Precarious Blood Supply | Hawkins Classification | AVN Risk | Urgent Reduction
- Blood supply enters posteriorly via artery of tarsal canal and sinus - displaced fractures disrupt this
- Hawkins sign at 6-8 weeks (subchondral lucency) indicates revascularization occurring, AVN unlikely
- Absence of Hawkins sign does NOT confirm AVN - need longer follow-up and MRI
- Dislocated talus (Hawkins II-IV) needs urgent reduction for skin/neurovascular safety; AVN is driven by initial displacement more than time-to-fixation
- Malunion causes hindfoot varus and medial ankle arthritis from altered biomechanics
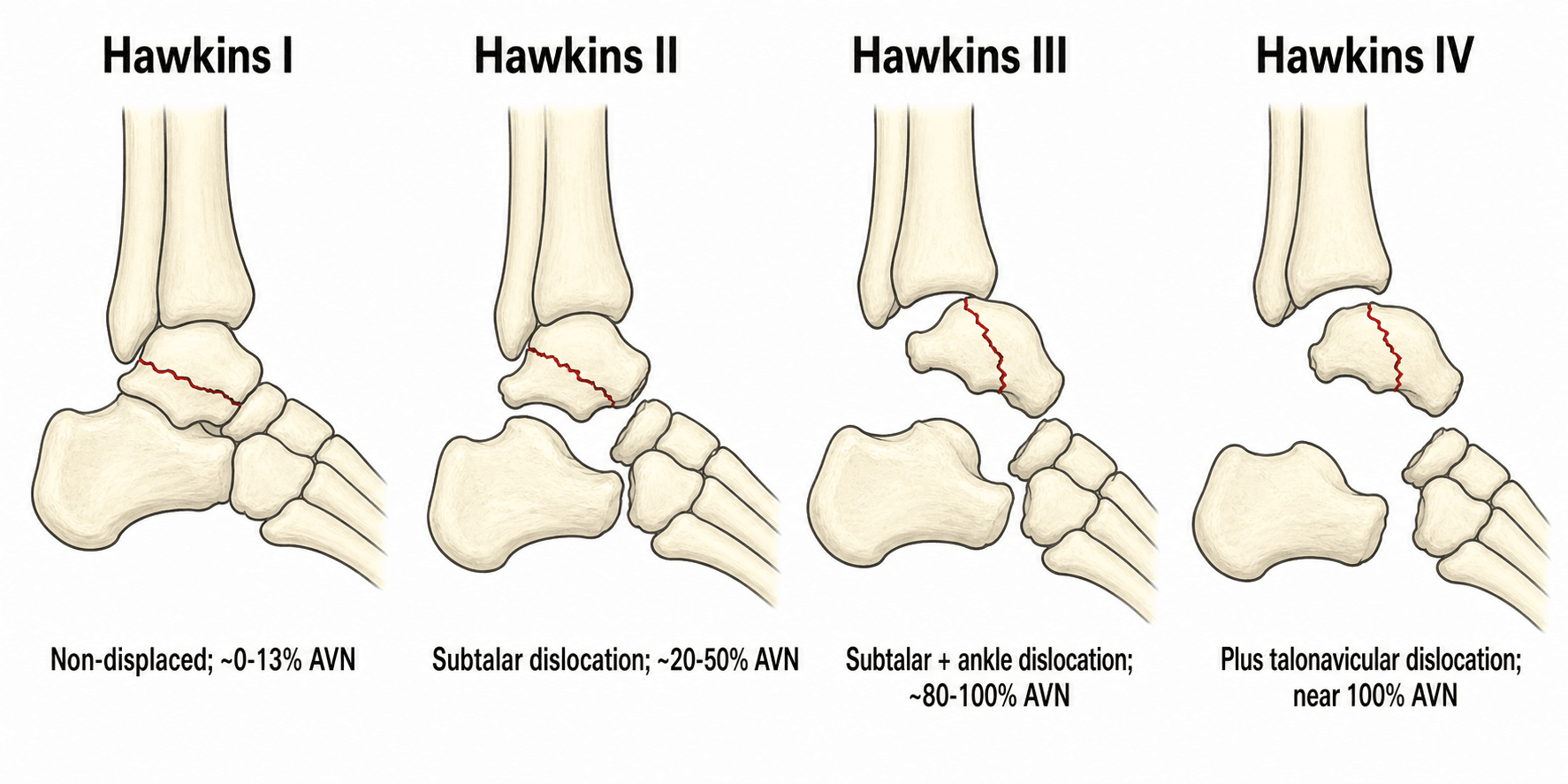
- “Hawkins I: 0-13% AVN | Hawkins II: 20-50% AVN | Hawkins III: 80-100% AVN | Hawkins IV: near 100% AVN
- “Canale view: foot maximally plantarflexed and pronated 15°, beam 75° from horizontal - shows talar neck en face
- “Dual incisions (anteromedial and anterolateral) reduce wound complications for talar neck ORIF
- “Body fractures treated based on displacement and pattern - often need CT for operative planning
Artery of tarsal canal and sinus tarsi enter posteriorly. Displaced talar neck fractures disrupt blood supply. Subtalar dislocation compounds ischemia. AVN develops in 50-100% of Hawkins III/IV without urgent reduction.
I: Non-displaced vertical neck. II: Displaced + subtalar dislocation. III: Type II + ankle dislocation. IV: Type III + talonavicular dislocation. Each type increases AVN risk exponentially.
Hawkins III and IV are surgical emergencies. Reduce within 6-12 hours to restore blood supply. Closed reduction attempted first. If unsuccessful, proceed to immediate open reduction and temporary K-wire fixation.
Hawkins sign positive at 6-8 weeks indicates subchondral lucency on ankle mortise radiograph indicating revascularization indicating AVN unlikely. Absence does NOT confirm AVN - longer follow-up needed. MRI gold standard for diagnosis.
- Dislocation Pattern
- No dislocation
- AVN Risk
- 0-13%
- Treatment
- ORIF with screws (anteromedial approach)
- Key Pearl
- Can often delay 24-48h for swelling
- Dislocation Pattern
- Subtalar dislocation
- AVN Risk
- 20-50%
- Treatment
- Urgent closed reduction, then ORIF
- Key Pearl
- Most common type - reduce urgently
- Dislocation Pattern
- Subtalar + ankle dislocation
- AVN Risk
- 80-100%
- Treatment
- EMERGENCY reduction + ORIF
- Key Pearl
- Every hour delay increases AVN risk
- Dislocation Pattern
- Triple dislocation (+ talonavicular)
- AVN Risk
- Near 100%
- Treatment
- EMERGENCY reduction + ORIF
- Key Pearl
- Extremely high energy - check for compartment syndrome
SCATTalus Blood Supply (Critical for AVN Understanding)
Hook:SCAT indicates Supply Comes from Artery entering Tail (posteriorly) - displaced neck fractures cut this supply!
Overview and Epidemiology
The talus is unique: 60% articular surface, no muscular attachments, precarious blood supply. This combination makes talus fractures challenging - high AVN risk, difficult surgical access, and poor outcomes. The talus is the second most common tarsal bone fractured after the calcaneus, but outcomes are often worse due to blood supply issues.
- High-energy trauma: MVA, fall from height (most common for displaced fractures)
- Forced dorsiflexion: Talar neck impacts against anterior tibial plafond
- Snowboarder's fracture: Lateral process fracture from eversion and dorsiflexion
- Aviation accidents: Original description by Anderson in aviators (rudder bar injury)
- Sports injuries: Basketball, football, snowboarding
- No muscular attachments - entirely dependent on ligamentous blood supply
- 60% covered by articular cartilage - limits surface area for vessel entry
- Blood supply enters posteriorly - severed by anterior neck displacement
- Watershed zone at talar neck - most vulnerable area
- Thin soft tissue envelope - high risk of open fracture and wound complications
Pathophysiology and Mechanisms
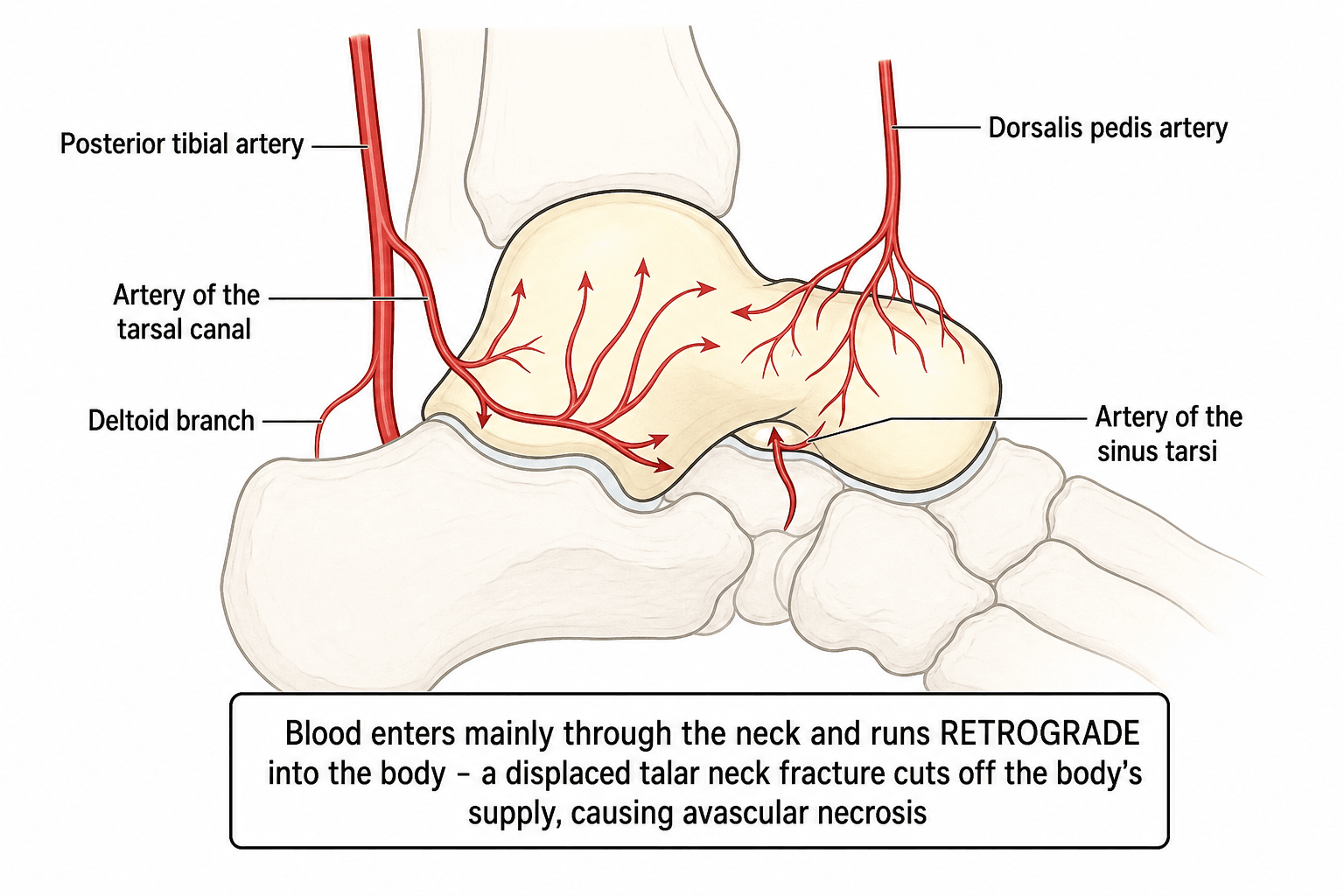
The talus receives blood from three main arteries that enter posteriorly and inferiorly. The artery of the tarsal canal (from posterior tibial artery) is the DOMINANT supply to the talar body, entering through the sinus tarsi. Displaced talar neck fractures with subtalar dislocation disrupt this blood supply, leading to AVN in 50-100% of cases. This is why emergency reduction within 6-12 hours is critical.
- Origin
- Posterior tibial artery
- Area Supplied
- Talar body (70-80%)
- Clinical Significance
- MAIN supply - disrupted in Hawkins II-IV
- Origin
- Dorsalis pedis (anterior tibial)
- Area Supplied
- Lateral talar body
- Clinical Significance
- Anastomoses with tarsal canal artery
- Origin
- Posterior tibial artery
- Area Supplied
- Medial talar body
- Clinical Significance
- Minor contribution, inconsistent
- Origin
- Dorsalis pedis
- Area Supplied
- Talar neck and head
- Clinical Significance
- Preserved in most neck fractures
Classification Systems
Hawkins Classification of Talar Neck Fractures
Most important classification for talus fractures - directly correlates with AVN risk based on degree of dislocation and blood supply disruption.
- Fracture Pattern
- Vertical neck fracture, non-displaced
- Dislocation
- None
- AVN Risk
- 0-13%
- Treatment Urgency
- Semi-urgent (24-48h acceptable)
- Fracture Pattern
- Vertical neck fracture, displaced
- Dislocation
- Subtalar joint only
- AVN Risk
- 20-50%
- Treatment Urgency
- Urgent (6-12h reduction goal)
- Fracture Pattern
- Vertical neck fracture, displaced
- Dislocation
- Subtalar AND ankle joints
- AVN Risk
- 80-100%
- Treatment Urgency
- EMERGENCY (immediate reduction)
- Fracture Pattern
- Vertical neck fracture, displaced
- Dislocation
- Subtalar, ankle, AND talonavicular
- AVN Risk
- Near 100%
- Treatment Urgency
- EMERGENCY (immediate reduction)
The critical distinction is the number of joints dislocated, not just fracture displacement. Each additional dislocation further compromises blood supply by severing more retinacular vessels entering posteriorly. Type III represents BOTH the tibiotalar AND subtalar joints being disrupted - this is a surgical emergency requiring reduction within 6 hours if possible.
Understanding the Hawkins classification helps predict AVN risk and guide treatment urgency.
NSSAHawkins Classification (1-4 Progression)
Hook:NSSA indicates Neck injury Successively Severs Arteries - each dislocation adds ischemia!
Clinical Assessment
- Mechanism: High-energy (MVA, fall from height) vs low-energy (sports)
- Pain location: Ankle vs hindfoot vs diffuse
- Ability to bear weight: Complete inability suggests significant injury
- Time of injury: Critical for planning urgent reduction
- Associated injuries: Always screen for polytrauma in high-energy mechanisms
- Neurovascular symptoms: Numbness, tingling, coldness
- Look: Swelling, deformity, skin integrity (open fracture?), compartments
- Feel: Bony tenderness (talar neck palpable anteromedially), pulses (dorsalis pedis, posterior tibial)
- Move: Passive ROM painful, crepitus with manipulation
- Neurovascular: Mandatory full assessment - document tibial nerve, deep peroneal nerve, sensation
- Compartments: Palpate all 9 compartments of foot if high-energy mechanism
The talus has a thin soft tissue envelope, especially anteriorly and medially. High-energy displaced talar neck fractures carry a substantial open-fracture rate (around 30% in some level-1 trauma series). [8] Any skin breach near the ankle or hindfoot in the setting of a talus fracture should be assumed to communicate with the fracture until proven otherwise. Open talus fractures carry markedly higher infection and osteonecrosis risk and require urgent surgical debridement and stabilisation. [4]
Investigations

Imaging Protocol for Suspected Talus Fracture
Views required:
- Ankle AP and lateral: Shows talar body, dome, ankle joint relationship
- Ankle mortise: Best for lateral process fractures and talar dome lesions
- Foot AP and lateral: Shows talar head, talonavicular joint
- Canale view (if neck fracture suspected): Foot plantarflexed maximally, pronated 15°, beam 75° from horizontal - shows talar neck en face without overlap
What to look for: Fracture line, displacement, dislocation of subtalar/ankle/talonavicular joints, associated fractures (calcaneus, malleoli).
Indications: ALL displaced talus fractures, body fractures, preoperative planning
What it shows:
- Fracture plane orientation (coronal vs sagittal)
- Degree of comminution
- Occult fracture lines extending into adjacent zones
- Subtalar and ankle joint congruity
- Screw trajectory planning
Timing: After emergency reduction if required, before definitive ORIF. CT helps plan surgical approach and fixation strategy.
Hawkins sign: Subchondral lucency in talar dome on ankle mortise view
Interpretation:
- Present indicates Revascularization occurring, AVN unlikely (90% predictive value)
- Absent indicates Does NOT confirm AVN - could be delayed revascularization or true AVN
Clinical significance: A positive Hawkins sign is reassuring. An absent Hawkins sign warrants MRI if clinically concerned.
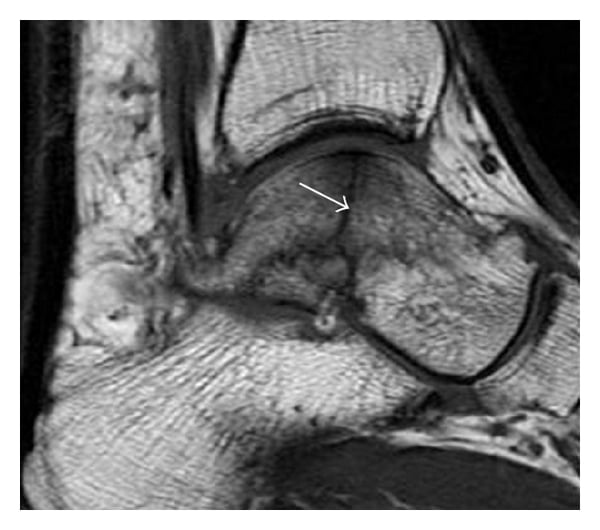
Gold standard for AVN diagnosis. Shows bone marrow edema, signal changes consistent with avascular bone.
Timing: Typically 3-6 months post-injury if Hawkins sign absent or clinical concern. Can detect AVN before radiographic changes (increased density) appear.
Prognosis: Early MRI changes do not predict final outcome - some patients with MRI changes do well, some collapse despite revascularization.
Canale View Technique
Patient positioning: Foot maximally plantarflexed and pronated 15 degrees. X-ray beam angled 75 degrees from horizontal (directed caudad). This view projects the talar neck without overlap from the ankle joint, allowing assessment of displacement and fracture plane. Essential for preoperative planning of talar neck fractures.
Management Algorithm
Non-displaced Talar Neck Fracture Management
Goal: Maintain alignment while allowing healing, monitor for displacement
Treatment Protocol
- Non-weight-bearing in below-knee cast or boot
- Repeat radiographs at 1 week to confirm no displacement
- Admit if unreliable patient or concern for compliance
- Low threshold for ORIF if any displacement seen on repeat films
Why conservative treatment acceptable: AVN risk is low (0-13%) because blood supply is not disrupted. However, secondary displacement can occur, so close monitoring is essential.
- Continue non-weight-bearing if bridging callus not visible
- Weekly radiographs for first month, then every 2 weeks
- If displacement occurs, proceed to ORIF immediately
- At 6 weeks: Check for Hawkins sign (reassuring if present)
- Progressive weight-bearing if radiographs show healing
- Ankle and subtalar ROM exercises begin at 8 weeks
- Return to normal activities by 12 weeks if healed
Any displacement on follow-up radiographs is an indication for ORIF. Even 2mm of displacement can lead to malunion and altered hindfoot biomechanics. Do not persist with conservative treatment if displacement occurs - the window for optimal reduction is narrow.
Conservative management is acceptable for truly non-displaced fractures with reliable follow-up.
Surgical Technique
Patient Positioning for Talar Neck ORIF
Setup Checklist
Supine on radiolucent table
- Head: Secure on donut or headrest
- Arms: Tucked or on arm boards
- Contralateral limb: Extended or frog-legged to allow C-arm access
- Operative leg: Hip externally rotated, knee slightly flexed
- Thigh tourniquet: Apply sterile or non-sterile (cover with drape)
- Bony prominences: Pad sacrum, contralateral heel
- Nerves at risk: Avoid pressure on contralateral fibular head (peroneal nerve)
Tourniquet use: Inflate to 300mmHg (or 100mmHg over systolic) for clear visualization. Deflate after fixation to check perfusion.
- Landmarks exposed: Entire leg from mid-thigh to toes
- Foot free draped: Allow manipulation for reduction
- C-arm access: Position fluoroscopy unit from opposite side of table - confirm AP, lateral, mortise views obtainable before prep
Pre-operative imaging: Take AP, lateral, and mortise views to confirm starting position.
- Implants: 3.5mm or 4.0mm cannulated screws (partially threaded)
- Guidewires: 2.0mm K-wires for temporary fixation and screw placement
- Drill: Cannulated drill bit matching screw size
- Reduction tools: Pointed reduction forceps, bone hook
- C-arm: With radiolucent table
- Small fragment set: For potential plate if comminution present
- AVN: 20-100% depending on Hawkins type (may require fusion later)
- Infection: 5-10% superficial, 2-5% deep (higher if open fracture)
- Nonunion: 5-10% (may need bone grafting and revision)
- Malunion: Varus deformity leading to medial ankle arthritis
- Post-traumatic arthritis: 50-90% at 5 years (ankle and subtalar joints)
- Wound complications: Skin necrosis (thin soft tissue envelope)
- Nerve injury: Sural nerve (anterolateral approach), saphenous nerve (anteromedial)
Proper positioning ensures good surgical access and adequate fluoroscopic imaging.
Complications
- Incidence
- Hawkins I: 0-13%, II: 20-50%, III: 80-100%, IV: near 100%
- Risk Factors
- Displaced fracture, delay to reduction, open fracture
- Prevention and Management
- PREVENTION: Emergency reduction within 6-12h. MANAGEMENT: Protected weight-bearing, monitor with X-ray and MRI, consider fusion if collapse
- Incidence
- 15-20% if not anatomically reduced
- Risk Factors
- Inadequate reduction, comminution, poor fixation
- Prevention and Management
- PREVENTION: Anatomic reduction mandatory, check fluoroscopy rigorously. MANAGEMENT: Corrective osteotomy vs fusion if symptomatic
- Incidence
- Neck: 5-10%, Body: 15-25%
- Risk Factors
- Poor blood supply, malreduction, smoking, diabetes
- Prevention and Management
- MANAGEMENT: Revision ORIF with bone grafting (iliac crest or distal tibia), consider fusion if bone quality poor
- Incidence
- Ankle: 50-70%, Subtalar: 60-90% at 5 years
- Risk Factors
- Articular surface damage, malunion, AVN
- Prevention and Management
- PREVENTION: Anatomic reduction. MANAGEMENT: Activity modification, bracing, eventual fusion (ankle, subtalar, or triple arthrodesis)
- Incidence
- 10-15% (dehiscence, necrosis)
- Risk Factors
- Thin soft tissue, dual incisions, smoking, diabetes
- Prevention and Management
- PREVENTION: Gentle soft tissue handling, avoid tension. MANAGEMENT: Early plastic surgery consult, possible flap coverage
- Incidence
- Open fractures: 25%, Closed: 2-5%
- Risk Factors
- Open fracture, contamination, diabetes, smoking
- Prevention and Management
- PREVENTION: Early debridement for open fractures, IV antibiotics. MANAGEMENT: Debridement, hardware retention if stable, long-term antibiotics
AVN develops over months to years. The Hawkins sign appears at 6-8 weeks post-injury on ankle mortise radiograph (subchondral lucency in talar dome) and indicates revascularization is occurring - AVN is unlikely. Absence of Hawkins sign does NOT confirm AVN - it may simply mean revascularization is delayed. If Hawkins sign is absent and patient is symptomatic, obtain MRI at 3-6 months to assess for AVN. Even with MRI evidence of AVN, some patients remain asymptomatic and do not require intervention.
VANIAComplications of Talus Fractures
Hook:VANIA indicates Varus And Necrosis are Inevitable Aftermaths in displaced talus fractures!
Salvage of Talar AVN and Collapse
The complications section establishes that AVN is the signature complication and that many cases revascularise without collapse, and the viva scenarios ask about core decompression and the choice of fusion for symptomatic AVN. The salvage pathway itself deserves to be set out.
- Option
- Observation with serial radiographs/MRI; protected weight-bearing
- Key point
- Many revascularise without collapse; prolonged offloading is NOT indicated for partial AVN and does not reliably prevent collapse
- Option
- Core decompression (and/or vascularised bone graft) as an adjunct
- Key point
- Borrowed from hip AVN; limited talar evidence - not standard and does not reliably prevent collapse
- Option
- Blair fusion: tibiotalar arthrodesis with an anterior sliding cortical graft from the distal tibia into the preserved talar neck/head
- Key point
- Preserves hindfoot height and some subtalar motion
- Option
- Tibiotalocalcaneal fusion (retrograde nail or plate; bulk graft to restore height)
- Key point
- Salvages a plantigrade foot when both joints are gone
- Option
- Tibiocalcaneal fusion was satisfactory in Canale's series but shortens the limb; talectomy alone did poorly and is avoided
- Key point
- Choose limb-shortening salvage only when reconstruction or a Blair fusion is not feasible
AVN is the signature complication of talar neck fracture, but many cases revascularise WITHOUT collapse, so partial AVN is observed (serial imaging, protected weight-bearing) - prolonged offloading is not indicated and does not reliably prevent collapse. Core decompression (with or without a vascularised graft) is borrowed from hip AVN as a pre-collapse adjunct with limited talar evidence. Once the avascular body COLLAPSES and is symptomatic, arthrodesis is the reliable salvage: a Blair fusion (tibiotalar fusion with an anterior sliding cortical graft from the distal tibia into the preserved talar neck/head) when the body is dead but the head and neck remain viable, preserving hindfoot height and some subtalar motion; a tibiotalocalcaneal fusion when both the ankle and subtalar joints are destroyed. Talectomy alone gives poor function and is avoided (Canale), while tibiocalcaneal fusion is a satisfactory but limb-shortening salvage.
Postoperative Care and Rehabilitation
Standard Postoperative Protocol (Hawkins I-II)
Rehabilitation Timeline
- Non-weight-bearing with crutches
- Below-knee posterior splint in neutral dorsiflexion
- Elevation: Leg elevated above heart level as much as possible
- DVT prophylaxis: Aspirin 325mg daily or LMWH (discuss with patient)
- Wound check: 10-14 days, remove sutures
- Radiographs: At first visit to confirm maintained reduction
- Convert to below-knee cast or CAM boot (removable for hygiene)
- Continue non-weight-bearing
- Ankle pumps: Gentle plantarflexion/dorsiflexion exercises in boot (no inversion/eversion)
- Radiographs: At 4 weeks and 6 weeks to assess healing
- Assess for Hawkins sign at 6-8 weeks (if present, reassuring)
- Begin partial weight-bearing at 6 weeks if radiographs show healing (bridging callus)
- Continue in boot until 10-12 weeks
- Physical therapy: ROM exercises (ankle plantarflexion/dorsiflexion, subtalar inversion/eversion)
- Strengthening: Theraband exercises, toe raises, balance training
- Progress to full weight-bearing by 10-12 weeks if healed
- Transition to regular shoes with supportive insert
- Impact activities: Begin jogging at 4-5 months if full ROM and strength
- Sports: Return to sports at 6 months if cleared by surgeon
- Radiographs: Every 3 months for first year to monitor for AVN
Standard protocol for most talar neck fractures treated with ORIF.
Varus Malunion: Recognition and Correction
Varus is named throughout as the commonest deformity after talar neck fracture, but how it arises, what it does to the foot, and how it is corrected are never developed - and it is a classic viva endpoint.
- Detail
- Under-appreciated dorsomedial neck comminution: the neck heals SHORT and in varus (often with dorsiflexion and medial deviation), frequently worsened by over-compressing a lag screw across the medial comminution
- Detail
- Hindfoot varus with forefoot adduction/supination; lateral-border weight-bearing and callus; subtalar motion locked and eversion lost; drives medial peritalar and ankle arthritis
- Detail
- Clinical hindfoot varus + forefoot adduction; the Canale view and CT show medial neck shortening, varus and rotation - always compare with the contralateral side
- Detail
- Read the medial comminution; use a medial plate and/or bone graft to hold length rather than crushing it with compression
- Detail
- Corrective talar neck osteotomy (recreating the original fracture plane) if the joints are preserved; corrective arthrodesis (e.g. triple) if the peritalar joints are already arthritic
Varus is the commonest talar-neck malunion, and it usually comes from under-appreciating dorsomedial neck comminution: the neck heals SHORT and in varus, often made worse by over-compressing a lag screw across the medial comminution. The result is a stiff, in-toed foot in hindfoot varus with forefoot adduction that weight-bears on its lateral border, locks the subtalar joint and drives medial peritalar arthritis. Prevent it by reading the medial comminution and holding length with a medial plate or bone graft rather than crushing it, confirming alignment on the Canale view. A symptomatic varus malunion with preserved joints is corrected by a talar neck osteotomy that recreates the original fracture plane; once the peritalar joints are arthritic, a corrective triple arthrodesis is preferred.
Outcomes and Prognosis
- Good Prognosis
- Type I (non-displaced)
- Poor Prognosis
- Type III-IV (triple dislocation)
- Good Prognosis
- Reduced within 6 hours
- Poor Prognosis
- Delayed over 12 hours
- Good Prognosis
- Neck fracture, isolated
- Poor Prognosis
- Body fracture or neck+body combined
- Good Prognosis
- Closed fracture
- Poor Prognosis
- Open fracture (infection + AVN risk)
- Good Prognosis
- Anatomic (under 1mm step-off)
- Poor Prognosis
- Malreduced (varus or step-off over 2mm)
- Good Prognosis
- No AVN or AVN without collapse
- Poor Prognosis
- AVN with talar dome collapse
Even with perfect reduction and fixation, outcomes are guarded. Studies show 50-90% of patients develop post-traumatic arthritis of the ankle or subtalar joints within 5 years. 20-30% require secondary surgery (fusion) within 10 years. The goal of ORIF is to delay arthritis onset and potentially avoid or delay fusion, but it does not prevent arthritis. Patient counseling about realistic expectations is critical.
Guidelines, Registries & Global Practice
- Rare injury: talar fractures account for only a small fraction of fractures (roughly 1% of all fractures and the second most common tarsal fracture after the calcaneus) [9]
- High-energy mechanism worldwide: motor-vehicle crashes and falls from height dominate displaced neck/body fractures; the great majority of patients in trauma-centre series are polytraumatised [5]
- Open fractures common: high-energy displaced injuries have a substantial open-fracture rate because of the thin soft-tissue envelope [4]
- Distinct sport pattern: the lateral process ("snowboarder's") fracture is the characteristic low-energy variant from dorsiflexion-eversion
- CT for operative planning: advanced imaging to assess the subtalar joint is endorsed across modern reviews, as even slight subtalar displacement predisposes to arthritis [7]
- Anatomical reduction is the goal: restoration of length, rotation and the subtalar/ankle joints, by ORIF where displaced [2,3]
- Modified Hawkins for AVN prediction: subtalar dislocation (Hawkins IIB/III) is the key driver of osteonecrosis [7,8]
- Emergency = the dislocation, not the clock to definitive fixation [4,8]
- Position on Talar Neck/Body Fractures
- Urgent reduction of dislocations; anatomical ORIF (screws +/- mini-plates), dual approaches for comminuted patterns; CT planning
- Evidence Level
- Expert consensus / Level V
- Position on Talar Neck/Body Fractures
- Dual anteromedial + anterolateral approaches with plate fixation increasingly favoured; modified Hawkins to predict AVN; subtalar joint scrutiny on CT
- Evidence Level
- Narrative review / Level V [7]
- Position on Talar Neck/Body Fractures
- Open talar fractures follow open-fracture standards: early IV antibiotics, combined ortho-plastic debridement, definitive skeletal and soft-tissue cover on a planned list
- Evidence Level
- National standard / consensus
- Position on Talar Neck/Body Fractures
- Timing of DEFINITIVE fixation does not drive AVN; stage ORIF until soft tissues settle once any dislocation is reduced
- Evidence Level
- Level III cohorts [3,4,8]
- National joint arthroplasty registries (NJR, AJRR, AOANJRR, SHAR, NZJR) do not track acute talus fracture fixation, so registry-level implant-survival data of the kind available for hip/knee arthroplasty do not exist for this injury
- The evidence base is therefore retrospective cohorts and reviews from trauma centres, not registries or large RCTs - reflected in the relatively low evidence levels above [5,7]
- Salvage data (ankle/hindfoot fusion) for failed talus fractures is likewise drawn from case series rather than registries [6]
- High-resource centres: CT planning, dual-approach plate fixation, ortho-plastic teams for open injuries, MRI surveillance for AVN
- Limited-resource settings: greater reliance on closed/percutaneous reduction and screw fixation, plain-film follow-up, and earlier acceptance of arthrodesis when reconstruction is not feasible
- Universal priorities everywhere: reduce any dislocation urgently, protect the soft tissues, achieve anatomical alignment, and counsel realistically about arthritis and AVN
References
- Hawkins LG. Fractures of the neck of the talus. J Bone Joint Surg Am. 1970;52(5):991-1002. PMID: 5479485.
- Canale ST, Kelly FB Jr. Fractures of the neck of the talus. Long-term evaluation of seventy-one cases. J Bone Joint Surg Am. 1978;60(2):143-156. PMID: 417084.
- Lindvall E, Haidukewych G, DiPasquale T, Herscovici D Jr, Sanders R. Open reduction and stable fixation of isolated, displaced talar neck and body fractures. J Bone Joint Surg Am. 2004;86(10):2229-2234. PMID: 15466732. doi:10.2106/00004623-200410000-00014.
- Vallier HA, Nork SE, Barei DP, Benirschke SK, Sangeorzan BJ. Talar neck fractures: results and outcomes. J Bone Joint Surg Am. 2004;86(8):1616-1624. PMID: 15292407.
- Elgafy H, Ebraheim NA, Tile M, Stephen D, Kase J. Fractures of the talus: experience of two level 1 trauma centers. Foot Ankle Int. 2000;21(12):1023-1029. PMID: 11139032. doi:10.1177/107110070002101208.
- Sanders DW, Busam M, Hattwick E, Edwards JR, McAndrew MP, Johnson KD. Functional outcomes following displaced talar neck fractures. J Orthop Trauma. 2004;18(5):265-270. PMID: 15105747. doi:10.1097/00005131-200405000-00001.
- Buza JA, Leucht P. Fractures of the talus: current concepts and new developments. Foot Ankle Surg. 2017;24(4):282-290. PMID: 29409210. doi:10.1016/j.fas.2017.04.008.
- Vallier HA, Reichard SG, Boyd AJ, Moore TA. A new look at the Hawkins classification for talar neck fractures: which features of injury and treatment are predictive of osteonecrosis? J Bone Joint Surg Am. 2014;96(3):192-197. PMID: 24500580. doi:10.2106/JBJS.L.01680.
- Rammelt S, Zwipp H. Talar neck and body fractures. Injury. 2009;40(2):120-135. PMID: 18439608. doi:10.1016/j.injury.2008.01.021.
MCQ Practice Points
Q: What is the MAIN blood supply to the talar body?
A: The artery of the tarsal canal, a branch of the posterior tibial artery. This vessel provides 70-80% of the blood supply to the talar body and enters through the tarsal canal beneath the sustentaculum tali. It is disrupted in displaced talar neck fractures with subtalar dislocation (Hawkins Type II-IV), leading to AVN risk.
Q: A 25-year-old has a displaced talar neck fracture with dislocation of the subtalar joint only. The ankle joint is reduced. What is the Hawkins classification and approximate AVN risk?
A: Hawkins Type II, with AVN risk of 20-50%. Type II is defined as a displaced talar neck fracture with subtalar dislocation but the ankle joint remains reduced. Type III would require BOTH subtalar AND ankle dislocation. The AVN risk in Type II is intermediate because the artery of the tarsal canal entering through the sinus tarsi is disrupted.
Q: What does the PRESENCE of the Hawkins sign indicate? What does ABSENCE mean?
A: Presence of Hawkins sign (subchondral lucency on mortise view at 6-8 weeks) indicates revascularization is occurring and AVN is unlikely (90% predictive value). Absence of Hawkins sign does NOT confirm AVN - it may indicate delayed revascularization or true AVN. Further workup with MRI at 3 months is indicated if clinically concerned.
Q: A Hawkins Type III talar neck fracture is seen in the ED. What is the time window for reduction and why?
A: The dislocation should be reduced as an emergency (closed reduction in the ED, or immediate open reduction if irreducible or the skin is threatened) to relieve neurovascular and soft-tissue compromise and restore alignment. The historical claim that each hour of delay proportionally raises AVN is not supported by current series (Vallier and colleagues; Lindvall and colleagues): osteonecrosis correlates with the degree of initial displacement, comminution and open injury rather than time-to-fixation. [4,8] Definitive ORIF can then be staged until soft tissues are safe. In the exam, distinguish the genuine emergency (reducing the dislocation) from the timing of definitive fixation.
Q: What is the internervous plane for the anteromedial approach to the talar neck? What nerve is at risk?
A: The anteromedial approach uses the interval between tibialis anterior (medial, supplied by deep peroneal nerve) and the neurovascular bundle (lateral, containing anterior tibial artery and deep peroneal nerve). The nerve at risk is the deep peroneal nerve, which runs just lateral to the extensor hallucis longus tendon. It must be identified and gently retracted laterally during exposure.
Q: What is the most common malunion deformity after talar neck fracture and what is the clinical consequence?
A: Varus malunion is the most common deformity. Clinical consequence is medial ankle pain and arthritis because the malunion shifts load medially, increasing pressure on the medial talar dome and tibial plafond. This leads to accelerated medial ankle arthritis and often requires corrective osteotomy or fusion if symptomatic.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old male presents to the ED after a motor vehicle accident. He has severe right ankle pain and deformity. On examination, there is gross swelling and deformity of the ankle. Dorsalis pedis pulse is present but diminished. Initial radiographs show a displaced talar neck fracture with subtalar dislocation. How do you assess and manage this patient?”
“You are in the operating room to perform ORIF of a Hawkins Type II talar neck fracture. The patient is positioned supine, the limb is prepped and draped. Walk me through your surgical approach, reduction technique, and fixation strategy for this fracture.”
“A 28-year-old female had ORIF of a Hawkins Type III talar neck fracture 8 weeks ago. She returns to clinic complaining of persistent pain. On examination, there is mild swelling and tenderness over the ankle. Radiographs show maintained reduction and no obvious AVN. However, you note the Hawkins sign is ABSENT on the mortise view. The patient is concerned. How do you counsel and manage this patient?”
Key Anatomy
- Artery of tarsal canal (posterior tibial) provides 70-80% of talar body blood supply
- Enters posteriorly through sinus tarsi - disrupted by anterior neck displacement
- 60% of talus is articular cartilage - limits surface for vessel entry
- No muscular attachments - entirely dependent on ligamentous blood supply
- Talar neck indicates watershed zone indicates most vulnerable to fracture and AVN
Hawkins Classification
- Type I: Non-displaced vertical neck indicates 0-13% AVN indicates ORIF (can delay 24-48h)
- Type II: Displaced neck + subtalar dislocation indicates 20-50% AVN indicates Urgent reduction within 6-12h
- Type III: Type II + ankle dislocation indicates 80-100% AVN indicates EMERGENCY reduction
- Type IV: Type III + talonavicular dislocation indicates near 100% AVN indicates EMERGENCY
- Hawkins sign (6-8 weeks) indicates subchondral lucency indicates revascularization indicates AVN unlikely
Treatment Algorithm
- Hawkins I: NWB cast 6 weeks, ORIF if any displacement on follow-up
- Hawkins II-IV: Emergency closed reduction, then ORIF within 24 hours
- Body fractures (over 2mm displacement): ORIF with lag screws (often dual approach)
- Comminuted body: Consider primary fusion (poor prognosis with ORIF)
- Open fractures: Emergent debridement + ORIF or temporary K-wire fixation
Surgical Pearls
- Anteromedial approach indicates workhorse (between tibialis anterior and NV bundle)
- Deep peroneal nerve at risk - runs lateral to EHL tendon
- Screw trajectory: Anteroposterior from dorsal neck into posterior body (2-3 screws)
- Use partially threaded screws for lag effect (interfragmentary compression)
- Avoid varus malreduction - leads to medial ankle arthritis
- Dual incisions (anteromedial + anterolateral) for complex fractures
Complications
- AVN: Type I 0-13%, Type II 20-50%, Type III 80-100%, Type IV near 100%
- Post-traumatic arthritis: 50-90% at 5 years (ankle and subtalar)
- Malunion (varus): 15-20% - causes medial ankle arthritis
- Nonunion: Neck 5-10%, Body 15-25% (requires bone grafting)
- Wound complications: 10-15% (thin soft tissue envelope)
Evidence Base and Key Trials
Hawkins Classification and AVN Risk - Original Description
- Retrospective series defining the three-part talar neck classification (Type I non-displaced, Type II with subtalar subluxation/dislocation, Type III with subtalar AND ankle dislocation)
- Osteonecrosis risk rose with the degree of dislocation across the three groups
- Described the Hawkins sign - subchondral lucency of the talar dome at roughly 6-8 weeks indicating preserved vascularity (revascularisation)
- Established that absence of the Hawkins sign is not by itself diagnostic of osteonecrosis
Canale and Kelly - Long-Term Evaluation of 71 Talar Neck Fractures
- Long-term review of 71 talar neck fractures with mean follow-up 12.7 years; good or excellent results in 59%
- Avascular necrosis of the talar body in 52% overall - 2 of 13 non-displaced, about half of those with subtalar subluxation/dislocation, and 16 of 19 with complete dislocation of the talar body
- Recommended accurate anatomical reduction of displaced fractures, by open reduction and internal fixation if necessary
- Complications required 25 secondary procedures; triple arthrodesis and tibiocalcaneal fusion did well, talectomy did not
ORIF of Displaced Talar Neck and Body Fractures - Timing and Outcomes
- Retrospective review of 26 isolated displaced talar neck and/or body fractures treated with ORIF, mean follow-up 74 months
- Overall union rate 88%; all closed displaced talar neck fractures healed regardless of the delay to surgery
- A delay in surgical fixation did NOT appear to affect outcome, union, or the prevalence of osteonecrosis
- Post-traumatic subtalar arthritis was actually more common than osteonecrosis; osteonecrosis occurred after 6 of 7 open fractures