SITS Muscles | Supraspinatus Most Common | Tear Size Predicts Outcome | Repair vs Reconstruction
- SITS muscles: Supraspinatus, Infraspinatus, Teres minor, Subscapularis - rotator cuff components
- Force couple concept: RC depresses humeral head while deltoid elevates - loss disrupts mechanics
- Tear progression: Natural history shows increasing size and fatty infiltration over time
- Double-row repair: Improved footprint contact and biomechanical strength vs single-row
- Irreparable tears: Massive retracted tears with Goutallier Grade 3-4 fatty infiltration
- “Supraspinatus initiates abduction - tear causes painful arc 60-120 degrees
- “External rotation lag sign indicates infraspinatus/teres minor insufficiency
- “Subscapularis tear: belly-press test, lift-off test, bear-hug test positive
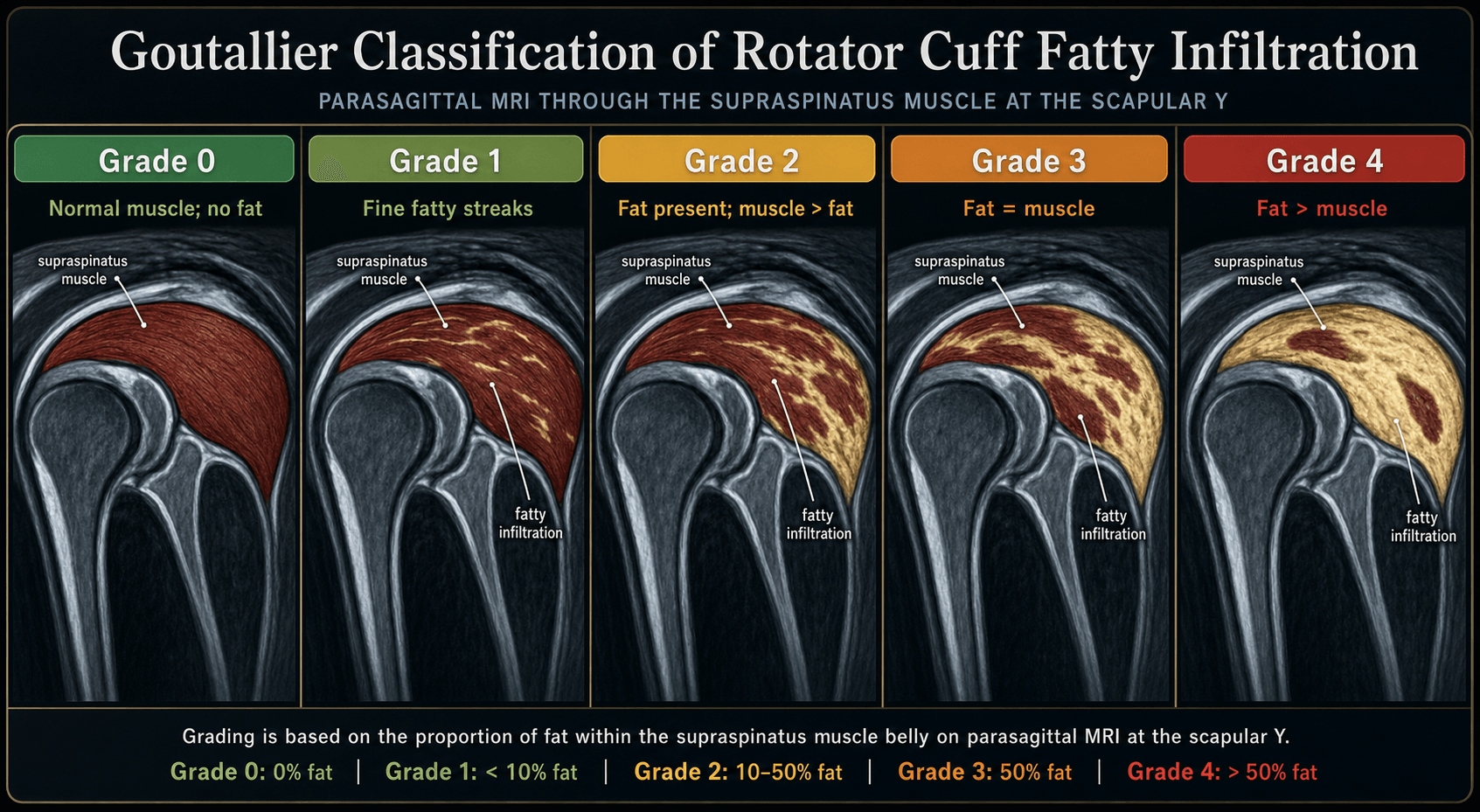
- “MRI shows tendon gap, retraction, muscle atrophy, fatty infiltration (Goutallier)

Four muscles form the rotator cuff: Supraspinatus (superior), Infraspinatus (posterior-superior), Teres minor (posterior-inferior), Subscapularis (anterior). SITS mnemonic. Supraspinatus is the most commonly torn tendon - critical area at footprint 1cm medial to greater tuberosity.
Hypovascular zone exists 1cm medial to supraspinatus insertion - watershed area between osseous and muscular blood supply. This critical zone is prone to degeneration and tears. Blood supply from suprascapular, anterior circumflex humeral, and posterior circumflex humeral arteries.
The rotator cuff creates a force couple with deltoid: RC compresses and depresses humeral head while deltoid elevates arm. Loss of this balance causes superior migration of humeral head and subacromial impingement. Subscapularis counterbalances posterior cuff.
Natural history shows progression in size and quality. Goutallier grading (0-4) quantifies fatty infiltration - Grade 3-4 predicts poor repair outcomes. Patte staging (1-3) measures retraction. Tangent sign on MRI indicates advanced atrophy.
- Tear Characteristics
- Small-medium tear, minimal retraction
- Treatment
- Arthroscopic single or double-row repair
- Key Pearl
- Early repair prevents progression and muscle atrophy
- Tear Characteristics
- Large tear (3-5cm), moderate fatty change
- Treatment
- Double-row repair with margin convergence
- Key Pearl
- Repair still possible but rehabilitation longer
- Tear Characteristics
- Massive tear, Goutallier 3-4
- Treatment
- Conservative management or reverse TSA
- Key Pearl
- Repair likely to fail - focus on function
- Tear Characteristics
- Greater than 5cm, severe retraction, fatty change
- Treatment
- Superior capsular reconstruction or graft augmentation
- Key Pearl
- Bridging option before arthroplasty
SITSSITS - Rotator Cuff Components
Hook:The rotator cuff SITS on the humeral head - four muscles stabilizing the glenohumeral joint
EMPTYEMPTY CAN - Supraspinatus Testing
Hook:EMPTY CAN test - like emptying a can with thumb down - isolates supraspinatus function
LAGERLAGER - External Rotation Lag Signs
Hook:LAGER - like a lager falling when you let go - the arm lags in external rotation with posterior cuff tear
BEARBEAR - Subscapularis Testing
Hook:BEAR HUG test - hugging like a bear tests the anterior cuff subscapularis muscle
Overview and Epidemiology
Rotator cuff tears are among the most common shoulder pathologies, representing a spectrum from partial-thickness tears to massive full-thickness defects involving multiple tendons. They result from a combination of intrinsic tendon degeneration and extrinsic mechanical factors.
Epidemiology:
- Prevalence increases dramatically with age - rare under 40, common over 60
- Many tears are asymptomatic (up to 50% of individuals over 60 have tears on imaging)
- Symptomatic tears often present with pain, weakness, and functional limitations
- Occupational and sports-related overhead activities increase risk
Many rotator cuff tears are asymptomatic, particularly in older individuals. The decision to treat is based on symptoms, functional impairment, and patient goals - not just the presence of a tear on imaging. Asymptomatic tears may progress over time to become symptomatic.
Etiology - Multifactorial:
- Tendon degeneration: Age-related collagen breakdown, decreased vascularity
- Hypovascular zone: Critical zone 1cm medial to insertion
- Genetics: Family history increases risk
- Smoking: Impairs healing, increases tear size
- Subacromial impingement: Type I (flat), II (curved), III (hooked) acromion
- Os acromiale: Unfused acromial apophysis causing impingement
- Trauma: Acute on chronic, fall on outstretched hand
- Overuse: Repetitive overhead activity (swimmers, painters, throwers)
Natural History:
- Tear size tends to increase over time (approximately 40% enlarge within 2 years)
- Muscle atrophy and fatty infiltration progress (often irreversible)
- Pain may decrease over time even as tear enlarges (pseudoparalytic shoulder)
- Functional deficits worsen with tear progression
Pathophysiology and Mechanisms
The Rotator Cuff Complex:
The rotator cuff consists of four muscles and their tendons that originate from the scapula and insert on the humeral head, forming a circumferential cuff around the glenohumeral joint.

- Origin
- Supraspinous fossa scapula
- Insertion
- Superior facet greater tuberosity
- Function
- Initiates abduction 0-30 degrees
- Nerve
- Suprascapular (C5-6)
- Origin
- Infraspinous fossa scapula
- Insertion
- Middle facet greater tuberosity
- Function
- External rotation, stabilization
- Nerve
- Suprascapular (C5-6)
- Origin
- Lateral border scapula
- Insertion
- Inferior facet greater tuberosity
- Function
- External rotation, adduction
- Nerve
- Axillary (C5-6)
- Origin
- Subscapular fossa scapula
- Insertion
- Lesser tuberosity
- Function
- Internal rotation, anterior stability
- Nerve
- Upper/lower subscapular (C5-7)
Blood Supply - Critical Zone:
The critical zone is a hypovascular area approximately 1cm medial to the supraspinatus insertion on the greater tuberosity. This represents a watershed zone between the osseous blood supply (from the humeral circumflex arteries) and the muscular blood supply (from the suprascapular and thoracoacromial arteries). This zone is particularly prone to degeneration and tear formation.
Arterial supply:
- Suprascapular artery - supplies supra/infraspinatus
- Anterior humeral circumflex artery - supplies anterior cuff and subscapularis
- Posterior humeral circumflex artery - supplies posterior cuff
- Thoracoacromial artery - contributes to anterior structures
Biomechanics - Force Couple Concept:
The rotator cuff creates force couples that stabilize the humeral head:
- Coronal plane: Deltoid (superior force) vs. infraspinatus/teres minor/subscapularis (inferior force)
- Transverse plane: Subscapularis (anterior force) vs. infraspinatus/teres minor (posterior force)
When the rotator cuff is torn, the force couple is disrupted. The deltoid pulls the humeral head superiorly without the opposing inferior force from the cuff. This causes superior migration of the humeral head, leading to subacromial impingement, acromioclavicular joint arthritis, and eventually rotator cuff arthropathy.
Functional Roles:
- Supraspinatus: Initiates abduction, provides superior compression
- Infraspinatus/Teres minor: External rotation, posterior stabilization
- Subscapularis: Internal rotation, anterior stabilization, resists posterior subluxation
Classification Systems
Cofield Classification by Tear Size
Based on maximum tear dimension in any plane:
- Dimension
- Less than 1cm
- Typical Repair
- Single-row arthroscopic
- Prognosis
- Excellent healing
- Dimension
- 1-3cm
- Typical Repair
- Double-row arthroscopic
- Prognosis
- Good healing potential
- Dimension
- 3-5cm
- Typical Repair
- Double-row with convergence
- Prognosis
- Guarded, longer rehab
- Dimension
- Greater than 5cm or 2+ tendons
- Typical Repair
- SCR or reverse TSA
- Prognosis
- Poor repair outcomes
A massive tear is defined as either: (1) greater than 5cm in maximum dimension, OR (2) involvement of two or more complete tendons. These tears have poor healing potential with standard repair and may require alternative treatments like superior capsular reconstruction or reverse total shoulder arthroplasty.
Clinical Assessment
History:
- Location: Anterolateral shoulder, often radiates to deltoid insertion
- Timing: Night pain common (lying on shoulder), difficulty sleeping
- Activity: Pain with overhead activities, reaching behind back
- Onset: Acute traumatic vs insidious degenerative
- Weakness: Difficulty with overhead activities, lifting
- Loss of motion: Active motion reduced more than passive
- Activities: Difficulty with hair combing, reaching for wallet
- Occupational: Impact on work, sports, daily living
Physical Examination:
Inspection and Range of Motion
- Inspect: Muscle atrophy (supraspinatus/infraspinatus fossae), asymmetry, scapular dyskinesis
- Active ROM: Often limited by pain and weakness (pseudoparalysis if massive tear)
- Passive ROM: Should be preserved (if limited, consider frozen shoulder, arthritis)
- Painful arc: Pain between 60-120 degrees abduction indicates impingement
Specific Tests for Individual Tendons
- Tendon Tested
- Supraspinatus
- Technique
- Arm 90deg abducted, 30deg forward, thumb down, resist downward force
- Positive Finding
- Pain or weakness
- Tendon Tested
- Supraspinatus
- Technique
- Arm 90deg abducted, 30deg forward, thumb up, resist downward force
- Positive Finding
- Pain or weakness (more specific)
- Tendon Tested
- Infraspinatus
- Technique
- Elbow 90deg flexed, arm at side, passively externally rotate, patient maintains
- Positive Finding
- Arm drops greater than 10 degrees
- Tendon Tested
- Teres minor
- Technique
- Arm 90deg abducted, elbow 90deg, externally rotate against resistance
- Positive Finding
- Cannot maintain external rotation
- Tendon Tested
- Subscapularis
- Technique
- Hand behind back, lift off from back against resistance
- Positive Finding
- Cannot lift hand off back
- Tendon Tested
- Subscapularis
- Technique
- Press hand against belly with elbow forward
- Positive Finding
- Elbow moves posterior to trunk
- Tendon Tested
- Subscapularis
- Technique
- Hand on opposite shoulder, resist pull-off
- Positive Finding
- Cannot resist or elbow drops
The external rotation lag sign is highly specific for a posterosuperior rotator cuff tear (infraspinatus/teres minor). A positive lag greater than 10 degrees indicates a large tear. The hornblower's sign (inability to externally rotate at 90 degrees abduction) suggests an even larger tear involving teres minor.
Impingement Tests
- Neer impingement sign: Passive forward flexion causes pain (subacromial impingement)
- Hawkins-Kennedy test: 90deg forward flexion, internal rotation causes pain
- These tests are sensitive but not specific for rotator cuff tears
Strength Testing
- Supraspinatus strength: Empty can or full can test
- External rotation strength: Resisted ER at side and at 90deg abduction
- Internal rotation strength: Resisted IR (belly press, lift-off)
- Pseudoparalysis: Inability to actively elevate arm despite full passive motion (massive tear)
Differential Diagnosis
- Key Distinguishing Features
- Active more than passive motion loss, night pain, weakness in plane of torn tendon
- Discriminating Test/Imaging
- Positive lag/empty-can tests; MRI or ultrasound shows tendon defect
- Key Distinguishing Features
- Global loss of BOTH active AND passive motion, especially external rotation
- Discriminating Test/Imaging
- Equal active/passive restriction; near-normal cuff on imaging
- Key Distinguishing Features
- Painful arc with preserved strength, no true tendon discontinuity
- Discriminating Test/Imaging
- Positive Neer/Hawkins; MRI shows tendinopathy without full-thickness gap
- Key Distinguishing Features
- Stiffness, crepitus, deep joint-line pain, reduced passive rotation
- Discriminating Test/Imaging
- Radiographs show joint-space loss, osteophytes, often intact cuff
- Key Distinguishing Features
- Neck pain, dermatomal radiation, sensory change, reflex changes
- Discriminating Test/Imaging
- Spurling test positive; normal shoulder exam; MRI cervical spine
- Key Distinguishing Features
- Isolated infraspinatus/supraspinatus weakness and wasting without tendon tear
- Discriminating Test/Imaging
- EMG/nerve conduction; MRI may show spinoglenoid/suprascapular ganglion cyst
- Key Distinguishing Features
- Acute severe pain, often self-limiting, may mimic tear
- Discriminating Test/Imaging
- Radiographs/ultrasound show calcific deposit in tendon
Investigations
Imaging Protocol for Suspected Rotator Cuff Tear
Standard shoulder series: AP (3 views - neutral, internal rotation, external rotation), scapular Y, axillary lateral
What to assess:
- Acromiohumeral distance (normal greater than 7mm, less than 7mm suggests massive tear)
- Acromial morphology (Type I flat, II curved, III hooked - Bigliani)
- Os acromiale (unfused acromial apophysis)
- Greater tuberosity cysts, sclerosis, osteophytes
- Glenohumeral arthritis, acromioclavicular arthritis
- Superior migration of humeral head (chronic massive tear)
MRI is the gold standard for rotator cuff assessment
Sensitivity/Specificity: Greater than 90% for full-thickness tears
What MRI shows:
- Tear presence, size (anteroposterior and mediolateral), location
- Partial vs full-thickness, articular vs bursal side
- Tendon retraction (Patte staging 1-3)
- Muscle atrophy (tangent sign on sagittal view)
- Fatty infiltration (Goutallier grading 0-4)
- Associated pathology (labral tears, biceps pathology, bone marrow edema)
Operator-dependent but useful in experienced hands
- Dynamic assessment, lower cost than MRI
- Good for full-thickness tears (sensitivity 90%)
- Less accurate for partial tears, muscle quality
- Useful for guided injections
Less commonly used, but helpful in specific scenarios
- Cannot have MRI (pacemaker, metallic implants)
- Assessment of bone quality (revision surgery, arthroplasty planning)
- Goutallier grading of fatty infiltration possible
Imaging Examples


Key MRI findings that predict poor repair outcomes:
- Goutallier Grade 3-4 fatty infiltration (more fat than muscle)
- Patte Stage 3 retraction (medial to glenoid)
- Positive tangent sign (muscle belly below superior glenoid line)
- Massive tear size (greater than 5cm or 2 tendons)
- Acromiohumeral distance less than 7mm (chronic massive tear with superior migration)

Management Algorithm
Non-Operative Treatment
Indications:
- Elderly, low-demand patients
- Asymptomatic or minimally symptomatic tears
- Massive tears with Goutallier 3-4 (poor repair prognosis)
- Medical comorbidities precluding surgery
- Patient preference
Conservative Treatment Steps
- Avoid painful overhead activities
- Modify work and sport activities
- Ergonomic adjustments
- Scapular stabilization: Strengthen periscapular muscles
- Deltoid strengthening: Compensate for cuff weakness
- Stretching: Maintain or improve passive range of motion
- Posterior capsule: Address tightness contributing to superior migration
- NSAIDs: Reduce inflammation and pain
- Analgesics: Paracetamol for pain control
- Subacromial corticosteroid injection: Reduce pain and inflammation
- Limit to 3 injections per year (tendon weakening risk)
- May provide temporary relief but does not heal tear
40% of rotator cuff tears increase in size within 2 years of conservative management. Muscle atrophy and fatty infiltration also progress and are largely irreversible. Delaying surgery may worsen repairability. In young, active patients with symptomatic tears, consider early surgery.
Management Algorithm

Surgical Technique
Single-Row Repair Technique
Indications: Small to medium tears (less than 3cm), good tissue quality
Pre-operative Planning:
- Re-tear: 10-30% depending on tear size and quality
- Stiffness: 5-10% risk, may require manipulation
- Infection: Less than 1% arthroscopic
- Nerve injury: Axillary nerve at risk (rare)
- Failure to heal: May require revision or alternative treatment
- Arthroscope: 30-degree and 70-degree
- Anchors: Suture anchors (typically 2-4 for small-medium tear)
- Suture: High-strength non-absorbable (FiberWire, MaxBraid)
- Instruments: Graspers, suture retrievers, knot pushers
- Radiofrequency device: For debridement, hemostasis
Patient Positioning
Beach chair position (most common) or lateral decubitus:
Beach Chair Setup
Beach chair at 60-70 degrees upright
- Head secured in headrest with neutral position
- Arm free-draped to allow full range of motion
- Arm holder or assistant to position limb
- Bony prominences: Pad sacrum, heels, contralateral elbow
- Blood pressure: Monitor on contralateral arm
- Hypotensive anesthesia: Consider to reduce bleeding (MAP 55-65)
- Mark bony landmarks: acromion, clavicle, coracoid, AC joint
- Plan portal sites: posterior, lateral, anterior
Surgical Steps
Arthroscopic Repair Steps
Posterior portal (standard viewing portal)
- Glenohumeral joint: Assess cartilage, labrum, biceps, subscapularis
- Identify tear location, size, mobility
- Assess articular-side partial tears
Subacromial space visualization
- Lateral portal for instrument access
- Bursectomy to visualize cuff tear
- Acromioplasty if Type II or III acromion
- Avoid aggressive acromioplasty (weakens deltoid origin)
Prepare tendon for repair
- Release adhesions (interval slide for anterior-posterior mobility)
- Debride frayed edges (minimal debridement to preserve tissue)
- Prepare footprint on greater tuberosity (remove soft tissue, light decortication)
Single-row medial anchors
- Place anchors at articular margin (medial footprint)
- Spacing: 1-1.5cm apart, typically 2-4 anchors depending on tear size
- 45-degree deadman angle for optimal pull-out strength
Pass sutures through tendon
- Suture passer through tear, retrieve anchor suture
- Horizontal mattress configuration for strength
- Ensure adequate tissue bites (5-8mm from edge)
- Consider medial-lateral or side-to-side sutures if large gap
Secure repair
- Tie sliding or non-sliding knots (surgeon preference)
- Assess repair integrity, tension, footprint coverage
- Check range of motion (should achieve 140deg forward flexion without undue tension)
Single-row repair restores partial footprint contact but may have higher re-tear rates for larger tears compared to double-row. The tendon is fixed to the medial edge of the footprint only. For medium to large tears, double-row provides better biomechanical strength and footprint restoration.
Biological Augmentation of the Repair
A rotator cuff repair is fundamentally a tendon-to-bone (enthesis) healing problem: the repaired interface heals with disorganised fibrovascular scar rather than a true graduated enthesis, which is why re-tear remains the commonest complication even with mechanically strong constructs. Strategies to augment the biology of healing - distinct from the construct itself - aim to lower the re-tear rate.
- Mechanism
- Multiple bone vents in the greater-tuberosity footprint release marrow stem cells and growth factors, forming a vascular clot over the footprint (the 'crimson duvet')
- Evidence / role
- Low-cost, low-risk; some studies show improved healing, particularly in larger tears
- Mechanism
- Autologous platelet concentrate delivering growth factors at the repair site
- Evidence / role
- Mixed evidence - at best a modest reduction in re-tear for small/medium tears with little functional gain; not a routine recommendation
- Mechanism
- Dermal allograft or biologic/synthetic patch laid over and reinforcing an intact but at-risk repair
- Evidence / role
- Reduces re-tear in selected larger repairs; distinct from bridging grafts or superior capsular reconstruction used for irreparable defects
- Mechanism
- Smoking cessation, diabetes control, avoiding NSAIDs in the early healing window
- Evidence / role
- The cheapest and most reliable lever on healing; optimise before elective repair
A rotator cuff repair fails at the tendon-to-bone interface, which heals as disorganised fibrovascular scar rather than a true enthesis - this is why re-tear is the commonest complication despite strong constructs. Biological augmentation targets that healing: footprint marrow-stimulation vents (the 'crimson duvet') recruit marrow stem cells over the footprint; PRP has mixed evidence and is not routine; an on-lay dermal or biologic patch reinforces an intact but at-risk repair and lowers re-tear in selected larger tears - this is distinct from the bridging grafts or superior capsular reconstruction used for irreparable tears. The cheapest, most reliable biological lever remains optimising the patient: stop smoking, control diabetes, and avoid NSAIDs during early healing.
Complications
- Incidence
- 10-30% (size-dependent)
- Risk Factors
- Large tears, poor tissue quality, Goutallier 3-4, age over 65
- Management
- Revision repair, SCR, or arthroplasty
- Incidence
- 5-10%
- Risk Factors
- Pre-existing stiffness, diabetes, prolonged immobilization
- Management
- Aggressive PT, manipulation under anesthesia
- Incidence
- Less than 1% arthroscopic
- Risk Factors
- Diabetes, immunosuppression, revision surgery
- Management
- Antibiotics, irrigation/debridement, anchor removal
- Incidence
- 1-2%
- Risk Factors
- Aggressive acromioplasty, nerve injury
- Management
- Observation, nerve recovery, physio
- Incidence
- Less than 1%
- Risk Factors
- Traction, retractor placement, anchor misplacement
- Management
- Observation (most recover), nerve exploration if no recovery
- Incidence
- 1-3%
- Risk Factors
- Poor bone quality, osteoporosis, incorrect angle
- Management
- Revision with larger anchors or different location
Re-tear - Most Common Complication:
Factors predicting rotator cuff re-tear:
- Tear size: Small (10%), medium (15%), large (20%), massive (30-40%)
- Fatty infiltration: Goutallier 3-4 dramatically increases re-tear
- Age: Over 65 years higher risk
- Smoking: Impairs healing, doubles re-tear rate
- Diabetes: Poor tissue quality, delayed healing
- Repair technique: Single-row higher re-tear than double-row for medium-large tears
Despite re-tear, many patients remain clinically improved with reduced pain even if MRI shows persistent defect.
Stiffness Prevention:
- Early passive range of motion (start within first week)
- Progress to active-assisted motion at 6 weeks
- Avoid prolonged immobilization
- Diabetic patients at highest risk - aggressive PT protocol
Assessing Repair Integrity and Patterns of Re-tear
Because re-tear is the dominant complication, it is worth knowing how repair integrity is graded and where repairs fail. Postoperative MRI (or ultrasound) integrity is described by the Sugaya classification, and the anatomical pattern of failure by the Cho classification.
- MRI appearance
- Sufficient thickness, homogeneously low signal
- Interpretation
- Intact, healed
- MRI appearance
- Sufficient thickness, partial high signal
- Interpretation
- Intact but some abnormal signal
- MRI appearance
- Insufficient thickness (less than half expected) without discontinuity
- Interpretation
- Thinned but continuous
- MRI appearance
- Minor discontinuity (one or two slices)
- Interpretation
- Small full-thickness re-tear
- MRI appearance
- Major discontinuity (more than two slices)
- Interpretation
- Medium-to-large re-tear
Types I-II are regarded as intact, type III as thinned but continuous, and types IV-V as re-tear.
The PATTERN of re-tear (Cho classification) is as important as its presence. Type 1 is failure at the tendon-bone interface - the tendon pulls off the lateral footprint. Type 2 is failure at the musculotendinous junction MEDIAL to the medial-row anchors ('medial cuff failure'). Type 2 is characteristic of knotless suture-bridge (transosseous-equivalent) double-row constructs: a very strong, over-tensioned medial row concentrates stress and strangulates the tendon, which then tears medial to it. This is the biomechanical reason for the warning against over-tensioning the medial row - and it guides revision, because the medial stump in a type 2 failure is often of poor quality.
Postoperative Care and Rehabilitation
Standard Rehabilitation Timeline
Goals: Protect repair, prevent stiffness, minimize pain
- Sling: Wear at all times except for exercises and hygiene (4-6 weeks)
- Passive ROM: Start within first week, pendulums, table slides
- Forward flexion passive: Progress to 140 degrees by 6 weeks
- External rotation passive: Progress to 30-40 degrees by 6 weeks
- No active motion: Avoid activating repaired tendons
- Cryotherapy and pain control: Ice, analgesics, minimize NSAIDs (may impair healing)
Goals: Transition to active motion, gentle strengthening
- Discontinue sling at 6 weeks
- Active-assisted ROM: Pulley exercises, wand exercises
- Progress to active ROM: Deltoid-initiated elevation, avoid substitution patterns
- Begin gentle isometrics: Sub-maximal contractions, avoid pain
- Scapular stabilization: Periscapular muscle activation
Goals: Restore strength and function
- Progressive resistance exercises: Light weights progressing to heavier
- Rotator cuff strengthening: Resistance band exercises (IR, ER, abduction)
- Functional activities: Return to daily activities, work
- Sport-specific training: Gradual return to overhead sports (6 months minimum)
Goals: Full strength and function
- Most patients achieve maximal improvement by 12 months
- Continued home exercise program for maintenance
- Return to full sport/work as tolerated
Outcomes and Prognosis
Outcomes by Tear Size:
- Healing Rate
- 90-95%
- Functional Outcome
- Excellent
- Notes
- Most reliable results
- Healing Rate
- 80-90%
- Functional Outcome
- Good to excellent
- Notes
- Double-row improves healing
- Healing Rate
- 60-80%
- Functional Outcome
- Good
- Notes
- Healing less predictable, longer rehab
- Healing Rate
- 30-60%
- Functional Outcome
- Fair to good
- Notes
- Even with re-tear, pain often improved
- Younger age (less than 60 years)
- Acute traumatic tear (as opposed to chronic degenerative)
- Small to medium tear size
- Good tissue quality (Goutallier 0-1)
- Minimal retraction (Patte 1-2)
- Non-smoker
- Compliant with rehabilitation
- Advanced age (over 70)
- Massive tear
- Chronic tear (greater than 6 months)
- Goutallier Grade 3-4 fatty infiltration
- Patte Stage 3 retraction
- Smoking, diabetes, worker's compensation
- Poor patient compliance
Important distinction: Structural healing (tendon heals on MRI) does not always correlate with clinical outcome (pain and function). Many patients with re-tears on imaging have good clinical outcomes with improved pain and function compared to pre-operative state. The goal is a satisfactory clinical result, not necessarily perfect anatomic healing.
Guidelines, Registries & Global Practice
Global Epidemiology
- Population ultrasound prevalence of full-thickness tears approximately 20% overall, rising steeply with age (Yamamoto, Japan)
- Tears in 16.9% of asymptomatic and 36% of symptomatic individuals - many tears are clinically silent
- Prevalence increases markedly beyond the sixth decade across all studied populations
- Independent risk factors: increasing age, history of trauma, and dominant arm involvement
- Higher rates in heavy manual and repetitive overhead work; smoking and diabetes impair tendon quality and healing
- Ageing populations worldwide are driving a rising burden of degenerative tears and cuff-tear arthropathy
According to PubMed, the population prevalence figures above are from Yamamoto et al (DOI).
Major Guidelines - Side by Side
- Position on Non-operative Care
- Structured exercise reasonable first-line for many tears
- Position on Surgery
- Repair appropriate for symptomatic full-thickness tears failing non-operative care; routine acromioplasty not required
- Evidence Strength
- Mostly moderate/limited - few strong recommendations
- Position on Non-operative Care
- Time-limited physiotherapy trial for atraumatic/degenerative tears
- Position on Surgery
- Early referral and repair for acute traumatic tears in suitable patients
- Evidence Strength
- Consensus-based national pathway
- Position on Non-operative Care
- Conservative care and physiotherapy as initial management
- Position on Surgery
- Surgery reserved for persistent symptoms after appropriate non-operative care
- Evidence Strength
- Pragmatic, resource-aware guidance
- Position on Non-operative Care
- Non-operative care for degenerative tears, especially low-demand patients
- Position on Surgery
- Earlier repair favoured in young/active and acute traumatic tears to limit irreversible change
- Evidence Strength
- Expert consensus and cohort evidence
The strongest cross-guideline agreement is that acute traumatic tears in active patients warrant early repair, while degenerative/atraumatic tears merit a structured physiotherapy trial first - supported by the MOON cohort showing roughly 75% avoid surgery (Kuhn et al, DOI). Practice variation is greatest around the value of routine acromioplasty and the role of superior capsular reconstruction.
Registry and High-Level Evidence
- Rotator cuff repair is a soft-tissue procedure and is not captured by the major arthroplasty joint registries (NJR, AJRR, AOANJRR, SHAR). The evidence base therefore rests on RCTs and meta-analyses (e.g. single- vs double-row, DOI) and large prospective cohorts (MOON).
- Reverse total shoulder arthroplasty for cuff-tear arthropathy is registry-tracked: national arthroplasty registries (NJR, AOANJRR, AJRR, Nordic registries) report rising reverse-TSA volumes and implant survival, complementing survivorship series such as Guery et al (DOI).
Global Practice Variation
- Arthroscopic repair is standard; MRI used routinely for staging
- Ready access to reverse TSA and graft augmentation (SCR, dermal allograft)
- Earlier surgical intervention in active patients
- Ultrasound often the primary imaging modality (lower cost, dynamic)
- Open or mini-open repair more common where arthroscopic expertise/equipment is limited
- Greater reliance on physiotherapy and longer non-operative trials
Consent and Documentation (Universal)
Applicable to any health system, informed consent for rotator cuff repair should cover:
- Re-tear risk (10-30%, size-dependent), and that re-tear does not always mean symptomatic failure
- Stiffness (5-10%, higher in diabetics), infection (under 1% arthroscopic), nerve injury and anchor complications
- Prolonged recovery (6-12 months to maximal improvement; longer for large/massive tears)
- Possibility of failed repair requiring revision, SCR or arthroplasty
- Documented trial and failure of appropriate non-operative care, and pre-operative staging of tear size, retraction and muscle quality (Goutallier)
MCQ Practice Points
Q: Which rotator cuff muscle is NOT innervated by the suprascapular nerve? A: Teres minor (innervated by axillary nerve). Supraspinatus and infraspinatus are both innervated by the suprascapular nerve (C5-6). Subscapularis is innervated by upper and lower subscapular nerves (C5-7).
Q: What is the critical zone of the rotator cuff and why is it significant? A: The critical zone is a hypovascular area approximately 1cm medial to the supraspinatus insertion. It represents a watershed zone between the osseous blood supply (humeral circumflex arteries) and muscular blood supply (suprascapular artery). This area is particularly prone to degeneration and tear formation.
Q: A rotator cuff tear measuring 4cm with Goutallier Grade 3 fatty infiltration and Patte Stage 3 retraction - what is the prognosis for repair? A: Poor prognosis. This is a large tear (3-5cm by Cofield) with unfavorable prognostic factors: Goutallier Grade 3 (more fat than muscle) predicts poor healing, and Patte Stage 3 retraction (medial to glenoid) makes repair technically difficult. This tear may be irreparable and alternative treatments (partial repair, SCR, reverse TSA) should be considered.
Q: What does a positive external rotation lag sign indicate? A: An external rotation lag sign (arm drops more than 10 degrees when released from passive external rotation) indicates a posterosuperior rotator cuff tear involving infraspinatus and possibly teres minor. It is highly specific for a significant tear and suggests the need for surgical intervention.
Q: What is the biomechanical advantage of double-row repair over single-row repair for medium to large rotator cuff tears? A: Double-row repair provides: (1) Increased footprint contact area - better anatomic restoration, (2) Higher ultimate load to failure - stronger construct, (3) Better pressure distribution across repair site, (4) Lower re-tear rates for medium-large tears compared to single-row. However, clinical outcome scores are similar between techniques.
Q: A patient has a confirmed rotator cuff re-tear on MRI at 1 year post-repair but reports good pain relief and improved function. What is your management? A: No further surgery. This demonstrates that structural healing (MRI) does not always correlate with clinical outcome. Many patients with re-tears have good clinical outcomes with improved pain and function. If the patient is satisfied and functional, no additional intervention is needed. Surgery would only be considered for symptomatic re-tear with significant pain or functional impairment.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old recreational golfer presents with 12 months of progressive right shoulder pain and weakness. He has failed physiotherapy and a subacromial steroid injection. On examination, he has full passive range of motion, painful arc 60-120 degrees, positive empty can test, and external rotation lag sign of 15 degrees. MRI shows a full-thickness supraspinatus tear measuring 2.5cm with minimal retraction and Goutallier Grade 1 fatty infiltration of supraspinatus and infraspinatus. What is your assessment and management?”
“A 55-year-old manual laborer presents with severe right shoulder pain and inability to lift his arm. He fell off a ladder 6 months ago but delayed seeking treatment. Examination shows pseudoparalysis - he cannot actively elevate beyond 40 degrees but has full passive forward flexion. External rotation lag is 30 degrees. MRI shows a massive retracted tear of supraspinatus and infraspinatus (5.5cm), Patte Stage 3 retraction medial to the glenoid, Goutallier Grade 3 fatty infiltration, and positive tangent sign. Acromiohumeral distance is 4mm. How would you manage this patient?”
“A 68-year-old diabetic woman underwent arthroscopic rotator cuff repair for a medium-sized tear 3 months ago. She returns to clinic with severe stiffness - active forward flexion is 60 degrees and passive forward flexion is 90 degrees. She reports shoulder pain at rest and with movement. She has been compliant with physiotherapy. How do you assess and manage this complication?”
Key Anatomy - SITS
- Supraspinatus: Superior cuff, initiates abduction, most commonly torn (suprascapular nerve C5-6)
- Infraspinatus: Posterior cuff, external rotation (suprascapular nerve C5-6)
- Teres minor: Posterior-inferior cuff, external rotation (axillary nerve C5-6)
- Subscapularis: Anterior cuff, internal rotation (upper/lower subscapular nerves C5-7)
- Critical zone: Hypovascular area 1cm medial to insertion - prone to degeneration
Classification Systems
- Cofield by size: Small (less than 1cm), Medium (1-3cm), Large (3-5cm), Massive (greater than 5cm or 2 tendons)
- Goutallier fatty infiltration: Grade 0 (normal) to Grade 4 (severe fat) - Grade 3-4 predicts poor repair
- Patte retraction: Stage 1 (near tuberosity), Stage 2 (glenoid rim), Stage 3 (medial to glenoid)
- Tangent sign: Muscle belly below superior glenoid line on sagittal MRI indicates severe atrophy
Clinical Assessment
- Empty can test: Supraspinatus (arm 90deg abducted, 30deg forward, thumb down)
- External rotation lag sign: Infraspinatus (drop greater than 10 degrees when released from ER)
- Belly-press, lift-off, bear-hug tests: Subscapularis tears
- Pseudoparalysis: Cannot actively elevate but full passive motion (massive tear)
Surgical Techniques
- Single-row repair: Medial anchors only, suitable for small tears
- Double-row repair: Medial and lateral rows, better for medium-large tears (improved footprint, lower re-tear)
- Margin convergence: Side-to-side sutures for large U-shaped tears before bone fixation
- Superior capsular reconstruction: Fascia lata graft for irreparable tears in young patients
- Reverse TSA: Gold standard for cuff arthropathy with pseudoparalysis in elderly
Complications and Outcomes
- Re-tear: 10-30% (size-dependent) - many asymptomatic, good clinical outcomes despite re-tear
- Stiffness: 5-10%, higher in diabetics - early mobilization, aggressive PT, consider MUA
- Prognostic factors: Tear size, Goutallier grade, Patte stage, age, smoking, diabetes
- Rehabilitation: Passive immediate, active-assisted 6 weeks, strengthening 12 weeks, maximal improvement 12-24 months
Key Evidence and Pearls
- Double-row reduces re-tear for medium-large tears but similar clinical outcomes to single-row
- Tears progress in size (40% enlarge in 2 years) and fatty change (irreversible)
- Goutallier 3-4 and Patte 3 indicate irreparable tear - consider SCR or reverse TSA
- Force couple concept: RC compresses humeral head, deltoid elevates - disruption causes superior migration
- Asymptomatic tears common (50% over age 60) - treat symptoms, not imaging
Evidence Base and Key Trials
Single-Row vs Double-Row Repair - Systematic Review and Meta-Analysis
- Systematic review and meta-analysis including 6 Level I RCTs of single-row versus double-row repair
- Odds of an intact (healed) tendon were significantly higher with double-row repair (OR 1.93)
- No clinically significant difference in Constant, UCLA or ASES scores between techniques
- Structural benefit of double-row was concentrated in tears greater than 3cm (large/massive)
Natural History of Asymptomatic Rotator Cuff Tears
- Longitudinal sonographic study of patients with a contralateral asymptomatic rotator cuff tear
- 51% (23/45) of initially asymptomatic tears became symptomatic over a mean of 2.8 years
- Onset of symptoms was associated with a significant rise in pain and fall in ADL scores
- 9 of 23 re-imaged shoulders showed tear enlargement; no tear ever decreased in size
MOON Shoulder Group - Physical Therapy for Atraumatic Cuff Tears
- Multicentre prospective cohort of 452 patients with atraumatic full-thickness tears on a structured physiotherapy programme
- Patient-reported outcomes improved significantly at 6 and 12 weeks
- Fewer than 25% elected surgery; most who converted did so between 6 and 12 weeks
- Approximately 75% avoided surgery at 2-year follow-up
Superior Capsular Reconstruction for Irreparable Tears (Original Series)
- Original clinical series: 24 shoulders in 23 patients (mean age 65) with irreparable tears, arthroscopic SCR using fascia lata autograft
- Active elevation improved from 84 to 148 degrees and external rotation from 26 to 40 degrees
- Acromiohumeral distance restored from 4.6mm to 8.7mm (reversed superior migration)
- 83.3% had no graft or tendon retear; ASES score improved from 23.5 to 92.9
Reverse Total Shoulder Arthroplasty - Survivorship Analysis
- Multicentre survivorship study of 80 reverse total shoulder replacements followed 5 to 10 years
- Implant survival 91% at 120 months (endpoint: prosthesis replacement); 84% for glenoid loosening
- Shoulders with cuff-tear arthropathy survived significantly better than other aetiologies
- Functional survival (Constant score under 30 as endpoint) fell to 58% at 120 months, with deterioration after 6 years
Prevalence and Risk Factors in the General Population
- Population-based ultrasound survey of 1,366 shoulders (683 residents) in a Japanese village
- Full-thickness rotator cuff tears present in 20.7% overall, with prevalence rising steeply with age
- Tears found in 36% of symptomatic but also 16.9% of asymptomatic individuals
- Independent risk factors on regression: history of trauma, dominant arm and increasing age