Localise the pain, test the DRUJ, then match treatment to tear biology and ulnar load
- Ulnar-sided wrist pain is a localisation problem; not every painful ulnar wrist is a TFCC tear.
- The TFCC includes the articular disc, dorsal and palmar radioulnar ligaments, ulnocarpal ligaments, meniscus homologue and ECU subsheath.
- DRUJ stability depends mainly on the deep foveal fibres of the radioulnar ligaments.
- Palmer classification describes the lesion; treatment also depends on DRUJ stability, reparability, cartilage status and ulnar variance.
- A central stable tear, a repairable peripheral tear and an unstable foveal tear are different clinical problems.
- “Pain with a positive foveal sign suggests TFCC or ulnotriquetral pathology, but it is not a standalone diagnosis.
- “Test DRUJ translation in neutral, pronation and supination, and always compare the opposite wrist.
- “A positive MRI without matching clinical symptoms should not automatically lead to surgery.
- “Debridement alone is a poor answer for a symptomatic foveal tear with DRUJ instability.
- “If ulnar impaction is the driver, the treatment must address ulnar overload, not just the torn disc.
TFCC and Ulnar-Sided Wrist Pain
TFCC signal change is common, especially with age and ulnar loading. The decision to operate should come from symptoms, examination, DRUJ stability, imaging concordance, cartilage status and patient goals.
Overview and Epidemiology
The triangular fibrocartilage complex is the main soft-tissue stabiliser and load-bearing structure on the ulnar side of the wrist. It sits between the distal ulna, sigmoid notch, proximal carpus and ECU subsheath. A painful TFCC lesion may be traumatic, degenerative or part of a wider ulnar-sided wrist problem.
Patients usually present with ulnar wrist pain, pain with gripping or forearm rotation, clicking, weakness, or a feeling that the distal radioulnar joint is unstable. The history must separate a single traumatic event from chronic overload. A fall on an extended wrist with forearm rotation suggests traumatic TFCC injury. Repetitive axial loading, racquet sport, gymnastics, manual work, positive ulnar variance or distal radius malunion suggest ulnocarpal overload.
TFCC abnormalities may also be incidental. Degenerative fraying increases with age and load. The clinical question is therefore not "is there a TFCC signal change?", but "is this lesion responsible for this patient's pain or instability, and what mechanical problem needs to be treated?"
Anatomy and Biomechanics
The TFCC is not one structure. It is a composite stabilising system. The articular disc carries load between the carpus and ulna. The dorsal and palmar radioulnar ligaments are the key stabilisers of the DRUJ. Their deep fibres insert into the ulnar fovea and are critical for stability. The ulnocarpal ligaments connect the ulna and TFCC region to the lunate and triquetrum. The meniscus homologue and ECU subsheath complete the ulnar soft-tissue complex.
The central disc is relatively avascular and has limited healing potential. The peripheral ulnar side is more vascular and is more suitable for repair. This is the biological reason central stable tears are treated differently from peripheral and foveal tears.
The TFCC also behaves as a load regulator. Positive ulnar variance increases ulnocarpal load and can produce degenerative disc wear, lunate or triquetral chondromalacia and lunotriquetral ligament involvement. Negative or neutral variance does not exclude TFCC injury, but it changes the likelihood that ulnar overload is the main driver.

- Role
- Ulnocarpal load-bearing surface
- Clinical implication
- Poor healing potential; symptomatic stable central tears are usually debrided rather than repaired
- Role
- Primary DRUJ stabiliser
- Clinical implication
- Foveal detachment produces instability and usually needs restoration if symptomatic
- Role
- Peripheral support and soft-tissue continuity
- Clinical implication
- Repairable if tissue quality is good and cartilage is preserved
- Role
- Support lunate and triquetrum
- Clinical implication
- Distal avulsions may mimic isolated TFCC pain but behave as carpal stabiliser injuries
- Role
- Stabilises ECU tendon at the ulnar wrist
- Clinical implication
- Snapping ECU can coexist with TFCC symptoms and needs specific treatment
Pathophysiology
TFCC pathology can be grouped into four practical mechanisms.
Usually follows axial load, rotation or traction. The important question is whether the tear is central and stable, peripheral and repairable, or foveal with DRUJ instability.
Ulnar impaction produces progressive wear of the TFCC, chondral change in the lunate or triquetrum and sometimes lunotriquetral ligament involvement.
Distal radius malunion, radial shortening, sigmoid notch incongruity or ulnar styloid base nonunion can create ulnar-sided pain and DRUJ dysfunction.
ECU instability, FCU or pisotriquetral disease, LT injury, inflammatory synovitis and ganglion can coexist with or mimic TFCC symptoms.
A patient with a stable central perforation and a patient with a foveal detachment may both report ulnar wrist pain. The first may need debridement after failed non-operative care. The second needs restoration of the DRUJ stabiliser if instability is symptomatic and cartilage is salvageable.
Classification Systems
- Lesion
- Central traumatic perforation
- Clinical meaning
- Stable disc tear with limited healing potential
- Typical treatment direction
- Debridement if symptomatic after non-operative care
- Lesion
- Ulnar-sided avulsion with or without styloid fracture
- Clinical meaning
- May involve peripheral or foveal attachment; assess DRUJ stability
- Typical treatment direction
- Repair or foveal refixation when symptomatic and repairable
- Lesion
- Distal ulnocarpal ligament avulsion
- Clinical meaning
- Carpal stabiliser injury rather than simple disc tear
- Typical treatment direction
- Repair or reconstruction when unstable or persistently symptomatic
- Lesion
- Radial-sided avulsion
- Clinical meaning
- Radial attachment injury; may be technically difficult
- Typical treatment direction
- Repair selected symptomatic unstable tears
- Lesion
- Degenerative spectrum
- Clinical meaning
- Progressive wear, chondromalacia, perforation, LT involvement and arthritis
- Typical treatment direction
- Debridement, wafer, ulnar shortening or salvage depending stage and load
Palmer describes where the tear is; the Atzei (EWAS) classification is the modern, treatment-oriented arthroscopic scheme for the peripheral/foveal (Palmer 1B) tear and is named above but worth laying out, because it maps directly onto repair vs reconstruction vs salvage:
- Class 1 - distal tear (repairable): the distal (proximal-carpal) component is torn but the deep foveal insertion is intact - DRUJ is stable - so a distal/capsular (suture) repair suffices.
- Class 2 - complete tear (repairable): both the distal and the deep foveal components are torn - DRUJ unstable - needs foveal reinsertion (anchor/transosseous).
- Class 3 - proximal (foveal) tear (repairable): the deep foveal fibres are detached with an intact distal component - again needs foveal reattachment.
- Class 4 - non-repairable tear: the TFCC tissue is irreparable (retracted/poor quality) but the DRUJ cartilage is preserved - needs ligament reconstruction (tendon graft).
- Class 5 - DRUJ arthritis: irreparable with established DRUJ osteoarthritis - repair/reconstruction is contraindicated; treat with DRUJ salvage/arthroplasty.
Exam point: use Atzei to convert "peripheral TFCC tear" into a decision - distal repair (Class 1), foveal reinsertion (Class 2-3), reconstruction (Class 4) or salvage (Class 5) - driven by foveal integrity and DRUJ cartilage.
Clinical Assessment
History should define the mechanism, chronicity and load demand. Ask about fall, twisting injury, racquet or bat sport, gymnastics, manual work, distal radius fracture, previous surgery, inflammatory arthritis, clicking, snapping, instability, weakness, pain with push-up from a chair, and symptoms during pronation or supination. Record hand dominance, work demands, sport and what the patient needs the wrist to do.
Examination starts with comparison. Look for swelling, ulnar head prominence, scars, distal radius malunion, ECU snapping, hypothenar wasting and range restriction. Palpate in a structured way: fovea, ECU groove, FCU and pisiform, lunotriquetral interval, ulnocarpal joint, hook of hamate and DRUJ. Then test motion, grip, DRUJ stability and tendon-specific provocative manoeuvres.
- How to do it
- Press in the soft spot between ulnar styloid, FCU, volar ulnar head and pisiform
- Positive finding
- Localised deep tenderness
- What it suggests
- TFCC peripheral/foveal or ulnotriquetral pathology
- How to do it
- Translate distal ulna dorsally and volarly relative to radius in neutral, pronation and supination
- Positive finding
- Painful excess translation or poor endpoint
- What it suggests
- DRUJ instability or foveal detachment
- How to do it
- Press prominent distal ulna volarly and observe rebound
- Positive finding
- Excess mobility or pain
- What it suggests
- DRUJ instability, but compare with the other side
- How to do it
- Axial load with ulnar deviation and forearm rotation
- Positive finding
- Ulnar-sided load pain
- What it suggests
- TFCC tear or ulnar impaction; not specific alone
- How to do it
- Patient pushes up from chair using the hand
- Positive finding
- Reproduction of ulnar wrist pain
- What it suggests
- Load-sensitive TFCC or ulnocarpal pathology
- How to do it
- Resisted thumb radial abduction or resisted wrist extension-ulnar deviation
- Positive finding
- ECU groove pain or snapping
- What it suggests
- ECU tendinopathy or subsheath pathology
- How to do it
- Stress lunate and triquetrum against each other
- Positive finding
- Painful clunk or local LT pain
- What it suggests
- Lunotriquetral ligament injury
Do not miss infection, inflammatory arthritis, occult fracture, malignancy, acute DRUJ dislocation, acute Essex-Lopresti pattern, vascular insufficiency or ulnar nerve symptoms. Numbness, coldness, progressive swelling, fever, severe night pain or acute deformity should change the pathway.
Investigations
Start with good radiographs. Standard PA and lateral wrist films should be obtained with reproducible positioning. Look for distal radius malunion, ulnar styloid base nonunion, DRUJ arthritis, ulnar variance, carpal alignment, lunate or triquetral cystic change and occult fracture signs. A clenched-fist or pronated grip view can accentuate dynamic ulnar variance in selected cases.
MRI is useful when the clinical picture matches TFCC or ulnar-sided soft-tissue pathology. MR arthrography may improve detection of full-thickness communication, but imaging must be interpreted with symptoms and examination. CT is valuable for DRUJ congruity, sigmoid notch deformity, malunion, ulnar styloid base nonunion and occult fracture. Dynamic ultrasound is useful for ECU subluxation.
Arthroscopy remains the most direct method of assessing tear location, cartilage, trampoline test, hook test, peripheral reparability and combined intra-articular pathology. It is both diagnostic and therapeutic, but should not be used as a substitute for a thoughtful preoperative diagnosis.
- Best for
- Variance, malunion, styloid nonunion, arthritis, carpal alignment
- Limitations
- Can miss soft-tissue tears and occult fractures
- Best for
- TFCC signal, marrow oedema, ECU, LT ligament, occult pathology
- Limitations
- False positives occur; resolution and reader expertise matter
- Best for
- Full-thickness communication and intra-articular tear assessment
- Limitations
- Invasive; still must be clinically correlated
- Best for
- DRUJ congruity, sigmoid notch, malunion and fracture
- Limitations
- Limited soft-tissue information
- Best for
- ECU subluxation and tendon pathology
- Limitations
- Operator dependent; not a full TFCC assessment
- Best for
- Direct tear assessment, cartilage and treatment
- Limitations
- Invasive; should answer a defined clinical question
Management Decisions
Management is based on symptoms, chronicity, DRUJ stability, tear location, tissue quality, cartilage status, ulnar variance and patient demand. Most stable, non-acute presentations deserve a period of non-operative care unless there is clear mechanical instability or a time-sensitive associated injury.
Non-operative care is appropriate for many stable TFCC and ulnar-sided wrist pain presentations. The usual elements are activity modification, splinting or cast immobilisation, anti-inflammatory measures when appropriate, hand therapy, proprioceptive retraining, ECU control when relevant, and graded return to load.
- Practical detail
- Wrist or Munster-style immobilisation depending on rotation pain and DRUJ symptoms
- Reason
- Reduces painful forearm rotation and ulnocarpal load
- Practical detail
- Range, proprioception, grip progression, ECU control and gradual loading
- Reason
- Restores function without provoking recurrent synovitis
- Practical detail
- Consider diagnostic or therapeutic injection when diagnosis remains uncertain
- Reason
- Can localise pain generator and reduce inflammation
- Practical detail
- Escalate if persistent mechanical symptoms, instability or load-limiting pain remains
- Reason
- Avoids prolonged ineffective treatment for repairable instability
For the arthritic or irreparably unstable DRUJ (Atzei Class 5), "DRUJ salvage" is named above but the candidate should be able to compare the actual options:
- Darrach (distal ulna resection): excise the distal ulna - simple, reliable pain relief for the low-demand/elderly patient, but risks painful ulnar stump instability and radioulnar convergence/impingement under load (so avoid in young, high-demand patients).
- Sauvé-Kapandji: arthrodese the DRUJ and create a proximal ulnar pseudarthrosis (segmental resection just proximal to the fused joint). It preserves the ulnar head buttress to the carpus (better than Darrach for ulnar-carpal support) and is favoured in the younger/higher-demand patient, but can still develop a painful/unstable proximal ulnar stump.
- Hemiresection-interposition arthroplasty (Bowers) / matched ulnar resection: resect the arthritic ulnar head but preserve the styloid/TFCC attachment and interpose soft tissue - relies on a competent TFCC, so not for the grossly unstable joint.
- Constrained (linked) DRUJ arthroplasty: an implant replacing the joint - increasingly favoured for the young, high-demand, painful arthritic/unstable DRUJ to avoid the stump problems of resection, though long-term durability data are still maturing.
Exam point: Darrach for low-demand; Sauvé-Kapandji preserves the ulnar buttress for the younger patient; hemiresection (Bowers) needs an intact TFCC; constrained DRUJ arthroplasty is the rising option for the high-demand arthritic/unstable joint - the shared late problem of the resection procedures is a painful unstable ulnar stump.
Surgical Technique
The operative plan should be written before the patient enters theatre: diagnostic arthroscopy only, debridement, peripheral repair, foveal repair, ulnar unloading, correction of malunion, ECU stabilisation or a combined procedure. Position the patient supine with the arm on a hand table. Use traction for wrist arthroscopy, protect superficial sensory nerves around portals, and confirm portals with surface anatomy before incision.
- Purpose
- Provide stable access to radiocarpal and midcarpal compartments
- Pitfall
- Excess traction can distort assessment and injure soft tissues
- Purpose
- Common radiocarpal portals include 3-4, 4-5 and 6R or 6U depending target
- Pitfall
- Protect dorsal sensory branches and ECU region
- Purpose
- Assess cartilage, SL, LT, TFCC disc, peripheral rim and synovitis
- Pitfall
- Do not focus only on the MRI-reported area
- Purpose
- Trampoline assesses central tension; hook test assesses foveal attachment
- Pitfall
- A stable central tear and foveal detachment need different operations
- Purpose
- Debride, repair, refix or unload according to the mechanical diagnosis
- Pitfall
- Debridement that destabilises the rim can worsen symptoms
- Core steps
- Diagnostic arthroscopy, define stable rim, shave unstable central flap, preserve peripheral attachments
- Technical priorities
- Remove only unstable tissue; avoid enlarging into the vascular/stabilising rim
- Core steps
- Freshen tear edge if needed, pass sutures, capture capsule/TFCC rim, secure outside capsule or with all-inside device
- Technical priorities
- Protect dorsal sensory nerve branches; avoid overtightening
- Core steps
- Confirm instability, prepare foveal footprint, pass sutures through deep fibres, fix to fovea with transosseous tunnels or anchor
- Technical priorities
- Reduction of the deep stabiliser matters more than cosmetic disc appearance
- Core steps
- Preoperative variance plan, diaphyseal osteotomy, compression plating, confirm length and rotation
- Technical priorities
- Avoid nonunion, hardware irritation and over-shortening
- Core steps
- Arthroscopic or open distal ulnar dome resection in selected overload cases
- Technical priorities
- Preserve DRUJ cartilage and avoid excessive resection
For TFCC surgery, a strong answer is not just a list of portals. State the diagnosis, why the lesion is symptomatic, whether the DRUJ is stable, what you will inspect arthroscopically, what finding will change treatment, and how you will protect the stabilising rim.
Complications
The commonest failure pattern is treating a visible TFCC tear while missing the real pain generator: ulnar impaction, ECU instability, LT injury, distal radius malunion, DRUJ arthritis or inflammatory disease.
Debridement without recognising foveal detachment can leave ongoing DRUJ instability.
Portal nerve irritation, stiffness, infection, tendon irritation, persistent synovitis and complex regional pain can occur after wrist arthroscopy.
Ulnar shortening can cause delayed union, nonunion, plate irritation, refracture after plate removal, DRUJ symptoms or overcorrection.
- Consider
- DRUJ instability, incongruity or arthritis
- Next step
- Repeat focused examination, CT and review arthroscopy findings
- Consider
- Ulnar impaction or uncorrected positive variance
- Next step
- Reassess radiographs and MRI for overload pattern
- Consider
- ECU subsheath instability
- Next step
- Dynamic ultrasound and ECU-specific examination
- Consider
- Complex regional pain, over-immobilisation or inflammatory pathology
- Next step
- Early recognition, therapy and pain strategy
Postoperative Care
Postoperative care depends on what was done. Debridement is usually followed by early motion once wounds settle. Peripheral repair or foveal repair needs protection from rotation and load while the repair heals. Ulnar shortening osteotomy needs bone-healing precautions and hardware surveillance.
- Protection
- Short period of dressing or splint comfort
- Progression
- Early wrist and forearm motion, then graded strengthening
- Protection
- Immobilise wrist and limit forearm rotation initially
- Progression
- Protected motion, then progressive strengthening and load
- Protection
- Stronger rotation protection, often above-elbow or Munster-style immobilisation early
- Progression
- Delay forceful pronation-supination until healing is secure
- Protection
- Protect weight bearing until osteotomy healing is evident
- Progression
- Monitor union and plate irritation; return to heavy load only after union
Patients should be warned that grip strength, rotation comfort and load tolerance recover gradually. Persistent ulnar wrist pain after surgery may reflect wrong diagnosis, untreated ulnar impaction, DRUJ arthritis, ECU pathology, neuroma, stiffness, nonunion after osteotomy or complex regional pain.
Outcomes and Prognosis
Outcomes are best when diagnosis, tear biology and mechanics match the operation. Stable central tears often improve after debridement when the symptoms are truly from the tear and there is no untreated overload. Peripheral and foveal repairs do best when tissue is repairable, cartilage is preserved, instability is corrected and rehabilitation is followed. Degenerative overload outcomes depend on correcting the load problem while avoiding overtreatment in low-demand or minimally symptomatic patients.
Poorer prognostic factors include chronic instability, DRUJ arthritis, marked cartilage loss, distal radius malunion that is not corrected, workers compensation or high-load occupational demands, smoking when osteotomy is performed, and prolonged pain sensitisation.
Guidelines, Registries & Global Practice
TFCC injury is one of the commonest causes of ulnar-sided wrist pain worldwide and is frequently associated with distal radius fractures: an ulnar styloid or peripheral TFCC injury accompanies a large proportion of displaced distal radius fractures, although most do not produce symptomatic DRUJ instability and do not require fixation. Because the TFCC is not an implant, there is no dedicated arthroplasty-style registry; the strongest pooled data come from systematic reviews rather than national joint registries. The principles below hold across FRCS (Tr and Orth), FRACS, EBOT/FEBOT, ABOS, DNB/MS and SICOT practice.
There is no single international society guideline that mandates one TFCC pathway. The points of genuine consensus and divergence between major bodies are summarised below.
- Emphasis
- Arthroscopy-based, treatment-oriented classification (Atzei classes 1 to 5; Herzberg disc-reins-wall scheme)
- Practical recommendation
- Define the unstable structure arthroscopically, then debride, repair the wall, reinsert the fovea or reconstruct accordingly
- Emphasis
- Stability-led decision making and non-operative first for stable tears
- Practical recommendation
- Confirm DRUJ stability and symptom concordance before surgery; hand-therapy-led rehabilitation
- Emphasis
- Distal radius fracture guidance notes routine ulnar styloid fixation is not required
- Practical recommendation
- Fix the styloid or repair the foveal TFCC only when the DRUJ is unstable after radius fixation
- Emphasis
- Restore radial length and alignment to protect the DRUJ
- Practical recommendation
- Correct distal radius malunion or sigmoid notch incongruity as a driver before shortening a normal ulna
Practice varies by resources rather than by principle. In high-resource settings, MRI, MR arthrography and diagnostic wrist arthroscopy are widely available, and foveal repair, ulnar shortening osteotomy and constrained DRUJ arthroplasty are routine. In limited-resource settings, diagnosis leans more heavily on a structured examination, plain radiographs for ulnar variance and malunion, and a diagnostic or therapeutic ulnocarpal injection, with arthroscopy reserved or replaced by open techniques. Across all settings, the documentation that justifies surgery is the same: the functional limitation, failed non-operative measures, imaging concordance with the symptomatic side, and objective DRUJ instability.
References
- 1Palmer AK, Werner FW. "The triangular fibrocartilage complex of the wrist: anatomy and function". Journal of Hand Surgery. 1981PubMed
- 2Palmer AK. "Triangular fibrocartilage complex lesions: a classification". Journal of Hand Surgery. 1989PubMed
- 3Vezeridis PS, Yoshioka H, Han R, Blazar P. "Ulnar-sided wrist pain. Part I: anatomy and physical examination". Skeletal Radiology. 2010PubMed
- 4Watanabe A, Souza F, Vezeridis PS, Blazar P, Yoshioka H. "Ulnar-sided wrist pain. II. Clinical imaging and treatment". Skeletal Radiology. 2010PubMed
- 5Tay SC, Tomita K, Berger RA. "The ulnar fovea sign for defining ulnar wrist pain: an analysis of sensitivity and specificity". Journal of Hand Surgery. 2007PubMed
- 6Andersson JK et al.. "A systematic review and analysis of Palmer type I triangular fibrocartilage complex injuries: outcomes of treatment". Journal of Wrist Surgery. 2020PubMed
- 7Atzei A, Luchetti R et al.. "Arthroscopic foveal repair of the triangular fibrocartilage complex". Journal of Wrist Surgery. 2015PubMed
- 8Herzberg G, Burnier M, Ly L, Nakamura T, del Pinal F, Atzei A. "A new arthroscopic classification of triangular fibrocartilage complex disorders". Journal of Wrist Surgery. 2024PubMed
- 9Owens J, Compton J, Day M, Glass N, Lawler E. "Nonunion rates among ulnar-shortening osteotomy for ulnar impaction syndrome: a systematic review". Journal of Hand Surgery (American). 2018PubMed
- 10Rodriguez-Merchan EC, Shojaie B, Kachooei AR. "Distal radioulnar joint instability: diagnosis and treatment". Archives of Bone and Joint Surgery. 2022PubMed
Controversies and Areas of Uncertainty
Much of TFCC practice rests on case series and expert classification rather than randomised data, so several decisions remain genuinely contested.
For mild positive variance with a central degenerative perforation, the arthroscopic wafer avoids hardware and nonunion but gives limited correction; ulnar shortening corrects variance more reliably but carries roughly a 4 percent nonunion risk and frequent hardware irritation. There is no high-level trial that settles which is superior, and selection is variance-, cartilage- and surgeon-driven.
Systematic reviews report broadly equivalent outcomes, with scant evidence to mandate either approach. The real determinant is whether the lesion is a peripheral wall tear or a deep foveal detachment, not the access route.
A styloid tip fracture rarely needs fixation. The debate is the styloid base fracture with DRUJ instability: some restore stability by fixing the base, others by repairing the foveal TFCC directly. The unifying principle is to treat the stabiliser, not the radiograph.
Degenerative TFCC change and even perforation are common with age and ulnar loading and are frequently asymptomatic. There is no agreed threshold at which an imaging finding alone justifies surgery; concordance with symptoms, examination and stability remains the arbiter.
For the irreparable, arthritic DRUJ, the balance between soft-tissue reconstruction, traditional salvage (Darrach, Sauve-Kapandji, hemiresection) and constrained DRUJ arthroplasty is shifting toward implant arthroplasty in suitable patients, but durability data are still maturing. Match the procedure to age, demand, bone stock and soft-tissue quality rather than defaulting to a single salvage.
At a Glance Table
- Likely source
- TFCC peripheral or foveal tear
- Confirm with
- Foveal sign, DRUJ ballottement, MRI or arthroscopy
- Management implication
- Assess stability before deciding debridement versus repair
- Likely source
- DRUJ instability
- Confirm with
- Ballottement in neutral, pronation and supination; CT if incongruent
- Management implication
- Foveal repair, reconstruction or salvage depends on cartilage and chronicity
- Likely source
- ECU subluxation or tendinopathy
- Confirm with
- ECU synergy test, resisted extension-ulnar deviation, dynamic ultrasound
- Management implication
- Treat ECU pathology, not TFCC alone
- Likely source
- Ulnar impaction
- Confirm with
- PA neutral wrist radiograph, grip view, MRI marrow signal
- Management implication
- Consider ulnar unloading when non-operative care fails
- Likely source
- Lunotriquetral ligament injury
- Confirm with
- LT shear or ballottement test, MRI arthrogram or arthroscopy
- Management implication
- Different reconstruction pathway from TFCC
- Likely source
- Pisotriquetral or FCU pathology
- Confirm with
- Pisotriquetral grind, carpal tunnel view, local injection
- Management implication
- Avoid mislabelling as TFCC
TIDEUlnar Wrist Differential
Hook:TIDE keeps the ulnar wrist differential broad.
CPFUTFCC Treatment Biology
Hook:Central, peripheral, foveal and ulnar overload are four different treatment problems.
NPSDRUJ Instability Check
Hook:Test the DRUJ in Neutral, Pronation and Supination.
Clinical Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old tennis player has six months of ulnar wrist pain after a twisting injury. MRI reports a TFCC tear. How do you assess and manage this?”
“A 55-year-old manual worker has chronic ulnar-sided wrist pain, positive ulnar variance and MRI marrow signal in the lunate with TFCC degeneration.”
“A 38-year-old has a clunking, painful DRUJ four months after a plated distal radius fracture. Radial length and alignment are restored on radiographs, but the ulnar head translates and the fovea sign is positive. How do you proceed?”
Assessment
- Localise the pain: fovea, ECU, ulnocarpal, lunotriquetral, pisotriquetral or DRUJ.
- Compare DRUJ translation with the other wrist in neutral, pronation and supination.
- Record load pain, clicking, snapping, instability and functional demand.
- Do not rely on MRI without concordant symptoms and examination.
Imaging
- PA and lateral radiographs first.
- Assess ulnar variance, malunion, styloid base, DRUJ arthritis and carpal alignment.
- MRI or MR arthrogram helps when the clinical question is soft-tissue pathology.
- CT is useful for DRUJ congruity, malunion and occult fracture.
Treatment
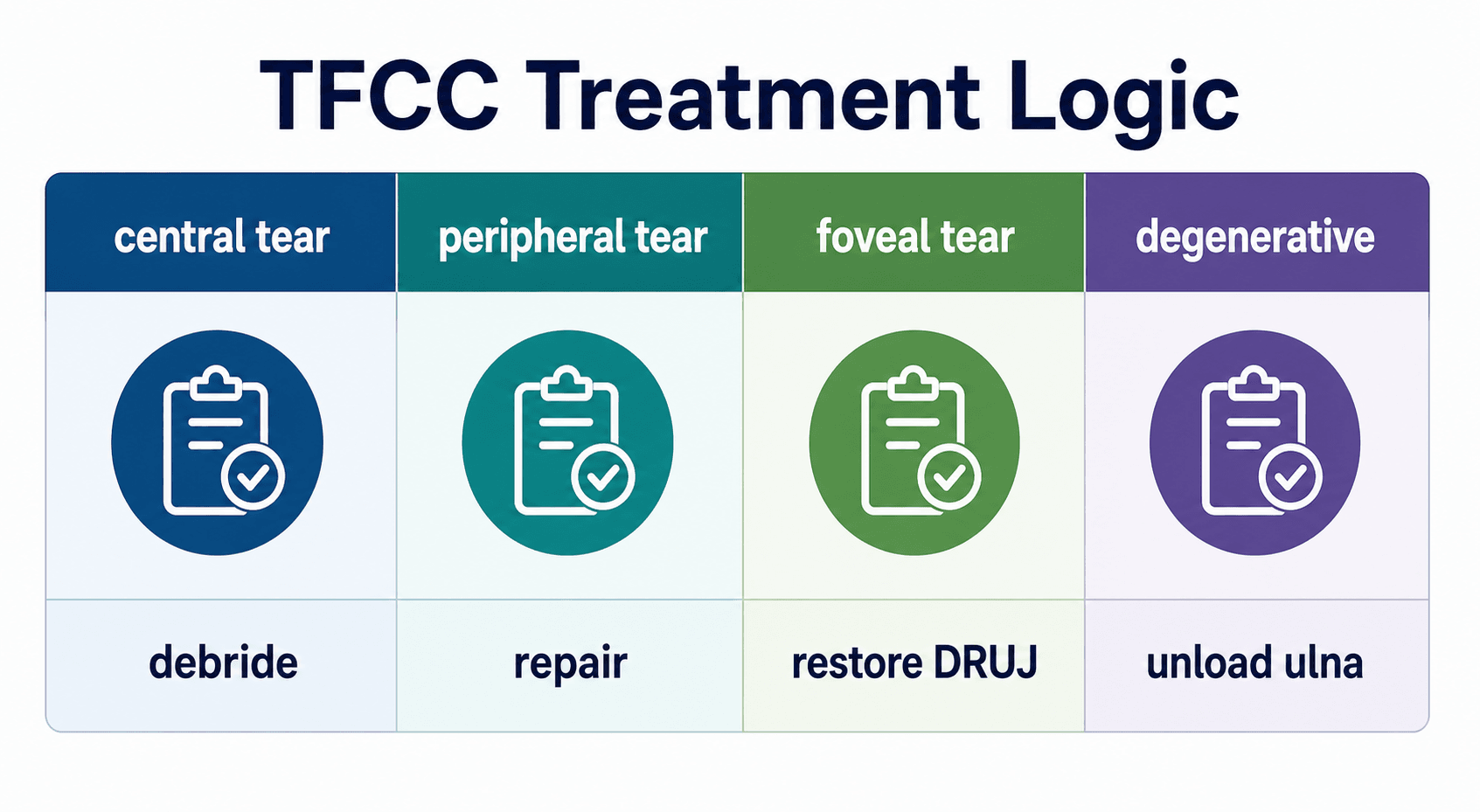
- Stable central tear: non-operative care, then debridement if persistent.
- Repairable peripheral tear: repair when symptoms persist.
- Foveal tear with instability: restore foveal attachment.
- Degenerative ulnar impaction: unload the ulna or correct the malunion.
Do Not Miss
- ECU instability.
- Lunotriquetral ligament injury.
- Distal radius malunion.
- DRUJ arthritis.
- Inflammatory, infectious, vascular or nerve pathology.
“The safest approach is to localise the ulnar wrist pain, define DRUJ stability, identify ulnar overload, then choose treatment according to tear biology and mechanics.”
Evidence Base
Palmer classification: the original descriptive framework
- Built from anatomic, biomechanical and 10 years of clinical experience using examination, radiographs, arthrography, arthroscopy and arthrotomy.
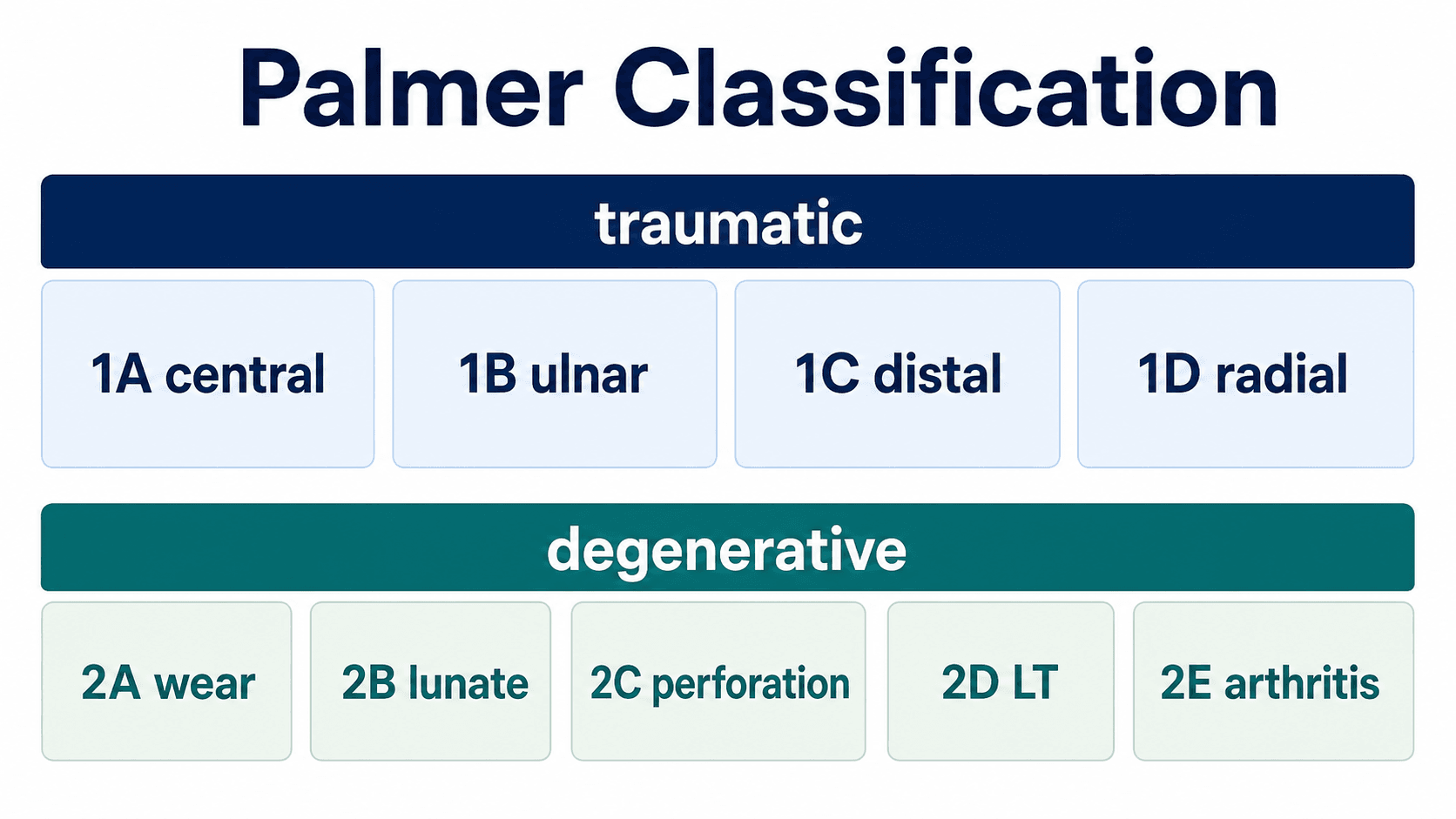
- Separates traumatic lesions (Class 1, classified by location: 1A central, 1B ulnar, 1C distal, 1D radial) from degenerative lesions (Class 2, graded 2A to 2E).
- Degenerative spectrum links TFCC wear with ulnar head, ulnocarpal and lunotriquetral disease.
Foundational anatomy: the TFCC as a composite load-bearer and DRUJ stabiliser
- Across 61 specimens the TFCC was a homogeneous complex of disc, dorsal and volar radioulnar ligaments, meniscus homologue, ulnar collateral ligament and ECU sheath.
- Perforations were present in 53 percent of specimens, and every perforated wrist showed lunate or distal ulna cartilage erosion.
- The TFCC both cushions the ulnar carpus and is a major DRUJ stabiliser; excision risks ulnolunate abutment and instability.
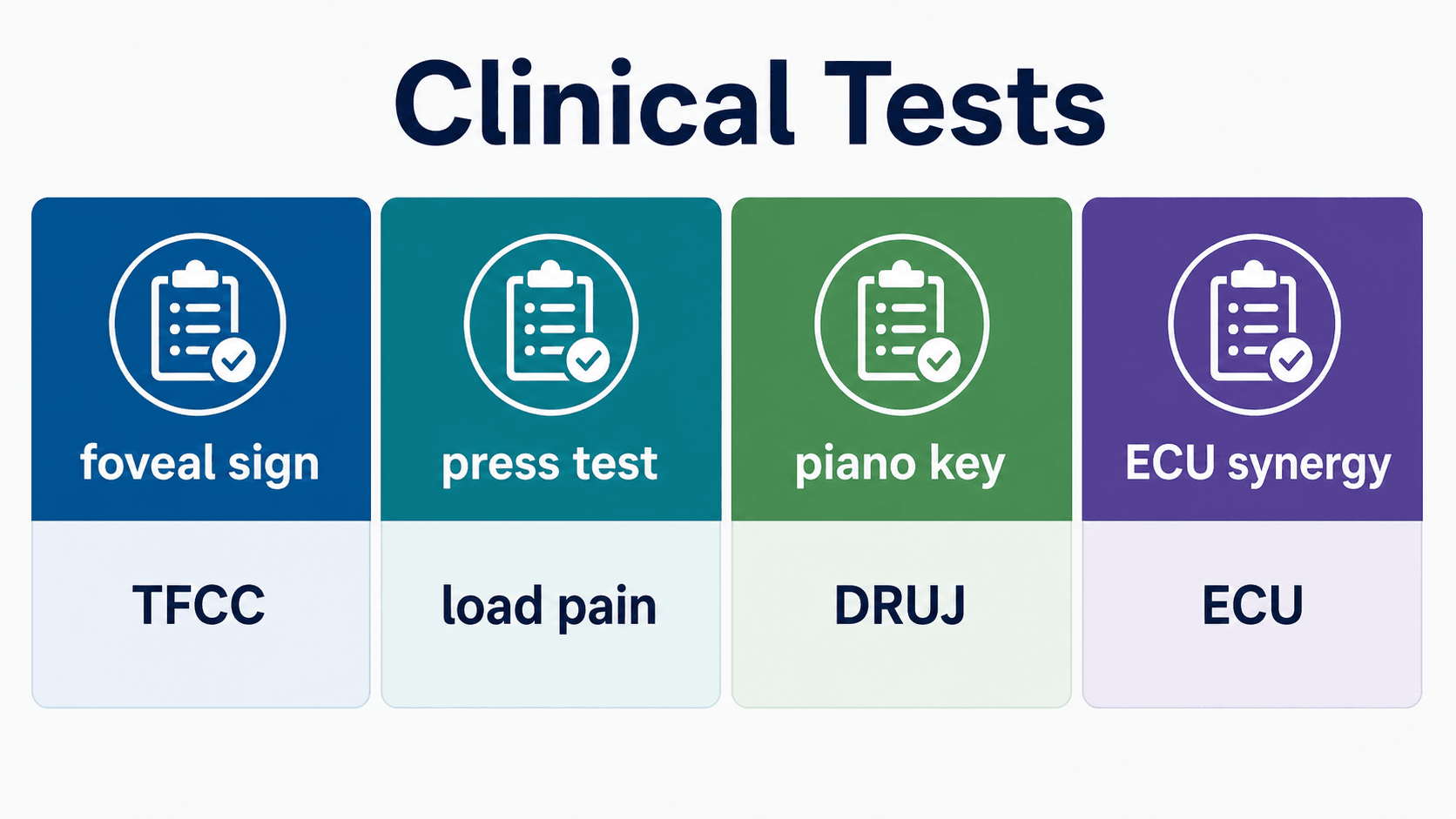
Ulnar fovea sign: a validated bedside localiser
- In 272 consecutive arthroscopy patients the fovea sign detected foveal disruption or ulnotriquetral ligament injury with 95.2 percent sensitivity and 86.5 percent specificity.
- Ulnotriquetral tears typically had a stable DRUJ; foveal disruptions typically had an unstable DRUJ.
- A simple, reproducible test that points to two distinct ulnar-sided pain sources.
Systematic approach to ulnar-sided wrist pain
- Ulnar-sided wrist pain has a broad anatomical differential with small structures and subtle imaging findings.
- TFCC, DRUJ, ECU, FCU, lunotriquetral ligament and ulnocarpal overload must be separated clinically.
- A structured physical examination should localise the structure before imaging is interpreted.