MPFL | Trochlear Dysplasia | TT-TG Distance | Surgical Options
- MPFL is the PRIMARY soft tissue restraint to lateral patellar translation (50-60%)
- MPFL ruptures in almost ALL acute patellar dislocations
- TT-TG greater than 20mm indicates lateral malalignment needing tibial tubercle osteotomy
- Trochlear dysplasia is the most common anatomical risk factor
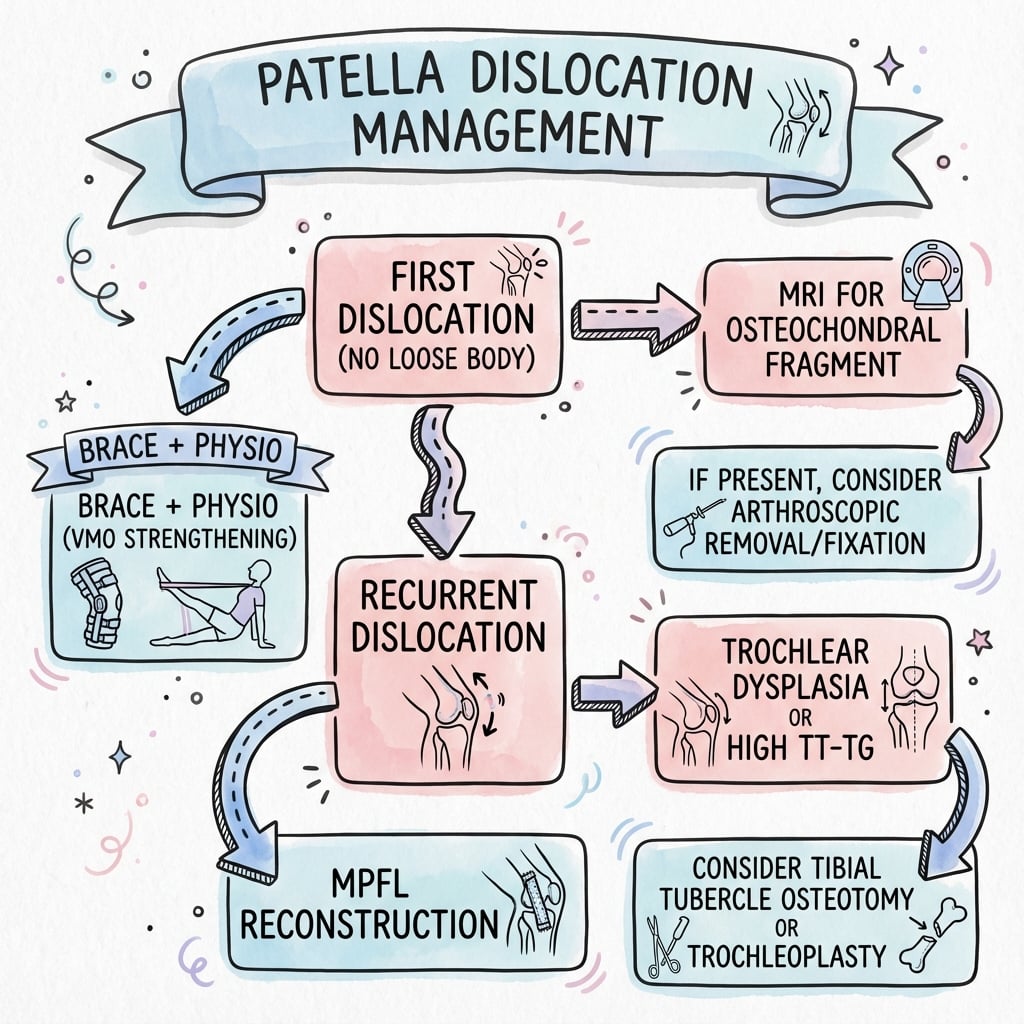
- First-time dislocators: conservative unless loose body or osteochondral fragment
- “MPFL attaches just distal to adductor tubercle on femur
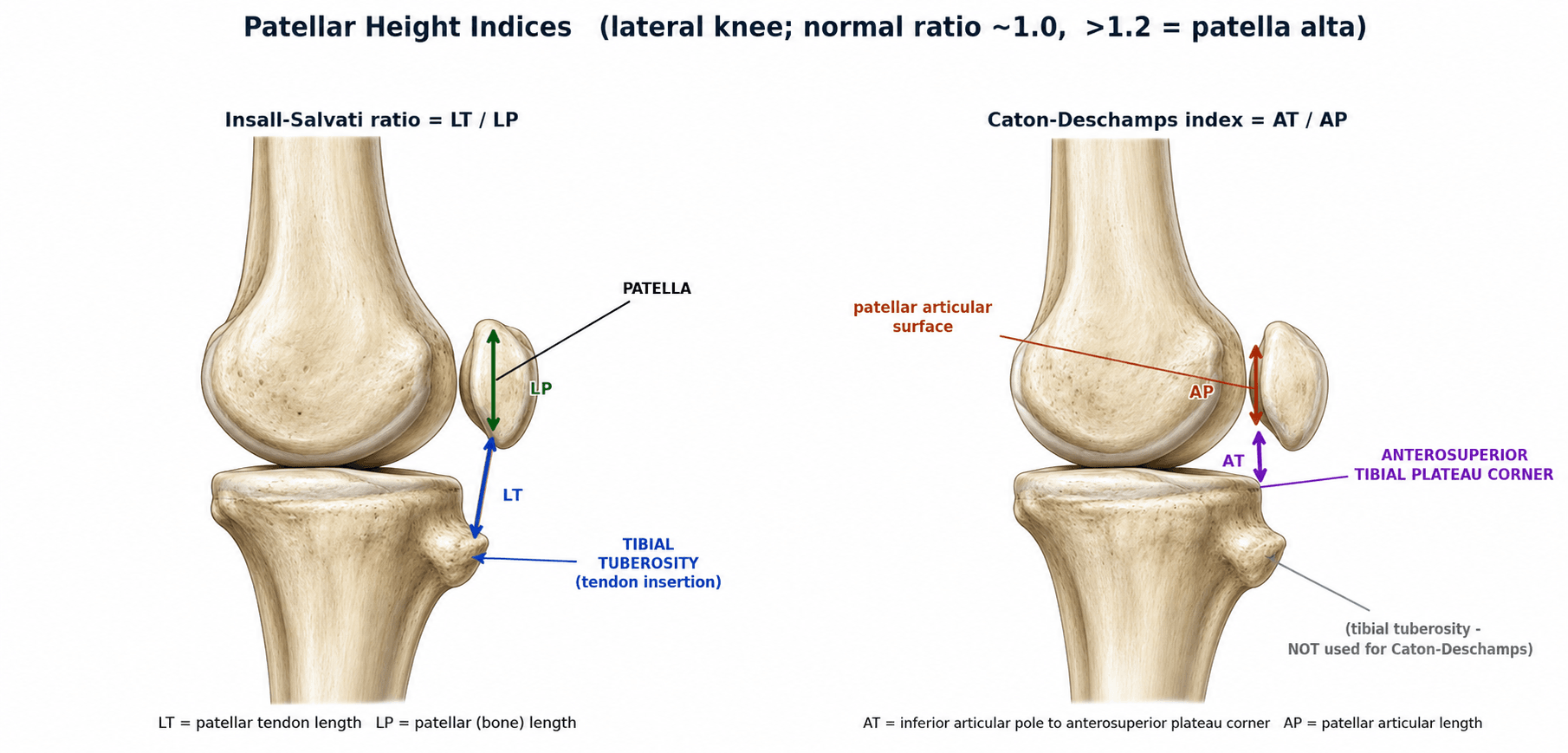
- “Patella alta (Insall-Salvati greater than 1.2) increases instability
- “Recurrence rate 50% after first dislocation, 80% after second
- “Combined procedures often needed for significant anatomical abnormalities
MPFL provides 50-60% of restraint to lateral patellar translation in the first 30° of flexion. It ruptures in almost all acute dislocations and is the target of surgical reconstruction.
Must assess ALL factors: Trochlear dysplasia, patella alta, increased TT-TG distance, femoral anteversion, genu valgum, rotational malalignment. Failure to address leads to recurrence.
Normal is less than 20mm. Greater than 20mm = pathological lateral offset. Indicates need for tibial tubercle osteotomy (medialization +/- distalization) in addition to MPFL reconstruction.
Most first-time dislocators: conservative treatment. Surgery indicated for: osteochondral loose body, large chondral/MPFL avulsion, recurrent instability, or high-risk anatomy.
- Key Factor
- No loose body
- Treatment
- Conservative 6 weeks
- Additional Procedures
- None usually
- Key Factor
- Osteochondral fragment
- Treatment
- Surgery - fix fragment + MPFL
- Additional Procedures
- Address fragment
- Key Factor
- Normal anatomy
- Treatment
- MPFL reconstruction
- Additional Procedures
- May be sufficient alone
- Key Factor
- TT-TG greater than 20mm
- Treatment
- MPFL + tibial tubercle osteotomy
- Additional Procedures
- Medialization required
- Key Factor
- Severe dysplasia (B-D)
- Treatment
- MPFL + consider trochleoplasty
- Additional Procedures
- Bony correction needed
PATELLAAnatomical Risk Factors
Hook:The PATELLA itself tells you all the risk factors!
SAFEMPFL Femoral Attachment
Hook:SAFE femoral tunnel placement is essential for MPFL reconstruction!
FLAPIndications for Surgery After First Dislocation
Hook:Fix the FLAP - surgical indications after first dislocation!
Overview and Epidemiology
First dislocation: 50% recurrence risk. Second dislocation: 80%+ recurrence risk. This dramatic increase after second dislocation justifies earlier surgical intervention in recurrent cases. Anatomical risk factors predict higher recurrence.
- Incidence: 7-77 per 100,000/year
- Peak age: 15-19 years (adolescents)
- Females greater than males in some studies
- Often during sports/pivoting activities
- Strong association with anatomical abnormalities
- Twisting on planted foot with knee flexed
- Valgus force with external rotation
- Direct blow to medial patella (rare)
- May occur with minimal trauma if dysplastic
- MPFL ruptures in essentially all cases
Predicting Recurrence: Instability Risk Scores
The "50% after a first dislocation" figure is an average — validated composite scores stratify the individual risk and help decide who to stabilise early rather than relying on dislocation count alone.
- Patellar Instability Severity Score (Balcarek) — a points-based score combining skeletal immaturity/young age, bilateral instability, trochlear dysplasia grade (Dejour), patellar height (Caton-Deschamps) and TT-TG distance. Higher total scores predict markedly higher redislocation risk and support earlier stabilisation in first-time dislocators with high-risk anatomy.
- Recurrent Instability of the Patella (RIP) score (Hevesi/Krych) — stratifies first-time dislocators using skeletal immaturity (open physes), trochlear dysplasia (sulcus depth) and tubercle lateralisation / patellar height; a high-risk profile carries a substantially elevated recurrence rate.
These tools operationalise the same message: it is the bundle of anatomical risk factors (dysplasia + alta + raised TT-TG + immaturity), not simply the number of dislocations, that drives recurrence.
Pathophysiology and Anatomy
Medial Patellofemoral Ligament
Provides 50-60% of restraint to lateral patellar translation in first 30° of flexion.
Between adductor tubercle and medial epicondyle (Schoettle point).
Proximal 2/3 of medial patella border, blends with VMO.
Approximately 55mm.
Most important in early flexion (0-30°) when patella not yet in trochlea.
Correct femoral tunnel placement is CRITICAL for MPFL reconstruction. The Schoettle point is just distal and anterior to the adductor tubercle, between the posterior cortex of the medial femoral condyle and the posterior edge of Blumensaat line. Malposition leads to graft failure or patellofemoral overload.
Classification Systems
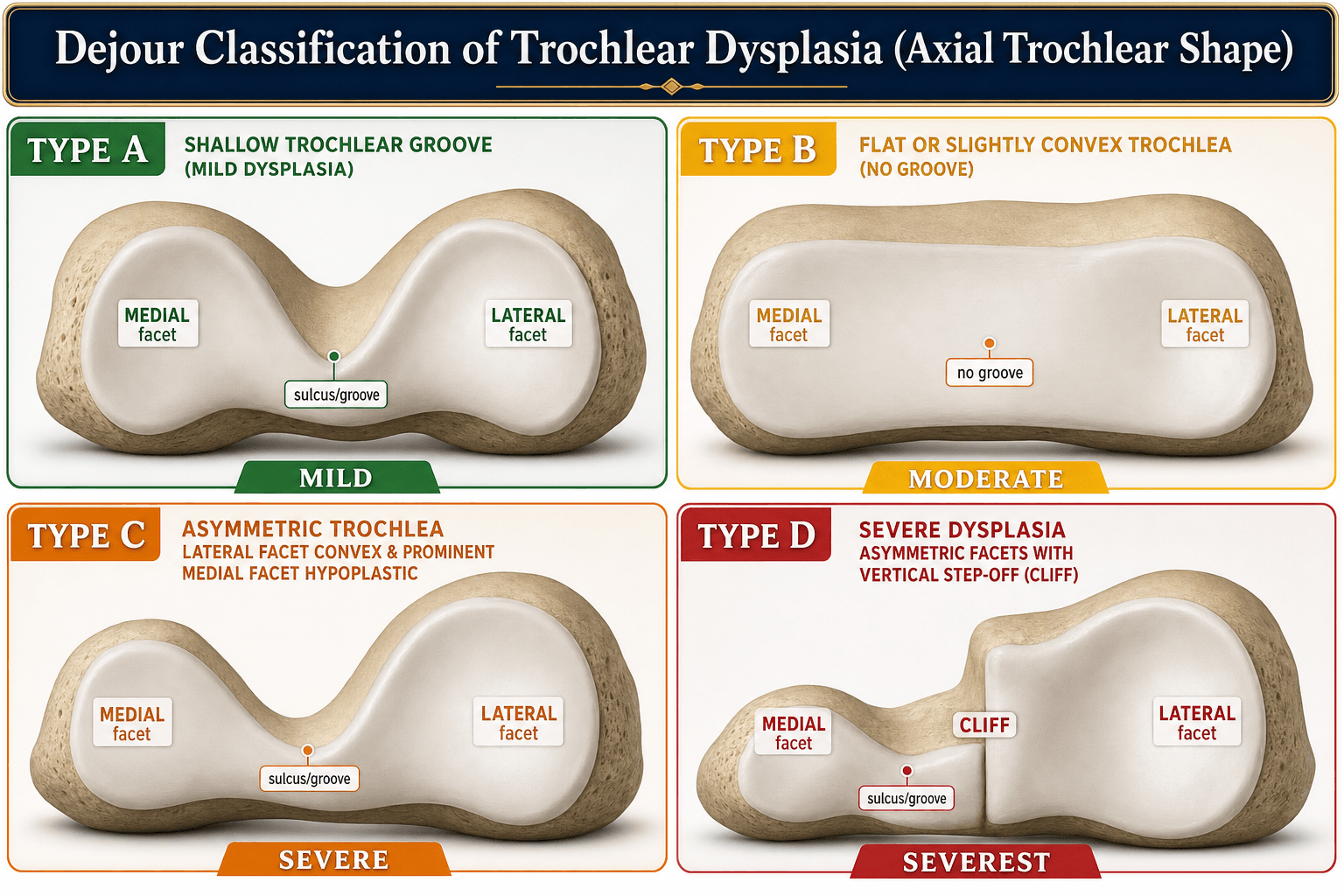
Dejour Trochlear Dysplasia Classification
- Radiograph/CT Finding
- Crossing sign only
- Trochlear Morphology
- Shallow trochlea
- Surgical Implication
- MPFL may suffice
- Radiograph/CT Finding
- Crossing sign + supratrochlear spur
- Trochlear Morphology
- Flat trochlea
- Surgical Implication
- Consider bony procedure
- Radiograph/CT Finding
- Crossing sign + double contour
- Trochlear Morphology
- Asymmetric facets
- Surgical Implication
- Bony procedure likely needed
- Radiograph/CT Finding
- All above + cliff pattern
- Trochlear Morphology
- Convex trochlea
- Surgical Implication
- Trochleoplasty may be needed
Crossing sign: Trochlear groove crosses anterior femoral cortex on lateral radiograph (most sensitive finding).
Clinical Assessment
- Mechanism: Twisting, pivoting injury
- Sensation: Often describe patella moving laterally
- Spontaneous reduction: Usually reduces on extension
- Swelling: Immediate hemarthrosis common
- Previous dislocations: Recurrence history
- Effusion: Hemarthrosis if acute
- Apprehension test: Positive with lateral pressure
- J-sign: Lateral tracking in terminal extension
- Q-angle: Increased suggests malalignment
- Generalized laxity: Beighton score
With the knee in 30° flexion, apply lateral force to the patella. Positive test: patient resists or shows apprehension (fear of dislocation). This is the most reliable clinical sign of patellofemoral instability.
Examination Checklist
Valgus, femoral anteversion, tibial torsion.
J-sign, lateral tilt, subluxation.
Beighton score for generalized hypermobility.
Often bilateral predisposition.
Investigations
Standard Views
Valgus alignment assessment.
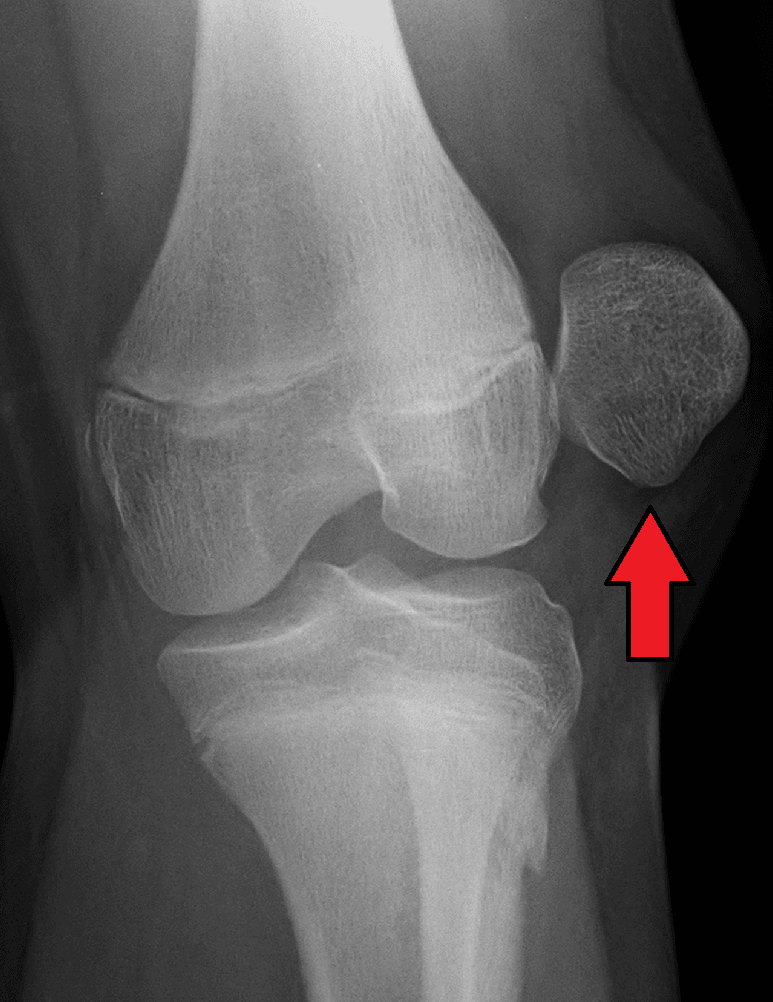
Trochlear dysplasia (crossing sign, supratrochlear spur), patella alta (Insall-Salvati).
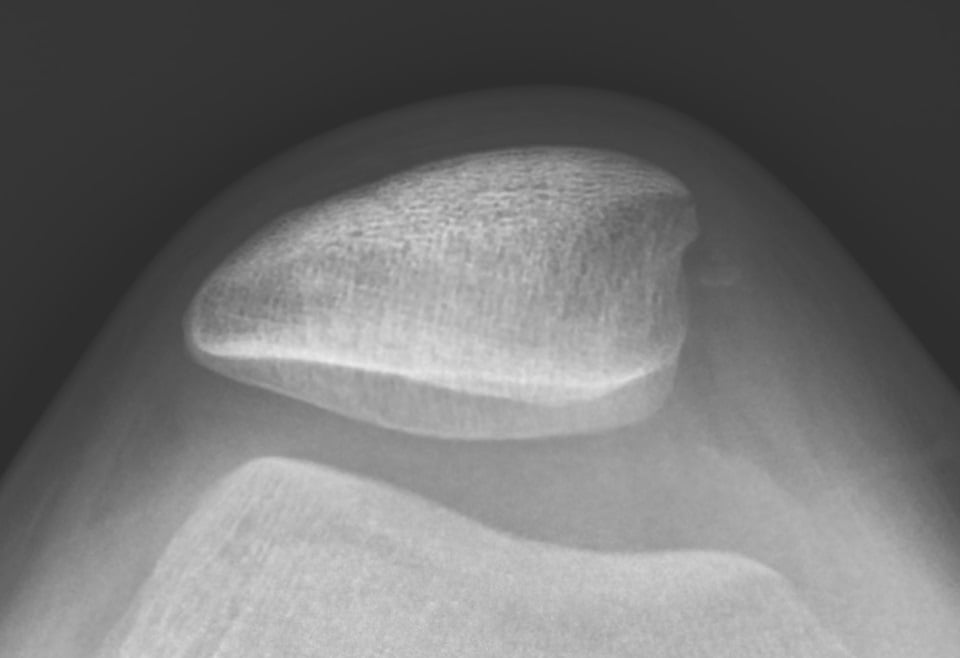
Patellar tilt, subluxation, trochlear morphology.
If considering osteotomy for valgus.
Crossing sign on lateral is most sensitive for dysplasia.
Acute patellar dislocation MRI: MPFL tear (usually femoral side), bone marrow edema medial patella AND lateral femoral condyle (kissing contusion pattern), possible osteochondral fragment, hemarthrosis. This pattern is pathognomonic.
Differential Diagnosis
- Key History
- Lateral give-way on pivot, visible/felt patellar shift
- Examination
- Positive apprehension, J-sign
- Discriminator
- Reduces on extension; medial patella/lateral condyle bone bruise on MRI
- Key History
- Anterior pain with stairs/sitting, no true dislocation
- Examination
- Pain on patellar compression, no apprehension
- Discriminator
- No instability event or apprehension
- Key History
- Pivot injury, audible pop, rapid effusion
- Examination
- Positive Lachman/pivot shift
- Discriminator
- Anterior tibial translation, not patellar shift
- Key History
- Medial click/snapping, no frank dislocation
- Examination
- Palpable tender medial band
- Discriminator
- Mechanical snapping without apprehension
- Key History
- Sudden inability to extend, palpable gap
- Examination
- Extensor lag, patella alta/baja
- Discriminator
- Loss of active extension
- Key History
- Locking, catching after injury
- Examination
- Effusion, locking
- Discriminator
- Loose body on imaging - may coexist with dislocation
Management Algorithm
First-Time Patellar Dislocation
Management Pathway
Usually self-reduces with knee extension. Aspiration if tense effusion. Radiographs to rule out fracture/loose body. MRI to assess MPFL and osteochondral injury.
If no loose body: brace in extension 2-4 weeks, then progressive ROM and quadriceps strengthening. Full recovery 6-12 weeks. 50% recurrence risk with conservative treatment.
Osteochondral loose body (fix or remove), large bony MPFL avulsion, high-risk anatomy, or professional athlete may warrant early MPFL repair or reconstruction.
Conservative treatment is appropriate for most first-time dislocators without loose bodies.
Surgical Technique
MPFL Reconstruction Technique
Surgical Steps
Gracilis or semitendinosus autograft (most common). Allograft option. Quadriceps tendon strip gaining popularity.
Two tunnels in proximal 2/3 of medial patella. Suture anchors or interference screws. Avoid full-thickness tunnels.
Schoettle point: between adductor tubercle and medial epicondyle. Fluoroscopy to confirm (intersection of posterior femoral cortex and Blumensaat line).
Tension with knee at 30-60° flexion. Avoid overtensioning (causes PF overload). Confirm full flexion and patella tracking before final fixation.
Correct femoral tunnel placement is THE most important technical factor. The Schoettle point on fluoroscopy: where the posterior femoral cortex line meets the posterior extent of Blumensaat line. Anterior or distal malposition causes graft failure or patellofemoral overload.
Overtensioning the MPFL graft leads to increased patellofemoral contact pressures and accelerated cartilage wear. Tension with knee in 30-60° flexion, ensure patella can still translate one quadrant laterally, and confirm full flexion before final fixation.
Complications
- Cause
- Missed anatomical factor, tunnel malposition
- Prevention
- Address all risk factors, correct tunnel placement
- Management
- Revision surgery addressing missed factors
- Cause
- Overtensioned graft, tunnel malposition
- Prevention
- Proper tensioning, correct tunnel position
- Management
- Graft release, revision if severe
- Cause
- Overtensioning, prolonged immobilization
- Prevention
- Early ROM, proper tensioning
- Management
- Physical therapy, MUA if needed
- Cause
- Full-thickness patellar tunnels
- Prevention
- Partial thickness tunnels or anchors
- Management
- ORIF
- Cause
- Tunnel malposition, early return to sport
- Prevention
- Correct technique, appropriate rehab
- Management
- Revision reconstruction
Femoral tunnel malposition is the most common cause of MPFL reconstruction failure. Anterior or distal placement changes graft isometry, leading to graft laxity in flexion or patellofemoral overload. Always confirm Schoettle point with intraoperative fluoroscopy.
Postoperative Care
Rehabilitation Protocol
Brace locked in extension for ambulation. ROM exercises 0-90° out of brace. WBAT with crutches. CPM if available.
Progressive ROM to full. Unlock brace. Wean crutches. Quadriceps strengthening, VMO focus. No resisted knee extension 0-45°.
Full weight-bearing, no brace. Progressive closed chain strengthening. Stationary bike, pool exercises.
Running at 3-4 months if strength adequate. Sport-specific training. Full return 6-9 months.
If TTO performed: protected weight-bearing for 6-8 weeks until osteotomy healed. Confirm radiographic healing before advancing to full weight-bearing. May delay return to sport.
Outcomes and Prognosis
Prognostic Factors
- Isolated MPFL rupture without dysplasia
- Normal TT-TG distance
- First or second dislocation
- Compliance with rehabilitation
- Correct surgical technique
- Severe trochlear dysplasia (Dejour C-D)
- Multiple dislocations with cartilage damage
- Uncorrected anatomical abnormalities
- Generalized ligamentous laxity
- Tunnel malposition
Guidelines, Registries & Global Practice
Global Epidemiology
- Incidence of first-time patellar dislocation approximately 5.8-7 per 100,000 overall, rising to 29-77 per 100,000 in adolescents aged 10-17.
- Peak incidence 15-19 years; sex distribution roughly equal, with the highest single-group risk in females aged 10-17 (Fithian cohort).
- The majority of patients carry 2 or more anatomical risk factors; trochlear dysplasia is present in around 85% of recurrent cases.
Society Guidance, Side by Side
- First Dislocation
- Non-operative unless osteochondral fragment or loose body
- Recurrent Instability
- MPFL reconstruction favoured over repair
- Bony Correction
- TTO when TT-TG elevated; trochleoplasty selectively
- First Dislocation
- Rehabilitation first-line; image to exclude fragment
- Recurrent Instability
- Reconstruction with anatomical femoral tunnel
- Bony Correction
- Address dysplasia/alta at high-volume centres
- First Dislocation
- Non-operative default; early surgery if APIFs plus fragment
- Recurrent Instability
- Reconstruction; a-la-carte philosophy
- Bony Correction
- Trochleoplasty established for high-grade (Dejour B-D)
- First Dislocation
- Individualised risk stratification
- Recurrent Instability
- Correct ALL contributing factors
- Bony Correction
- Bony procedures driven by measurements, not reflex
The unifying global theme is an "a-la-carte" or menu-based philosophy (popularised by the Lyon/Dejour school and endorsed across ESSKA): identify every contributing factor and correct each one, rather than applying a single operation to all patients.
- No dedicated arthroplasty-style registry exists for patellar instability; evidence is driven by RCTs, cohorts and meta-analyses.
- Pooled MPFL reconstruction redislocation approximately 1-2% (Schneider meta-analysis).
- Trochleoplasty recurrence approximately 2.4% but with 17-27% rates of stiffness/OA/reoperation (Leclerc meta-analysis).
- High-resource: routine MRI plus CT for TT-TG, intra-operative fluoroscopy, trochleoplasty at specialist centres, allograft availability.
- Limited-resource: diagnosis on plain radiographs and clinical exam; gracilis/semitendinosus autograft preferred (no allograft cost); trochleoplasty rarely available - reconstruction plus TTO is the workhorse.
- Adjustable-loop or anchor fixation chosen by availability; the anatomical Schöttle target remains universal regardless of fixation device.
Patellofemoral instability is a common viva topic. Know the MPFL anatomy, TT-TG threshold (20mm), Dejour classification, and be able to articulate a systematic "a-la-carte" approach to surgical planning that addresses every anatomical abnormality.
Controversies and Areas of Uncertainty
Acute repair reduces redislocation in high-risk children (Askenberger RCT) but most data favour reconstruction for established recurrent instability. The role of repair in adults remains debated.
TT-TG of 20mm is a guide, not an absolute cut-off. Borderline values (15-20mm), TT-PCL, patellar height and dysplasia must be weighed together. Over-medialisation risks medial overload and arthrosis.
Highly effective for dislocation control in Dejour B-D, but the 17-27% rates of stiffness, OA and reoperation, plus a steep learning curve, keep it confined to specialist centres. The threshold for offering it is not standardised.
In open physes, femoral tunnels risk physeal injury and growth disturbance. Physeal-sparing or soft-tissue techniques are preferred, and TTO is generally deferred until skeletal maturity.
MCQ Practice Points
Q: What percent of restraint to lateral patellar translation does the MPFL provide? A: 50-60% of restraint in the first 30° of flexion. It is the primary soft tissue restraint and ruptures in almost all acute dislocations.
Q: What TT-TG distance is considered pathological? A: Greater than 20mm. This indicates need for tibial tubercle medialization in addition to MPFL reconstruction.
Q: What is the recurrence rate after a first patellar dislocation treated conservatively? A: Approximately 50%. After a second dislocation, the rate increases to 80%+.
Q: Where does the MPFL attach on the femur? A: Between the adductor tubercle and medial epicondyle at the Schoettle point. This is just distal and anterior to the adductor tubercle.
Q: What Insall-Salvati ratio indicates patella alta? A: Greater than 1.2. Normal is 0.8-1.2. Patella alta delays patellar engagement in the trochlea.
Q: What radiographic finding is common to all Dejour types of trochlear dysplasia? A: The crossing sign - where the trochlear groove line crosses the anterior femoral cortex on lateral radiograph.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 16-year-old netball player presents after her knee gave way while pivoting. She felt the patella move laterally and it reduced when she extended her knee. There is a moderate effusion. Radiographs show no fracture. How would you manage this?”
“A 22-year-old woman has had 4 patellar dislocations in the past 2 years. Examination shows positive apprehension, no significant valgus. CT shows TT-TG of 24mm. Radiographs show Dejour Type A trochlear dysplasia. What would you recommend?”
“A 19-year-old male had MPFL reconstruction 18 months ago but has had 2 further dislocations since. Examination shows persistent apprehension. CT shows TT-TG of 16mm. Review of operative notes shows the femoral tunnel was placed at the medial epicondyle. What is your assessment?”
MPFL Anatomy
- Primary restraint 50-60% (first 30° flexion)
- Femoral attachment: Schoettle point
- Between adductor tubercle and medial epicondyle
- Ruptures in almost all acute dislocations
Risk Factors (PATELLA)
- Patella alta (Insall-Salvati greater than 1.2)
- Anteversion (femoral)
- Trochlear dysplasia (Dejour A-D)
- Excessive TT-TG (greater than 20mm)
Measurements
- TT-TG: Normal less than 20mm
- Insall-Salvati: Normal 0.8-1.2
- Crossing sign: Trochlear dysplasia marker
- Sulcus angle: greater than 145° = dysplasia
Treatment Algorithm
- First dislocation no loose body: Conservative
- Recurrent, normal anatomy: MPFL reconstruction
- TT-TG greater than 20mm: MPFL + TTO medialization
- Patella alta: MPFL + TTO distalization
MPFL Reconstruction Keys
- Femoral tunnel at Schoettle point (CRITICAL)
- Tension at 30-60° flexion
- Avoid overtensioning
- Confirm full flexion before fixation
Prognosis
- 50% recurrence after 1st dislocation
- 80%+ recurrence after 2nd dislocation
- 80-95% success with MPFL reconstruction
- Tunnel malposition = most common failure cause
Evidence Base and Key Studies
Epidemiology and Natural History of Acute Patellar Dislocation
- Prospective cohort of 189 patients followed 2-5 years
- First-time dislocators had a 17% recurrent instability rate during follow-up
- Patients with a prior history of instability had a 49% recurrence rate
- Prior instability conferred 6.6x higher odds of further episodes; risk highest in females aged 10-17
Outcomes After Isolated MPFL Reconstruction (Meta-analysis)
- Systematic review and meta-analysis of 14 studies
- Pooled recurrent instability after isolated MPFL reconstruction only 1.2% (95% CI 0.3-2.1%)
- 84.1% of patients returned to sport; mean postoperative Kujala 85.8
- Reoperation risk 3.1%; positive apprehension sign in 3.6%
MPFL Repair vs Brace After First-Time Dislocation (RCT)
- Randomised controlled trial of 74 skeletally immature children (9-14 years)
- Redislocation rate 22% after arthroscopic MPFL repair vs 43% with knee brace (P = 0.047)
- Repair did NOT improve subjective or objective knee function over bracing
- 81% of patients had 2 or more anatomical patellar instability risk factors
Factors of Patellar Instability (Landmark Classification Paper)
- Analysed 143 unstable knees vs control radiographs/CT
- Trochlear dysplasia present in 85% (crossing sign in 96%) - the dominant factor
- TT-TG distance pathological (20mm or more) in 56% of unstable knees
- Patella alta (Caton-Deschamps 1.2 or more) in 24%; factors seen in only 3-6.5% of controls
Radiographic Landmark for the MPFL Femoral Tunnel (Schöttle Point)
- Cadaveric study of 8 knees defining the radiographic femoral insertion
- Point lies 1mm anterior to the posterior cortex extension line
- 2.5mm distal to the posterior origin of the medial femoral condyle
- Proximal to the most posterior point of the Blumensaat line on a true lateral
Trochleoplasty Outcomes and Complications (Meta-analysis)
- Meta-analysis of 28 studies and 1000 trochleoplasty procedures
- Overall recurrent dislocation rate only 2.4%
- Dejour deepening trochleoplasty most effective (1 recurrence in 349 knees, 0.28%)
- Patellofemoral osteoarthritis 27%, stiffness 7%, further surgery 17%
TT-PCL Distance Threshold (Systematic Review)
- Systematic review of 4 studies (300 unstable knees, 144 control knees)
- Mean TT-PCL 21.1mm in instability vs 18.8mm in controls (P less than 0.0001)
- Moderate-to-strong correlation between TT-PCL and TT-TG on MRI
- Excellent inter- and intra-observer reliability; pathological threshold of 21mm advocated