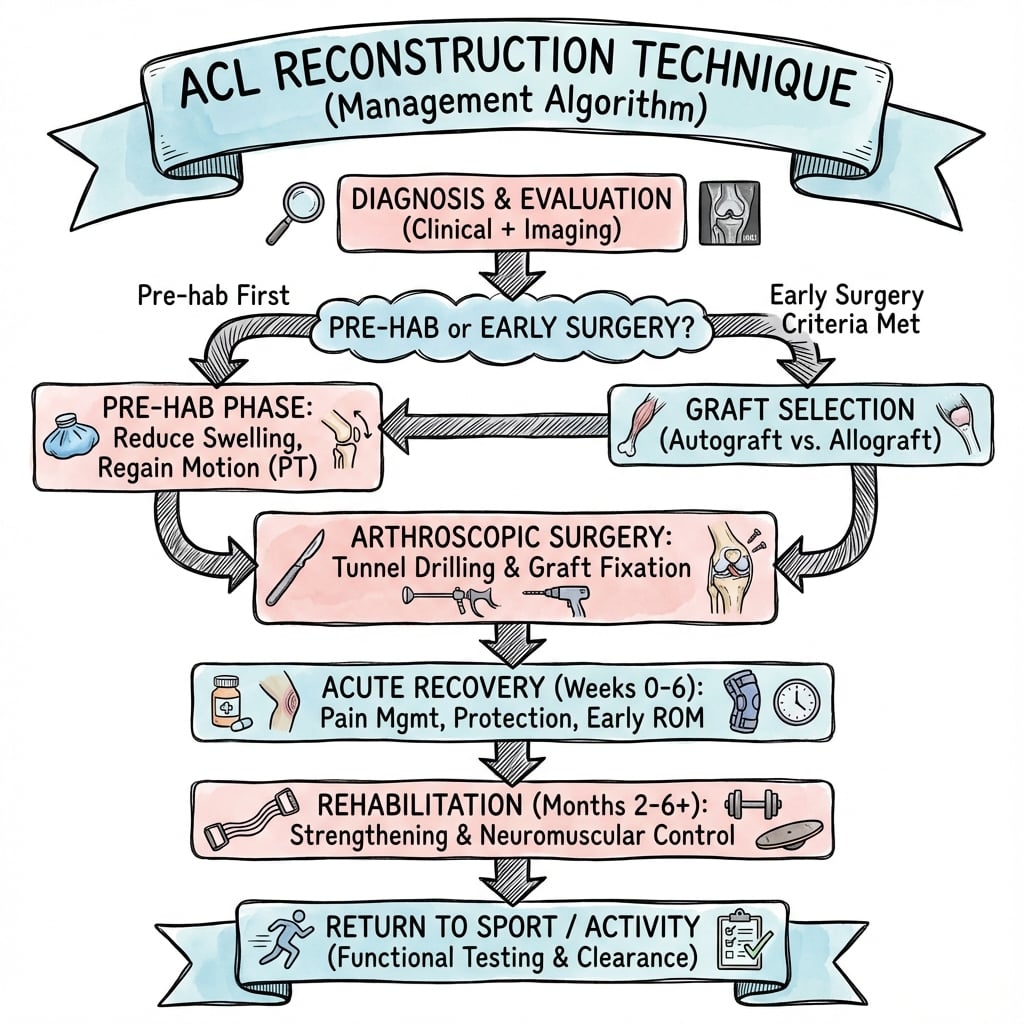
Anatomic reconstruction · Graft selection · Tunnel placement at the native footprints
- Anatomic reconstruction replicates the native ACL footprints — the femoral and tibial tunnel centres sit in the centre of the native insertion sites, not in an isometric or vertical position.
- Tunnel position is the most important technical factor determining stability, graft survival and return to sport.
- Femoral tunnel placed in the centre of the native AM/PL footprint, posterior to the resident's ridge (the anterior border of the footprint), at approximately 10 o'clock on a right knee (2 o'clock left knee).
- Tibial tunnel centred in the native footprint, posterior to the anterior horn of the lateral meniscus and lateral to the medial spine — too anterior placement causes roof impingement in extension.
- Graft selection (BTB versus hamstring versus quadriceps versus allograft) is individualised to patient factors and surgeon preference; graft diameter greater than 8mm matters more than graft type for failure risk.
When & Why
Indication. ACL reconstruction aims to restore knee stability and allow return to pre-injury activity. The modern operation is an anatomic reconstruction that places the graft in the centre of the native ACL footprints, in contrast to historical non-anatomic (isometric) techniques that placed the femoral tunnel more anterior and proximal. Most surgeons perform single-bundle reconstruction; double-bundle (separate anteromedial and posterolateral bundles) aims to replicate anatomy more closely but has not shown clear superiority in outcomes. Decide who to operate on. Reconstruction is offered when instability is symptomatic or when protecting other structures:
Symptomatic instability affecting activities of daily living, combined ligament injuries requiring surgery, and a repairable meniscal tear in an unstable knee (reconstruction improves meniscal healing).
Young active patient (25 years or younger), high-level athlete wanting return to pivoting sport, high-demand occupation, high-grade pivot shift, or a meniscal injury at high risk of further damage.
Significant established osteoarthritis, knee range of motion not yet restored, active infection, or unrealistic patient expectations. Manage these first.
Timing. The optimal window is 4 to 8 weeks post-injury, once full range of motion has been restored and the effusion has settled — operating too early (before regaining motion) raises the risk of arthrofibrosis. Not every acute tear needs early surgery: the KANON trial showed that a trial of structured rehabilitation, with delayed reconstruction reserved for ongoing instability, is a valid pathway in motivated patients. Who not to operate on. Low-demand patients, older sedentary individuals, those with no symptomatic instability who will modify activities, and partial tears with minimal laxity are managed non-operatively — RICE and protected weight-bearing in the acute phase (0 to 2 weeks), then progressive strengthening, proprioception and cycling through 2 to 12 weeks, with a functional brace and activity modification on return. Recurrent giving way despite a proper rehabilitation programme is the clearest signal to reconstruct. Graft selection — the one real choice. All autografts give comparable stability; the choice is individualised. Graft diameter greater than 8mm matters more than graft type.
- Advantages
- Bone-to-bone healing in the tunnels (faster, stronger integration); historical gold standard; some evidence of lower re-rupture in young athletes
- Disadvantages
- Anterior knee pain (up to 20 percent); kneeling pain; risk of patellar fracture and tendon rupture; fixed graft size
- Best use
- First-time reconstruction in young athletes when early return to high-level sport is the priority
- Advantages
- Less anterior knee pain; smaller incision; variable graft diameter (can be quadrupled)
- Disadvantages
- Soft-tissue-to-bone healing (slower); graft may be small (less than 8mm increases failure); some hamstring weakness; tunnel widening
- Best use
- First-time reconstruction, patients concerned about kneeling or at risk of anterior knee pain
- Advantages
- Full or partial thickness; bone-block option; good size; growing popularity
- Disadvantages
- Technically more demanding harvest; extensor mechanism morbidity (low)
- Best use
- An alternative autograft, increasingly used in primary and revision settings
- Advantages
- No donor-site morbidity
- Disadvantages
- Higher failure rate in young athletes; slower incorporation; small risk of disease transmission (rare with modern processing)
- Best use
- Best reserved for revision surgery or older, lower-demand patients
Address associated pathology at the same sitting. Meniscal tears accompany 40 to 60 percent of ACL injuries — repair is preferred over meniscectomy and reconstruction improves healing rates. Isolated MCL injury is managed non-operatively and the ACL reconstruction staged; LCL or posterolateral corner injury may require reconstruction. Chondral damage is debrided or treated with microfracture or osteochondral grafting as indicated. A lateral extra-articular tenodesis (LET) is added in high-risk young patients (see the STABILITY evidence below).
The Operation
The goal is to place a tendon graft anatomically — in the centre of the native femoral and tibial ACL footprints — and fix it under correct tension so it restores anteroposterior and rotational stability. The exposure is arthroscopic, working through standard knee portals with the graft harvested through small separate incisions. The relevant anatomy is laid out first, because tunnel placement is the whole operation.
Native anatomy you must reproduce. The ACL originates on the posteromedial aspect of the lateral femoral condyle and inserts on the anterior tibial plateau between the tibial spines. It has two functional bundles: - Anteromedial (AM) bundle — a more anterior and proximal femoral attachment; taut in flexion; the primary restraint to anterior tibial translation and the target that guides single-bundle reconstruction.
- Posterolateral (PL) bundle — a more posterior and distal femoral attachment; taut in extension; controls rotational stability and contributes to the pivot-shift phenomenon. The femoral footprint is semicircular and approximately 18 mm long. Its critical landmark is resident's ridge (the lateral intercondylar ridge), the bony ridge marking the anterior border of the footprint — the femoral tunnel is placed posterior to it. The tibial footprint is a broad oval depression (area approximately 120 to 150 mm²), sitting posterior to the anterior horn of the lateral meniscus and lateral to the medial tibial spine. The ACL's poor intrinsic healing — its blood supply is the middle genicular artery via the synovial membrane, and its mechanoreceptor-rich innervation is the posterior articular nerve — is why ruptures are reconstructed rather than repaired.
Operative sequence
- Supine with a thigh holder or lateral post so the knee can be flexed freely over the side of the table; a well-padded high-thigh tourniquet; the foot of the table dropped.
- Mark the landmarks and portal sites with the knee flexed: patella, patellar tendon, tibial tubercle, joint line and the proposed anterolateral and anteromedial portal positions.
- Confirm prepped graft options and that an adequate graft (greater than 8 mm once prepared) is feasible.
- Establish the anterolateral viewing portal just lateral to the patellar tendon at the level of the inferior pole of the patella — this is the primary viewing portal.
- Establish the anteromedial working portal just medial to the patellar tendon, under arthroscopic visualisation with a spinal needle to confirm trajectory; this portal must allow access to the notch and the femoral footprint.
- An accessory anteromedial or superomedial portal is often made for the transportal femoral guide; some surgeons use a transpatellar (central) portal.
- This portal arrangement is the exposure for the whole reconstruction — there is no open arthrotomy. Place portals precisely so instruments reach both footprints without clashing against the femur or the fat pad.
- Systematically inspect the patellofemoral joint, both compartments, both menisci (probe for tears) and the articular surfaces.
- Address meniscal and chondral pathology first — meniscal repair is done before tunnel drilling so the meniscal sutures and ACL tunnels do not interfere.
- Confirm the ACL rupture from within and grade the pivot shift and Lachman under anaesthesia.
- Excise the ruptured ACL stump, preserving the footprint remnants on the tibia and femur as landmarks for anatomic placement.
- Clear soft tissue and perform a notchplasty only if the notch is stenotic and would impinge the graft (avoid over-resection).
- Mark the centres of the native footprints — the femoral centre posterior to resident's ridge, the tibial centre behind the anterior horn of the lateral meniscus.
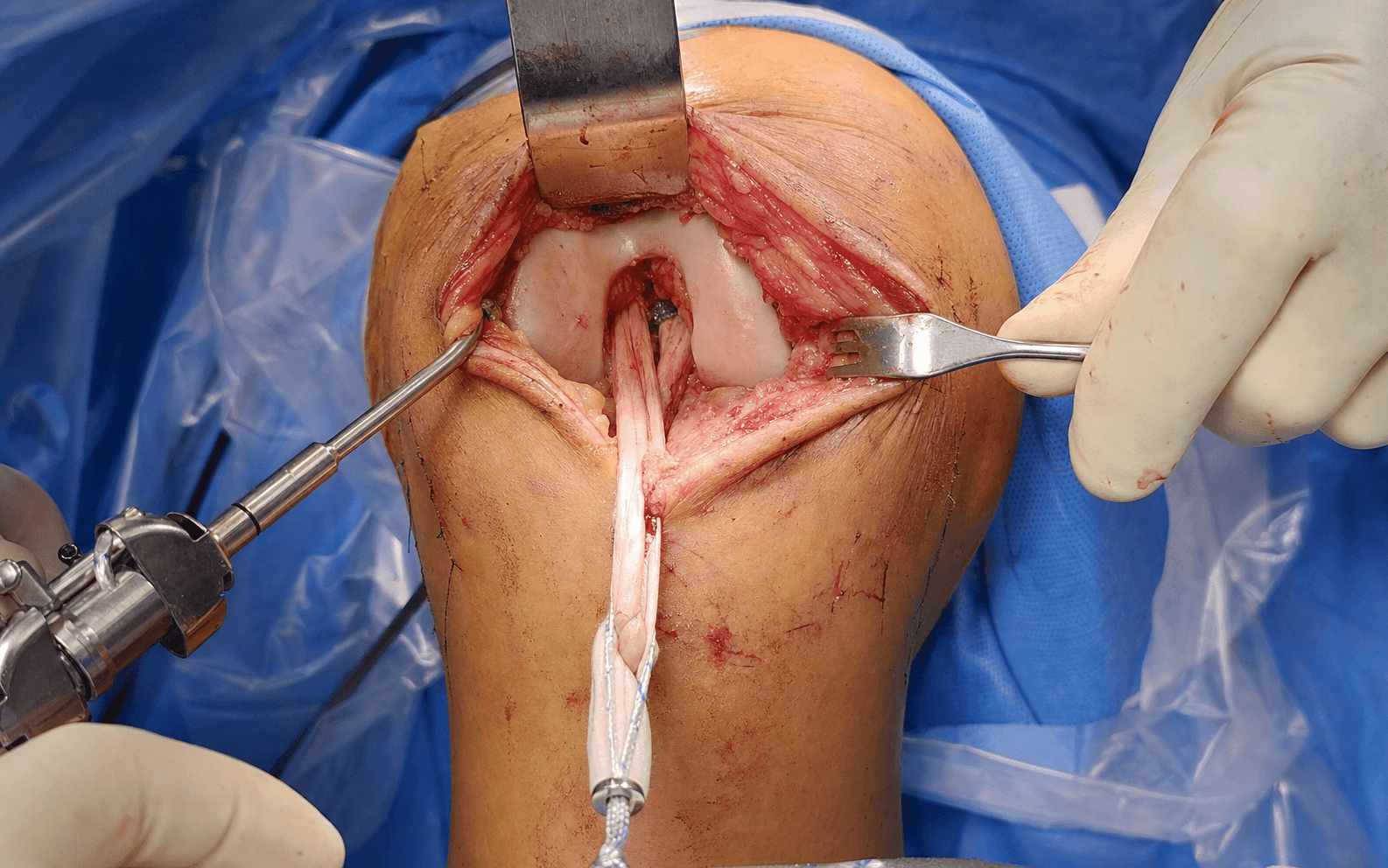
- BTB — a longitudinal incision over the patellar tendon; harvest the central third (usually 10 mm) with patellar and tibial bone blocks; preserve the paratenon and close the defect.
- Hamstring — a longitudinal incision over the pes anserinus on the anteromedial tibia; identify and harvest semitendinosus (and gracilis if needed for diameter) with an open-ended tendon stripper, leaving the distal insertion intact during harvest; protect the saphenous nerve.
- Size bone plugs (BTB) or whipstitch the tendon ends and size the diameter (hamstring); prepare to a quadrupled graft to reach a diameter greater than 8 mm.
- Mark the bone–tendon junction (BTB) and the rotation/demarkation lines so graft length in the tunnels can be confirmed after passage.
- Keep the graft moist on the back table under a tensioning board.
- Use a tibial aiming guide (usually 55 to 65 degrees), starting point on the anteromedial tibia medial to the tubercle.
- Target the centre of the native tibial footprint — posterior to the anterior horn of the lateral meniscus, lateral to the medial tibial spine, behind the intersection of the ACL stump remnant and the lateral meniscus.
- Avoid the common error — a tunnel placed too anterior causes roof impingement in extension and graft failure. Confirm guidewire position arthroscopically (and with fluoroscopy) before drilling.
- Transportal technique (current standard) — drill through the anteromedial portal with the knee hyperflexed to access the lateral wall; this gives the most anatomic position.
- Place the tunnel in the centre of the native footprint, posterior to resident's ridge, at approximately 10 o'clock on a right knee (2 o'clock left knee); avoid the vertical 12 o'clock position of older non-anatomic techniques.
- Alternatives: transtibial (drilled through the tibial tunnel — historical, may limit anatomic positioning) and outside-in (drilled from the lateral femoral cortex — allows independent positioning).
- Protect soft tissues and limit drill depth to avoid a posterior cortical blowout and lateral neurovascular injury.
- Pass a passing suture from tibia to femur (transportal or transtibial), then shuttle the graft from the tibial tunnel, through the joint, into the femoral tunnel.
- Orient the graft correctly (BTB bone plugs tracking the tunnels; hamstring maintaining its quadrupled configuration) and confirm it seats fully with the marked lines at the expected positions.
- Femoral fixation — suspensory (EndoButton, TightRope), interference screw, or cross-pin, depending on graft and tunnel.
- Tibial fixation — interference screw, with backup post or staple as required.
- Tension at 15 to 20 degrees of flexion — apply tension while cycling the knee through full flexion and extension several times to eliminate creep before final tibial fixation; confirm there is no impingement in extension and a firm endpoint.
- Wash, achieve haemostasis, close the portals and harvest incision in layers, and apply a compressive dressing with or without a hinged brace (surgeon preference).
- Check stability (negative Lachman and pivot shift) and full extension before waking the patient; begin early range-of-motion and quadriceps activation on day one.
- Tibial tunnel too anterior is the commonest technical error — it causes roof impingement in extension, graft failure and loss of extension. Keep the centre posterior to the anterior horn of the lateral meniscus and confirm full extension free of impingement before final fixation.
- Femoral tunnel too vertical or anterior abandons the anatomic footprint and compromises rotational control — target posterior to resident's ridge.
- Graft diameter less than 8 mm roughly doubles revision risk (MOON data). Quadruple the hamstring or add gracilis/quadriceps to reach a diameter greater than 8 mm, especially in young patients.
- Avoid operating before range of motion is restored, and use a criteria-based return-to-sport pathway to reduce re-rupture.
For a single-bundle graft the femoral tunnel sits in the centre of the native footprint, posterior to resident's ridge, at approximately 10 o'clock on a right knee and 2 o'clock on a left knee. Avoid the vertical 12 o'clock position — that is the legacy non-anatomic placement that fails to control rotation.
The most common tibial tunnel error is placing it too anterior. This produces roof impingement in extension, graft wear and failure, and a fixed extension deficit. The correct centre is posterior to the anterior horn of the lateral meniscus, lateral to the medial spine, behind the intersection of the ACL stump and the lateral meniscus.
Aftercare & Complications
Rehabilitation progresses through four phases on a criteria-based pathway rather than a fixed calendar.
- Timing
- 0–2 weeks
- Goals
- Protect graft; control pain and swelling; restore full extension; reach 90 degrees flexion
- Key exercises & restrictions
- Quadriceps sets, straight-leg raises, heel slides, passive extension to 0 degrees, patellar mobilisation, ice and compression. Partial weight-bearing with crutches, weight-bearing as tolerated by 2 weeks
- Timing
- 2–6 weeks
- Goals
- Full range (0–130 degrees); normal gait; progressive strengthening
- Key exercises & restrictions
- Closed-kinetic-chain work (mini squats, leg press), stationary cycling, pool exercises, core work. Full weight-bearing without crutches by 4–6 weeks. No open-chain extension 0–45 degrees, no running or jumping
- Timing
- 6–12 weeks
- Goals
- Strength to 70 percent of the other side; single-leg balance; begin sport-specific drills
- Key exercises & restrictions
- Progressive resistance, balance and proprioception, light jogging after 12 weeks, non-contact sport-specific drills
- Timing
- 4–9 months
- Goals
- Criteria-based return — strength, hops and psychology all passing
- Key exercises & restrictions
- Non-contact training from 4–6 months, full contact practice 6–9 months, competition 9–12 months depending on level
Return to sport is criteria-based, not time-based. The modern benchmarks are a quadriceps strength index greater than 90 percent of the contralateral side, a hop-test battery greater than 90 percent, an ACL-RSI psychological readiness score greater than 70, and completion of sport-specific training without symptoms. Around 85 to 90 percent of well-selected patients return to sport, with graft survival of about 85 to 90 percent at 10 years. Functional scores (IKDC, Lysholm) typically improve from around 50 to the mid-80s, though the Tegner activity level often sits one to two levels below pre-injury. Long-term, 50 to 70 percent develop radiographic osteoarthritis by 15 to 20 years (less often symptomatic); meniscal injury at the index event is the major driver.
- BTB
- 5–8 percent
- Hamstring
- 8–12 percent
- Interpretation
- BTB slightly lower, especially in the young
- BTB
- 15–20 percent
- Hamstring
- 5–10 percent
- Interpretation
- Lower with hamstring
- BTB
- 20–30 percent
- Hamstring
- 5–10 percent
- Interpretation
- Lower with hamstring — relevant for tradespeople
- BTB
- Approximately 5 percent
- Hamstring
- Approximately 5 percent
- Interpretation
- Similar
- BTB
- Excellent
- Hamstring
- Excellent
- Interpretation
- Comparable overall; meta-analyses show no significant difference in laxity, pivot-shift or revision
Complications. Recognise them early — most late failures trace back to tunnel position, graft size or premature return to sport.
- Recognition
- Loss of posterior cortex on drilling; graft migration
- Prevention
- Hyperflex for transportal drilling; visualise the posterior wall before over-drilling
- Management
- Convert to outside-in or two-stage; ensure secure fixation
- Recognition
- Frayed or clamped graft during passage
- Prevention
- Avoid clamping; gentle passage; size tunnels to the graft
- Management
- Discard and prepare a new graft if compromised
- Recognition
- Lateral femoral drill exit; peroneal or saphenous signs
- Prevention
- Protect soft tissues; limit drill depth; careful positioning
- Management
- Vascular repair if injured; saphenous neuropraxia usually recovers
- Recognition
- Tense swollen knee in first days
- Prevention
- Meticulous haemostasis
- Management
- Aspiration if tense; rule out infection
- Recognition
- 0.5–1 percent incidence; pain, fever, effusion
- Prevention
- Aseptic technique; prophylactic antibiotics
- Management
- Aggressive irrigation and debridement; retain graft if possible
- Recognition
- Calf pain, swelling, dyspnoea
- Prevention
- Thromboprophylaxis and early mobilisation
- Management
- Anticoagulation per protocol
- Recognition
- 5–15 percent; recurrent instability, positive pivot shift
- Prevention
- Anatomic tunnels; graft greater than 8mm; criteria-based return; LET in high risk
- Management
- Revision ACL reconstruction (often staged)
- Recognition
- 5–10 percent; stiff knee, flexion contracture
- Prevention
- Avoid early surgery before motion returns; controlled rehab
- Management
- MUA, arthroscopic lysis of adhesions
- Recognition
- 5–10 percent; mechanical block to terminal extension
- Prevention
- Posterior tibial tunnel; check extension intra-operatively
- Management
- Arthroscopic excision of the cyclops lesion — good outcomes
- Recognition
- 20–30 percent, more with soft-tissue grafts
- Prevention
- Secure, aperture-type fixation; avoid graft motion
- Management
- Usually asymptomatic; relevant at revision (staged bone grafting)
Revision reconstruction succeeds in 75 to 85 percent — lower than primary, with higher failure in revision-of-revision, often requiring staged procedures (bone grafting widened tunnels first) and consideration of lateral extra-articular augmentation.
Viva & Exam Focus
REARREAR — femoral tunnel landmarks
LMBLMB — tibial tunnel landmarks
Anatomic placement in the centre of the native footprint, posterior to resident's ridge. Transportal (or outside-in) technique. Clock face 10 o'clock right knee, 2 o'clock left knee. Avoid posterior blowout and the vertical 12 o'clock position.
Centre in the native footprint, posterior to the anterior horn of the lateral meniscus, behind the ACL-stump–lateral-meniscus intersection. Too anterior equals roof impingement in extension. Use a 55–65 degree guide.
Bone-to-bone healing in the tunnels (faster integration). Higher anterior knee pain and kneeling pain. Some evidence of lower re-rupture in young athletes. Fixed graft size.
Soft-tissue-to-bone healing (slower). Less anterior knee pain. Needs a minimum diameter greater than 8 mm (quadruple, add gracilis). May leave some hamstring weakness and tunnel widening.
Placing the tunnel too anterior. This causes roof impingement in extension, leading to graft failure, loss of extension and anterior knee pain.
8 mm. MOON cohort data show grafts less than 8 mm have significantly higher failure and revision rates — in patients 18 years or younger, revision was 18.3 percent with grafts 8 mm or smaller versus 0 percent above 8 mm. Always ensure adequate graft size.
A bony ridge on the lateral femoral wall marking the anterior border of the native ACL femoral footprint. The femoral tunnel is placed posterior to this landmark.
10 o'clock for a right knee, 2 o'clock for a left knee. This is the centre of the native footprint and avoids the vertical 12 o'clock position of older non-anatomic techniques.
15 to 20 degrees of flexion. Cycle the knee several times through flexion and extension to eliminate creep before final fixation.
Viva scenarios
Practise clinical reasoning and management decisions out loud
“Describe your technique for ACL reconstruction in a 22-year-old footballer.”
“A 35-year-old tradesman who works on his knees needs ACL reconstruction. How do you counsel him about graft choice?”
“Six months after ACL reconstruction your patient has a persistent loss of terminal extension. What is your approach?”
Femoral tunnel
- Centre of the native footprint
- Posterior to resident's ridge (anterior border of the footprint)
- 10 o'clock right knee, 2 o'clock left knee
- Transportal or outside-in technique
Tibial tunnel
- Posterior to the anterior horn of the lateral meniscus
- Behind the ACL-stump–lateral-meniscus intersection
- Too anterior equals roof impingement in extension
- 55–65 degree guide angle
Graft options
- BTB: bone-to-bone healing, more anterior knee pain
- Hamstring: less donor morbidity, slower soft-tissue healing
- Minimum diameter greater than 8 mm
- All autografts give comparable stability
Fixation & rehab
- Femoral: suspensory or interference
- Tibial: interference screw
- Tension at 15–20 degrees flexion, cycle to remove creep
- Criteria-based return to sport at 9–12 months
Background & Evidence
Epidemiology. Population studies across high-income countries report roughly 30 to 80 ACL reconstructions per 100,000 person-years, with rates rising fastest in adolescents. The peak age is 15 to 25 years, and in the same pivoting sports females have a two- to three-fold higher rate than males (anatomical, hormonal and neuromuscular factors). High-risk sports include football (soccer), basketball, netball, handball, rugby, Australian rules football and alpine skiing. A second ACL injury — graft rupture or contralateral tear — occurs in 15 to 20 percent of athletes under 25 returning to pivoting sport. Neuromuscular warm-up programmes (FIFA 11+, PEP, netball KNEE programmes) reduce non-contact ACL injury by approximately 50 percent and are endorsed internationally. ACL injury classification guides who is reconstructed.
- Description
- Mild stretch, fibres intact
- Clinical features
- Pain, minimal laxity, negative Lachman
- Management
- Non-operative
- Description
- Partial tear, some fibres intact
- Clinical features
- Moderate laxity, soft endpoint
- Management
- Variable — trial non-operative versus reconstruction
- Description
- Complete rupture
- Clinical features
- Positive Lachman and pivot shift
- Management
- Reconstruction in active patients
Clinical assessment. The Lachman test (20–30 degrees flexion) is the most sensitive (85–95 percent); the anterior drawer (90 degrees flexion) is less sensitive (40–50 percent); the pivot shift is the most specific for rotational instability (35–95 percent); and the Lever Sign is a useful adjunct (80–90 percent). Lachman is graded by translation: grade 1 (3–5 mm), grade 2 (5–10 mm), grade 3 (greater than 10 mm). A non-contact pivoting mechanism, a palpable pop (around 70 percent), and immediate haemarthrosis within 4–6 hours (contrast with the delayed effusion of a meniscal injury) are the hallmark history. Imaging. Plain radiographs (AP, lateral, skyline) are usually normal acutely, but a Segond fracture (avulsion of the lateral tibial plateau rim) is pathognomonic, as is a tibial spine avulsion in adolescents. Pre-operatively assess notch width (a narrow notch raises impingement risk), alignment and any established arthritis. MRI is the gold standard: primary signs are non-visualisation or discontinuity of the fibres and abnormal (horizontal) orientation; the classic secondary sign is the bone-bruise pattern of kissing contusions on the lateral femoral condyle and posterolateral tibial plateau. CT is reserved for revision planning (tunnel position and size), and stress radiographs (KT-1000/2000, side-to-side difference greater than 3 mm significant) provide objective translation. Associated injury patterns.
- Components
- ACL only
- Frequency
- 30 percent
- Components
- ACL plus medial or lateral meniscus
- Frequency
- 40–60 percent
- Components
- ACL plus medial collateral ligament
- Frequency
- 20 percent
- Components
- ACL plus MCL plus medial meniscus
- Frequency
- 10 percent
- Components
- ACL plus PCL, with or without collaterals
- Frequency
- 5 percent
Global society guidance and registry evidence. There is broad international consensus on the principles:
- Position or finding
- Clinical practice guideline supports reconstruction to restore stability in active patients; autograft favoured over allograft in the young
- Position or finding
- Anatomic reconstruction, individualised graft choice, consider anterolateral augmentation in high-risk knees
- Position or finding
- Structured rehabilitation pathway; reconstruction for symptomatic instability or to protect a repairable meniscus
- Position or finding
- Criteria-based return to sport; minimum graft diameter and anatomic tunnels emphasised
- Position or finding
- Hamstring autograft carried a higher revision rate than patellar tendon in young patients
- Position or finding
- Allograft and small-diameter hamstring grafts associated with higher revision, especially under 21
- Position or finding
- Autograft outperforms allograft at revision; meniscal and chondral status drive long-term outcome
AAOS, ESSKA/ISAKOS, AOSSM and BOA/BASK converge on anatomic reconstruction, autograft in the young, graft diameter greater than 8 mm, criteria-based return to sport, and selective lateral extra-articular augmentation in high-risk patients.
FIFA 11+, PEP and sport-specific neuromuscular programmes reduce non-contact ACL injury by approximately 50 percent and are promoted globally.
Key evidence. The STABILITY trial (Getgood, 2020) showed that adding a lateral extra-articular tenodesis to hamstring ACL reconstruction in patients 25 years or younger cut graft rupture from 11 percent to 4 percent at two years (relative risk reduction approximately 67 percent; number-needed-to-treat 14) and reduced composite clinical failure from 40 percent to 25 percent — the basis for adding LET in high-risk young knees. The MOON cohort (Mariscalco, 2013) established graft diameter as a dominant failure risk: revision in 0 percent of grafts greater than 8 mm versus 7 percent at 8 mm or smaller. The KANON trial (Frobell, 2010) showed that structured rehabilitation with delayed reconstruction is a valid pathway, and the Chen meta-analysis (2020) confirmed BTB and hamstring give comparable stability with less anterior knee pain for hamstring. The MOON autograft risk calculator (Marmura, 2021) supports shared decision-making, favouring BTB or hamstring-plus-LET over isolated hamstring in high-risk young athletes.
References
Lateral Extra-articular Tenodesis Reduces Failure of Hamstring ACL Reconstruction: 2-Year Outcomes From the STABILITY Study
- Multicentre RCT of 618 patients aged 25 years or under at high risk of failure
- Adding LET (iliotibial band strip) to single-bundle hamstring ACLR cut graft rupture from 11 percent to 4 percent at 2 years (relative risk reduction approximately 67 percent)
- Composite clinical failure (rupture or persistent rotatory laxity) fell from 40 percent to 25 percent
- Number-needed-to-treat with LET to prevent one rupture was 14.3 over 2 years
The Influence of Hamstring Autograft Size on Patient-Reported Outcomes and Risk of Revision After ACL Reconstruction (MOON Cohort)
- 263 primary hamstring ACLRs from the prospective MOON cohort
- Revision occurred in 0 percent of grafts greater than 8 mm versus 7.0 percent of grafts 8 mm or smaller (p equals 0.037)
- In patients 18 years or under, revision was 18.3 percent with grafts 8 mm or smaller versus 0 percent above 8 mm
- Each 1 mm increase in diameter improved KOOS and IKDC subjective scores
A Randomized Trial of Treatment for Acute Anterior Cruciate Ligament Tears (KANON)
- 121 young active adults with acute ACL tears randomised to early reconstruction plus rehab versus rehab with optional delayed reconstruction
- No difference in KOOS4 at 2 years (between-group difference 0.2 points)
- 61 percent of the optional-delayed group avoided surgery without worse outcomes
- Supports a trial of structured rehabilitation in selected patients
Patellar Tendon Versus 4-Strand Semitendinosus and Gracilis Autografts for ACL Reconstruction: Meta-analysis of RCTs With Mid- to Long-Term Follow-Up
- 9 RCTs, 630 patients, minimum 5-year follow-up
- No significant difference in laxity, Lachman, pivot-shift, re-rupture, revision or osteoarthritis
- Significantly less anterior knee pain with hamstring (STG) grafts (p equals 0.003)
- Kneeling-pain difference did not reach significance but trended toward hamstring
Validation of a Risk Calculator to Personalize Graft Choice and Reduce Rupture Rates for ACL Reconstruction
- MOON autograft risk calculator validated externally on the STABILITY 1 RCT dataset
- Age, high-grade preoperative laxity and graft type were the strongest predictors of rupture
- BPTB and addition of LET to hamstring were protective versus isolated hamstring autograft
- Supports avoiding isolated hamstring autograft in young, active patients