
Article summary
Practical techniques for committing the many orthopaedic classifications to durable memory for exams.
Educational content is reviewed for source visibility, editorial coherence, and correction readiness.
No individual clinician credential is claimed unless a named person is shown.
Verify before clinical use; this is not medical advice or a substitute for local guidance.
As an orthopaedic surgeon, your brain must hold a vast library of fractures, mechanisms, and management pathways. To survive high-stakes exams like the FRCS (Tr & Orth) or the American Board of Orthopaedic Surgery exams, you need to do much more than simply recognise an injury—you must instantly recall its exact alphanumeric classification. Moving these complex schemas from short-term cramming to durable, long-term memory requires a strategic, active approach to learning.
The Danger of Rote Memorisation
When faced with the sheer volume of orthopaedic classifications, the default response for many surgical trainees is to lock themselves in a room and attempt to recite the texts until the numbers stick. This method of rote memorisation is fundamentally flawed for the budding orthopaedic surgeon. The human brain is remarkably inefficient at storing isolated, context-free alphanumeric data. When you try to memorise the Weber classification solely as "A, B, C", you are placing an immense burden on your working memory. Under the intense, sweaty-palmed pressure of a viva examination, this fragile mental house of cards collapses entirely. You find yourself confusing the AO/OTA alphanumeric system, second-guessing whether a specific fracture is a Type II or a Type III, and losing valuable time.
The most common mistake trainees make is treating classifications as arbitrary trivia. To build durable memory, you must stop viewing these systems as lists to be memorised and start understanding them as descriptive biological tools. Classifications were not designed to torture medical students; they were created by surgeons to guide treatment, predict outcomes, and facilitate communication.
To memorise them effectively, you must anchor the classification to its underlying purpose. Ask yourself: Why did the author group these specific fractures together? Usually, it is because they share a common mechanism of injury, a similar prognosis, or require the same surgical fixation. When you attach clinical relevance to an alphanumeric code, you transform an abstract digit into a meaningful clinical concept, giving your brain a sturdy scaffolding to hold onto.
Deconstruct the Logic Before You Memorise
Before you attempt to commit a classification to memory, take a step back and map out the architectural logic of the system. Almost every well-known orthopaedic classification follows an internal, highly logical rule set. If you can decode the matrix, you rarely have to memorise the individual tiers.
Take the AO/OTA classification for long bones as the ultimate example. Instead of trying to memorise hundreds of individual permutations, you must learn the grammar of the system. Once you understand that the first number dictates the bone, the second dictates the segment (1 for proximal, 2 for diaphyseal, 3 for distal), and the third dictates the fracture pattern (1 for simple, 2 for wedge, 3 for complex), you can logically deduce the classification of fractures you have never even seen before.
Similarly, look at the Neer classification for proximal humeral fractures. It is not an arbitrary scale. It is an anatomical puzzle governed by a strict rule: a segment is only considered "displaced" if it is separated by more than one centimetre or angulated by more than 45 degrees. If you internalise that one defining rule, you do not need to memorise every two-part, three-part, and four-part combination—you simply count the displaced segments. By deconstructing the logic first, you drastically reduce the sheer volume of raw data you need to rote learn.

Build a Visual Memory Palace
Orthopaedics is an inherently visual surgical specialty. Reading a description of a fracture in a textbook engages the language centres of your brain, but recognising and classifying a fracture on a radiograph engages the visual and spatial centres. To excel in both written exams and clinical viva stations, you must translate two-dimensional word problems into three-dimensional mental images.
For logically grouped classifications, try assigning specific visual archetypes to each category. Let us return to the Weber ankle classification, which is elegantly tied to the level of the fibular fracture relative to the syndesmosis. Do not just memorise the letters. Construct a vivid mental image of the anterior inferior tibiofibular ligament (AITFL) as a firm, unyielding band.
For a Weber A, picture the fibula breaking cleanly below that intact band—the mortise is stable. For a Weber B, imagine the fracture line spiralling right through the level of the syndesmosis, partially tearing the ligament and leaving the ankle in a state of precarious uncertainty. For a Weber C, picture the fibula snapping high above the syndesmotic complex, rupturing the entire syndesmosis and rendering the ankle joint grossly unstable. When you build these vivid, almost cinematic mental images, you bypass the rote memory centres and wire the classification directly into your visual cortex, which is far more powerful and durable.
Harness the Power of Clinical Contrast
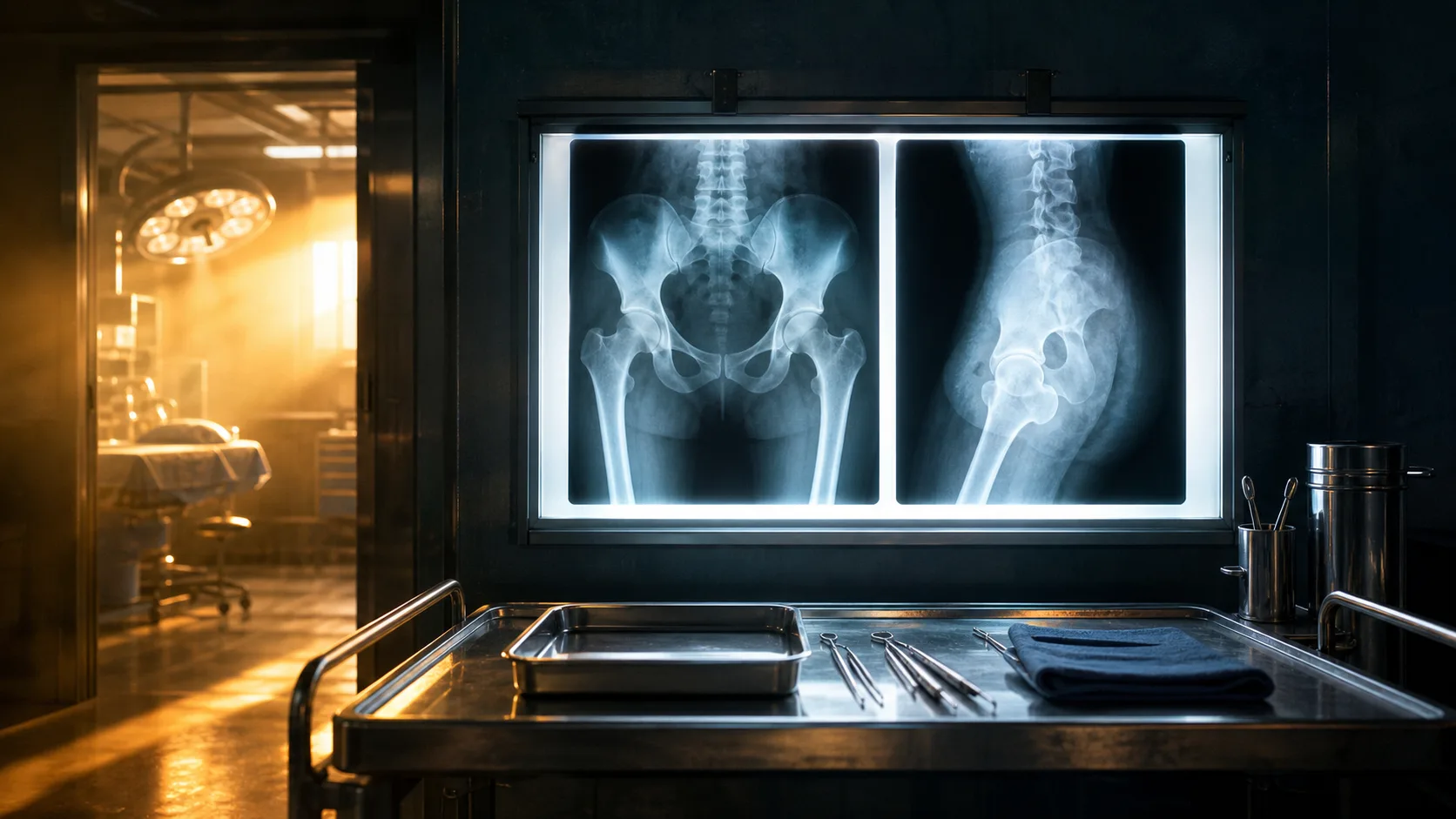
To audit your memory, you must subject it to active recall, but doing this with isolated, textbook-perfect radiographs is a common trap. Real fractures—and real exam cases—rarely present as perfect, classic archetypes. To build a robust, exam-proof memory, you need to actively use clinical contrast.
This technique involves placing two subtly different pathologies side-by-side and forcing your brain to articulate the exact distinguishing features. Take the Garden classification of femoral neck fractures. Trainees frequently confuse a Garden I (incomplete/valgus impacted) with a Garden III (complete, partially displaced). Both are intracapsular, and both can present with similar clinical signs in an elderly patient. To cement the difference, pull up both imaging sets simultaneously. Train your eye to trace the trabeculae. In the Garden I fracture, forcefully note how the primary compressive trabeculae form a slight valgus angle. In the Garden III, trace how those same trabeculae have rotated into a varus alignment.
By actively contrasting the imaging, you train your brain to look for the specific visual triggers that separate an undisplaced fracture (which might be managed conservatively or with parallel screws) from a displaced one (which dictates an arthroplasty). This cements the classification far more effectively than staring at a single, perfectly impacted Garden I fracture in isolation.
Spaced Repetition and the Intelligent Flashcard
If there is a single "cheat code" for long-term retention, it is spaced repetition. The premise is simple: you review a piece of information just as your brain is on the verge of forgetting it. This forces the neural pathway to strengthen, moving the data from short-term to durable, long-term memory. For the modern orthopaedic trainee, this is best achieved using digital flashcard applications.
However, many trainees use these digital tools incorrectly. They create text-heavy flashcards asking, "What are the types of Rockwood AC joint dislocations?" This is ineffective. The golden rule of orthopaedic spaced repetition is that your flashcards must be radiological.
How to Build the Perfect Orthopaedic Flashcard
- Front of the card: A high-quality, anonymised radiograph of a fracture. Add a brief clinical vignette if you want to mimic a viva scenario, but avoid giving the diagnosis away.
- Back of the card: The exact name of the classification system, the specific grade or type of the fracture shown, and most importantly, the defining feature that gives it that grade.
- Review schedule: Let the software's algorithm dictate when you see the card again. If you instantly recognise a Salter-Harris IV fracture and can explain the transphyseal component, you will not see it for weeks. If you struggle to differentiate a Type II from a Type III, the system will aggressively surface the card until you master it.
Building a high-yield deck of radiological flashcards is time-consuming, but it is arguably the single highest-yield investment you can make during your exam preparation.
The Magnetic Drawing Board Technique
There is a deeply uncomfortable moment in oral examinations where the examiner slides a blank piece of paper and a pen across the table and asks you to draw a classification. Suddenly, the spatial relationships that seemed so obvious on a radiograph become a tangled mess of overlapping lines under the pressure of the examiner's gaze. To prevent this, you must add a kinetic element to your study routine.
Purchase a small whiteboard or a magnetic drawing board. When studying, challenge yourself to rapidly draw the foundational schema of the classification. This is particularly effective for pattern-based systems like the Salter-Harris classification for paediatric physeal fractures.
The SALTER Mnemonic: A Kinetic Example
- S - Slipped (Type I)
- A - Above (Type II - above the growth plate, through the metaphysis)
- L - Lower (Type III - below the growth plate, through the epiphysis)
- T - Through (Type IV - through the metaphysis, plate, and epiphysis)
- E - ERasure / Crush (Type V - compression of the plate)
Do not just recite the mnemonic. Draw the growth plate as a thick, bold line. Practise drawing the fracture line cleanly through the correct anatomical zones. As you draw Type II, physically say "Above." As you draw Type IV, say "Through." By engaging your motor cortex and your vocal cords simultaneously, you create multiple overlapping memory traces. When you are eventually standing at a viva board, you will have the muscle memory to confidently draw exactly what the examiner is describing.
Integrate Mock Vivas and Verbalisation
Knowledge that remains unspoken is rarely exam-ready. You may have perfectly memorised the Schatzker classification for tibial plateau fractures, but if you cannot articulate it smoothly, confidently, and concisely out loud, your exam performance will suffer.
Find a fellow surgical trainee, a supportive consultant, or even a trusted medical student. Sit down in front of a computer screen displaying a random bank of orthopaedic trauma. Set a strict timer. When the image appears, you must talk out loud.
Start with the obvious: "I am presented with an anteroposterior and lateral radiograph of a left knee." Proceed to your classification: "This demonstrates a bicondylar tibial plateau fracture. According to the Schatzker classification, this represents a Type VI injury." Then—crucially—justify your reasoning just as you would in a clinical scenario: "I have classified this as a Type VI because there is a metadiaphyseal dissociation separating the condylar block from the diaphysis."
Verbalisation forces your brain to organise information chronologically and coherently. You will quickly discover where your mental blocks lie. You might find you can smoothly articulate Types I through IV of a system, only to stumble entirely on the rare Type V and VI. This form of active, high-stakes retrieval highlights your exact weaknesses, allowing you to refine your study strategy before the actual exam day.
True mastery of orthopaedic classifications requires you to evolve from a passive consumer of textbook tables into an active, visual, and logical thinker. By anchoring data to clinical purpose, leveraging spaced repetition with high-quality imaging, and pressure-testing your knowledge through drawing and speech, you transform fragile memorisation into permanent expertise. Classifications will cease to be a source of exam anxiety and will instead become the precise, intuitive language of your daily surgical practice.
Share this article
Useful for a journal club, study list, or teaching session.

