Proximal Tibiofibular Joint | Peroneal Nerve Risk | Often Missed
- Anterolateral (Type I) is MOST COMMON - fibula displaced forward and lateral
- Common peroneal nerve wraps around fibular neck - AT RISK in all types
- Closed reduction: knee flexed 90 degrees, direct pressure on fibular head
- Recurrent instability: may need PTFJ fusion or ligament reconstruction
- “Often missed - requires specific examination for lateral knee pain
- “Check peroneal nerve function BEFORE any reduction attempt
- “If irreducible: may have soft tissue interposition
- “Chronic instability more problematic than acute injury
Proximal Tibiofibular Joint Dislocations
Common peroneal nerve wraps around fibular neck. Traction during dislocation can injure nerve. Reduction maneuver can also cause injury. Type II (posteromedial) = highest risk. DOCUMENT nerve function before ANY manipulation.
Foot dorsiflexion (peroneus longus/brevis). Toe extension (EHL, EDL). First web space sensation. Lateral leg sensation. Compare to contralateral side.
Overview
Overview
Proximal tibiofibular joint (PTFJ) dislocations are uncommon injuries that are frequently missed at initial presentation. The joint, located just below the lateral knee, is stabilized by the anterior and posterior tibiofibular ligaments. Dislocation occurs when these ligaments are disrupted, most commonly resulting in anterolateral displacement of the fibular head.
The critical structure at risk is the common peroneal nerve, which wraps around the fibular neck just distal to the joint. Nerve function must be assessed before and after any reduction attempt.
Most acute dislocations reduce with closed manipulation. However, some patients develop recurrent instability that may require surgical stabilization. The Ogden classification categorizes these injuries by direction of displacement and mechanism.
Anatomy
Anatomy
Joint Anatomy
Articulation:
- Plane synovial joint
- Fibular head articulates with posterolateral tibia
- Inclined articular surface (variable angle)
- Oblique orientation allows rotation
Ligamentous Stabilizers:
- Location
- Anterior joint
- Function
- Primary restraint to anterior translation
- Location
- Posterior joint
- Function
- Primary restraint to posterior translation
- Location
- Circumferential
- Function
- Secondary stabilizer
- Location
- Lateral
- Function
- Attaches to fibular head
- Location
- Posterolateral
- Function
- Attaches to fibular head
Common Peroneal Nerve
- Branches from sciatic in popliteal fossa
- Winds around fibular neck
- Only 1-2cm from joint
- Divides into superficial and deep branches
- Superficial location
- Tethered around bone
- Little surrounding soft tissue
- Traction during dislocation
Joint Variants
- More horizontal articular surface
- More stable inherently
- More common (70%)
- More oblique surface
- Less stable
- Predisposes to instability
Biomechanical Role of the PTFJ
Biomechanical Role: Why Fusion Is Tolerated but Can Cause Ankle Symptoms
The anatomy section notes the joint permits rotation, and the operative Milankov case (see Evidence) describes the joint's function, but the body of the topic never develops the load-bearing role that underpins the treatment logic. Classically (Ogden), the proximal tibiofibular joint has three biomechanical functions:
- Dissipation of torsional stress from the ankle - rotational forces generated at the ankle are transmitted up the fibula and absorbed at the PTFJ rather than concentrated at a single point.
- Dissipation of lateral tibial bending moments - the fibula and PTFJ share the lateral bending load of the leg.
- Transmission of a share of the axial (weight-bearing) load - the fibula bears part of the vertical load, greatest in ankle dorsiflexion when the mortise widens and the fibula is loaded.
Normal PTFJ excursion is small - only a few millimetres of glide with slight rotation. This is precisely why arthrodesis is generally well tolerated and is the reliable option for chronic instability: eliminating a low-motion joint causes little functional deficit. The trade-off is that fusion removes the joint's torsional accommodation, so more rotational and axial stress is transmitted to the ankle and along the fibula - the mechanistic explanation for the fibular or ankle pain occasionally reported after arthrodesis, and the rationale for offering motion-preserving reconstruction to selected patients. The articular orientation modulates this: a horizontal surface is inherently more stable, whereas an oblique surface transmits more rotational load and predisposes to instability.
Q: Why is proximal tibiofibular arthrodesis usually well tolerated, and what is its theoretical downside? A: Normal PTFJ motion is only a few millimetres of glide with slight rotation, so fusion causes minimal functional loss - the basis for it being the reliable choice in chronic instability. The downside is mechanistic: the joint normally dissipates torsional and lateral-bending forces transmitted up the fibula from the ankle, so fusion can concentrate rotational stress at the ankle and produce fibular or ankle symptoms, which is the rationale for motion-preserving reconstruction in selected patients.
Classification Systems
Classification
Ogden Classification
Most Common Type (70%)
- Fall with knee flexed and foot inverted
- Direct blow to posteromedial fibular head
- Twisting injury during sports
- Parachuting injury classic
- Fibular head prominent anterolaterally
- May be visible or palpable bump
- Usually reducible with closed technique
- Lower peroneal nerve risk
- Closed reduction (knee flexed 90 degrees)
- Direct posterior pressure on fibular head
- External rotation of foot aids reduction
- Immobilize 2-3 weeks
This is the most commonly encountered type in clinical practice.
Clinical Presentation
Clinical Presentation
History
- Twisting knee injury
- Direct blow to fibular head
- Fall onto flexed knee
- Sports (parachuting, football)
- Lateral knee pain
- Feeling of instability
- "Something out of place"
- Pain with weight-bearing
Physical Examination
- Prominent fibular head (anterolateral)
- Asymmetry compared to other side
- Swelling lateral knee
- May see obvious deformity
- Tender over fibular head
- Mobile fibular head
- Compare to contralateral
- Technique
- Grasp and translate
- Finding
- Increased anteroposterior motion
- Technique
- Push fibular head
- Finding
- Excessive movement
- Technique
- Cross legs while sitting
- Finding
- Reproduces symptoms
Neurovascular Examination (CRITICAL):
- Foot dorsiflexion (deep peroneal)
- Toe extension (deep peroneal)
- Foot eversion (superficial peroneal)
- First web space sensation
- Lateral leg sensation
Provocative Tests for PTFJ Instability
Provocative Tests: the Cross-Leg Sign and Fibular-Head Translation
The special-tests table and the CHECK mnemonic both invoke a "cross-leg test" and a "fibular head mobility" test, but the topic never describes how they are performed or interpreted. Because there is no validated radiographic threshold for subluxation (see Controversies), the diagnosis of subtle or chronic instability rests on these reproducible bedside signs compared with the uninjured side.
- Knee flexed to about 90 degrees to relax the LCL and biceps femoris.
- Grasp the fibular head between thumb and index finger and translate it anteriorly and posteriorly.
- Excessive anteroposterior glide - especially when it reproduces the patient's lateral knee pain or apprehension - indicates instability. Always grade against the contralateral fibular head, as normal laxity varies between individuals.
- With the patient seated and the affected leg crossed over the opposite knee (figure-of-four position), the fibular head is thrown into prominence and the maneuver reproduces lateral knee pain or a sense of the fibular head subluxing.
- Symptoms typically resolve when the leg is uncrossed. It is a useful bedside test for chronic anterolateral instability, where standard radiographs are frequently normal.
- Active ankle dorsiflexion and eversion tensions the biceps femoris and peroneal musculature and can provoke anterolateral subluxation of the fibular head in an unstable joint.
Reproducible fibular-head hypermobility plus a positive cross-leg sign, correlated with comparison radiographs, is more informative than any single static image in this diagnosis.
Q: What is the cross-leg sign in proximal tibiofibular joint instability? A: With the patient seated and the affected leg crossed over the contralateral knee (figure-of-four), the fibular head is thrown into prominence and lateral knee pain or a sense of subluxation is reproduced, resolving when the leg is uncrossed. It is a bedside test for chronic anterolateral PTFJ instability, valuable because standard radiographs are often normal and there is no validated radiographic threshold for subluxation.
Investigations
Investigations
Plain Radiographs
- AP knee
- Lateral knee
- Compare to contralateral
- Fibular head position abnormal
- Overlap with tibia on AP view
- Position on lateral view
- Associated fractures
- Subtle findings
- May appear normal
- Comparison views helpful
CT Scan
Indications:
- Uncertain diagnosis
- Associated fractures
- Surgical planning
- Chronic instability assessment
MRI
Indications:
- Ligament assessment
- Chronic instability
- Associated soft tissue injury
- Not routine acute
Differential Diagnosis
Lateral knee pain with a prominent or mobile fibular head has several mimics. The key discriminators are the position of the fibular head on comparison radiographs and reproducible fibular head hypermobility.
- Key Distinguishing Features
- Displaced or hypermobile fibular head; lateral knee pain; cross-leg test positive
- Confirmatory Test
- Comparison AP/lateral radiographs; CT if uncertain
- Key Distinguishing Features
- Varus laxity; pain over LCL, not the joint line of PTFJ; fibular head reduced
- Confirmatory Test
- Varus stress test; MRI
- Key Distinguishing Features
- Combined varus and external-rotation laxity; dial test positive at 30 degrees
- Confirmatory Test
- Dial test; MRI of PLC structures
- Key Distinguishing Features
- Foot drop/sensory loss without joint displacement; Tinel at fibular neck
- Confirmatory Test
- Nerve conduction studies; normal PTFJ radiographs
- Key Distinguishing Features
- Cortical break on radiograph; consider Maisonneuve if ankle tender
- Confirmatory Test
- Radiograph; full-length tibia-fibula views
- Key Distinguishing Features
- Joint-line tenderness; mechanical symptoms; fibular head normal
- Confirmatory Test
- MRI; McMurray test
- Key Distinguishing Features
- Posterolateral pain with resisted knee flexion; fibular head reduced
- Confirmatory Test
- MRI; clinical exam
Management Algorithm
Management Algorithm
Type I and II - Closed Reduction First
- Document peroneal nerve function (MANDATORY)
- Obtain AP and lateral knee radiographs
- Compare to contralateral side
- Rule out associated injuries
- Adequate analgesia/sedation in ED
- Flex knee to 90 degrees (relaxes LCL and biceps)
- Externally rotate foot
- Apply direct pressure on fibular head
- Type I: push posteriorly
- Type II: push anteriorly
- Feel/hear "clunk" with successful reduction
- Confirm reduction with radiographs
- Reassess peroneal nerve function
85%+ for acute dislocations.
Closed reduction is the first-line treatment for most acute PTFJ dislocations.
Surgical Technique
Surgical Technique
Acute Irreducible Dislocation
- Supine on operating table
- Bump under ipsilateral hip
- Knee flexed over bolster
- Longitudinal lateral incision
- Centered over fibular head
- 6-8 cm length
- Incise skin and subcutaneous tissue
- Identify and protect common peroneal nerve (CRITICAL)
- Incise fascia anterior to nerve
- Reflect biceps femoris posteriorly
- Expose PTFJ capsule
- Incise capsule longitudinally
- Remove any interposed soft tissue (biceps, capsule)
- Reduce fibular head under direct vision
- Repair anterior and posterior tibiofibular ligaments
- Consider temporary 3.5mm screw if unstable
- Repair capsule with absorbable sutures
- Repair fascia
- Skin closure
- Apply long leg splint in slight flexion
Immobilize 3-4 weeks, remove screw at 6-8 weeks if used.
Complications
Complications
Peroneal Nerve Injury
5-10% of all PTFJ dislocations
- Neurapraxia (most common, 80%)
- Axonotmesis (15%)
- Neurotmesis (rare, less than 5%)
- Observation for neurapraxia initially
- EMG/NCS at 3-4 weeks if no clinical recovery
- Exploration if no improvement by 3 months
- Ankle-foot orthosis for foot drop during recovery
- Nerve repair or grafting if needed at exploration
- Most neurapraxia recover within 6-12 weeks
- Axonotmesis may take 3-6 months
- Complete recovery in 85% of nerve injuries
- Some permanent deficit possible in severe cases
Recurrent Instability
5-10% after initial reduction
- Oblique joint variant
- Inadequate immobilization (less than 2 weeks)
- Generalized ligamentous laxity
- Return to activity too early
- Inadequate rehabilitation
- Rehabilitation initially (3-6 months trial)
- Bracing during sport
- Surgery if persistent symptomatic instability
Chronic Pain
10-15% have ongoing pain
- Articular cartilage damage at injury
- Residual microinstability
- Peroneal nerve irritation
- Post-traumatic arthritis
- Activity modification
- Physical therapy and strengthening
- Corticosteroid injection if localized synovitis
- Fusion for severe refractory cases
Failed Reduction
10-15% cannot reduce closed
- Soft tissue interposition (biceps, capsule)
- Delayed presentation (more than 2 weeks)
- Associated fracture
- Fibular head button-holed through fascia
- Open reduction required
- Remove interposed tissue
- Repair ligaments
- Consider temporary screw fixation
Other Complications
- Vascular injury (rare)
- Compartment syndrome (rare)
- Wound complications after surgery
- Post-traumatic arthritis (uncommon)
- Hardware complications if screw used
- Non-union after fusion (less than 5%)
Postoperative Care
Postoperative Care
After Open Reduction
- Long leg splint with knee 15-20 degrees flexion
- Non-weight bearing
- Ice and elevation
- Pain management
- Monitor peroneal nerve function daily
- Convert to hinged knee brace
- Start gentle ROM exercises
- Maintain NWB or touch weight bearing
- Physiotherapy begins
- Progress to partial weight bearing
- Increase ROM exercises
- Strengthening begins
- Remove temporary screw if placed
- Progress to full weight bearing
- Continue strengthening
- Return to normal activities
- Sport-specific rehabilitation
After PTFJ Fusion
- Long leg cast with knee in slight flexion
- Non-weight bearing
- Wound care
- Monitor for complications
- Remove cast
- Hinged brace
- Start ROM exercises (fusion site stable)
- Progressive weight bearing
- Continue strengthening
- Gradual return to activities
- Monitor fusion on radiographs
- Return to sport if fusion solid
- Resume full activities
- Minimal functional deficit expected
After Ligament Reconstruction
- Long leg cast or locked brace
- Non-weight bearing
- Protect reconstruction
- Unlock brace
- Start gentle ROM
- Progress to partial weight bearing
- Avoid stress on reconstruction
- Full ROM goal
- Strengthening program
- Progress to full weight bearing
- Return to sport
- Functional testing before clearance
Red Flags Postoperatively
- New foot drop (peroneal nerve injury)
- Loss of reduction on radiograph
- Wound infection
- Compartment syndrome symptoms
- Recurrent instability
- Persistent pain
- Hardware failure
- Non-union (fusion cases)
Outcomes/Prognosis
Outcomes and Prognosis
After Closed Reduction
- 85-90% good to excellent outcomes
- Reduction success rate 85%+
- Most maintain reduction with 2-3 weeks immobilization
- Return to normal activities 6-8 weeks
- Return to sport 8-12 weeks
- 5-10% develop recurrent instability
- Higher in oblique joint variant
- Higher with inadequate immobilization
- Most occur within first 6 months
- Minimal long-term functional deficit
- Most return to pre-injury activity level
- Rare post-traumatic arthritis
- Occasional mild discomfort with extreme flexion
After Open Reduction
- 85-90% maintain reduction
- Slightly higher recurrence than closed reduction (10-15%)
- Good functional outcomes in most cases
- Longer immobilization (3-4 weeks)
- Return to sport 3-4 months
- May have mild stiffness initially
After PTFJ Fusion
- 90-95% achieve solid fusion
- Fusion rate greater than 95% at 3 months
- Excellent stability, no recurrence
- 90%+ good to excellent patient satisfaction
- Minimal functional deficit from fusion
- No significant gait abnormality
- Can return to high-level sport
- Return to activities 3-4 months
- Return to sport 4-6 months
- Permanent stability achieved
- Non-union less than 5%
- Minimal restriction from fusion
After Ligament Reconstruction
- 80-85% good stability (higher recurrence than fusion)
- Motion preserved
- 10-15% recurrent instability
- Good outcomes in 80-85%
- Preserves joint motion
- May feel more "normal" than fusion
- Longer rehabilitation (4-6 months)
- Return to sport 6-9 months
- Requires compliance with rehab
Peroneal Nerve Recovery
- 85-90% of nerve injuries recover completely
- Neurapraxia: 6-12 weeks recovery
- Axonotmesis: 3-6 months recovery
- 10% have mild residual weakness
- Usually does not limit function significantly
- May need ankle-foot orthosis initially
- Less than 5% have permanent significant deficit
- May need tendon transfers or ankle fusion
Prognostic Factors
- Acute injury (less than 2 weeks)
- Type I (anterolateral) dislocation
- Successful closed reduction
- Adequate immobilization
- No peroneal nerve injury
- Horizontal joint variant
- Delayed presentation (greater than 4 weeks)
- Type II (posteromedial) with nerve injury
- Irreducible dislocation
- Oblique joint variant
- Generalized ligamentous laxity
- Multiple recurrences
Long-Term Follow-Up Studies
- 85% excellent outcomes after appropriate treatment
- 10% mild symptoms not limiting activities
- 5% significant ongoing problems
- 90% return to pre-injury sport level
- May take 6-12 months for high-level athletes
- Contact sports may require longer recovery
- Greater than 90% satisfied with outcome
- Fusion patients report excellent stability
- Reconstruction patients value preserved motion
Guidelines, Registries & Global Practice
Guidelines, Registries & Global Practice
Global Epidemiology
PTFJ dislocation is a rare injury - Ogden's original 1974 literature review identified only 108 reported cases, and few large series exist anywhere in the world. It is consistently under-recognised: lateral knee pain is frequently attributed to soft-tissue injury and the diagnosis missed at first presentation. Reported demographics across case series are similar internationally: young, active adults, with sport (skiing/snowboarding, parachuting, football codes, soccer) and high-energy trauma (with the superior/Maisonneuve pattern) the dominant mechanisms.
Guidelines - No Dedicated Society Guideline
Because the injury is rare, no orthopaedic society (AAOS, BOA/NICE, AO Foundation, EFORT) publishes a dedicated PTFJ-dislocation guideline. Practice is therefore derived from general acute joint-injury and trauma principles, which are consistent worldwide:
- Position on PTFJ Dislocation
- Document neurovascular status, closed reduction first, confirm with imaging, temporary trans-fixation/ORIF for irreducible or unstable joints
- Position on PTFJ Dislocation
- Early neurovascular assessment and documentation; timely reduction; orthoplastic input only if open/associated injury
- Position on PTFJ Dislocation
- No specific recommendation; supports reduction and immobilisation, surgery for recurrent instability
- Position on PTFJ Dislocation
- No dedicated statement; same principle-based approach
There is no implant registry data for this joint (no arthroplasty/standard implant is used), so registry evidence does not apply.
Areas of Consensus (Global)
- Peroneal nerve documentation before and after any manipulation is universal.
- Closed reduction is first-line for acute Types I and II.
- Temporary screw transfixation (removed at 6-8 weeks) is the most widely reported stabilisation for irreducible acute injury.
- Arthrodesis vs ligament reconstruction for chronic instability remains surgeon-dependent (see Controversies).
High- vs Limited-Resource Practice Variation
- Well-resourced settings: CT/MRI available for diagnostic uncertainty and chronic instability work-up; arthroscopic-assisted or anatomic reconstruction techniques offered to preserve motion.
- Limited-resource settings: Diagnosis rests on comparison radiographs of both knees; closed reduction under sedation and, if needed, open reduction with screw transfixation are reliable, low-cost solutions with good reported outcomes (e.g. Fang et al. series).
Sport-Specific Considerations
- Skiing/snowboarding: classic mechanism - knee flexed, foot inverted, twisting fall.
- Parachuting/landing injuries: the textbook mechanism for Type I.
- Football codes / soccer: twisting tackles with a planted foot.
- Return to contact sport is typically 8-12 weeks after successful closed reduction, often with a hinged knee brace initially.
Controversies & Areas of Uncertainty
Controversies & Areas of Uncertainty
The rarity of PTFJ dislocation means the evidence base is limited to case reports and small series (Level IV), with no randomised or comparative trials. Several practical questions remain unresolved.
Fusion is reliable but sacrifices the small rotational accommodation of the joint; some authors report fibular pain or ankle symptoms after arthrodesis. Anatomic/biceps reconstruction preserves motion but has higher reported recurrence. No comparative trial exists - choice is surgeon- and patient-dependent.
Whether a trans-fixation screw is needed after open reduction (vs ligament repair alone), and the optimal timing of removal (commonly 6-8 weeks), is based on case-series opinion, not trial data. Retained or broken hardware is a recognised concern.
Reported immobilisation after closed reduction ranges from a few days to 3 weeks. The trade-off between recurrence (too little) and stiffness (too much) is not defined by evidence.
Many atraumatic/habitual subluxations are asymptomatic and best left alone. Surgery in hypermobile or Ehlers-Danlos patients carries a high recurrence risk and is controversial - reserved for genuinely disabling, refractory cases.
Diagnostic uncertainty: there is no validated radiographic measurement defining PTFJ subluxation, so subtle or chronic cases rely on comparison views and clinical hypermobility rather than an objective threshold.
Viva Scenarios
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old parachutist lands awkwardly and presents with lateral knee pain. Examination shows a prominent fibular head anterolaterally. What is your diagnosis and management?”
“Describe the Ogden classification of proximal tibiofibular joint dislocations and the significance of the common peroneal nerve.”
“A patient has recurrent PTFJ instability despite conservative treatment. The joint subluxes with activity. What are your surgical options?”
MCQ Practice Points
Q: What is the most common type of proximal tibiofibular joint dislocation? A: Type I (anterolateral) accounts for 70% of PTFJ dislocations. The fibular head displaces anteriorly and laterally, typically from a twisting injury with the knee flexed.
Q: Which type of PTFJ dislocation has the highest risk of peroneal nerve injury? A: Type II (posteromedial) has the highest peroneal nerve risk because the fibula displaces posteromedially, directly compressing the common peroneal nerve against the fibular neck where it wraps around.
Q: What ankle injury is associated with Type III (superior) PTFJ dislocation? A: The Maisonneuve fracture. In this injury, the fibula migrates superiorly due to complete disruption of the syndesmosis and interosseous membrane. Always obtain full-length tibia-fibula views in ankle injuries.
Q: What must be documented BEFORE reducing a PTFJ dislocation? A: Common peroneal nerve function. Test foot dorsiflexion (tibialis anterior), great toe extension (EHL), and first web space sensation. The nerve is only 1-2cm from the PTFJ and at risk in ALL dislocation types.
Q: What is the reduction technique for a Type I (anterolateral) PTFJ dislocation? A: Flex the knee to 90 degrees (relaxes LCL and biceps femoris), externally rotate the foot, then apply direct pressure pushing the fibular head POSTERIORLY. For Type II, push the fibular head anteriorly.
Q: What is the definitive treatment for recurrent PTFJ instability? A: PTFJ arthrodesis (fusion) has over 90% success rate. While it sacrifices some tibial rotation, most patients have minimal functional limitation. Ligament reconstruction preserves motion but has higher recurrence rates.
- PTFJ fusion: simple, reliable, 90%+ success, minimal functional deficit
- Ligament reconstruction: motion-preserving, more technically demanding
- Temporary screw: allows ligament healing, remove at 6-8 weeks
- Acute closed reduction: 85-90% excellent outcomes
- PTFJ fusion: greater than 90% patient satisfaction
- Ligament reconstruction: 80-85% good stability
- Peroneal nerve recovery: 85-90% complete recovery
Common Exam Scenarios
"28-year-old parachutist with lateral knee pain after landing"
- Answer: Type I anterolateral PTFJ dislocation
"Patient with PTFJ dislocation, irreducible after two attempts"
- Answer: Open reduction required, likely soft tissue interposition
"Recurrent PTFJ instability despite 6 months conservative treatment"
- Answer: Surgical options are fusion (preferred) or reconstruction
"Ankle fracture with tender proximal fibula"
- Answer: Type III superior PTFJ dislocation (Maisonneuve pattern)
"New foot drop after PTFJ reduction"
- Answer: Peroneal nerve injury from reduction maneuver
Key Numbers to Remember
- 70% - Type I (anterolateral) proportion
- 85% - Closed reduction success rate
- 90 degrees - Knee flexion for reduction
- 2-3 weeks - Immobilization duration
- 5-10% - Peroneal nerve injury rate
- 5-10% - Recurrent instability rate
- 90%+ - PTFJ fusion success rate
- 85-90% - Nerve recovery rate
- 6-8 weeks - Screw removal timing
Examiner Favorites
"Why does knee flexion help with reduction?"
- Relaxes LCL and biceps femoris attachments to fibular head
"What structure is interposed in irreducible dislocations?"
- Biceps femoris tendon or joint capsule most common
"Why is PTFJ fusion well-tolerated?"
- Joint has minimal motion normally (less than 5 degrees)
- No significant functional deficit from fusion
"What predisposes to recurrent instability?"
- Oblique joint variant (more vertical articular surface)
- Inadequate immobilization duration
- Generalized ligamentous laxity
At a Glance
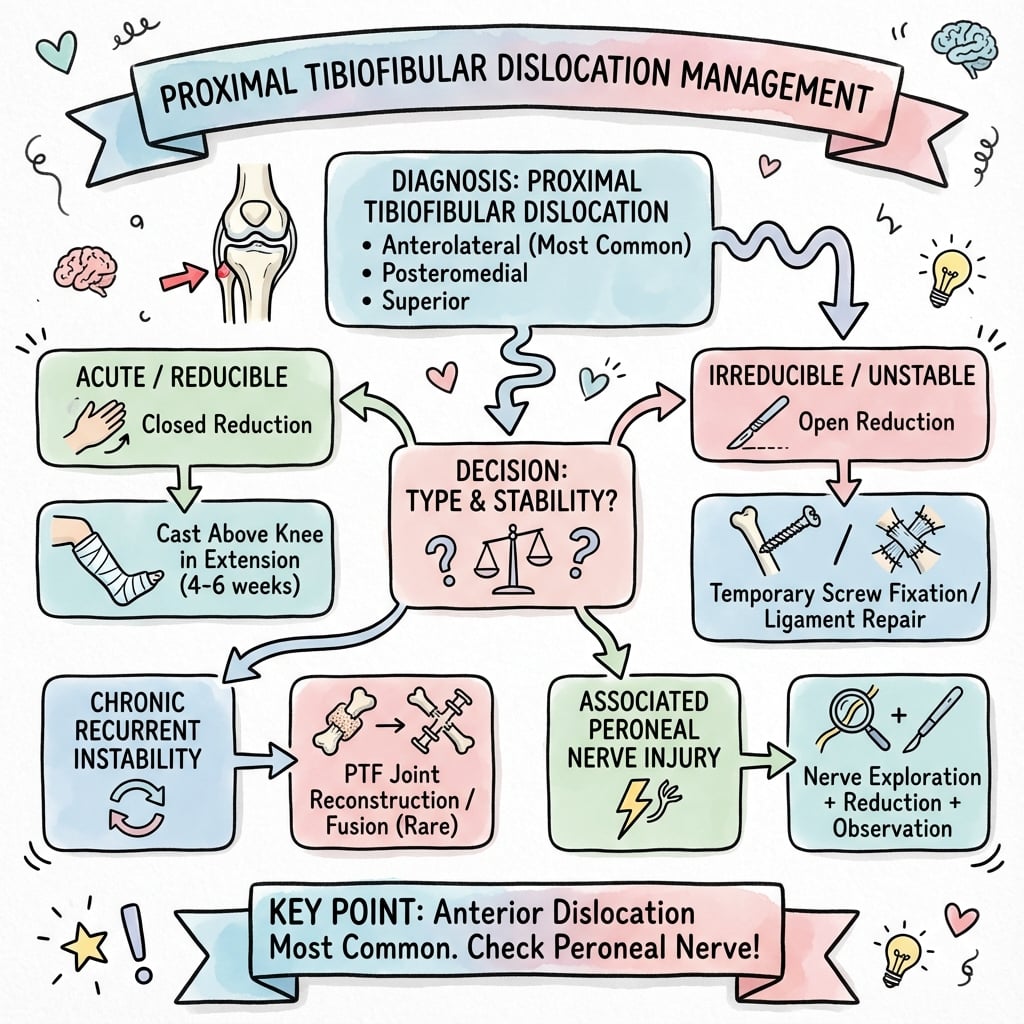
Proximal tibiofibular joint (PTFJ) dislocations are rare injuries that are often missed, requiring a high index of suspicion for lateral knee pain. Classified by Ogden: Type I (anterolateral) is most common; Type II (posteromedial) has highest peroneal nerve risk; Type III involves proximal fibular migration with ankle injury; Type IV is atraumatic from hypermobility. The common peroneal nerve wraps around the fibular neck and is at risk in all types - document nerve function BEFORE any reduction attempt. Most reduce closed with knee flexed 90° and direct pressure on the fibular head. Recurrent instability may require PTFJ fusion or ligament reconstruction.
- Direction
- Fibula forward/lateral
- Management
- Closed reduction with direct pressure
- Direction
- Fibula backward/medial
- Management
- Closed reduction, higher nerve risk
- Direction
- Fibula proximal migration
- Management
- Address ankle injury, fibula follows
- Direction
- Subluxation from hypermobility
- Management
- Rehabilitation, activity modification
- Direction
- Any type
- Management
- Open reduction, remove interposed tissue
- Direction
- Any type
- Management
- Urgent reduction, observe nerve recovery
- Direction
- Usually Type I
- Management
- Ligament reconstruction or PTFJ fusion
- Direction
- Type III pattern
- Management
- Fix ankle, PTFJ usually reduces
PTFJPTFJ for Joint
Hook:PTFJ - the often forgotten joint by the Peroneal nerve!
OGDENOGDEN for Classification
Hook:OGDEN Types 1-4: Anterior, Posterior, Superior, Atraumatic!
FLEXFLEX for Reduction
Hook:FLEX the knee and push that fibula back!
CHECKCHECK for Assessment
Hook:CHECK the peroneal nerve before and after!
Exam Cheat Sheet
Exam Day Cheat Sheet
Classification (Ogden)
- Type I: Anterolateral (MOST COMMON)
- Type II: Posteromedial (highest nerve risk)
- Type III: Superior (with ankle injury)
- Type IV: Atraumatic (hypermobility)
Peroneal Nerve
- Wraps around fibular neck
- At risk in ALL types
- Document function BEFORE reduction
- Test: dorsiflexion, toe extension, sensation
Reduction Technique
- Flex knee to 90 degrees
- Externally rotate foot
- Direct pressure on fibular head
- Type I: push posterior, Type II: push anterior
Post-Reduction
- Confirm reduction on XR
- Long leg cast 2-3 weeks
- Protected weight-bearing
- Monitor for recurrence
Surgical Indications
- Irreducible dislocation
- Recurrent instability
- Associated nerve injury requiring exploration
- Type III with ankle fixation
Surgical Options
- Open reduction (acute irreducible)
- PTFJ fusion (chronic instability)
- Ligament reconstruction (motion-preserving)
- Temporary screw fixation
Quick Reference: Key Points
- Details
- Type I (Anterolateral)
- Details
- Common peroneal
- Details
- Knee flexed 90 degrees
- Details
- 2-3 weeks
- Details
- 5-10%
- Details
- 85%+
- Details
- Over 90%
Ogden Classification Summary
- Direction
- Anterolateral
- Mechanism
- Fall with flexed knee
- Nerve Risk
- Lower
- Direction
- Posteromedial
- Mechanism
- Direct blow anterior
- Nerve Risk
- Higher
- Direction
- Superior
- Mechanism
- Ankle injury
- Nerve Risk
- Moderate
- Direction
- Atraumatic
- Mechanism
- Hypermobility
- Nerve Risk
- Low
Evidence
Evidence Base
Ogden Classification (Original Description)
- Cadaveric and clinical study describing PTFJ anatomy, biomechanics and a four-type classification (anterolateral, posteromedial, superior, atraumatic) from a literature review of 108 cases
Ogden - Subluxation and Surgical Management
- Companion paper detailing chronic subluxation, association with hypermobility/Ehlers-Danlos, and surgical options including arthrodesis and screw fixation for symptomatic recurrent instability
Early Diagnosis is Critical
- Bilateral fibular head dislocation case with 9- and 5-year follow-up; prompt recognition and early reduction were associated with good recovery, whereas delay complicates management
Surgical Outcomes in Traumatic Dislocation
- Series of 12 acute traumatic superior tibiofibular dislocations (8 anterolateral, 2 posteromedial, 2 superior); 11 surgically treated, mean Lysholm 95, with 11 excellent and 1 good result and full nerve recovery
Closed and Open Reduction in Recurrent Dislocation
- Case report and literature review confirming anterolateral is the most common Ogden type; immediate closed reduction is often successful, with open reduction or temporary fixation reserved for irreducible or chronically unstable joints
Single-Case Operative Technique
- Soccer injury with failed closed reduction managed by open reduction and temporary screw transfixation; screw removed at 6 weeks, return to sport at 4 months with full ROM and no arthrosis at 1 year
AO Foundation / BOA Principles
- No dedicated society guideline exists for this rare injury; management follows general trauma principles - document neurovascular status, attempt closed reduction, image to confirm, and stabilise irreducible or unstable joints