Dashboard Injury | Posterior Drawer | Isolated vs Combined
- PCL is PRIMARY restraint to posterior tibial translation
- Dashboard injury = flexed knee against dashboard
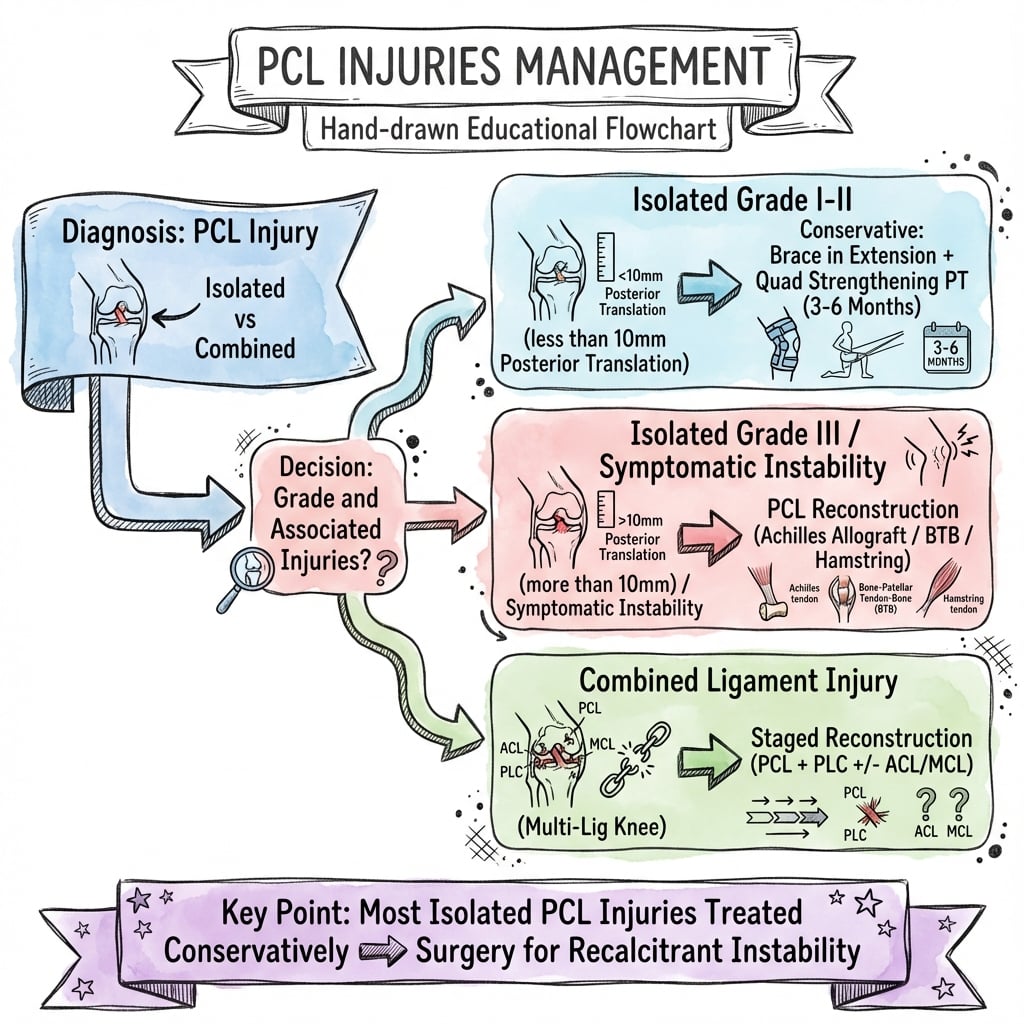
- Isolated Grade I-II injuries often do well non-operatively
- Combined injuries (especially with PLC) = surgical indication
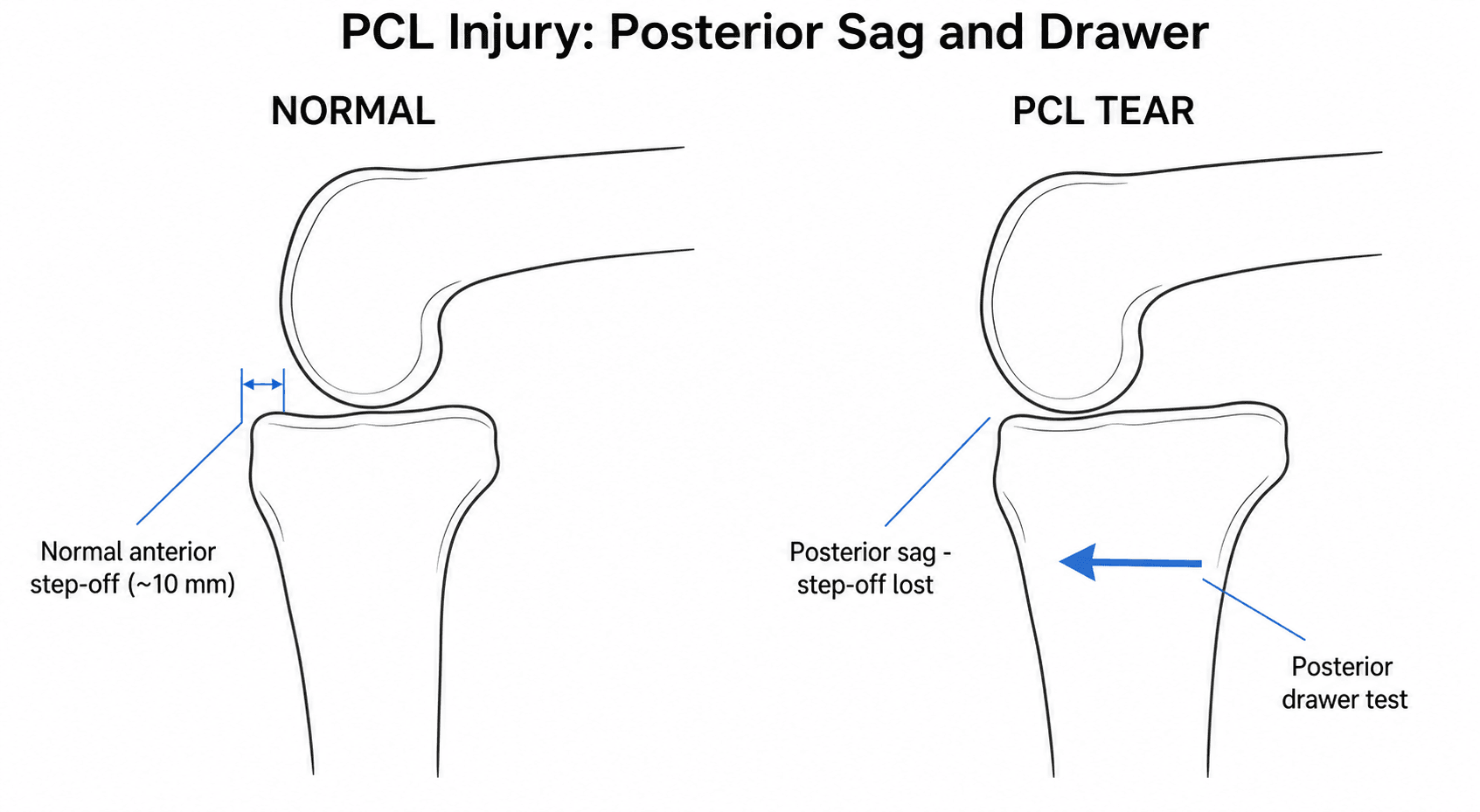
- Posterior drawer test is the key examination
- “PCL has better blood supply than ACL - some healing capacity
- “Posterior sag sign - observe with hip and knee 90 degrees
- “MRI sensitivity 99%+ for PCL injuries
- “Reconstruct early if combined injury to avoid contracture
Isolated Grade I-II often conservative. Combined injuries (especially with PLC) usually need surgery. Always check for associated injuries.
Classic mechanism - proximal tibia hits dashboard with knee flexed. Posterior force on tibia. Always check vascular status.
Key test at 90 degrees flexion. Grade by relationship of tibia to femoral condyles. Start position critical (sag may false positive).
PLC injury most commonly associated with PCL tears. Dial test at 30 degrees and 90 degrees differentiates isolated PLC from combined.
- Translation
- 0-5mm
- Finding
- Tibia anterior to condyles
- Treatment
- Conservative
- Translation
- 5-10mm
- Finding
- Tibia flush with condyles
- Treatment
- Usually conservative
- Translation
- Greater than 10mm
- Finding
- Tibia posterior to condyles
- Treatment
- Consider surgery
- Translation
- Variable
- Finding
- PLC or ACL involvement
- Treatment
- Surgery indicated
DASHPCL Injury Mechanism
Hook:DASH to the dashboard causes PCL injury!
COGSPCL Reconstruction Indications
Hook:Turn the COGS toward surgery when indicated!
Overview and Epidemiology
PCL injuries are often missed on initial presentation. Look for posterior knee pain, instability going downstairs, and subtle posterior sag. MRI confirms diagnosis.
- 3-40% of knee ligament injuries
- MVCs most common cause
- Sports: football, soccer, skiing
- Males greater than females
- Often associated injuries (60%+)
- Dashboard: Proximal tibia hits dashboard
- Fall on flexed knee: Direct blow
- Hyperflexion: Forced flexion
- Hyperextension: May also tear
- Sports contact: Direct blow to tibia
Pathophysiology and Mechanisms
PCL Anatomy
Lateral aspect of medial femoral condyle (in notch).
Posterior intercondylar area of tibia, depression below plateau.
- Anterolateral (AL): larger, tight in flexion
- Posteromedial (PM): smaller, tight in extension
Middle genicular artery. Better than ACL.
32-38mm. Cross-sectional area greater than ACL.
PCL and PLC injuries often occur together. Varus/external rotation force injures both. Always perform dial test at 30 and 90 degrees. Missing PLC leads to poor outcomes.
Classification Systems
PCL Injury Grading
- Translation
- 0-5mm
- Tibial Position
- Anterior to femoral condyles
- Implication
- Partial tear, good prognosis
- Translation
- 5-10mm
- Tibial Position
- Flush with condyles
- Implication
- Complete tear, often conservative
- Translation
- Greater than 10mm
- Tibial Position
- Posterior to condyles
- Implication
- Combined injury likely
Grade III usually indicates associated PLC or capsular injury.
Clinical Assessment
- Mechanism: Dashboard, fall on flexed knee
- Pain: Posterior knee, may be mild
- Instability: Downstairs, deceleration
- Swelling: Often less than ACL
- Other injuries: Common (60%+)
- Posterior sag: Observe at 90/90 position
- Posterior drawer: At 90 degrees flexion
- Quadriceps active: Tibia translates forward
- Dial test: 30 and 90 degrees for PLC
- Varus/valgus: Check collaterals
Patient supine, knee 90 degrees. Ensure tibia not already sagged (start from reduced position). Push tibia posteriorly. Grade by tibial plateau position relative to femoral condyles. Compare to contralateral side.
Key Clinical Pearls
With patient supine, hip and knee 90 degrees, observe profile of tibial tuberosity. Sagged tibia = PCL injury.
From 90/90 position, have patient contract quad. Positive = tibia translates forward (reduces posterior sag).
Differential Diagnosis of the Posteriorly Unstable / Painful Knee
The cardinal trap is mistaking a posterior sag for a positive anterior drawer (the "false anterior drawer"). Start examination from a reduced tibial position and always compare sides.
- Key Examination Finding
- Posterior sag, posterior drawer positive, dial negative
- Distinguishing Feature
- Translation only; no rotatory laxity
- Key Examination Finding
- Posterior drawer positive PLUS dial positive at 30 AND 90 degrees
- Distinguishing Feature
- Increased external rotation persists at 90 degrees
- Key Examination Finding
- Dial positive at 30 degrees only, varus laxity, normal posterior drawer
- Distinguishing Feature
- Rotation normalises at 90 degrees (PCL intact)
- Key Examination Finding
- Lachman/anterior drawer positive
- Distinguishing Feature
- Tibia reduces from a posteriorly sagged start - mimics anterior translation
- Key Examination Finding
- Gross multidirectional laxity, possible dimple sign
- Distinguishing Feature
- Vascular and nerve assessment mandatory; ABPI
- Key Examination Finding
- Joint line tenderness, positive McMurray
- Distinguishing Feature
- Mechanical symptoms, no ligamentous laxity
SPDQPCL Examination
Hook:Do SPDQ tests for PCL!
The Dial Test: Technique and Interpretation
The dial test is the topic's central tool for separating an isolated PLC injury from a combined PCL/PLC injury, but how it is actually performed and why the 30-versus-90-degree distinction works is never set out.
- How / what
- Prone (preferred) or supine; flex the knee to 30 degrees, then 90 degrees, and externally rotate both feet
- Interpretation
- Measure the thigh-foot angle and compare side-to-side
- How / what
- An increase of more than about 10 to 15 degrees of external rotation versus the normal side
- Interpretation
- The side-to-side difference is the key, not the absolute angle
- How / what
- Rotation normalises at 90 degrees
- Interpretation
- ISOLATED posterolateral corner injury (PCL intact)
- How / what
- Rotation persists at 90 degrees
- Interpretation
- COMBINED PCL plus PLC injury
At 30 degrees the posterolateral corner is the dominant restraint to external rotation, so an isolated PLC injury increases external rotation at 30 degrees only. At 90 degrees the PCL becomes the principal restraint to external rotation, so if the increased rotation PERSISTS at 90 degrees the PCL must also be torn. A dial test positive at both angles therefore signals a combined injury and shifts management toward reconstructing both the PCL and the PLC.
Investigations
MRI Assessment

99%+ for PCL injuries.
Very high.
Increased signal, discontinuity, thickening.
PLC, meniscus, cartilage, other ligaments.
Essential for surgical planning and identifying all pathology.


MRI gold standard for PCL diagnosis. Look for bucket-handle appearance (horizontal tear pattern) and assess both bundles. Always evaluate PLC, menisci, and cartilage.
Quantifying Posterior Translation: Stress Radiography
The investigations section names "stress views (kneeling vs standing)", the "Telos device" and "stress radiography" but never gives the technique or the numbers that make it useful. Stress radiography provides an objective, reproducible side-to-side measurement of posterior tibial translation that the manual posterior drawer cannot.
- Interpretation
- Partial PCL injury (grade I-II)
- Implication
- Usually managed nonoperatively
- Interpretation
- Complete isolated PCL tear (grade III)
- Implication
- Individualised - nonoperative trial versus reconstruction
- Interpretation
- Combined PCL plus posterolateral/capsular injury
- Implication
- Favours surgical reconstruction of all injured structures
A Telos device (a standardised posterior force at 90 degrees) or a gravity kneeling view gives a numerical side-to-side translation that is far more reproducible than the manual drawer. It lets you grade the injury objectively, flags a likely COMBINED injury when the difference is large (over about 12 mm), and provides a baseline to monitor graft laxity over time after reconstruction.
Management Algorithm
Treatment Decision
PCL Injury Management
Determine Grade I-III. Identify isolated vs combined. Check PLC with dial test.
Quadriceps strengthening program. Avoid posterior tibial sag. Brace in extension.
In active patient with significant laxity. May trial conservative in low-demand.
Combined with PLC, ACL, or persistent instability. Reconstruct all injured structures.
Surgical Technique
PCL Reconstruction
- Achilles allograft: Most common
- BTB autograft: Stronger fixation
- Hamstring autograft: Less morbidity
- Tibial tunnel: Posterior, safe zone for popliteal vessels
- Femoral tunnel: At native PCL footprint
Double bundle may better restore rotation but technically demanding.
All-inside techniques minimize dissection.
Popliteal artery at risk during tibial tunnel drilling. Stay within safe zone. Use posterior approach or trans-septal technique to visualize. Avoid exiting too posterior.
Complications
- Cause
- Graft stretch, tunnel malposition
- Prevention
- Anatomic placement, adequate graft
- Management
- Revision or accept
- Cause
- Immobilization, adhesions
- Prevention
- Early ROM
- Management
- Manipulation, arthrolysis
- Cause
- Tibial tunnel drilling
- Prevention
- Safe zone, visualization
- Management
- Immediate repair
- Cause
- Altered kinematics
- Prevention
- Restore PCL function
- Management
- Symptomatic treatment
Chronic PCL deficiency leads to patellofemoral and medial compartment OA. Altered kinematics increase joint loading. Early intervention in combined injuries may prevent this.
Postoperative Care
PCL Reconstruction Rehabilitation
Brace locked extension. Non-weight bearing or toe touch. Quad sets only.
Progressive flexion (avoid beyond 90 degrees early). Avoid hamstring loading.
Full ROM. Weight bearing progression. Closed chain exercises.
Sport-specific preparation. Pool running. Light jogging.
Full activity after passing functional tests. May be longer than ACL.
Avoid hamstring activation early (increases posterior tibial translation). Emphasize quads. Limit flexion beyond 90 degrees initially. Progress slower than ACL rehab.
Outcomes and Prognosis
Isolated vs Combined Outcomes
Many do well with rehabilitation. Some develop chronic laxity and OA over time.
Good outcomes in motivated patients. Return to sport possible.
Outcomes depend on addressing all injured structures. Missing PLC leads to failure.
Long-Term Concerns
Common long-term sequela of PCL deficiency.
Also increased with chronic PCL laxity.
Guidelines, Registries & Global Practice
Global Epidemiology
PCL injuries account for roughly 3-40% of acute knee ligament injuries depending on the population studied, with the higher proportions reported in trauma centres and the lower proportions in general sports clinics. Two distinct injury populations dominate worldwide: high-energy road-traffic trauma (the classic dashboard mechanism, and the predominant cause of displaced bony tibial avulsions in regions with high motorcycle/two-wheeler use such as parts of South and East Asia) and sporting contact injuries (football/soccer, rugby, skiing). Up to 60% of PCL injuries occur as part of a combined or multiligament injury pattern.
Side-by-Side Guidance
- Position on Isolated Low-Grade
- Structured nonoperative rehabilitation for grade I-II
- Position on Combined / Bony Avulsion
- Surgery for combined instability and displaced avulsions
- Position on Isolated Low-Grade
- Conservative, quadriceps-focused programme first-line
- Position on Combined / Bony Avulsion
- Refer for reconstruction in combined/multiligament knees
- Position on Isolated Low-Grade
- Emphasises bony avulsion fixation principles
- Position on Combined / Bony Avulsion
- ORIF of displaced tibial avulsion; reconstruct midsubstance tears
- Position on Isolated Low-Grade
- Nonoperative for isolated grade I-II
- Position on Combined / Bony Avulsion
- Anatomic reconstruction; address PLC concurrently
The substantive agreement across societies is greater than the disagreement: isolated grade I-II injuries are rehabilitated, while combined patterns and displaced bony avulsions are operated. Differences are largely emphasis (graft choice, single vs double bundle, timing) rather than principle.
Registry and Outcome Notes
- Unlike arthroplasty, PCL surgery is not captured by dedicated implant registries (NJR/AJRR/AOANJRR track joint replacement, not ligament reconstruction). Outcome evidence therefore comes from prospective cohorts and meta-analyses rather than national registries.
- The Danish and Norwegian knee-ligament reconstruction registries (which began with the ACL) increasingly capture PCL and multiligament procedures, and are emerging as the best population-level data source for revision and re-operation rates.
High- vs Limited-Resource Practice Variation
- Routine MRI and stress radiography for diagnosis and grading
- Allograft availability supports single-stage multiligament reconstruction
- Subspecialist sports/knee surgeons; arthroscopic and all-inside techniques
- Diagnosis may rely on clinical examination and plain films; MRI access limited
- Allograft often unavailable - autograft and open techniques predominate
- Displaced bony avulsions managed by open posterior ORIF (reliable, low-cost, good outcomes)
PCL injuries are important viva topics globally. Know the grading system, dial test interpretation, and when to operate. Be prepared to discuss combined injuries and the rationale for addressing the PLC at the index operation.
Controversies and Areas of Uncertainty
There is no high-level RCT defining the threshold for reconstructing isolated grade III injuries. Practice ranges from nonoperative rehabilitation to early reconstruction in high-demand patients. Decision rests on activity level, symptomatic instability and the long-term arthritis concern.
Double-bundle reconstruction improves objective posterior translation in meta-analysis but has not translated into a reproducible functional advantage, while adding technical complexity and cost. Most surgeons still use single-bundle.
The "killer turn" at the proximal tibial tunnel aperture is implicated in graft attrition. Tibial inlay (open posterior bone-block fixation) avoids this acute angle but is more invasive; comparative clinical superiority remains unproven.
Allograft (commonly Achilles) avoids donor-site morbidity and suits multiligament reconstruction; autograft avoids disease transmission and may have a biological healing advantage. No robust evidence establishes superiority for the PCL specifically.
MCQ Practice Points
Q: What is the primary function of the PCL? A: Restraint to posterior tibial translation - provides 95% of restraint near full flexion.
Q: What is the classic mechanism for PCL injury? A: Dashboard injury - proximal tibia strikes dashboard with knee flexed, driving tibia posteriorly.
Q: What defines a Grade II PCL injury? A: Tibia flush with femoral condyles on posterior drawer. 5-10mm translation. Complete tear but may do well conservative.
Q: Dial test positive at 30 degrees only vs 30 and 90 degrees? A: 30 degrees only = isolated PLC. 30 and 90 degrees = combined PCL + PLC. At 90 degrees, intact PCL prevents rotation.
Q: What are long-term consequences of PCL deficiency? A: Patellofemoral and medial compartment OA. Altered kinematics increase loading on these compartments.
Q: Why do combined PCL/PLC injuries need surgery? A: PLC must be addressed to prevent PCL graft failure. Isolated PCL reconstruction with untreated PLC has high failure rate.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man presents after an MVC. His knee hit the dashboard. He has posterior knee pain and mild swelling. Posterior drawer shows the tibia flush with the femoral condyles. Dial test is negative. MRI confirms isolated PCL tear. How would you manage this?”
“A 28-year-old football player has a knee injury during a game. He has posterior and lateral knee pain. Posterior drawer shows Grade III laxity. Dial test shows 15 degrees increased external rotation at both 30 and 90 degrees compared to the opposite side. What is your management?”
“A 40-year-old presents with anterior knee pain and medial knee pain for 2 years. He had a PCL injury 10 years ago treated conservatively. He now has difficulty with stairs. X-rays show Grade 2 patellofemoral and medial OA. Posterior drawer is Grade II. What would you recommend?”
Grading (Posterior Drawer)
- Grade I: Tibia anterior to condyles (0-5mm)
- Grade II: Tibia flush with condyles (5-10mm)
- Grade III: Tibia posterior to condyles (greater than 10mm)
- Grade III often indicates combined injury
Clinical Tests (SPDQ)
- Sag sign: Observe at 90/90
- Posterior drawer: Key test at 90 degrees
- Dial test: 30 and 90 degrees for PLC
- Quadriceps active: Forward translation
Dial Test
- Positive at 30 only = isolated PLC
- Positive at 30 AND 90 = combined PCL + PLC
- At 90 degrees, intact PCL prevents rotation
- Critical for operative planning
Treatment Guidelines
- Isolated Grade I-II: Conservative with quad rehab
- Isolated Grade III: Consider surgery if active
- Combined injuries: Surgery for both
- Address PLC or PCL graft will fail
Surgical Pearls
- Fix tibial avulsions if present
- Tibial tunnel: beware popliteal artery
- Reconstruct PLC if combined
- Early surgery prevents PLC contracture
Evidence Base and Key Studies
Natural History of Acute Isolated Nonoperatively Treated PCL Injury
- Prospective study of 133 acute isolated PCL injuries, mean age 25 years
- Mean follow-up 5.4 years; objective laxity unchanged from injury to review
- Knee function was INDEPENDENT of the grade of laxity
- Roughly half returned to the same sport at the same or higher level
Minimum 10-Year Follow-Up of Nonoperatively Treated Isolated PCL Injury
- 68 patients with acute isolated PCL injury followed prospectively (mean 14-17 years)
- Mean quadriceps strength 97% of the uninvolved leg with full range of motion maintained
- Prevalence of moderate-to-severe radiographic osteoarthritis was 11%
- Osteoarthritis grade did NOT differ by PCL laxity grade
Outcomes of Acute Grade-III Posterolateral (PLC) Knee Injuries
- Prospective series of 30 knees with grade-III posterolateral injury treated within 6 weeks
- 4 had an associated PCL tear and 8 had both cruciate ligaments torn
- Varus side-to-side gap improved from 6.2 mm to 0.1 mm at final follow-up
- Mean IKDC subjective score improved from 29 to 82 points
Single-Bundle vs Double-Bundle PCL Reconstruction (Meta-Analysis)
- Systematic review and meta-analysis of 11 studies, 441 patients (232 SB, 209 DB)
- No significant difference in Lysholm or Tegner scores between SB and DB
- DB gave significantly better objective posterior translation (Telos) at 90 degrees
- Both techniques produced improved patient-reported outcomes
Open vs Arthroscopic Fixation of Displaced PCL Avulsion Fractures
- Systematic review of 12 studies: 134 open posterior approach, 174 arthroscopic suture fixation
- Lysholm scores 85-100 (open) and 80-100 (arthroscopic)
- 90-100% rated normal/nearly normal on subjective IKDC in both groups
- Side-to-side laxity difference 0-5 mm for both approaches
All-Inside PCL Reconstruction - Current Practice
- PRISMA systematic review of 14 studies on all-inside PCL reconstruction technique
- Allograft was the preferred graft in 9 of 14 studies; semitendinosus when autograft used
- Quadruple-folded graft, 8-12 mm diameter, was the commonest configuration
- Most docked the graft into the tibial socket first then the femoral socket
AAOS / AO Foundation / ESSKA Practice Principles for PCL Injury
- Isolated grade I-II injuries: structured nonoperative rehabilitation with quadriceps emphasis
- Combined PCL injuries (especially PCL + PLC) and displaced bony avulsions: surgical management
- Dial test at 30 and 90 degrees is the key examination to separate isolated PLC from combined injury
- Address all injured structures at index surgery to protect the PCL graft