Avulsion Injury | Extensor Mechanism | Ogden Classification
- Mechanism: eccentric quadriceps contraction pulling patellar tendon off tubercle
- Type III involves articular surface - MUST achieve anatomic reduction
- Compartment syndrome risk from anterior tibial artery disruption
- Usually adolescents but also occurs in adults with violent mechanism
- “Check for extensor lag - indicates complete avulsion
- “Lateral radiograph best for diagnosis
- “Monitor for compartment syndrome post-injury and post-op
- “Subtype A vs B: B has comminuted fragment - may need additional fixation
Tibial Tubercle Fractures
Anterior tibial recurrent artery at risk. Runs near tibial tubercle. Injured during fracture/reduction. Can cause anterior compartment syndrome. MONITOR closely post-injury and post-op.
Pain out of proportion. Pain with passive toe extension. Anterior compartment tense. Paresthesia anterior leg/foot. If concerned: check pressures or fasciotomy.
Overview
Overview
Tibial tubercle fractures are avulsion injuries caused by forceful contraction of the quadriceps against resistance, most commonly during jumping or landing activities. While classically described in adolescents (particularly males aged 14-16 with an open tibial tubercle physis), these injuries also occur in adults with sufficiently violent mechanisms.
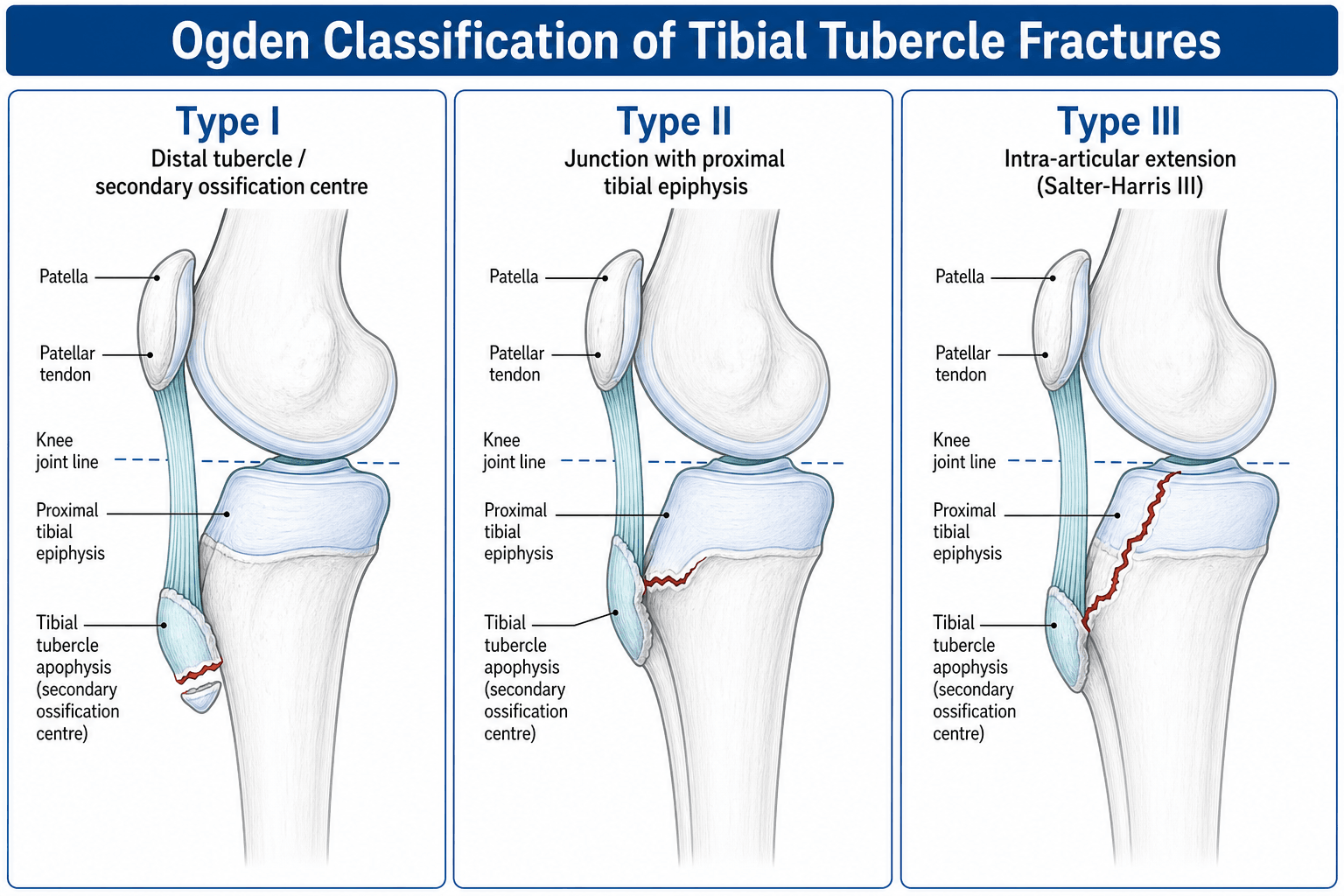
The Ogden classification (modification of Watson-Jones) categorizes these fractures based on the proximal extent: Type I involves only the secondary ossification center of the tubercle, Type II extends to the junction with the main tibial ossification center, and Type III extends into the tibial plateau articular surface. Each type has A (single fragment) and B (comminuted) subtypes.
A critical complication to recognize is anterior compartment syndrome, which occurs due to injury to the anterior tibial recurrent artery that runs near the tubercle. This must be monitored both at presentation and postoperatively.
Anatomy
Anatomy and Biomechanics
Tibial Tubercle Anatomy
- Tibial tubercle = secondary ossification center
- Appears around age 10-12
- Fuses distally first, then proximally
- Completely fused by 17-18 years
- Vulnerable during final fusion period
- Patellar tendon inserts on tubercle
- Transmits quadriceps force
- Maximum stress during eccentric contraction
- Anterior tibial recurrent artery
- Runs near tubercle
- At risk during injury
- Source of compartment syndrome
Biomechanics of Injury
- Violent quadriceps contraction
- Against fixed or flexed knee
- Eccentric load on extensor mechanism
- Patellar tendon avulses tubercle
- Basketball (jumping/landing)
- Volleyball
- High jump
- Sprinting
- Any deceleration injury
Classification Systems
Classification
Ogden Classification (Modified Watson-Jones)
Type I - Through Secondary Ossification Center
- Fracture limited to tubercle apophysis
- Does not extend to main tibial body
- Lowest energy pattern
- Subtype IA: Single fragment, often minimally displaced
- Subtype IB: Comminuted apophysis
Type II - Junction of Ossification Centers
- Extends to junction with main tibial physis
- More significant injury
- Usually displaced
- Subtype IIA: Single large fragment
- Subtype IIB: Comminuted at junction
Type III - Extends to Articular Surface
- Propagates into tibial plateau
- Intra-articular fracture
- Most severe pattern
- Subtype IIIA: Single fragment with joint involvement
- Subtype IIIB: Comminuted articular involvement
Type IV - Posterior Extension (Later Addition)
- Fracture extends posterior to physis
- May involve entire proximal tibia
- High-energy mechanism
This classification system guides surgical planning and predicts outcomes.
Clinical Presentation
Clinical Presentation
History
- Jumping activity (basketball, volleyball)
- Sudden deceleration
- Missed step/landing
- Direct blow (less common)
- Sudden anterior knee pain
- Unable to extend knee (complete tear)
- Felt "pop" or "snap"
- Cannot weight-bear
Physical Examination
- Swelling at anterior proximal tibia
- Palpable/visible defect at tubercle
- High-riding patella (if complete)
- Ecchymosis
- Tender tubercle
- Gap at fracture site
- Avulsed fragment may be palpable
- Finding
- Unable or weak
- Significance
- Complete avulsion
- Finding
- Loss of full extension
- Significance
- Extensor mechanism disruption
- Finding
- High (alta)
- Significance
- Tendon/tubercle avulsion
Compartment Syndrome Assessment (CRITICAL):
- Anterior compartment tension
- Pain with passive toe flexion
- Paresthesia anterior leg
- Check within 24-48 hours
Differential Diagnosis
- Distinguishing Features
- Adolescent, jumping mechanism, bony fragment at tubercle on lateral XR, high-riding patella if complete
- Key Discriminator
- Osseous avulsed fragment on radiograph
- Distinguishing Features
- Adult (often over 40 or steroid/tendinopathy history), no bony fragment, patella alta
- Key Discriminator
- Soft-tissue gap, no fragment on XR; ultrasound/MRI confirms
- Distinguishing Features
- Direct blow or eccentric load, fracture at patella not tubercle, extensor lag
- Key Discriminator
- Fracture line within patella on XR
- Distinguishing Features
- Chronic activity-related pain, fragmented apophysis, no acute high-energy event
- Key Discriminator
- Chronic onset, no acute displacement
- Distinguishing Features
- Fracture line through proximal tibial physis, risk of vascular injury (popliteal)
- Key Discriminator
- Physeal rather than apophyseal line; assess popliteal vessels
- Distinguishing Features
- Younger child, avulsion at distal patellar pole, sparse ossification
- Key Discriminator
- Avulsion at patella pole, not tubercle
- Distinguishing Features
- Older adult, defect above patella, patella baja
- Key Discriminator
- Suprapatellar gap; loss of active extension
A tibial tubercle avulsion that is bilateral and simultaneous, follows trivial force, or occurs outside the typical mid-adolescent athletic male should prompt a search for an underlying systemic cause that has weakened the apophysis - it is a classic "both knees" viva trap. Recognised associations include vitamin D deficiency / nutritional rickets, renal osteodystrophy (secondary or tertiary hyperparathyroidism), osteogenesis imperfecta, and endocrinopathy; pre-existing Osgood-Schlatter disease is also over-represented. Work up with a bone profile (calcium, phosphate, alkaline phosphatase), 25-OH vitamin D, renal function and PTH, a medication review (chronic corticosteroids), and a metabolic-bone or endocrine referral where indicated. The fracture is still fixed on its merits, but identifying and treating the metabolic driver is what prevents a contralateral fracture or refracture.
Investigations
Investigations
Plain Radiographs
- AP and Lateral knee (lateral best)
- Compare to contralateral if uncertain
- Avulsed tubercle fragment
- Displacement (anterior/superior)
- Extent of fracture line
- Articular involvement
- May show fracture
- Assess for rotation
- Look for articular step
CT Scan
- Type III fractures (articular assessment)
- Complex/comminuted patterns
- Surgical planning
- Fracture extent
- Articular step-off
- Comminution
- Fragment size
MRI
Indications:
- Rule out associated soft tissue injury
- Assess meniscus/ligaments
- Not routine
The patellar tendon transmits an enormous load, and the same eccentric force can disrupt the extensor mechanism at more than one level - so do not let the obvious tubercle fragment stop your assessment. Specifically look for: (1) a second-level extensor injury - a concurrent patellar tendon avulsion or intrasubstance tear, or an inferior-pole patellar (sleeve) avulsion - producing a "double-level" disruption, so examine and image both the tubercle and the patella; (2) intra-articular associated lesions in Ogden III - osteochondral fragments, meniscal tears and tibial spine / ACL avulsions - which is exactly why direct articular visualisation (arthrotomy, or arthroscopic assistance) is valuable when the fracture enters the joint; and (3) retinacular tears, which must be repaired to restore the extensor mechanism. MRI is the investigation when a soft-tissue or second-level injury is suspected. Missing the second injury leaves the patient with a persistent extensor lag despite a perfectly fixed tubercle.
Management

Management
Non-Operative Treatment
- Type IA with minimal displacement (under 2mm)
- Intact extensor mechanism
- Compliant patient
- Long leg cast or cylinder cast
- Knee in extension
- Duration: 4-6 weeks
- Non-weight-bearing initially
- Close radiographic follow-up
- Weekly XR first 2 weeks
- Check for loss of reduction
- If displacement occurs, proceed to ORIF
- Displacement remains under 2mm
- No extensor lag develops
- Healing evident by 6 weeks
Close monitoring is essential for non-operative management success.
Surgical Technique
Surgical Technique
Patient Positioning and Setup
- Supine on radiolucent table
- Bump under ipsilateral hip
- Tourniquet on proximal thigh
- Image intensifier available
- Anterior midline or anterolateral incision
- 8-10 cm centered over tibial tubercle
- Protect infrapatellar branch of saphenous nerve
- Develop plane on either side of patellar tendon
Proper setup and positioning are essential for optimal visualization and surgical access to the tibial tubercle.
Complications
Complications
Compartment Syndrome (CRITICAL)
Historically quoted as high (10-20%) from early case reports, but contemporary data are reassuring: 3.57% in a systematic review (Pretell-Mazzini 2016), 0.46% in a 25,483-patient database (Milner 2024) and 0.4% in a population study (Koivisto 2022). Pandya (2012) reported nearly 10% in a high-energy operative cohort. The true risk is therefore low but non-trivial, and clinical vigilance remains mandatory.
- Anterior tibial recurrent artery injury
- Bleeding into anterior compartment
- Can occur post-injury or post-op
- High index of suspicion
- Serial examinations
- Low threshold for pressure check
- Emergent fasciotomy if confirmed
Other Complications
- Recurvatum deformity
- Leg length discrepancy
- More common if physis damaged
- Extensor mechanism adhesions
- Usually responds to therapy
- May need manipulation under anesthesia
- Rare with adequate fixation
- May need revision surgery
- If return to sport too early
- Uncommon with proper rehabilitation
- Hardware irritation
- Bony prominence
- May need hardware removal
Postoperative Care
Postoperative Care
Immediate Postoperative Period (0-48 hours)
- Neurovascular checks every 2-4 hours
- Compartment syndrome surveillance
- Pain out of proportion should trigger immediate assessment
- Check anterior compartment tension
- Low threshold for pressure measurement
- Knee immobilizer or cylinder cast
- Knee in full extension
- Elevation of leg
- Ice therapy
- Non-weight-bearing initially
- Toe-touch weight-bearing with crutches
- Upper extremity strengthening
Early Phase (0-2 weeks)
- Dressing change at 2-3 days
- Suture/staple removal at 14 days
- Monitor for infection
- If fixation stable: begin passive ROM day 2-3
- Gentle heel slides
- Limit flexion to 30 degrees first week
- Progress to 60 degrees by 2 weeks
- Avoid active extension initially
- Multimodal analgesia
- Avoid NSAIDs first 6 weeks (fracture healing)
- Ice and elevation
Intermediate Phase (2-6 weeks)
- Week 2-4: Partial weight-bearing (50%)
- Week 4-6: Weight-bearing as tolerated
- Wean from crutches when comfortable
- Progress flexion by 15 degrees per week
- Goal: 90 degrees by 6 weeks
- Active assisted ROM
- Add active quadriceps exercises week 4
- Quad sets starting week 2
- Straight leg raises week 4
- Closed kinetic chain exercises week 6
- 2 weeks: Check fixation, early healing
- 6 weeks: Assess union
- 12 weeks: Confirm healing
Late Phase (6-12 weeks)
- Advance to full weight-bearing
- Goal: Full ROM by 12 weeks
- Progressive resistance exercises
- Proprioception training
- Balance exercises
- Stationary bike week 8
- Light jogging week 12 (if healed)
- Sport-specific drills week 16
- Full return to sport: 4-6 months
Criteria for Progression
- Radiographic evidence of healing
- Minimal pain with protected weight-bearing
- No increase in swelling
- No increase in effusion
- Comfortable with current ROM
- Fixation intact on XR
- Full ROM compared to contralateral
- Quadriceps strength over 90% of opposite side
- Hop testing over 90% of opposite side
- Pain-free with running and jumping
- Radiographic union complete
Complications to Monitor
- Compartment syndrome
- Wound infection
- Loss of fixation
- Stiffness
- Nonunion
- Hardware irritation
- Malunion
- Growth disturbance (adolescents)
- Persistent prominence
Outcomes/Prognosis
Outcomes and Prognosis
Overall Outcomes
Excellent Results Expected (systematic review data, Pretell-Mazzini 2016, PMID 25887827):
- Return to pre-injury activity and full knee ROM each reached ~98% regardless of fracture type
- Fracture union achieved in ~99% of cases
- Mean return to sport around 4-6 months in reported cohorts
- Overall complication rate ~28%, dominated by symptomatic implant requiring removal (the commonest reoperation)
Outcomes by Ogden Type
- Best prognosis
- Union rate: 98-100%
- Minimal risk of growth disturbance
- Rare complications if treated appropriately
- Excellent outcomes with ORIF
- Union rate: 95-98%
- Low complication rate
- Full ROM expected
- Good outcomes with anatomic reduction
- Articular step-off over 2mm associated with worse outcomes
- May develop mild post-traumatic arthritis (5-10%)
- Requires longer rehabilitation
Prognostic Factors
- Early diagnosis and treatment (within 7 days)
- Anatomic reduction achieved
- Stable fixation allowing early motion
- Good rehabilitation compliance
- Non-articular fractures (Type I/II)
- Delayed diagnosis (over 2 weeks)
- Articular step-off over 2mm
- Development of compartment syndrome
- Infection
- Loss of fixation requiring revision
Specific Outcome Measures
- 95% achieve full ROM by 6 months
- Early stiffness common but resolves with therapy
- Extension deficit rare (under 5%) with proper treatment
- Quadriceps strength returns to 90% by 4 months
- Full strength by 6-8 months
- Isokinetic testing shows symmetric strength at 1 year
- Union typically evident by 8-12 weeks
- Nonunion rare (under 2%) with adequate fixation
- Malunion uncommon with anatomic reduction
- Light activities: 6-8 weeks
- Full weight-bearing: 8-12 weeks
- Running: 3-4 months
- Full sport participation: 4-6 months
- Contact sports: 6 months minimum
Growth-Related Outcomes (Adolescents)
- Incidence: 5-10% overall
- Recurvatum deformity most common
- Usually mild (under 5 degrees)
- Rarely requires corrective osteotomy
- Rare (under 5%)
- Usually under 1cm
- Does not typically require treatment
Long-Term Outcomes
- No pain in 95% of patients
- Full return to pre-injury activity level
- Bony prominence may persist (hardware removal sometimes needed)
- No difference in outcomes between adolescents and adults
- Mild post-traumatic arthritis in 10% of Type III fractures
- Usually asymptomatic
- No increased risk of patellofemoral problems
- Ossicle formation at fracture site occasional finding
Factors Affecting Return to Sport
- Type I fractures
- Non-displaced or minimally displaced
- Excellent fixation
- Early mobilization
- Good rehabilitation compliance
- Type III articular fractures
- Comminuted patterns
- Compartment syndrome requiring fasciotomy
- Post-operative stiffness
- Loss of fixation
Patient Satisfaction
High Satisfaction Rates:
- Over 90% patient satisfaction at 1 year
- Most patients would undergo same treatment again
- Return to desired activity level achieved
- Minimal long-term disability
Guidelines, Registries & Global Practice
Guidelines, Registries & Global Practice
Tibial tubercle fractures are uncommon worldwide and there is no dedicated AAOS, NICE, BOA-BOAST or EFORT clinical practice guideline specific to them. Management is therefore consensus- and evidence-based rather than guideline-mandated, and the principles below are consistent across high-income health systems.
Global Epidemiology
- Figure
- ~21 per 100,000 per year
- Source (PubMed)
- Koivisto 2022 (PMID 36268729)
- Figure
- 15 years (mid-adolescence)
- Source (PubMed)
- Koivisto 2022; Pretell-Mazzini 2016
- Figure
- Strong male predominance
- Source (PubMed)
- Ogden 1980; Cole 2020
- Figure
- Type III (intra-articular), ~50%
- Source (PubMed)
- Pretell-Mazzini 2016 (PMID 25887827)
- Figure
- Over-represented vs general population
- Source (PubMed)
- Ogden 1980 (PMID 7358751)
- Figure
- ~99%
- Source (PubMed)
- Pretell-Mazzini 2016
Mechanism is near-universal: eccentric quadriceps loading during jumping or sprinting at the end of physeal closure, when the tubercle apophysis is mechanically vulnerable (Cole 2020, PMID 32304501).
Where Guidance Converges (Global Standard of Care)
- Accepted position
- Ogden (modified Watson-Jones) is the working standard; CT-based schemes (Pandya) add intra-articular detail
- Evidence level
- IV-III
- Accepted position
- Lateral radiograph for screening; CT for suspected intra-articular/physeal extension (lateral view alone underestimates 50%)
- Evidence level
- III (Pandya, PMID 23147615)
- Accepted position
- Reserved for minimally displaced (under 2 mm) extra-articular fractures with intact extensor mechanism
- Evidence level
- IV
- Accepted position
- Displaced, intra-articular, or extensor-mechanism-disrupting fractures - ORIF (screws +/- tension band/plate)
- Evidence level
- III-IV
- Accepted position
- Restore extensor mechanism and articular congruity; stable fixation for early motion
- Evidence level
- III (Cole 2020)
- Accepted position
- Recognised emergency; vigilance 24-48 h despite low absolute risk
- Evidence level
- IV (Pape, PMID 8403649)
Registry Evidence
This is a paediatric/adolescent trauma entity, not an arthroplasty or implant-survival topic, so the national joint registries (NJR, AJRR, AOANJRR, SHAR, NZJR) do not capture it. The best population-level denominators come instead from dedicated paediatric fracture databases: the Finnish Kids' Fracture Tool (Koivisto 2022, incidence and 0.4% compartment-syndrome rate) and large US administrative cohorts (Milner 2024, 25,483 patients, 0.46% compartment-syndrome rate, PMID 39482931). These have been pivotal in revising the historical 10-20% compartment-syndrome teaching downwards.
Practice Variation
- Imaging thresholds: centres with ready CT access image intra-articular patterns routinely (Pandya approach); resource-limited settings rely on the lateral radiograph and intra-operative assessment.
- Fixation choice: cannulated screws for large single fragments versus tension-band/suture-augmented constructs for comminuted apophyseal fragments - surgeon and resource dependent, with no high-level comparative trial.
- Physeal-sparing concern: emphasised in skeletally immature patients, though most injuries occur peri-closure so growth disturbance is uncommon.
- NSAID avoidance in early fracture healing remains common practice but rests on mixed evidence and varies between units.
- Antibiotic prophylaxis for the rare open fracture follows local trauma protocols (e.g. first-generation cephalosporin for low-grade open injury) rather than a tubercle-specific guideline.
Long-Term Follow-Up
Skeletally immature patients are followed to maturity to detect genu recurvatum or limb-length discrepancy from proximal tibial physeal injury, both uncommon with isolated tubercle fractures. Skeletally mature patients need shorter follow-up centred on union, return to activity, and symptomatic-hardware assessment (the commonest reason for reoperation; Pretell-Mazzini 2016).
Viva Scenarios
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 15-year-old male basketball player lands awkwardly and presents with severe anterior knee pain. He cannot actively extend his knee. Examination shows significant swelling anterior proximal tibia, palpable defect at tibial tubercle, unable to perform straight leg raise, high-riding patella. Neurovascularly intact. Anterior compartment soft.”
“You are asked to describe the Ogden classification for tibial tubercle fractures and explain how it guides your management.”
“6 hours after ORIF of a tibial tubercle fracture, the patient complains of severe anterior leg pain. Examination shows anterior compartment tense and tender, severe pain with passive toe extension, paresthesia in first web space, foot cool compared to other side.”
MCQ Practice Points
MCQ Practice Points
Q: What is the Ogden classification for tibial tubercle fractures? A: Type I = fracture through secondary ossification center only, Type II = fracture at junction with main ossification center, Type III = fracture extends to articular surface (intra-articular). Each has subtypes A (single fragment) and B (comminuted). Type III MUST have anatomic reduction because it involves the joint surface. This is THE standard classification system.
Q: What is the compartment syndrome risk with tibial tubercle fractures and why? A: Anterior compartment syndrome from anterior tibial recurrent artery injury. The "10-20%" figure comes from early case reports; contemporary large series and population data show roughly 0.4-4% (Pretell-Mazzini 3.57%, Milner 0.46%, Koivisto 0.4%), with up to ~10% in high-energy operative cohorts (Pandya). The point examiners want: the mechanism (anterior tibial recurrent artery) and that it is a treatable emergency. Monitor closely for 24-48 hours post-injury and post-operatively, low threshold for fasciotomy. Pain out of proportion is the earliest and most reliable sign.
Q: What finding indicates complete extensor mechanism disruption and absolute need for surgery? A: Extensor lag (inability to actively extend the knee) or inability to perform straight leg raise indicates complete extensor mechanism disruption and is an absolute indication for ORIF. High-riding patella (patella alta) is another sign of complete disruption. These patients need urgent surgical repair.
Q: What is the displacement threshold for surgical treatment of tibial tubercle fractures? A: 2mm is the magic number. Displacement over 2mm is the threshold for surgical treatment. Type IA fractures with displacement under 2mm may be treated conservatively with casting, but require close weekly radiographic follow-up for the first 2 weeks to ensure no loss of reduction.
Q: What is the best radiographic view for diagnosing tibial tubercle fractures? A: The lateral knee radiograph is the best view for diagnosis and classification. AP views may miss the fracture or underestimate displacement. Always order both AP and lateral views, but the lateral is key for decision-making and surgical planning.
Q: What growth considerations are important when treating adolescent tibial tubercle fractures? A: These fractures occur during the vulnerable period of tibial tubercle fusion (ages 14-16). Avoid crossing the physis with fixation if possible by placing screws parallel to the physis. Growth disturbance (recurvatum deformity) occurs in 5-10% but is usually mild. Monitor until skeletal maturity (approximately 18 years).
High-Yield Facts for Exam
- Ogden Type I = secondary ossification center only
- Ogden Type II = junction of ossification centers
- Ogden Type III = extends to articular surface (intra-articular)
- Each type has subtype A (single fragment) and B (comminuted)
- Watson-Jones classification is historical; Ogden is standard
- Eccentric quadriceps contraction during jumping/landing
- Patellar tendon avulses tibial tubercle
- Peak age: 14-16 years (adolescent males)
- Can occur in adults with violent mechanism
- Compartment syndrome risk roughly 0.4-4% in large/population series (the classic "10-20%" derives from early case reports); higher in high-energy injuries
- Caused by anterior tibial recurrent artery injury
- Monitor closely first 24-48 hours post-injury and post-op
- Low threshold for fasciotomy
- Lateral radiograph best for diagnosis
- Extensor lag indicates complete avulsion
- High-riding patella (patella alta) suggests extensor mechanism disruption
- CT scan for Type III to assess articular involvement
- Type IA with displacement under 2mm: may trial casting
- Type II and III: usually require ORIF
- Type III requires anatomic articular reduction
- Cannulated screws for large single fragments
- Tension band wiring for comminuted patterns
- Early passive ROM if fixation stable
- Protected weight-bearing 2-6 weeks
- Return to sport: 4-6 months
- Avoid crossing physis in adolescents
- Excellent outcomes in over 95% with ORIF
- Full return to sport expected in 90%
- Growth disturbance uncommon (5-10%)
- Long-term complications rare
Common Exam Scenarios
15-year-old basketball player unable to extend knee after landing
- Answer: Tibial tubercle avulsion with complete extensor mechanism disruption, requires ORIF
Post-op day 1, severe anterior leg pain out of proportion
- Answer: Compartment syndrome, emergent fasciotomy indicated
Lateral XR shows fracture extending to tibial plateau
- Answer: Ogden Type III, requires anatomic articular reduction
Type IA fracture with 1mm displacement
- Answer: May trial non-operative management with casting
Comminuted tubercle fracture in 15-year-old
- Answer: Ogden Type IB or IIB, tension band wiring appropriate
Key Differentials
- Tubercle avulsion: bony fragment on XR
- Tendon rupture: no bony fragment, soft tissue injury
- Acute fracture: acute traumatic event, displacement
- Osgood-Schlatter: chronic apophysitis, no acute trauma
- Type III: fracture line from tubercle to joint
- Physeal fracture: through proximal tibial physis (Salter-Harris pattern)
Must-Know Numbers
- Peak age: 14-16 years
- Compartment syndrome risk: roughly 0.4-4% (large/population series; classic teaching of 10-20% is from early case reports)
- Displacement threshold for surgery: over 2mm
- Union rate with ORIF: over 95%
- Return to sport: 4-6 months
- Growth disturbance risk: 5-10%
Exam Traps to Avoid
Assuming all tibial tubercle fractures are in adolescents
- Reality: Can occur in adults with violent mechanism
Missing compartment syndrome
- Key: High index of suspicion, monitor closely
Not recognizing need for anatomic reduction in Type III
- Key: Articular involvement requires perfect reduction
Crossing physis with fixation in adolescents
- Key: Place screws parallel to physis when possible
Assuming conservative treatment always fails
- Reality: Type IA with minimal displacement may heal with casting
At a Glance
Tibial tubercle fractures are avulsion injuries caused by eccentric quadriceps contraction pulling the patellar tendon off the tubercle. Most common in adolescent males (14-16 years) with open physes but can occur in adults. Classified by Ogden: Type I through secondary ossification center; Type II at junction of ossification centers; Type III extends to articular surface (must achieve anatomic reduction). Critical complication: anterior compartment syndrome from anterior tibial recurrent artery injury (historically over-stated; large series and population data show roughly 0.4-4%, but it remains a feared, treatable emergency). Treatment is ORIF with screws for displaced fractures; cast only for minimally displaced Type IA. Monitor compartments closely post-injury and post-operatively.
- Fracture Pattern
- Minimally displaced, small fragment
- Management
- Long leg cast, close follow-up
- Fracture Pattern
- Comminuted secondary center
- Management
- ORIF with screws/tension band
- Fracture Pattern
- Displaced, junction fracture
- Management
- ORIF with cannulated screws
- Fracture Pattern
- Comminuted junction
- Management
- ORIF, may need additional fixation
- Fracture Pattern
- Extends into joint, large fragment
- Management
- ORIF - anatomic articular reduction
- Fracture Pattern
- Comminuted into joint
- Management
- ORIF, possible buttress plate
- Fracture Pattern
- Complete avulsion
- Management
- Urgent surgical repair
- Fracture Pattern
- Any type
- Management
- Emergent fasciotomy
OGDENOGDEN for Classification
Hook:OGDEN: 1-2-3 gets progressively worse and more proximal!
TUBERCLETUBERCLE for Exam
Hook:TUBERCLE - the whole story of these fractures!
JUMPJUMP for Mechanism
Hook:JUMPing causes the tubercle to JUMP off the tibia!
ABSubtype A vs B
Hook:B = Broken (comminuted)!
Exam Cheat Sheet
Exam Day Cheat Sheet
Mechanism
- Eccentric quadriceps contraction
- Jumping/landing activities
- Patellar tendon avulses tubercle
- Usually adolescent males (14-16)
Ogden Classification
- Type I: Secondary ossification center only
- Type II: Junction of ossification centers
- Type III: Extends to articular surface
- Subtypes: A (single), B (comminuted)
Clinical Assessment
- Extensor lag = complete avulsion
- High-riding patella
- Lateral XR best for diagnosis
- Monitor for compartment syndrome
Management
- Type IA minimally displaced: may cast
- Type II/III: ORIF indicated
- Cannulated screws or tension band
- Anatomic reduction for Type III
Compartment Syndrome
- Roughly 0.4-4% (large series)
- Anterior tibial recurrent artery
- Monitor 24-48 hours post-injury/surgery
- Low threshold for fasciotomy
Return to Sport
- 4-6 months typically
- Must have full strength
- Pain-free range of motion
- Excellent prognosis with ORIF
Quick Reference: Key Numbers
- Value
- 14-16 years
- Value
- Roughly 0.4-4% (large series)
- Value
- Over 2mm
- Value
- 4-6 weeks
- Value
- 4-6 months
- Value
- Over 95%
Ogden Classification Summary
- Location
- Secondary center, single
- Treatment
- Cast or ORIF
- Location
- Secondary center, comminuted
- Treatment
- ORIF
- Location
- Junction, single
- Treatment
- ORIF
- Location
- Junction, comminuted
- Treatment
- ORIF
- Location
- Articular, single
- Treatment
- ORIF (anatomic)
- Location
- Articular, comminuted
- Treatment
- ORIF + buttress
Evidence
Evidence Base
Ogden Classification (Defining Paper)
- Review of 15 physeal tibial tuberosity fractures in 14 adolescents that produced the modified classification (Types I-III, with A/B subtypes for comminution) emphasising intra-articular extension. Primary surgical indications were anterosuperior fragment displacement and fracture extension through the proximal tibial ossification centre into the joint. An increased incidence of pre-existing Osgood-Schlatter disease was noted, and complications were rare.
Compartment Syndrome First Described in This Fracture
- Case series of adolescent boys who developed anterior compartment syndrome after tibial tubercle avulsion. The authors implicated injury to branches of the anterior tibial recurrent artery near the tubercle and argued that soft-tissue injury is more extensive than usually appreciated, establishing compartment syndrome as a recognised complication of this fracture.
Population Incidence and True Compartment Syndrome Rate
- Population-based study (Kids' Fracture Tool, 241 proximal tibial fractures including 42 tibial tubercle fractures). Tibial tubercle fractures peaked at age 15 with an estimated incidence of 21 per 100,000 in 13-16 year-olds. Compartment syndrome occurred in 0.4% (1/241) and vascular compromise in 0%, much lower than historically reported.
Compartment Syndrome - Large Database Comparison
- Matched-cohort analysis of 25,483 paediatric patients found acute compartment syndrome in only 0.46% of tibial tubercle fractures - significantly lower than the 0.70% rate after tibial shaft fractures. Male sex and increasing age were risk factors. This refutes the long-held assumption that tibial tubercle fractures carry a uniquely high compartment-syndrome risk.
Lateral Radiograph Underestimates Injury - Role of CT
- 41 operatively treated tibial tubercle fractures. A single lateral radiograph underestimated or missed injury severity in 50% of cases; CT/MRI revealed consistent 3D fragment patterns (anterior sagittal, lateral coronal, anterolateral axial). Compartment syndrome or vascular compromise occurred in nearly 10% (all physeal-pattern injuries). All fractures united; 2 developed premature physeal closure.
Outcomes and Complications - Systematic Review
- Systematic review of 23 studies (336 fractures, mean age 14.6 y). Type III was the most common pattern (50.6%); compartment syndrome occurred in 3.57%; ORIF was used in 98% of operative cases. Return to pre-injury activity and full knee ROM each reached 98% and union was achieved in 99.4%. The overall complication rate was 28.3%, dominated by symptomatic implant requiring removal (55.8% of complications).
Contemporary Review of Diagnosis and Management
- Narrative review confirming the injury as rare, typically in adolescent boys in jumping/sprinting sports, with avulsion predisposed by the distal-to-proximal (posteromedial to anterolateral) pattern of proximal tibial physeal closure. The Ogden classification continues to guide non-operative versus operative management, with multiple fixation methods all aimed at restoring the extensor mechanism and joint surface.