Largest Sesamoid | Tension Band Principle | Extension is Key
- Extensor mechanism function is key - can patient actively extend knee against gravity?
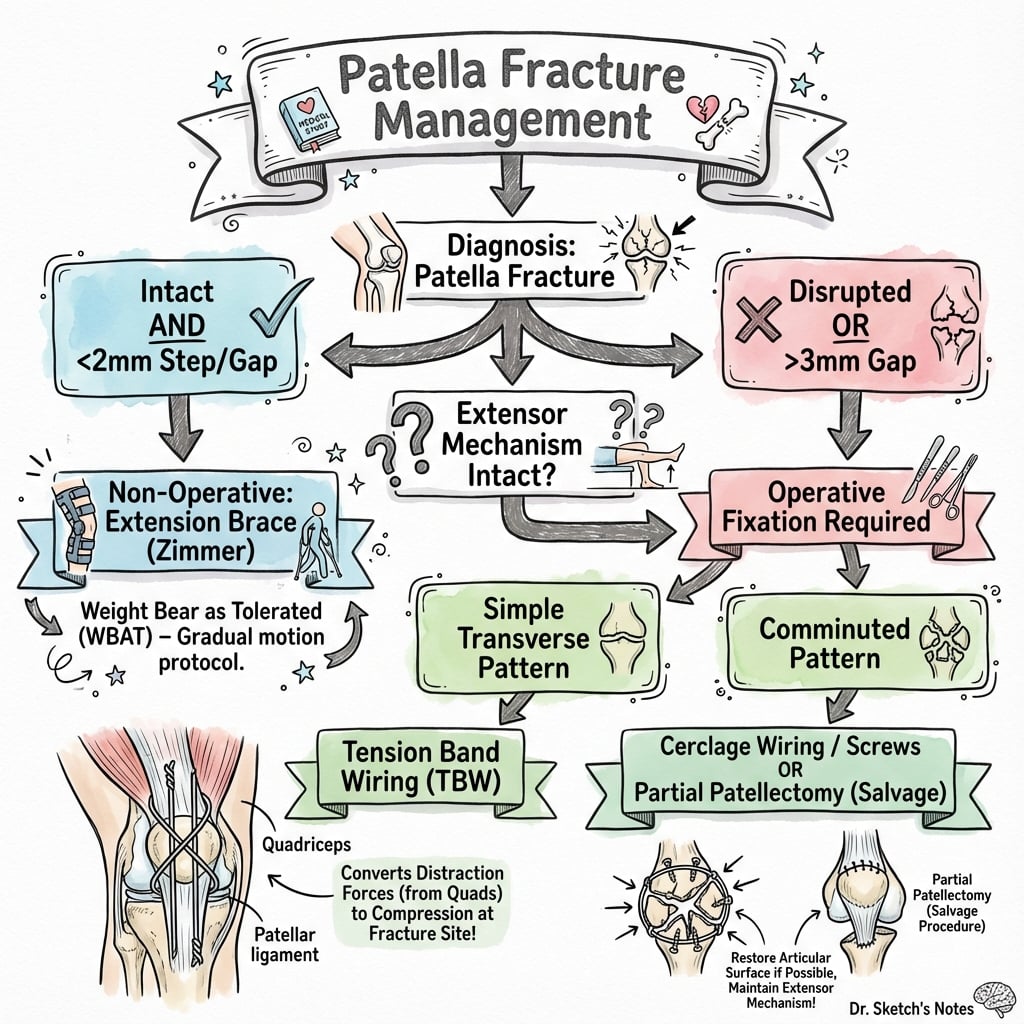
- Operative indications: displacement over 2-3mm, articular step over 2-3mm, loss of active extension
- Tension band principle: converts tensile force to compression at articular surface
- Tension band wiring (TBW) is classic, but screw fixation increasingly preferred for transverse
- Hardware removal common (50%) due to prominence - counsel patients preoperatively
- “50% of patients need hardware removal - wire prominence is main reason
- “Check active extension BEFORE giving analgesia - critical exam finding
- “Vertical fractures often stable (patella wide in sagittal plane)
- “Inferior pole excision + tendon repair = satisfactory if under 30% pole

Active straight leg raise is the key exam finding. Failed SLR = disrupted extensor mechanism = needs surgery. Test BEFORE giving analgesia - cannot assess after.
Surgery indicated for: Displacement over 2-3mm, articular step over 2mm, loss of active extension. Any doubt about extension = operative management.
Converts tensile forces to compressive forces at articular surface during knee flexion. This allows early motion and compression with loading.
50% require hardware removal - mainly K-wires/TBW prominence. Counsel patients preoperatively. Screw fixation may have lower removal rates.
- Key Assessment
- Can actively extend
- Treatment
- Cylinder cast/brace 4-6 weeks
- Pearl
- Weekly X-rays first 2 weeks
- Key Assessment
- Gap or step-off visible
- Treatment
- ORIF - TBW or cannulated screws
- Pearl
- Tension band principle applies
- Key Assessment
- Major fragments identifiable
- Treatment
- ORIF with multiple techniques
- Pearl
- Cerclage + TBW or basket plate
- Key Assessment
- Multiple small fragments
- Treatment
- Partial patellectomy + repair
- Pearl
- Preserve as much as possible
- Key Assessment
- Small pole, intact mechanism
- Treatment
- Excision + tendon repair
- Pearl
- Under 30% pole excised OK
GAPSOperative Indications
Hook:If there are GAPS, you need surgery!
COMPRESSTension Band Principle
Hook:The wire on the front COMPRESSES the joint as you bend the knee!
LEVERPatella Function
Hook:The patella is a LEVER that increases extension power!
WIREDTBW Construct
Hook:WIRED correctly means the patella will heal!
Overview and Epidemiology
Patella fractures test your understanding of the extensor mechanism, the tension band principle, and decision-making around fixation vs partial patellectomy. The examiner wants to hear you discuss biomechanics and early motion.
- Bimodal: Young (high-energy) and elderly (falls)
- Male:Female 2:1
- Peak age: 20-50 years
- Often isolated injury in direct blow
- Direct blow: Dashboard injury, fall on knee
- Indirect: Forceful eccentric contraction (landing)
- Combined: Most common - direct + muscle contraction
Anatomy and Biomechanics
The patella is the largest sesamoid bone in the body. It increases the lever arm of the extensor mechanism by up to 50%, improving quadriceps efficiency. Patellofemoral contact forces reach 3-7x body weight during stair descent.
Patella Anatomy
- Largest sesamoid in body
- Triangular with apex inferior
- Articular surface has lateral facet (larger) and medial facet
- Odd facet on far medial edge
- 3-7cm long, 2-3cm thick
- Quadriceps tendon inserts on superior pole
- Patellar tendon originates from inferior pole
- Medial retinaculum: VMO, MPFL
- Lateral retinaculum: VL, ITB fibers
- Expansions allow some extension even with fracture
Blood supply from superior and inferior genicular arteries forming an extraosseous anastomotic ring. Vessels enter mainly on the anterior surface and inferior pole. This is why anterior surgical approach is safe.
Classification Systems
Fracture Pattern Classification
- Frequency
- 50%
- Characteristics
- Central fracture, usually 2 fragments
- Treatment
- TBW or screws if displaced
- Frequency
- 30%
- Characteristics
- Multiple fragments, high-energy
- Treatment
- Reconstruct if possible, partial patellectomy if not
- Frequency
- 10%
- Characteristics
- Avulsion by patellar tendon
- Treatment
- Excision + repair if small, ORIF if large
- Frequency
- Rare
- Characteristics
- Avulsion by quads tendon
- Treatment
- ORIF or excision + repair
- Frequency
- 5%
- Characteristics
- Sagittal plane, often undisplaced
- Treatment
- Usually stable, conservative
- Frequency
- Rare
- Characteristics
- With patellar dislocation
- Treatment
- Fragment removal or fixation
A growing, distinct entity as knee arthroplasty numbers rise: the patella fracture after total knee replacement is managed by a different algorithm from the native fracture, classified (Goldberg / Ortiguera-Berry) by extensor-mechanism integrity and patellar-component fixation:
- Type I - extensor mechanism intact AND patellar component well-fixed: by far the commonest; treated non-operatively (brace, activity modification). Fixation of the thin, often avascular resurfaced patella has a high failure rate, so leaving a stable, extensor-intact fracture alone is the preferred course.
- Type II - extensor mechanism disrupted (regardless of component): needs ORIF / extensor-mechanism repair or reconstruction - the indication is the lost extension, exactly as in the native patella.
- Type III - loose/failed patellar component (IIIA reasonable bone stock, IIIB poor stock): requires component removal +/- revision, patelloplasty, or resection - fixing around a loose button does not work.
Why it matters: the resurfaced patella is thin and devascularised (especially after a lateral release), so periprosthetic fractures heal poorly and fixation often fails - hence the strong default to non-operative care for the common extensor-intact pattern and to revision/extensor reconstruction only when function or the implant demands it.
Exam point: a post-TKA patella fracture is classified by extensor-mechanism integrity and component fixation - intact extensor + stable component = non-operative (the rule, because fixation of the thin resurfaced patella fails), extensor disruption = repair/ORIF, loose component = revision.
Clinical Assessment
- Mechanism: Direct blow, fall, dashboard
- Ability to walk after injury
- Knee swelling - hemarthrosis if intra-articular
- Previous knee surgery or patella problems
- Occupation/sport - return to activity considerations
- Palpable gap at patella (indicates displacement)
- Hemarthrosis - tense effusion
- ACTIVE EXTENSION - straight leg raise (critical!)
- Retinacular integrity (can extend despite fracture?)
- Skin condition - may be open fracture
Active straight leg raise is the KEY clinical test. Perform BEFORE giving analgesia - pain inhibits accurate assessment. Failed SLR = disrupted extensor mechanism = operative indication regardless of displacement.
Some patients with patella fractures can still extend the knee via intact retinaculae (medial and lateral expansions). This doesn't mean the fracture is stable - X-ray and examination of gap still determine treatment.
Differential Diagnosis
- Distinguishing Features
- Palpable gap, hemarthrosis, failed SLR, sharp fracture margins
- Key Investigation
- Lateral radiograph
- Pitfall
- Confirm extension before analgesia
- Distinguishing Features
- No trauma or trivial injury, rounded sclerotic margins, often superolateral and bilateral
- Key Investigation
- AP radiograph plus contralateral comparison
- Pitfall
- Mistaking smooth corticated fragment for acute fracture
- Distinguishing Features
- Palpable infrapatellar gap, patella alta, failed SLR, no bony fracture line
- Key Investigation
- Lateral radiograph (patella alta), ultrasound or MRI
- Pitfall
- Attributing failed SLR to fracture when tendon is torn
- Distinguishing Features
- Suprapatellar gap, patella baja, failed SLR, often over 40 years
- Key Investigation
- Ultrasound or MRI
- Pitfall
- Missed in obese or swollen knee
- Distinguishing Features
- Lateral instability, MPFL tenderness, possible osteochondral fragment
- Key Investigation
- Skyline view, MRI for osteochondral injury
- Pitfall
- Overlooking osteochondral loose body
- Distinguishing Features
- Diffuse tenderness, intact SLR, no fracture line
- Key Investigation
- Radiograph (normal)
- Pitfall
- Over-treating a simple contusion
Investigations
Imaging Protocol
Lateral view is most important - shows displacement, gap, step-off. AP shows transverse vs vertical pattern. Get knee fully extended for accurate assessment.
Shows patellofemoral joint articular surface. Helps assess vertical fractures and chondral injury. May be difficult acutely due to pain.
For comminuted fractures to plan reconstruction. Assess posterior cortex integrity. 3D reconstructions helpful for operative planning.
Key X-ray Findings
- Measure displacement (gap between fragments)
- Articular step-off at patellofemoral joint
- Over 2-3mm separation = surgical indication
- May see hemarthrosis (joint effusion)
- Fracture pattern (transverse, vertical, comminuted)
- Width of patella
- Bipartite patella (DDx - typically superolateral)
- Osteochondral fragments if dislocated
Bipartite patella is present in 1-2% of population, usually superolateral fragment. Differentiate from fracture by: rounded margins, no hemarthrosis, bilateral comparison (often bilateral). Occasionally symptomatic without trauma.
"Restore patellar height" is a hollow instruction unless you can measure it - and patellar height is the number that tells you whether a comminuted-pole repair, a partial patellectomy, or a healed tendon has left the patient with a functionally normal extensor mechanism. The three classic lateral-radiograph ratios:
- Insall-Salvati ratio = patellar tendon length divided by patellar bone (pole-to-pole) length. Normal is roughly 0.8 to 1.2; a high ratio is patella alta, a low ratio is patella baja/infera. Independent of knee flexion angle, but it uses the patella's own length as the denominator - so it is unreliable after a fracture that shortens the patella or after a partial patellectomy, because the bony reference is no longer normal.
- Blackburne-Peel and Caton-Deschamps ratios reference the articular surface to the tibial plateau instead of patellar length, so they are the better choices when the patella itself has been altered by injury or excision.
Two examiner uses: (1) Setting tension at surgery - when you do a partial patellectomy or repair a comminuted inferior pole, you advance/repair the patellar tendon so the operated patella sits at the same height as the uninjured contralateral side (compare on a template/contralateral film); over-tightening creates iatrogenic patella baja (stiffness, anterior knee pain, loss of flexion) and under-tensioning leaves an extensor lag. (2) Diagnosing late failure - new patella alta after fixation signals patellar tendon rupture or fixation pull-out, while progressive baja signals over-shortening or contracture.
Exam point: quote Insall-Salvati ~0.8 to 1.2 as the normal patellar-height ratio, know that alta = high / baja = low, and recognise that Blackburne-Peel / Caton-Deschamps are preferred once the patella has been fractured or partially excised because they do not rely on the patella's own (now-abnormal) length.
Radiographic Examples
Management Algorithm
Operative indications: (1) Displacement over 2-3mm, (2) Articular step over 2mm, (3) Lost active extension. Non-operative only if: non-displaced (under 2mm), intact active extension, and patient compliant.
Conservative Management
Non-Operative Protocol
Cylinder cast or hinged knee brace locked in extension. Weight bearing as tolerated with brace.
Repeat X-ray to confirm no displacement. If displaced now, conversion to surgery.
If stable at 2 weeks, begin ROM exercises. Unlock brace gradually. Continue cylinder for walking.
Discard brace if X-ray shows healing. Quadriceps strengthening. Return to activity by 3 months.
Non-operative management requires: Displacement under 2mm, articular step under 2mm, intact active extension, and reliable patient for weekly X-rays initially (secondary displacement occurs).
Surgical Technique
Modified Tension Band Wiring
- Supine on radiolucent table
- Knee flexed over bolster or triangle
- Ensure full fluoroscopy access
- Longitudinal midline incision
- Preserve prepatellar bursa if possible
- Evacuate hematoma and debris
- Inspect articular surface
- Reduce fracture with pointed reduction clamps
- Assess articular congruity with palpation and fluoro
- Accept no more than 2mm step-off
- Two parallel 1.6-2.0mm K-wires
- Enter through superior pole, exit inferior pole
- Avoid articular penetration
- Wires parallel and medial-lateral to avoid impingement
- 18-gauge cerclage wire
- Pass through anterior cortex (not intramedullary)
- Figure-of-eight configuration around K-wire ends
- Twist anteriorly to compress fracture
- Bend K-wires and bury into bone
Proper technique ensures compression during knee flexion.


Complications
- Incidence
- Up to 50%
- Risk Factors
- TBW, thin soft tissue
- Management
- Planned second surgery counseling
- Incidence
- 10-20%
- Risk Factors
- Prolonged immobilization, poor rehab
- Management
- Early ROM, aggressive physio
- Incidence
- 40-50% long-term
- Risk Factors
- Articular damage, malreduction
- Management
- Activity modification, ?later arthroplasty
- Incidence
- 2-5%
- Risk Factors
- Poor fixation, comminution, infection
- Management
- Revision fixation or partial patellectomy
- Incidence
- 5-10%
- Risk Factors
- Poor fixation technique, early loading
- Management
- Revision ORIF
- Incidence
- 5-10%
- Risk Factors
- Lengthening of mechanism
- Management
- Quadriceps strengthening, rarely requires revision
- Incidence
- 1-2%
- Risk Factors
- Open fracture, multiple surgeries
- Management
- Washout, antibiotics, hardware removal if needed
50% of patients undergoing TBW require hardware removal (mainly K-wire prominence). Counsel patients preoperatively about likely second surgery. Screw fixation may have lower removal rate.
Postoperative Care and Rehabilitation
Post-ORIF Rehabilitation
Hinged knee brace. Immediate ROM exercises (tension band allows motion). Brace locked for walking. Heel slides, SLR with brace.
Increase ROM goal to 90° by week 4. Weight bearing as tolerated in brace. Pool therapy if available.
Discard brace as strength improves. Quadriceps strengthening progresses. Stationary biking.
Return to normal activity if X-ray shows union. Running at 3-4 months. Sport-specific by 4-6 months.
Tension band fixation is designed for early active motion. Knee flexion creates compression at articular surface, promoting healing. Prolonged immobilization leads to stiffness and poor outcomes.
Outcomes and Prognosis
Functional Outcomes
- Union Rate
- 95-98%
- Good Function
- 85-90%
- Key Issues
- Hardware removal common (50%)
- Union Rate
- 95-98%
- Good Function
- 85-90%
- Key Issues
- Lower removal rate (10%)
- Union Rate
- 85-95%
- Good Function
- 70-80%
- Key Issues
- Depends on articular restoration
- Union Rate
- N/A
- Good Function
- 70-80%
- Key Issues
- Up to 30% excision well tolerated
- Union Rate
- 95%+
- Good Function
- 85-90%
- Key Issues
- For undisplaced, intact mechanism
Prognostic Factors
Simple transverse pattern, Minimal articular comminution, Anatomic reduction achieved, Early ROM rehabilitation, Compliant patient
Comminuted pattern, Significant articular damage, Malreduction (over 2mm step-off), Prolonged immobilization, Open fracture or infection
Long-term Outcomes
Most patients achieve satisfactory outcomes with proper treatment. The main long-term issue is patellofemoral osteoarthritis, which develops in 40-50% of patients by 10-20 years. Hardware irritation requiring removal is the most common early complication with TBW. Extensor mechanism function is generally well preserved with modern fixation techniques. Total knee arthroplasty may eventually be required for severe post-traumatic arthritis.
Guidelines, Registries & Global Practice
- Account for approximately 1% of all skeletal fractures
- Bimodal: young adults from high-energy direct trauma (road traffic, falls from height, sport) and older adults from low-energy falls
- Male predominance in young cohorts; rising proportion in older women with osteoporosis
- Increasing periprosthetic patella fractures with the global growth in knee arthroplasty
- No dedicated international patella-fracture registry; evidence comes from trauma series and meta-analyses
- Pooled data favour cannulated-screw constructs over K-wire TBW for ROM, function and reoperation
- Implant-removal remains the dominant secondary procedure, driven by K-wire/cerclage prominence
- Periprosthetic patella fractures are captured indirectly via arthroplasty registries (NJR, AOANJRR, AJRR)
- Operative Threshold Emphasis
- Displacement over 2-3mm, articular step over 2mm, or extensor lag
- Preferred Construct Trend
- Tension band; screws + tension band for biomechanical superiority
- Distinctive Point
- Early active motion central to the tension band concept
- Operative Threshold Emphasis
- Loss of active extension or significant displacement
- Preferred Construct Trend
- Stable construct allowing early rehabilitation
- Distinctive Point
- Soft-tissue assessment and open-fracture pathways prioritised
- Operative Threshold Emphasis
- Extensor mechanism disruption or displacement over 2-3mm
- Preferred Construct Trend
- Shift toward low-profile screw / suture constructs
- Distinctive Point
- Strong emphasis on counselling re hardware removal
- Operative Threshold Emphasis
- Same displacement/step thresholds; individualise by bone quality
- Preferred Construct Trend
- Angular-stable plates for comminution
- Distinctive Point
- Plating gaining favour for multifragmentary patterns
- Cannulated-screw and screw-plus-tension-band constructs increasingly default for transverse patterns
- Angular-stable/mesh plates and suture-based fixation available for comminution and osteoporotic bone
- CT and 3D planning routine for complex patterns
- K-wire tension band wiring remains the workhorse - cheap, available, effective
- Implant cost and supply may dictate technique over biomechanical ideal
- Higher burden of neglected fractures and aseptic nonunion presenting late
Key documentation (globally applicable): (1) Active extension tested BEFORE analgesia given, (2) Displacement and articular step measured on a good-quality lateral radiograph, (3) Informed consent including the high hardware-removal likelihood, particularly for K-wire TBW, (4) A defined serial-radiograph protocol for non-operative management. Missed secondary displacement in non-operative cases is a recognised source of litigation worldwide.
Controversies and Areas of Uncertainty
K-wire tension band wiring is being displaced by cannulated-screw constructs in the literature, yet TBW remains widespread because it is cheap and familiar. The debate is how strongly to recommend screws given largely retrospective comparative data.
Whether symptomatic-only or routine removal is best after TBW is unsettled. Removal rates up to half of TBW cases drive interest in lower-profile constructs, but elective removal carries its own morbidity.
For comminuted inferior pole fractures, separate vertical wiring / suture anchor reconstruction preserves patellar height, whereas partial patellectomy is simpler. Long-term data support both, and the threshold for excision varies between surgeons.
All-suture and suture-anchor constructs avoid metalwork irritation and show promising early results, but high-level comparative evidence on union and re-displacement is still limited.
MCQ Practice Points
Q: By how much does the patella increase the extensor mechanism moment arm? A: 30-50%. The patella acts as a lever (sesamoid) that increases the quadriceps moment arm, improving efficiency. Patellectomy significantly weakens extension.
Q: What displacement threshold indicates need for surgical fixation of patella fractures? A: Greater than 2-3mm fracture displacement or greater than 2mm articular step. Loss of active extension is also an absolute indication regardless of displacement.
Q: What is the principle behind tension band wiring? A: The wire is placed on the tension side (anterior) of the patella. During knee flexion, the tensile forces are converted to compressive forces at the articular surface, promoting healing.
Q: What percentage of patients require hardware removal after TBW? A: Up to 50%. This is mainly due to K-wire prominence causing anterior knee pain. Cannulated screw fixation has lower removal rates due to lower profile.
Q: What percentage of the patella can be safely excised without significant functional loss? A: Up to 30% of the inferior pole. Beyond 50% excision, extensor strength is significantly compromised. Total patellectomy results in 30% strength loss.
Q: What is the most common patella fracture pattern? A: Transverse fracture (50%). This is followed by comminuted (30%), polar fractures (10-15%), and vertical (5%). Transverse fractures are typically fixed with TBW or screws.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man falls off a ladder onto his knee. He cannot straighten his leg. X-ray shows a transverse patella fracture with 5mm of displacement. He is otherwise healthy. What is your management?”
“A 50-year-old woman trips and falls onto her knee. X-ray shows a comminuted inferior pole patella fracture with multiple small fragments (largest 1cm). She cannot actively extend. CT confirms 4 small fragments making up the inferior 25% of the patella. How would you manage this?”
“A 65-year-old diabetic woman presents after tripping on a rug. She has painful knee swelling but can actively extend her knee (demonstrated straight leg raise in ED before analgesia was given). X-ray shows a transverse patella fracture with approximately 1-2mm of displacement. How would you manage this?”
Key Anatomy
- Largest sesamoid bone
- Increases extensor moment arm by 30-50%
- Blood supply: genicular arteries, anterior
- Thickest articular cartilage (5-7mm)
Operative Indications (GAPS)
- Gap over 2-3mm displacement
- Active extension lost (failed SLR)
- Patellofemoral step over 2mm
- Surgery for any of the above
Tension Band Principle
- Wire placed ANTERIOR to fracture
- Converts tensile to compressive force
- Allows early ROM (motion = compression)
- Only works if posterior cortex intact
Fixation Options
- TBW: K-wires + figure-8 wire (classic)
- Cannulated screws: lower profile, less removal
- Basket plates: for comminuted fractures
- Partial patellectomy: non-reconstructable poles
Complications
- Hardware removal: 50% for TBW
- Patellofemoral OA: 40-50% long-term
- Stiffness: if immobilized too long
- Extensor lag: if lengthened mechanism
Important Numbers
- 2-3mm: displacement threshold for surgery
- 2mm: step-off threshold for surgery
- 30%: pole excision acceptable
- 50%: hardware removal rate TBW
Evidence Base and Key Trials
The modern literature has shifted decisively: multiple 2025-2026 meta-analyses now show cannulated screw constructs (with or without a tension band) outperform K-wire tension band wiring on knee ROM, functional scores, complications and reoperation. Quote a meta-analysis plus the Carpenter biomechanical rationale and you cover both the "what" and the "why".
Cannulated Screw vs K-wire Tension Band - Meta-Analysis
- Systematic review and meta-analysis of 11 studies, 1,358 patients
- No difference in operative time, healing time or VAS pain
- Cannulated screw tension band gave superior knee ROM (MD 7.16 degrees) and Lysholm scores (MD 4.80)
- Reoperation (OR 5.14) and overall complications (OR 14.19) markedly lower with cannulated screws
Cannulated Screws +/- Tension Band vs TBW - Meta-Analysis
- 14 studies comparing TBW, cannulated screws (CS) and CS + tension band wire (CSTBW)
- CSTBW gave better 3-month flexion (SMD 0.92) and 3-month VAS (SMD -1.27) than TBW
- 12-month Lysholm favoured CSTBW (SMD 0.80)
- Complications and implant removal more frequent with TBW
Biomechanics of Patella Fixation Techniques
- Cadaveric RCT comparing modified tension band, parallel lag screws, and screws plus tension band
- Modified tension band displaced significantly more in simulated extension than either screw construct
- Screws plus tension band failed at highest load (mean 732 N) vs screws alone (554 N) and TBW (395 N)
- Cannulated screws allow simple, reliable addition of a tension band