Retrograde Blood Supply | AVN Risk | Vascularized Bone Graft | SNAC Progression
- Retrograde blood supply - proximal pole at highest AVN risk (80% from dorsal scaphoid branch)
- Humpback deformity - flexion through nonunion site creates dorsal angulation
- DISI pattern develops - lunate extends as scaphoid flexes (carpal collapse)
- 100% progress to SNAC wrist if untreated - arthritis is inevitable
- VBG (1,2 ICSRA) indicated for AVN or failed previous fixation
- “Lateral intrascaphoid angle greater than 45 degrees = significant humpback requiring wedge graft
- “MRI with gadolinium assesses AVN - lack of enhancement means AVN, requires VBG
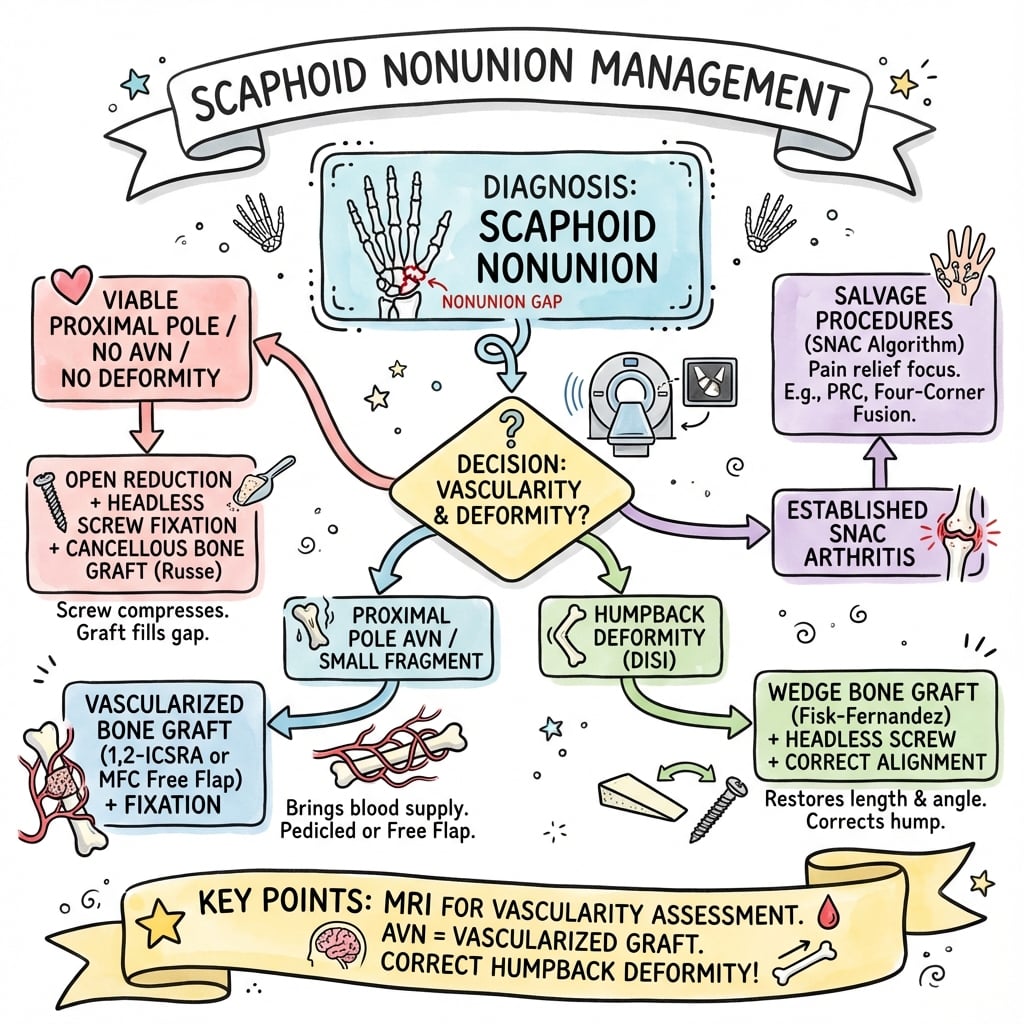
- “Non-vascularized graft if viable proximal pole, VBG if AVN or failed surgery
- “Union rates: 90-95% non-VBG viable bone, 80-90% VBG for AVN
Nonunion allows flexion through fracture site creating dorsal angulation (convex dorsally like a humpback). Lateral intrascaphoid angle greater than 45 degrees is significant. Must correct with wedge graft for union.
MRI with gadolinium is gold standard - lack of proximal pole enhancement indicates AVN. Intraoperative punctate bleeding confirms vascularity. AVN requires vascularized bone graft.
1,2 Intercompartmental Supraretinacular Artery pedicled graft from dorsal distal radius. Gold standard for AVN nonunion. Described by Zaidemberg 1991.
Untreated nonunion = 100% SNAC wrist. Arthritis progresses: Stage 1 radial styloid, Stage 2 scaphocapitate, Stage 3 capitolunate, Stage 4 pancarpal.
- Assessment
- Minimal motion at nonunion
- Treatment
- ORIF alone may suffice
- Graft Type
- Cancellous graft if needed
- Assessment
- Mobile nonunion, viable bone
- Treatment
- ORIF + bone graft
- Graft Type
- Iliac crest cancellous
- Assessment
- ISA greater than 45 degrees, MRI signal intact
- Treatment
- Correct deformity + fix
- Graft Type
- Corticocancellous wedge
- Assessment
- No MRI enhancement, no intraop bleeding
- Treatment
- Vascularized bone graft
- Graft Type
- 1,2 ICSRA pedicled graft
- Assessment
- Prior nonunion repair failed
- Treatment
- Revision with VBG
- Graft Type
- Free vascularized MFC graft
RSC-PSNAC Wrist Stages
Hook:SNAC progresses RSC-P: Radial styloid first, then Scaphocapitate, Capitolunate, finally Pancarpal!
Overview and Epidemiology
Scaphoid nonunion is failure of a scaphoid fracture to heal, typically defined as absence of radiographic union at 6 months despite treatment, or presence of an established nonunion pattern.
- 5-15% of all scaphoid fractures progress to nonunion
- Higher rates in:
- Proximal pole fractures (up to 30%)
- Displaced fractures (greater than 1mm)
- Delayed presentation (greater than 4 weeks)
- Missed diagnosis
- Smokers (2-3x increased risk)
- Proximal pole location - poor blood supply
- Displacement greater than 1mm
- Delayed treatment greater than 4 weeks
- Smoking - major modifiable factor
- NSAID use - inhibits healing
- Initial AVN
- Poor immobilization compliance
- 100% progress to SNAC wrist if untreated
- Mean time to symptomatic SNAC: 5-10 years
- Even asymptomatic nonunions deteriorate
- Mack et al: 97% radioscaphoid arthritis within 10 years
- Young patients especially vulnerable
Key exam point: Unlike other nonunions where the question is "will it cause problems?", scaphoid nonunion has a 100% certainty of progression to SNAC wrist arthritis. Treatment is almost always indicated.
Scaphoid nonunion in the skeletally immature child/adolescent behaves differently from the adult and is a distinct examinable scenario:
- Different fracture profile: paediatric scaphoid fractures are more often distal-third/avulsion (rather than waist) and are frequently missed/treated late, which is the main driver of the (uncommon) nonunion.
- Greater intrinsic healing: the child's robust periosteal vascularity and remodelling mean a trial of immobilisation (cast) can still unite an established nonunion in a way it rarely would in an adult, and AVN/SNAC are comparatively rare.
- Surgery when conservative fails: persistent nonunion is treated with debridement, bone grafting (usually non-vascularised distal radius/iliac crest) and fixation (screw or K-wires sized to the small bone), with high union rates (often over 90%) and good remodelling.
- Vascularised grafts are rarely needed because proximal pole AVN is uncommon in this group - reserve them for the rare avascular or revision case.
Exam point: in a child/adolescent with a "forgotten" scaphoid fracture and nonunion, the prognosis is better than in adults - consider a cast trial first, and grafting+fixation gives high union without usually needing a vascularised graft.
Anatomy and Blood Supply
Scaphoid Anatomy:
- Largest carpal bone in proximal row
- Spans both carpal rows (proximal and distal)
- 80% covered by articular cartilage - limits periosteal blood supply
- Acts as kinematic link between carpal rows
Blood Supply (Critical for Exam):
- Contribution
- 70-80%
- Entry Point
- Dorsal ridge at waist
- Area Supplied
- Majority of bone via retrograde flow
- Contribution
- 20-30%
- Entry Point
- Scaphoid tubercle
- Area Supplied
- Distal pole and tuberosity
- Contribution
- Variable (20%)
- Entry Point
- Variable
- Area Supplied
- Small portion proximal pole
Clinical Implications:
- Retrograde flow = proximal pole at highest AVN risk
- Waist fractures interrupt main blood supply to proximal pole
- Proximal pole fractures have highest nonunion rate (up to 30%)
- Only 20-30% of proximal pole has any direct blood supply
Proximal pole fractures have the highest nonunion and AVN rates (up to 30%) because they completely disrupt the retrograde blood supply from the main dorsal scaphoid branch. Always consider these high-risk injuries.
RETROScaphoid Blood Supply
Hook:Blood enters distally and runs RETRO (backwards) up the scaphoid - proximal pole is at highest risk!
Pathophysiology of Nonunion
Humpback Deformity:
The scaphoid normally acts as a strut connecting the proximal and distal carpal rows. When nonunion develops:
- Loss of structural integrity at nonunion site
- Flexion force from scaphotrapezial ligament pulls distal fragment into flexion
- Dorsal angulation develops at nonunion site
- Dorsal convexity creates "humpback" appearance
Measuring Humpback:
- Lateral intrascaphoid angle measured on lateral radiograph or sagittal CT
- Lines drawn along proximal and distal pole axes
- Normal: less than 35 degrees
- Significant humpback: greater than 45 degrees
- Must correct with wedge graft for successful union
DISI Pattern Development:
- Scaphoid links proximal and distal rows
- Flexion tendency balanced by lunate
- Lunate in neutral position
- Normal scapholunate angle: 30-60 degrees
- Scaphoid collapses into flexion
- Lunate (attached to proximal fragment) extends
- Dorsal intercalated segment instability (DISI)
- Scapholunate angle increases (greater than 60 degrees)
- Leads to abnormal load distribution
DISI pattern from scaphoid nonunion leads to abnormal carpal mechanics, altered load distribution, and ultimately SNAC wrist (Scaphoid Nonunion Advanced Collapse). This is the inevitable endpoint without treatment.
SNAPSNonunion Risk Factors
Hook:SNAPS cause nonunion - especially Smoking and proximal pole location!
Classification Systems
Herbert Nonunion Classification (Type D):
- Description
- Fibrous union
- Characteristics
- Minimal motion, may heal with prolonged immobilization
- Treatment
- ORIF, may not need graft
- Description
- Pseudarthrosis
- Characteristics
- Established nonunion, mobile but viable
- Treatment
- ORIF + bone graft
- Description
- Sclerotic
- Characteristics
- Dense sclerosis at nonunion margins
- Treatment
- Debride + extensive graft
- Description
- Avascular necrosis
- Characteristics
- No proximal pole vascularity
- Treatment
- Vascularized bone graft
Herbert D classification is the exam standard. D4 (AVN) is the critical type - requires vascularized bone graft. D1-D3 may be treated with non-vascularized graft if bone is viable.
Alongside the Herbert classification, the Slade-Geissler classification grades nonunion by the degree of healing/sclerosis seen arthroscopically and on CT, and it maps onto whether a percutaneous/arthroscopic approach is feasible or whether open structural grafting is required:
- Grades I-II (delayed union, fibrous union without sclerosis): minimal pathology - amenable to percutaneous headless compression screw fixation alone (no formal graft).
- Grades III-IV (progressive minimal-to-comprehensive sclerosis at the nonunion): arthroscopic-assisted debridement and bone grafting with percutaneous screw fixation can achieve union while avoiding an open approach and preserving blood supply.
- Grades V-VI (cyst formation/resorption, then wide gap with humpback/carpal collapse): the deformity and bone loss demand open reduction with a structural (wedge) graft - and an avascular proximal pole demands a vascularised graft.
Why it matters: arthroscopic-assisted grafting is soft-tissue-sparing and protects the dorsal blood supply, with union rates comparable to open surgery in selected (lower-grade, non-humpback, vascular) nonunions - but it is not appropriate where humpback deformity must be corrected. The Slade-Geissler grade is the practical tool for deciding percutaneous-vs-arthroscopic-vs-open.
Clinical Assessment
History:
- Often delayed presentation with chronic wrist pain
- May have history of wrist injury (sometimes remote, forgotten)
- Pain with gripping, loading wrist
- Weakness, reduced grip strength
- Decreased range of motion
Physical Examination:
- Swelling often minimal in chronic cases
- Dorsal wrist fullness may be present
- Compare with contralateral side
- Assess overall wrist posture
- Anatomical snuffbox tenderness
- Scaphoid tubercle tenderness (volar)
- Dorsal scaphoid tenderness
- Check for crepitus
- Scaphoid shift test (Watson test): Painful clunk with radial deviation
- Thumb compression: Pain with axial load through thumb
- Grip strength: Compare to contralateral side
- Decreased wrist flexion/extension
- Decreased radial deviation
- May have relatively preserved ulnar deviation
Many scaphoid nonunions are "forgotten fractures" - patients may not recall injury. Always have high index of suspicion for nonunion in chronic wrist pain with snuffbox tenderness.
Differential Diagnosis of Radial-Sided Wrist Pain
- Key features
- Snuffbox tenderness, prior injury (often forgotten), reduced grip
- Distinguishing finding
- CT shows nonunion gap/sclerosis; MRI assesses proximal pole AVN
- Key features
- Recent fall on outstretched hand, snuffbox tenderness
- Distinguishing finding
- Fracture line without sclerosis; MRI positive within days
- Key features
- Dorsal SL tenderness, positive Watson scaphoid shift
- Distinguishing finding
- Widened SL interval (Terry Thomas sign), no scaphoid fracture line
- Key features
- Insidious radial wrist pain, no fracture history
- Distinguishing finding
- MRI AVN of intact (non-fractured) scaphoid
- Key features
- Pain over 1st dorsal compartment, positive Finkelstein
- Distinguishing finding
- Tenderness/swelling over APL-EPB, normal scaphoid imaging
- Key features
- Pain at thumb base, positive CMC grind
- Distinguishing finding
- Trapeziometacarpal joint changes, not scaphoid
- Key features
- Tenderness more proximal/dorsal, crepitus
- Distinguishing finding
- Soft-tissue, normal bony scaphoid imaging
Investigations
Plain Radiographs:
- Assessment
- Overall alignment, DISI
- Key Findings
- Signet ring sign, widened SL interval
- Assessment
- Humpback measurement, DISI
- Key Findings
- Intrascaphoid angle, SL angle greater than 60 degrees
- Assessment
- Nonunion site detail
- Key Findings
- Gap, sclerosis, cystic changes
- Assessment
- Scaphoid length
- Key Findings
- Additional nonunion detail
X-ray Findings in Nonunion:
- Gap at fracture site
- Sclerotic margins
- Cystic changes
- Bone resorption
- Humpback deformity on lateral
- DISI pattern (scapholunate angle greater than 60 degrees)
- SNAC changes if advanced
- Gold standard for assessing bony union/nonunion
- Sagittal reconstructions for humpback measurement
- Identifies cystic changes, sclerosis
- Essential for surgical planning
- Assesses arthritic changes (SNAC staging)
- Essential for AVN assessment - determines graft choice
- T1 sequences show marrow signal
- Gadolinium enhancement confirms vascularity
- No proximal pole enhancement = AVN = VBG required
MRI with gadolinium is mandatory before scaphoid nonunion surgery to assess proximal pole vascularity. Lack of enhancement indicates AVN and mandates vascularized bone graft. Non-vascularized graft in AVN has high failure rate.
Bone Scan:
- Less commonly used now
- Decreased uptake suggests AVN
- Non-specific

Management Algorithm
Management Decision Tree
- Achieve union - primary goal
- Restore anatomy - correct humpback, length
- Prevent SNAC progression - all nonunions lead to arthritis
- Maintain/restore function - motion, grip strength
- History and examination - symptom duration, prior treatment
- Plain radiographs (4 views) - confirm nonunion
- CT scan - nonunion detail, bone quality
- MRI with gadolinium - AVN assessment (critical)
- Check for SNAC changes - determines if salvage needed
- Herbert D type (D1-D4)
- Location (proximal/waist/distal)
- SNAC stage if arthritis present
- Degree of humpback (ISA measurement)
Complete assessment guides appropriate treatment selection.
Bone Graft Selection
Indications:
- Viable proximal pole (MRI enhancement, intraop bleeding)
- Herbert D1, D2, D3 with vascularity
- Primary nonunion surgery
Types:
- Source
- Distal radius, iliac crest
- Indication
- Minimal deformity, fill defect
- Source
- Iliac crest
- Indication
- Moderate defect, some stability
- Source
- Iliac crest
- Indication
- Humpback correction
- Source
- Iliac crest
- Indication
- Classic corticocancellous inlay
- Debride sclerotic bone to punctate bleeding
- Size graft to correct deformity
- Pack cancellous around cortical strut
- Fix with headless compression screw
85-95% with appropriate patient selection
VIABLESGraft Selection Algorithm
Hook:Is the bone VIABLE? Use this checklist to decide if patient needs VBG or non-vascularized graft!
Surgical Technique
Modified Russe Volar Approach
- Waist nonunions
- Humpback deformity requiring correction
- Non-vascularized bone graft
-
Incision: Longitudinal over scaphoid tubercle, between FCR and radial artery. Protect palmar cutaneous branch of median nerve.
-
Exposure: Incise joint capsule, identify nonunion site. Wrist flexion improves access.
-
Debridement: Remove fibrous tissue, debride sclerotic bone margins. Continue until punctate bleeding seen. Preserve periosteum where possible.
-
Graft Insertion: Size wedge graft to correct humpback. Insert graft into prepared slot. Pack cancellous around. Confirm correction on fluoroscopy.
-
Fixation: Headless compression screw (Acutrak, Herbert). Guidewire placement checked fluoroscopically. Screw should cross nonunion and engage proximal pole.
The volar approach provides excellent access for waist nonunions and humpback correction.
Complications
- Incidence
- 5-20%
- Prevention
- Appropriate graft selection, technique
- Management
- Revision with VBG if AVN
- Incidence
- Variable
- Prevention
- VBG for at-risk cases
- Management
- Free vascularized graft
- Incidence
- If nonunion persists
- Prevention
- Achieve union
- Management
- Salvage procedure
- Incidence
- 10-20%
- Prevention
- Early motion when healed
- Management
- Physiotherapy
- Incidence
- 5-10%
- Prevention
- Appropriate screw sizing
- Management
- Hardware removal if symptomatic
- Incidence
- 5-10%
- Prevention
- Minimize graft size
- Management
- Symptomatic treatment
- Incidence
- less than 2%
- Prevention
- Sterile technique, prophylaxis
- Management
- Antibiotics, debridement
- Identify cause (inadequate graft, AVN, poor fixation, smoking)
- Address modifiable factors
- Revision with vascularized graft if non-VBG failed
- Consider free vascularized (MFC) if pedicled VBG failed
- If SNAC advanced, salvage procedures
- If arthritis too advanced for nonunion repair:
- Stage 1-2: Scaphoid excision + 4-corner fusion
- Stage 2-3: Proximal row carpectomy (if capitolunate preserved)
- Stage 3-4: Total wrist fusion or arthroplasty
Postoperative Care and Rehabilitation
Rehabilitation Protocol
- Thumb spica cast or splint
- Immobilize wrist and thumb IP joint
- Allow finger motion
- Serial radiographs at 4, 6, 8 weeks
- No loading, gripping
- CT scan at 8 weeks to assess union
- If signs of healing, transition to removable splint
- Gentle active ROM exercises
- Continue night splinting
- No resistance activities
- Progressive strengthening if union confirmed
- Grip exercises, putty
- Proprioception work
- Gradually increase resistance
- Return to manual work when pain-free, strong
- Contact sports delayed until 6 months
- Monitor for complications
CT Monitoring:
- Serial CT scans best for union assessment
- Bridging trabeculae indicate healing
- Complete bridging = union
- May take 12+ weeks for VBG cases
Union Rates by Graft Type:
- Indication
- D1-D3, no AVN
- Union Rate
- 85-95%
- Time to Union
- 8-12 weeks
- Indication
- Humpback correction
- Union Rate
- 85-95%
- Time to Union
- 10-14 weeks
- Indication
- D4, AVN
- Union Rate
- 80-90%
- Time to Union
- 12-16 weeks
- Indication
- Failed VBG
- Union Rate
- 70-85%
- Time to Union
- 14-20 weeks
Outcomes and Prognosis
- Vascularity - AVN has lower union rates
- Time from injury - chronic worse than acute
- Deformity correction - humpback must be addressed
- Graft choice - appropriate graft selection critical
- Smoking cessation - major modifiable factor
- Most patients achieve pain relief with union
- Grip strength 70-85% of contralateral
- Range of motion 70-85% of contralateral
- Return to work/sport in 4-6 months if union achieved
Exam key: Prognosis is excellent if union achieved - most patients return to normal function. The key is selecting the right graft (VBG for AVN) and correcting deformity (wedge graft for humpback).
Guidelines, Registries & Global Practice
Global Epidemiology
The scaphoid is the most commonly fractured carpal bone, and nonunion is the dominant late complication that drives carpal collapse and arthritis worldwide.
- Figure
- approximately 12.4 in 100,000 per year
- Source population
- UK regional cohort (Garala 2016)
- Figure
- Young men, highest aged 15-19 years
- Source population
- UK regional cohort (Garala 2016)
- Figure
- Waist 64%, tubercle 18.1%
- Source population
- UK regional cohort (Garala 2016)
- Figure
- approximately 5-15% (up to 30% proximal pole)
- Source population
- Pooled clinical series
- Figure
- approximately 27.9 years (87.8% male)
- Source population
- Systematic review, 7,671 patients (Duncumb 2022)
Incidence rises with social deprivation and shows summer seasonality, reflecting the high-energy sporting and occupational mechanisms typical of the young male population at risk (Garala 2016).
Guideline and Society Guidance, Side by Side
There is no single high-level (Level I) guideline dedicated to scaphoid nonunion; recommendations are drawn from society resources and pooled evidence, which broadly agree.
- Core guidance on scaphoid nonunion
- CT to confirm nonunion and assess deformity; debride to bleeding bone, restore length/alignment, structural graft plus stable internal fixation (headless compression screw)
- Evidence basis
- Expert consensus / surgical reference
- Core guidance on scaphoid nonunion
- Refer suspected nonunion to a hand unit; image with CT (union/deformity) and MRI (proximal pole viability); graft and fix; counsel that untreated nonunion risks collapse and arthritis
- Evidence basis
- Society best-practice / narrative
- Core guidance on scaphoid nonunion
- Operative reconstruction for symptomatic nonunion; vascularised graft considered for avascular proximal pole or failed prior surgery; salvage (4-corner fusion, PRC) once SNAC arthritis established
- Evidence basis
- Society resources / pooled series
- Core guidance on scaphoid nonunion
- Consistent with AO: address vascularity, deformity and stability; reserve vascularised grafts for avascular or revision cases
- Evidence basis
- Instructional / consensus
confirm nonunion and deformity on CT; assess proximal pole vascularity (MRI plus intra-operative bleeding); debride, correct humpback and stabilise; salvage rather than reconstruct once SNAC arthritis is established.
- Vascularised versus non-vascularised graft. Classic series and the Merrell meta-analysis favour vascularised grafts for avascular proximal poles, but the larger Duncumb 2022 systematic review found no significant difference in pooled union (88.7% versus 87.5%), and called for randomised trials.
- Open versus arthroscopic-assisted grafting for nonunion without major humpback, where union rates appear comparable.
Registry Evidence
Unlike arthroplasty, scaphoid nonunion is not tracked by national joint registries (NJR, AJRR, AOANJRR, SHAR, NZJR), which capture hip, knee and other joint replacements rather than carpal reconstruction. The best population-level evidence therefore comes from epidemiological cohorts (Garala 2016) and large pooled systematic reviews (Duncumb 2022) rather than implant registries.
Global Practice Variation
- Routine CT for union/deformity and MRI for proximal pole viability
- Access to headless compression screws and vascularised graft (1,2 ICSRA, free MFC) techniques
- Microsurgical capability concentrated in tertiary hand units
- Reliance on plain radiographs; delayed or missed initial diagnosis more common
- K-wire fixation and non-vascularised iliac crest/distal radius grafts predominate
- Later presentation increases the proportion presenting with established SNAC
Exam framing: scaphoid nonunion has no Level I guideline, so candidates should reason from principles - confirm nonunion and deformity (CT), assess vascularity (MRI plus intra-operative bleeding), debride, correct humpback, stabilise, and salvage once SNAC arthritis is established - and be able to cite the controversy that pooled data (Duncumb 2022) question the assumed superiority of vascularised grafts.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old male presents with wrist pain 2 years after a fall. He recalls being told he fractured his wrist but didn't follow up after initial casting. CT shows a waist nonunion with humpback deformity (intrascaphoid angle 55 degrees). MRI shows no gadolinium enhancement of the proximal pole.”
“A 22-year-old female presents with 1 year of wrist ache after a fall playing netball. She was initially treated in a cast for 6 weeks. CT shows a waist nonunion with minimal deformity (intrascaphoid angle 35 degrees). MRI shows normal proximal pole signal with good gadolinium enhancement.”
“A 45-year-old manual laborer presents with progressive wrist pain and stiffness. Radiographs show a long-standing scaphoid nonunion with arthritic changes at the radial styloid and scaphocapitate joint. The capitolunate joint appears preserved.”
MCQ Practice Points
Q: What is the primary blood supply to the scaphoid and why is the proximal pole at risk for AVN?
A: The dorsal scaphoid branch of the radial artery provides 70-80% of the blood supply. It enters the scaphoid at the dorsal ridge (waist level) and supplies the bone via retrograde flow. The proximal pole receives only 20-30% of its supply directly, making it highly vulnerable to AVN when the waist is fractured.
Q: What lateral intrascaphoid angle indicates significant humpback deformity requiring wedge graft correction?
A: A lateral intrascaphoid angle greater than 45 degrees indicates significant humpback deformity. Normal is less than 35 degrees. Angles between 35-45 degrees are borderline. Significant humpback must be corrected with a wedge graft (e.g., Fisk-Fernandez) to restore scaphoid length and allow union.
Q: When is a vascularized bone graft indicated for scaphoid nonunion?
A: Vascularized bone graft (typically 1,2 ICSRA) is indicated for:
- AVN of the proximal pole (no MRI gadolinium enhancement)
- Failed previous non-vascularized graft
- Prolonged nonunion (greater than 5 years)
Non-vascularized graft in AVN has unacceptably low union rates (less than 60%). VBG achieves 80-90% union in AVN.
Q: Where is the 1,2 ICSRA located and how is it harvested?
A: The 1,2 ICSRA (1,2 Intercompartmental Supraretinacular Artery) runs between the 1st extensor compartment (APL, EPB) and the 2nd extensor compartment (ECRL, ECRB) in the supraretinacular plane (above the extensor retinaculum). It is harvested from the dorsal distal radius as a pedicled bone flap, maintaining the vascular pedicle for transfer to the scaphoid nonunion site.
Q: What is the sequence of joint involvement in SNAC wrist?
A: SNAC wrist progresses through 4 stages:
- Stage 1: Radial styloid to scaphoid
- Stage 2: + Scaphocapitate joint
- Stage 3: + Capitolunate joint
- Stage 4: Pancarpal (including radiolunate)
Key difference from SLAC: In SNAC, radiolunate is preserved until Stage 4, allowing salvage procedures (4-corner fusion, PRC) in earlier stages.
Q: What percentage of untreated scaphoid nonunions develop arthritis?
A: 100% of untreated scaphoid nonunions will eventually develop SNAC wrist arthritis. Mack et al (1984) showed 97% had radioscaphoid arthritis within 10 years. This makes observation inappropriate - all symptomatic nonunions should be treated surgically.
Key Statistics
- 5-15% nonunion rate (30% proximal pole)
- 100% progress to SNAC wrist if untreated
- 80% blood from dorsal scaphoid branch (retrograde)
- Only 20-30% of proximal pole has direct supply
Herbert D Classification
- D1: Fibrous union - ORIF, may not need graft
- D2: Pseudarthrosis - ORIF + bone graft
- D3: Sclerotic - Debride + extensive graft
- D4: AVN - VASCULARIZED bone graft required
Humpback Deformity
- Flexion through nonunion site
- Creates dorsal convexity (humpback)
- Measure lateral intrascaphoid angle
- Greater than 45 degrees = significant = wedge graft needed
Graft Selection
- Viable bone (MRI signal+) = Non-vascularized graft
- AVN (no MRI enhancement) = VBG (1,2 ICSRA)
- Failed surgery = Free vascularized (MFC)
- 1,2 ICSRA: between 1st and 2nd compartments, supraretinacular
SNAC Stages
- Stage 1: Radial styloid-scaphoid
- Stage 2: + Scaphocapitate
- Stage 3: + Capitolunate
- Stage 4: Pancarpal (including radiolunate)
Must Know for Exam
- Retrograde blood supply - proximal pole at risk
- MRI with gadolinium for AVN assessment
- VBG (1,2 ICSRA) for AVN - gold standard
- Correct humpback with wedge graft
- All untreated nonunions become SNAC
Evidence Base
1,2 ICSRA Vascularized Bone Graft (Zaidemberg)
- Cadaveric study (10 dissections) defined a consistent vascularised bone graft from the distal dorsoradial radius (later termed the 1,2 ICSRA graft)
- Used in 11 patients with long-standing scaphoid nonunion with good results
- Described as technically easy, offering shorter immobilisation and a higher union rate than conventional inlay grafting
- Pedicled graft avoids the microsurgical anastomosis needed for free transfers
Natural History of Scaphoid Nonunion (Mack)
- 47 nonunions in 46 symptomatic patients; duration of nonunion 5 to 53 years
- Three radiographic stages: changes confined to scaphoid (8.2 years), radioscaphoid arthritis (17.0 years), generalised wrist arthritis (31.6 years)
- Fracture displacement and carpal instability (lunate dorsiflexion 10 degrees or more) correlated with severity of degeneration
- Few nonunions remained undisplaced, stable or arthritis-free beyond 10 years
Scaphoid Malunion and Humpback Deformity (Amadio)
- 45 patients with 46 healed scaphoid fractures assessed by trispiral tomography after union
- Normal lateral intrascaphoid angle defined as less than 35 degrees; humpback malunion ranged up to 60 degrees
- Normal alignment gave 83% satisfactory outcomes and only 22% post-traumatic arthritis
- Lateral intrascaphoid angulation greater than 45 degrees gave just 27% satisfactory outcomes and 54% arthritis
Treatment of Scaphoid Nonunions: Quantitative Meta-analysis (Merrell)
- Meta-analysis of 36 eligible studies addressing scaphoid nonunion treatment
- Unstable nonunions: screw fixation with grafting 94% union versus K-wires and wedge grafting 77%
- Avascular proximal pole: vascularised graft 88% union versus 47% with screw and wedge fixation
- Solid screw fixation showed no clear benefit from prolonged postoperative casting
Medial Femoral Condyle vs Distal Radial Pedicle Graft for Avascular Nonunion (Jones)
- 22 scaphoid waist nonunions with an avascular proximal pole and carpal collapse, treated at two institutions
- Free vascularised medial femoral condyle (MFC) graft: 12 of 12 united (100%) at a median 13 weeks
- Distal radial pedicled graft: only 4 of 10 united (40%) at a median 19 weeks
- Union rate significantly higher and time to union shorter with the MFC graft (p = 0.005)
Vascularised vs Non-vascularised Grafting: Systematic Review (Duncumb)
- 78 studies, 7,671 patients (mean age 27.9 years, 87.8% male) pooled for scaphoid nonunion union rates
- Mean union 88.7% for non-vascularised versus 87.5% for vascularised grafts, with no significant difference (p = 0.685)
- No significant difference between fixation techniques, or between distal radius and iliac crest graft sources
- Studies excluding both proximal pole fractures and AVN achieved 96.5% union, significantly higher than the rest (86.8%, p less than 0.001)