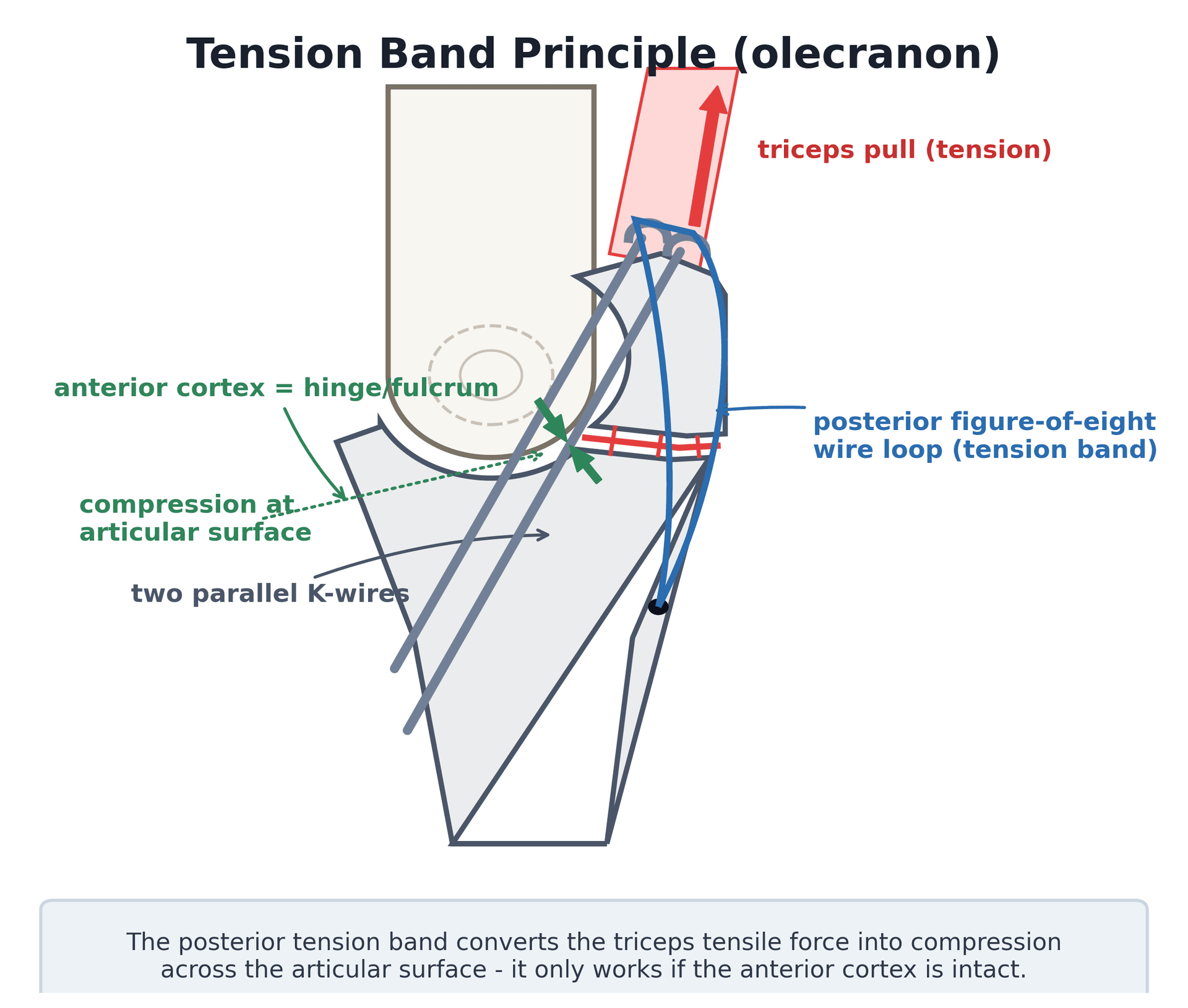
- Triceps force: up to 3x body weight
- Posterior tension, anterior compression during flexion
- Tension band only works with intact anterior cortex
- Comminution disrupts the hinge - plate fixation required
- Ulnar nerve - posterior to medial epicondyle, at risk with medial dissection
- Subcutaneous position - easy access but high hardware prominence
Classification Systems
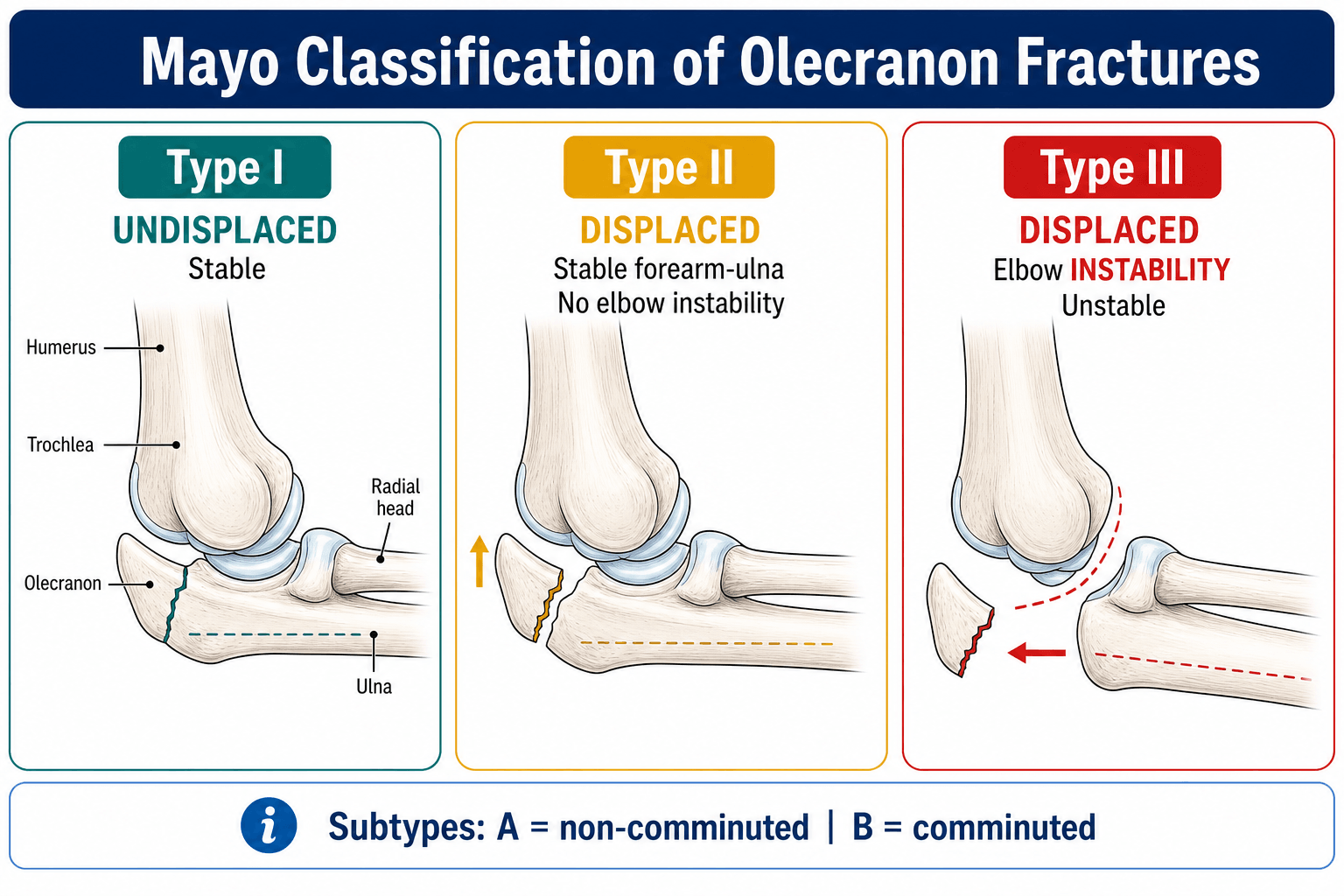
Mayo Classification (most widely used)
- Displacement
- Undisplaced (less than 2mm)
- Stability
- Stable
- Subtype
- -
- Displacement
- Displaced
- Stability
- Stable
- Subtype
- A = non-comminuted, B = comminuted
- Displacement
- Displaced
- Stability
- Unstable
- Subtype
- A = non-comminuted, B = comminuted
Stable = intact ulnohumeral joint with no subluxation. Unstable = associated elbow instability, subluxation, or fracture-dislocation pattern. Type III requires addressing both fracture and instability.
MAYOMAYO - Classification Framework
Hook:MAYO classification: displacement + stability + comminution guide treatment
Clinical Presentation and Assessment
History:
- Mechanism (direct blow, fall, sports)
- Ability to extend elbow post-injury
- Previous elbow problems
- Hand dominance
- Occupation and activity level
Physical examination:
- Significance
- Displaced fracture
- Action
- Confirms diagnosis
- Significance
- Extensor mechanism disruption
- Action
- Surgical indication
- Significance
- Open fracture or at risk
- Action
- Antibiotics if open, protect skin
- Significance
- Mayo Type III pattern
- Action
- Plan for additional stabilization
- Significance
- Articular involvement
- Action
- CT for surgical planning
- Active extension test: Patient attempts to extend elbow against gravity
- Inability to extend = complete extensor mechanism disruption = surgical indication
- Intact extension with minimal displacement may be treated conservatively
- Ulnar nerve function (little finger sensation, FDI strength)
- Median and radial nerve function
- Vascular status
The olecranon is subcutaneous. Direct trauma often causes skin abrasion or laceration. Assess carefully for open injury. Even closed fractures may have compromised skin that affects surgical timing and approach.
Investigations
Radiographic assessment:
Standard views:
- True lateral elbow - most important view
- Shows fracture pattern, displacement, articular involvement
- Assess ulnohumeral alignment
- AP elbow - confirms fracture, shows medial/lateral extent
- Oblique views - may help characterize pattern
The true lateral X-ray is essential. It shows fracture displacement, angulation, comminution, and most importantly ulnohumeral joint alignment. Anterior subluxation suggests Type III or trans-olecranon fracture-dislocation.

CT imaging:
Indications:
- Complex/comminuted fractures
- Trans-olecranon fracture-dislocations
- Associated coronoid or radial head fractures
- Surgical planning for plate placement
What to assess:
- Fracture pattern and comminution
- Articular surface involvement
- Coronoid integrity
- Associated injuries
Differential Diagnosis
The radiocapitellar dislocation and posterior elbow pain of an olecranon injury overlap with several patterns that change management completely. The discriminators below are high-yield.
- Discriminating feature
- Fracture through olecranon, ulnohumeral joint congruent, radiocapitellar line normal
- Why it matters
- Treat the fracture alone (TBW or plate)
- Discriminating feature
- Comminuted proximal ulna with anterior ulnohumeral subluxation; radiocapitellar relationship usually preserved (coronoid often a large fragment)
- Why it matters
- Must restore trochlear-notch contour with a plate; not a Monteggia [9]
- Discriminating feature
- Ulnar shaft fracture (more distal) with true radial head dislocation - radiocapitellar line disrupted
- Why it matters
- Reduce and fix ulna to length/rotation to relocate radial head
- Discriminating feature
- Radial head fracture + coronoid fracture + posterolateral dislocation; olecranon usually intact
- Why it matters
- Address all three plus LCL to restore stability
- Discriminating feature
- Avulsion of triceps insertion +/- bony flake; loss of active extension with little olecranon comminution
- Why it matters
- Tendon repair, not standard fracture fixation
- Discriminating feature
- Adolescent throwing athlete; sclerotic margins, transverse line; no acute trauma
- Why it matters
- Often non-operative or screw fixation; not an acute trauma construct
Management
Conservative management criteria:
- Requirement
- Less than 2mm step-off
- Requirement
- Intact (can extend against gravity)
- Requirement
- No elbow instability
- Requirement
- Low-demand, compliant with restrictions
Protocol:
- Posterior splint at 45-90 degrees flexion
- Begin ROM exercises at 1-2 weeks
- Avoid resisted extension for 6 weeks
- Serial X-rays to monitor displacement
Fractures treated conservatively must be monitored closely. Displacement can occur in first 2 weeks. Weekly X-rays initially, convert to surgery if displacement exceeds 2mm.
Surgical Technique
Tension Band Wiring (TBW) - classic technique
- Simple transverse or short oblique fractures
- Non-comminuted (Mayo IIA)
- Intact anterior cortex
- Posterior longitudinal incision
- Reduce fracture anatomically
- Two parallel 1.6-2.0mm K-wires, intramedullary or bicortical
- Figure-of-8 wire (1.0-1.2mm) deep to triceps, superficial to K-wires
- Tighten wire to achieve compression
- Bend and bury K-wire ends
- K-wires should engage anterior cortex distally
- Wire must be posterior to K-wires (on tension side)
- Check reduction with flexion-extension before final tightening
Tension band only works when the anterior cortex is intact to act as a compression hinge. With elbow flexion, tensile forces on posterior wire are converted to compression at the articular surface.
Distinct from fixing an olecranon fracture, the olecranon osteotomy is a deliberate surgical division of the olecranon used to expose the articular surface of the distal humerus (e.g. for a comminuted intra-articular distal humeral fracture). It is examined alongside olecranon fractures because the repair uses the same tension-band/plate principles:
- Make it an apex-distal chevron osteotomy (not transverse) - the V interdigitates, resists rotation and increases the surface area for union.
- Site it through the "bare area" of the trochlear notch (a non-articular sulcus) to spare articular cartilage.
- Predrill and pretap (or provisionally apply the plate/screw) BEFORE cutting, so the fixation re-establishes the exact anatomy on closure.
- Repair with a tension-band construct or a plate, exactly as for a transverse fracture.
- Recognised downsides: osteotomy non-union and symptomatic hardware (the same prominence problem as fracture fixation).
- Key contraindication: do not perform an olecranon osteotomy if the distal humerus may need a total elbow arthroplasty (e.g. unreconstructable articular comminution in the elderly) - it sacrifices the olecranon and extensor mechanism you would otherwise preserve; use a triceps-sparing or triceps-reflecting approach instead.
TBWTBW - Tension Band Wiring Technique
Hook:TBW: Two wires Behind the cortex, Wire in figure-8
Complications

- Incidence
- 50% TBW, 22% plate (RCT)
- Management
- Hardware removal after union
- Incidence
- 10-20%
- Management
- Physiotherapy, dynamic splinting, release if severe
- Incidence
- 5-10%
- Management
- Revision fixation with bone graft
- Incidence
- 2-5%
- Management
- Antibiotics, debridement, may need hardware removal
- Incidence
- 5-15%
- Management
- Arthroplasty if severe and symptomatic
- Incidence
- 2-5%
- Management
- Usually neurapraxia, protect nerve intraoperatively
- Incidence
- 5-10% TBW
- Management
- Bend ends, early removal if backing out
Hardware-related issues:
Pre-operative counseling about hardware prominence is essential. The olecranon is subcutaneous with minimal soft tissue coverage. Most TBW patients require hardware removal. Plate fixation has lower but still significant removal rates.
- Common after elbow trauma
- Goal: functional arc 30-130 degrees
- Prevention: stable fixation, early motion
- Treatment: physiotherapy, splinting, surgical release
- More common with inadequate fixation or infection
- Treatment: revision with plate fixation and bone graft
- May need triceps advancement if fragment excision required
Postoperative Care and Rehabilitation
Post-fixation protocol:
- Posterior splint at 90 degrees
- Elevation, ice
- Finger motion encouraged
- Wound check
- Begin active ROM
- Splint between exercises if needed
- No resisted extension
- Gravity-assisted extension
- Progressive active ROM
- Goal: full extension by 6 weeks
- Continue avoiding resisted extension
- May use dynamic splinting if stiff
- Begin gentle strengthening
- Progressive loading
- Functional activities
- Full strengthening
- Return to sport/work
- Hardware removal if symptomatic (after union confirmed)
Key rehabilitation principles:
- Early motion is essential
- Avoid resisted extension until 6 weeks
- Stable fixation permits aggressive ROM
- Hardware prominence may limit motion (remove if symptomatic)
Outcomes and Prognosis
Outcomes by treatment:
In the only head-to-head RCT of active adults, TBW and plate fixation produced equivalent patient-reported function (1-year DASH 12.8 vs 8.5; not significant), and both meta-analyses confirm no functional difference - the constructs differ in complication profile, not outcome. [1,2,3]
- Functional outcome
- Equivalent DASH to plate
- Key evidence point
- Higher symptomatic implant removal (50%) [1]
- Functional outcome
- Equivalent DASH to TBW
- Key evidence point
- Lower removal (22%) but infection/revision risk concentrated here [1]
- Functional outcome
- Comparable pain/ROM/strength to ORIF
- Key evidence point
- Fewer local complications and no extensor-strength loss vs ORIF [4]
- Functional outcome
- No significant DASH difference vs surgery at 12 months
- Key evidence point
- Small residual extension deficit; avoids operative complications [5,6]
Prognostic factors:
- Fracture complexity (comminution worse)
- Associated injuries (coronoid, radial head)
- Quality of reduction
- Patient compliance with rehabilitation
- Bone quality
Functional outcomes are similar between TBW and plate fixation. The main difference is hardware-related complications - higher with TBW. Plate fixation is increasingly preferred, especially for comminuted patterns.
Guidelines, Registries & Global Practice
Global epidemiology
Olecranon fractures account for roughly 10% of upper-limb fractures and around 20% of fractures of the proximal forearm. [3,7] In contemporary high-income populations they behave as fragility fractures: in a prospective series of 78 proximal ulna fractures the mean age was 57 years and 67% followed a simple fall from standing height, with a unimodal older-male and older-female (type-F) distribution rather than the classic young high-energy peak. Mayo IIA was the commonest pattern (60%). [8] Younger patients still sustain high-energy injuries (sport, road trauma) and are more likely to have associated proximal radius fractures.
Practice positions, side by side
There is no formal AAOS clinical practice guideline or NICE guideline dedicated to olecranon fractures; practice is driven by RCT and meta-analysis evidence and by AO Foundation principles. The table summarises where guidance converges and where genuine debate remains.
- Position
- Absolute stability for simple articular patterns (TBW for simple stable; plate for comminuted, oblique, Monteggia variants, trans-olecranon). Restore the trochlear-notch contour.
- Evidence level
- Consensus / biomechanical
- Position
- TBW and plate give equivalent function for simple fractures; plate has fewer overall complications (mainly less symptomatic hardware), but infection/revision cluster with plating.
- Evidence level
- Level I [1,2,3]
- Position
- Non-operative care is a reasonable default in low-demand patients aged 75+ - no significant DASH difference, far fewer complications.
- Evidence level
- Level I [5,6]
- Position
- Acceptable for comminuted fractures in low-demand patients if the joint stays stable; equivalent strength to ORIF with fewer local complications.
- Evidence level
- Level III [4]
Registry evidence: Olecranon fixation is not separately tracked by the major arthroplasty registries (NJR, AJRR, AOANJRR, SHAR, NZJR), which capture joint replacement rather than fracture fixation, so registry-level implant-survival data do not exist for this injury. The evidence base is therefore RCT- and meta-analysis-led rather than registry-led.
Global practice variation
- Implant choice: TBW remains widespread worldwide because it is cheap, quick and effective for simple patterns; precontoured locking plates dominate where cost is less constraining, especially for comminuted and osteoporotic fractures. The functional outcome is the same - the difference is reoperation profile and cost. [1,2]
- Elderly displaced fractures: a clear international shift toward non-operative management of low-demand elderly patients, led by Edinburgh and Australasian (SOFIE) randomised data. [5,6]
- Resource-limited settings: TBW and even fragment excision retain a larger role where locking-plate availability and theatre access are limited.
Be ready to argue TBW versus plate with indications for each, to cite the equivalent function but different complication profile (Level I), and to defend non-operative management of the frail elderly using SOFIE and the Edinburgh RCT. Know the tension-band biomechanics cold.
MCQ Practice Points
Q: According to the Mayo classification, what defines a Type III olecranon fracture? A: Displaced fracture with elbow instability. Type I = undisplaced, Type II = displaced but stable, Type III = displaced and unstable. Subtype A = non-comminuted, B = comminuted.
Q: How does tension band wiring work? A: The figure-of-8 wire converts tensile forces (from triceps pull) to compressive forces at the articular surface. This requires an intact anterior cortex to act as a fulcrum/hinge. With elbow flexion, compression increases at the fracture site.
Q: Where should the K-wires engage in tension band wiring? A: The K-wires should engage the anterior cortex of the ulna distally. This creates a more stable construct. Intramedullary placement with engagement of anterior cortex is preferred.
Q: When is plate fixation preferred over tension band wiring for olecranon fractures? A: Oblique fractures (greater than 30 degrees), comminuted fractures, osteoporotic bone, Monteggia variants, trans-olecranon fracture-dislocations, and Mayo Type III (unstable).
Q: What is the approximate rate of symptomatic hardware removal after tension band wiring for olecranon fractures? A: Around 50% in the best randomised data (Duckworth, JBJS Am 2017: 50% vs 22% for plates), with some older observational series quoting higher figures. Hardware prominence is common because of the subcutaneous position of the olecranon. Plate fixation has a lower removal rate but carries the more serious risks of infection and revision.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man falls directly onto his left elbow. X-rays show a displaced transverse olecranon fracture with 5mm of articular step-off. The elbow is stable on examination. Describe your management.”
“A 72-year-old woman with osteoporosis falls and sustains a comminuted olecranon fracture. The lateral X-ray shows the ulna is anteriorly subluxated relative to the trochlea. How do you manage this?”
“A patient returns 3 months after TBW for an olecranon fracture. They have united but have prominent hardware causing pain and skin irritation. The K-wire is backing out. What is your management?”
KEY CONCEPTS
- Triceps insertion - extensor mechanism disruption
- Articular fracture - affects ulnohumeral joint
- Subcutaneous - high hardware prominence
- 2mm step-off threshold for surgery
MAYO CLASSIFICATION
- Type I: Undisplaced (less than 2mm)
- Type II: Displaced, stable (A = simple, B = comminuted)
- Type III: Displaced, unstable (A = simple, B = comminuted)
- Stability = ulnohumeral joint status
TBW INDICATIONS
- Simple transverse or short oblique fracture
- Non-comminuted (Mayo IIA)
- Intact anterior cortex (for tension band to work)
- Accept ~50% symptomatic hardware removal rate (RCT)
PLATE INDICATIONS
- Oblique fracture (greater than 30 degrees)
- Comminuted (Mayo IIB, IIIB)
- Osteoporotic bone
- Trans-olecranon fracture-dislocation
- Mayo Type III (unstable)
TBW TECHNIQUE
- Two parallel K-wires (1.6-2.0mm)
- Intramedullary or bicortical - engage anterior cortex
- Figure-of-8 wire (1.0-1.2mm)
- Wire deep to triceps, superficial to K-wires
- Tension wire on posterior (tension) side
TRAPS AND PEARLS
- TBW only for simple patterns - plate for comminution
- Check for trans-olecranon subluxation on lateral
- ~50% TBW symptomatic hardware removal - counsel pre-op
- Anterior cortex must be intact for TBW to work
- Early motion essential to prevent stiffness
Evidence Base
- Single-centre RCT of 67 active patients (16 to 74 years) with simple displaced olecranon fractures. No significant difference in DASH at 1 year (TBW 12.8 vs plate 8.5; p=0.315) or in range of motion, Broberg-Morrey or Mayo Elbow Score. Overall complication rate was higher with TBW (63% vs 38%; p=0.042), driven by symptomatic implant removal (50% vs 22%; p=0.021). All four infections and all three revision operations occurred exclusively in the plate group.
- Thirteen studies (1 RCT, 12 observational) comparing TBW and plate fixation. No significant difference in DASH (SMD 0.07; p=0.73), range of motion, operative time or blood loss. Complications were significantly more frequent after TBW (pooled OR 2.61, 95% CI 1.65 to 4.14; p less than 0.0001).
- Eleven studies (449 TBW, 378 plate) restricted to Mayo II fractures. Plate fixation gave modestly better long-term MEPS and DASH and fewer complications (RR 2.13, 95% CI 1.48 to 3.08), while TBW had shorter operative time and less blood loss. Long-term elbow flexion and extension deficits did not differ.
- Multicentre pragmatic RCT (24 hospitals, Australia/New Zealand) of 60 patients aged 75 years or older with displaced isolated olecranon fractures. No significant difference in 12-month DASH (operative 12.3 vs non-operative 18.9; mean difference -6.6, 95% CI -14.9 to 1.8; p=0.12). Active elbow extension was better after surgery, but no other secondary outcome differed.
- RCT of patients aged 75 years or older randomised to non-operative or operative care. Stopped early because the operative complication rate (9 of 11; 81.8%) was unacceptable. DASH at 1 year did not differ (non-operative 23 vs operative 22; p=0.763).
- 107 patients with isolated olecranon fractures: 53 primary fragment excision versus 54 ORIF. Pain, function, range of motion, stability and arthritis were similar, with no difference in extensor strength on biomechanical testing. ORIF had more local complications (13 vs 2) plus 13 implant-removal procedures.
- Series of 17 anterior (trans-olecranon) fracture-dislocations. Distinct from anterior Monteggia: the distal humerus is driven through the olecranon, producing a comminuted proximal ulna with the radiocapitellar joint usually intact. Stable anatomic restoration of the trochlear-notch contour gave excellent/good results in 15 of 17 at 25 months.
- Prospective series of 78 proximal ulna fractures (mean age 57 years). A simple fall from standing height caused 67%; younger patients sustained higher-energy mechanisms. Distribution was a unimodal older-male and older-female (type-F) curve, and Mayo IIA was the commonest olecranon pattern (60%).
References
- Duckworth AD, Clement ND, White TO, Court-Brown CM, McQueen MM. Plate versus tension-band wire fixation for olecranon fractures: a prospective randomized trial. J Bone Joint Surg Am. 2017;99(15):1261-1273. doi:10.2106/JBJS.16.00773
- Ren YM, Qiao HY, Wei ZJ, et al. Efficacy and safety of tension band wiring versus plate fixation in olecranon fractures: a systematic review and meta-analysis. J Orthop Surg Res. 2016;11(1):137. doi:10.1186/s13018-016-0465-z
- Jia Y, Liu A, Guo T, et al. Efficacy and safety of tension band wire versus plate for Mayo II olecranon fractures: a systematic review and meta-analysis. J Orthop Surg Res. 2022;17(1):373. doi:10.1186/s13018-022-03262-7
- Gartsman GM, Sculco TP, Otis JC. Operative treatment of olecranon fractures. Excision or open reduction with internal fixation. J Bone Joint Surg Am. 1981;63(5):718-721. PMID:7240294
- Joshi MA, Le M, Campbell R, et al. Surgery for Olecranon Fractures in the Elderly (SOFIE): results of the SOFIE randomized controlled trial. J Bone Joint Surg Am. 2025;107(5):452-458. doi:10.2106/JBJS.24.00655
- Duckworth AD, Clement ND, McEachan JE, White TO, Court-Brown CM, McQueen MM. Prospective randomised trial of non-operative versus operative management of olecranon fractures in the elderly. Bone Joint J. 2017;99-B(7):964-972. doi:10.1302/0301-620X.99B7.BJJ-2016-1112.R2
- Carter TH, Molyneux SG, Reid JT, White TO, Duckworth AD. Tension-band wire fixation of olecranon fractures. JBJS Essent Surg Tech. 2018;8(3):e22. doi:10.2106/JBJS.ST.17.00071
- Duckworth AD, Clement ND, Aitken SA, Court-Brown CM, McQueen MM. The epidemiology of fractures of the proximal ulna. Injury. 2012;43(3):343-346. doi:10.1016/j.injury.2011.10.017
- Ring D, Jupiter JB, Sanders RW, Mast J, Simpson NS. Transolecranon fracture-dislocation of the elbow. J Orthop Trauma. 1997;11(8):545-550. doi:10.1097/00005131-199711000-00001