Advanced Pelvic Surgery | High-Risk Neurovascular Structures | Expert Level
- Rarely used approach - most SI pathology managed posteriorly or percutaneously
- Primary indication: irreducible posterior SI disruption needing open anterior reduction; also failed posterior fixation, revision arthrodesis and prominent anterior hardware
- L5 nerve root/lumbosacral trunk at extreme risk - crosses the sacral ala roughly 2cm medial to the SI joint, directly in the operative corridor
- Iliac vessels cross operative field - major vascular injury possible
- Requires excellent knowledge of lumbosacral plexus anatomy
When & Why
What it exposes. The anterior approach gives direct access to the anterior sacroiliac joint, the sacral ala and the inner table of the ilium for open reduction and plating of posterior SI joint disruptions that cannot be reduced closed, and for selected revision arthrodesis or anterior hardware problems. Access is via the lateral (iliac) window of the ilioinguinal approach, or a modified Stoppa, elevating iliacus off the inner table to reach the anterior SI joint and sacral ala. Why anterior (and not posterior or percutaneous). Most SI pathology is now managed posteriorly or percutaneously because those routes are simpler, safer and give better screw purchase. The anterior approach is reserved for the small subset that need direct visualisation of the anterior joint and the L5 nerve root, placement of an anterior column plate from ilium to sacrum, or address of anterior soft-tissue problems such as scarring or nerve entrapment. It is technically demanding and not a routine exposure - reserve it for complex revision cases performed by experienced pelvic surgeons. Indications.
- Irreducible posterior SI disruption needing open anterior reduction (the classic absolute indication)
- Failed posterior SI fusion with pseudarthrosis and persistent instability in a high-demand patient
- Revision SI arthrodesis after posterior-only fusion has failed
- Prominent anterior SI screws or hardware causing nerve compression or vascular compromise, requiring removal
- Selected anterior column / pelvic ring ORIF in vertical-shear (APC III, LC III) injuries with anterior SI disruption
- L5 nerve root decompression (compressed by callus, hardware or scar) and excision of heterotopic ossification around the joint Relative indications and contraindications. Relative: tumour resection involving the anterior SI joint. Avoid the anterior approach when posterior or percutaneous fixation is feasible, in active infection over the field, when the patient is unfit for prolonged complex pelvic surgery, in severe obesity (BMI more than 40), after pelvic radiotherapy (poor tissue quality), or in marked osteoporosis (poor screw purchase). Pre-operative assessment. Document baseline L5 (extensor hallucis longus, ankle dorsiflexion, dorsal foot sensation) and S1 (ankle plantarflexion, sole sensation) function carefully - these are the roots at risk and the baseline against which any post-operative deficit is judged. Image with an AP pelvis, inlet and outlet views (a Ferguson view - AP with 30 degrees of cephalad tilt - best shows the SI joint), a fine-cut CT (1mm slices) with 3D reconstruction to define joint morphology, nonunion, bone quality and hardware position, and MRI where infection, nerve entrapment or marrow oedema are in question; consider CT angiography in scarred revisions to map aberrant iliac anatomy. Position, setup and equipment. Supine on a radiolucent table, with a bump under the ipsilateral buttock (15-20 degrees) and the hip slightly flexed and externally rotated to open the joint; arms tucked or out on boards; C-arm access from multiple angles is essential. General anaesthesia with muscle relaxation, arterial line for revisions, tranexamic acid 1g at induction, broad-spectrum antibiotics, cell saver and 4-6 units crossmatched with vascular surgery on standby. Surface landmarks are the ASIS and pubic tubercle (the two anchors of the ilioinguinal incision), the inguinal ligament, the iliac crest (graft harvest site), and the midline (umbilicus to pubis) for the Stoppa alternative; the SI joint itself lies deep and is localised with fluoroscopy.
- What to have ready
- Anterior SI plates and 3.5mm pelvic reconstruction plates; 4.5mm lag screws for joint compression; cannulated 7.0-7.3mm screws if percutaneous augmentation added; iliac crest autograft or allograft (femoral head, cancellous chips)
- What to have ready
- Hohmann, malleable and visceral retractors; fine nerve dissectors, vessel loops and a nerve stimulator for the L5/trunk; pelvic reduction clamps; curettes and osteotomes for joint preparation; headlamp for deep pelvic exposure; vascular instruments available
- What to have ready
- Fluoroscopy (C-arm, essential); cell saver; 4-6 units PRBC crossmatched; vascular surgery backup on standby; neurosurgical backup if nerve decompression needed; nerve stimulator to identify the L5/lumbosacral trunk
The Exposure
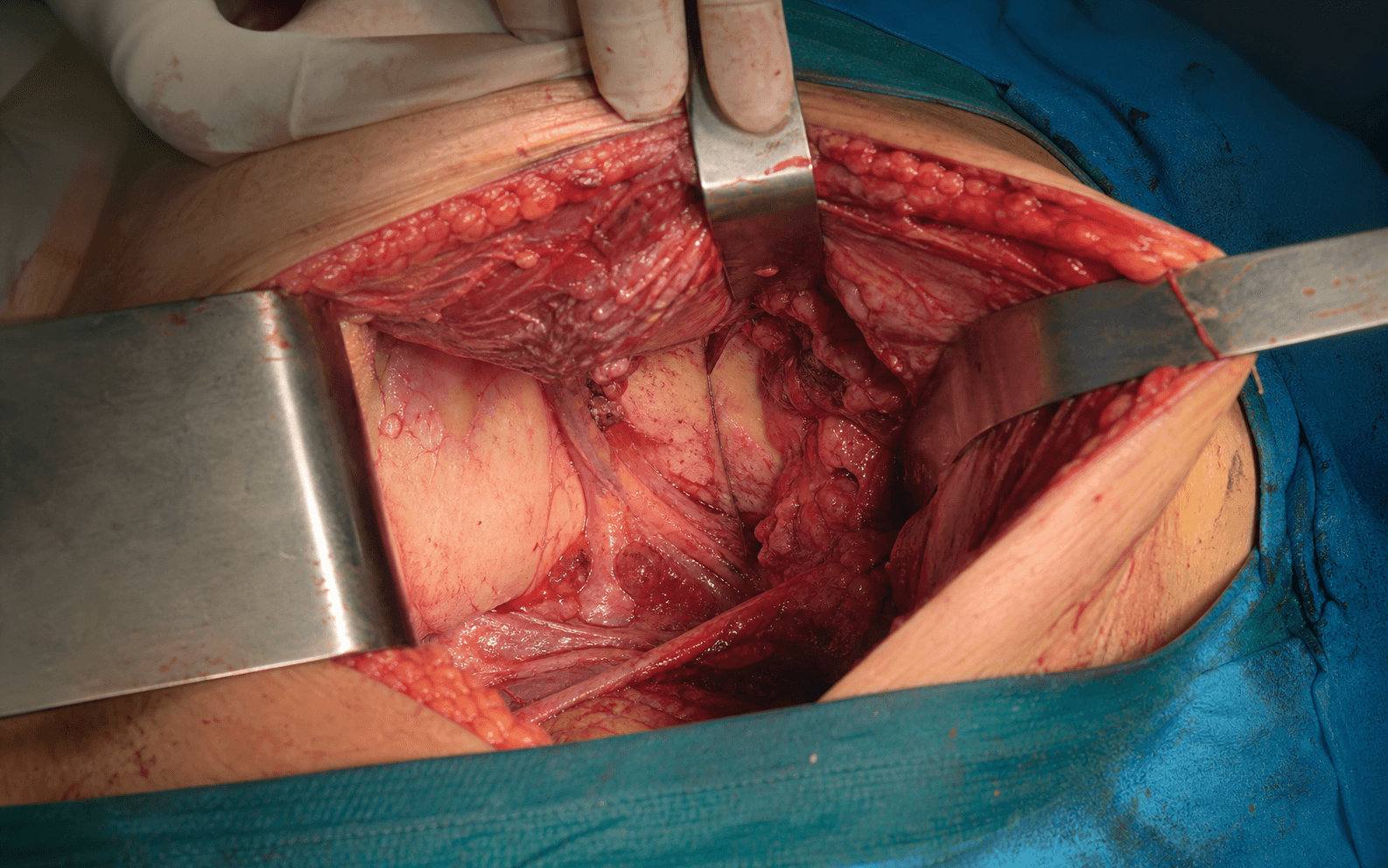
Work through the ilioinguinal exposure in layers, developing the lateral then the middle window, mobilising the iliac vessels medially and shielding the L5/lumbosacral trunk before opening the joint lateral to it.
Exposure sequence
- Begin about 2cm medial and superior to the ASIS, curve along the iliac crest for 6-8cm, then curve medially and inferiorly toward the pubic tubercle (15-20cm total; extend to a Pfannenstiel if wider exposure is needed).
- Incise through skin and subcutaneous tissue to the external oblique aponeurosis; the approach develops three windows (lateral, middle, medial).
- Incise the external oblique along the iliac crest and elevate the iliacus subperiosteally off the inner table of the ilium.
- Identify and protect the lateral femoral cutaneous nerve; expose the inner pelvic brim. This window exposes the iliac wing (for graft) but rarely the SI joint itself, which lies too medial.
- Identify the femoral nerve on the lateral border of psoas and the iliac vessels running on psoas across the pelvic brim.
- Mobilise the iliac vessels medially (ligating small branches, using vascular tapes, avoiding excess traction) and retract the psoas laterally; this window opens access to the sacral ala and the anterior SI joint.
- The L5 ventral ramus joins a small S1 contribution to form the lumbosacral trunk, which runs over the anterior sacral ala roughly 2cm medial to the SI joint, covered only by fascia and psoas/iliacus fibres - the joint is lateral to the nerve and the ala is medial.
- Palpate the ala and identify the trunk as a firm cord about 5-8mm across; a nerve stimulator confirms it (foot dorsiflexion at low voltage).
- Protect it by keeping all dissection on the joint/iliac side, placing a blunt malleable or Hohmann retractor between the nerve and the joint, retracting medially only as much as necessary with periodic release, and keeping cautery and drill off the ala.
- With the trunk shielded medially and the iliac vessels safeguarded, palpate the SI joint through its thin anterior capsule lateral to the nerve (ala medial, ilium lateral; the joint runs obliquely, superior-medial to inferior-lateral).
- Confirm position with fluoroscopy (AP and outlet), mark with a K-wire, then make a longitudinal capsulotomy with stay sutures for later repair.
- Curette all cartilage from both surfaces down to bleeding subchondral bone and fenestrate the subchondral bone with a small drill to encourage fusion.
- Pack the joint with iliac crest autograft and reduce it with pelvic clamps, compressing in an anterior-to-posterior direction.
- Contour a 3.5mm pelvic reconstruction plate from the ilium (lateral) across the joint onto the sacral ala (medial), lying on the anterior capsule.
- Reconfirm the L5/lumbosacral trunk position before any drilling; place iliac screws (4-6) and sacral-ala screws (2-4) aiming for the S1 body under fluoroscopy, avoiding the L5/S1 foramen. Alternatively use 2-3 iliosacral screws crossing the joint.
- Release all retractors and inspect the L5/lumbosacral trunk (intact, normal appearance; the stimulator confirms function) and the iliac vessels (no injury, good flow).
- Image in AP, inlet, outlet and lateral to confirm reduction, hardware position and no foraminal or canal encroachment.
- Repair the anterior SI joint capsule with 0-Vicryl and reconstruct the pelvic floor if disrupted; ensure the iliac vessels lie in anatomic position.
- Close the external oblique and transversalis fascia (1-0 Vicryl), place a deep drain (19Fr Blake), then close Scarpa's fascia (2-0 Vicryl) and skin.
The L5 nerve root within the lumbosacral trunk is the structure most at risk: it lies on the sacral ala roughly 2cm medial to the joint, so medial dissection over the ala, retractors on the ala, or sacral screws placed too far medially cause an L5 deficit and foot drop. The iliac vessels lie within the operative field and must be mobilised medially to reach the joint - they are friable, especially in scarred revision cases, and a tear of the common iliac vein is life-threatening. Have vascular surgery on standby, use gentle blunt dissection only, keep all work lateral to the nerve on the joint side, and confirm the trunk with a stimulator before any drilling.
This is not a classical internervous-plane approach - it is an extensile ilioinguinal or Stoppa exposure that depends on mobilising the iliac vessels and shielding the lumbosacral trunk. That is exactly why it is reserved for experienced pelvic surgeons and only for joints that cannot be reduced closed or for revision cases.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- L5 nerve root / lumbosacral trunk (about 2cm medial to the joint)
- Protection
- Keep dissection off the ala; blunt malleable retractor shield; nerve stimulator; no medial screws or cautery on the ala
- Structure at risk
- Common, internal and external iliac vessels
- Protection
- Gentle medial mobilisation; vascular backup; proximal and distal control ready; blunt dissection only
- Structure at risk
- L5 and S1 roots, lumbosacral trunk, obturator nerve
- Protection
- Minimise medial retraction over the ala; periodic retractor release
- Structure at risk
- Bowel and bladder (adhesions in revision cases)
- Protection
- Careful dissection; general surgery backup if recognised
- Structure at risk
- Lateral femoral cutaneous nerve
- Protection
- Identify and protect when elevating iliacus off the inner table
Intra-operative complications. The feared complications are L5/lumbosacral trunk injury - the commonest neurological problem, reported in up to about 5 percent in some series, usually a traction neuropraxia that recovers over 6-18 months but with permanent foot drop after complete transection reported - and iliac vessel injury (uncommon but potentially fatal haemorrhage, most often from the common iliac vein). Lumbosacral plexus injury and bowel or bladder injury (from adhesions in revision cases) are rare (each less than 1 to 3 percent). Quoted rates come from small, heterogeneous series and should be quoted as ranges, not precise figures. Managing an iliac vessel injury. Apply direct pressure with a pack for at least five minutes and do not lift it to look; call vascular surgery and activate the massive transfusion protocol (1:1:1 PRBC to FFP to platelets, tranexamic acid, calcium) through two large-bore cannulae and an arterial line. Extend the exposure (medially to a Stoppa or to a full laparotomy if needed) and gain proximal and distal control. A small tear (less than 1cm) is repaired with lateral venorrhaphy using 5-0 or 6-0 Prolene; a large or complex injury needs a patch venoplasty (saphenous vein or PTFE) or an interposition graft (femoral vein or PTFE), and ligation of the common iliac vein is a last resort that is acceptable in an unstable patient because collateral flow is usually adequate, at the cost of leg oedema managed with compression stockings. Internal iliac vein ligation is better tolerated than common iliac ligation. If the patient is in extremis despite resuscitation, pack the pelvis, close rapidly and return to theatre in 24-48 hours for definitive repair. Post-operatively, monitor in ICU for re-bleeding, thrombosis and compartment syndrome, with serial haemoglobin and distal perfusion checks. Extensile options and alternatives. Extend medially from the ilioinguinal to a modified Stoppa for more medial joint and ala access; the lateral window extends proximally along the iliac crest for graft and iliac-wing control. For most primary SI pathology the safer alternatives are percutaneous iliosacral screws (Routt) or a posterior open approach, which avoid this neurovascular corridor entirely. Closure and post-operative surveillance. Repair the capsule and pelvic floor, restore the iliac vessels to anatomic position, and close in layers over a deep drain. Post-operatively, watch in ICU with neurological checks every two hours for 24 hours (L5 and S1 function versus the documented baseline), protect with toe-touch weight bearing for 6-8 weeks, advance to partial then full weight bearing by 10-12 weeks if radiographs progress, and assess fusion with CT at 6-12 months. Outcome correlates strongly with the quality of reduction; revision arthrodesis carries a guarded prognosis.
Procedures Through This Approach
- Open reduction and anterior plating of an irreducible posterior SI disruption (ilium-to-sacrum plate) - the classic indication.
- Revision SI arthrodesis after failed posterior fusion (joint preparation, bone graft, anterior plate).
- Removal of prominent anterior SI screws or hardware causing nerve or vascular compromise.
- Anterior column / pelvic ring ORIF in unstable vertical-shear or LC III injuries.
- L5 nerve root decompression (callus, hardware or scar) and excision of heterotopic ossification around the joint.
- Selected tumour resection involving the anterior SI joint.
Viva & Exam Focus
ANTERIORANTERIOR - the exposure sequence
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old man had posterior SI fusion 18 months ago for chronic SI joint pain after a pelvic fracture. He has persistent pain and CT confirms a nonunion. You are considering an anterior approach to the SI joint. What are the risks and how would you counsel him?”
“During an anterior approach to the SI joint you accidentally tear the common iliac vein, causing massive haemorrhage. How do you manage this?”
Indications (rare - last resort)
- Irreducible posterior SI disruption needing open anterior reduction
- Failed posterior SI fusion / revision arthrodesis
- Removal of prominent anterior SI hardware
- Most SI pathology is managed posteriorly or percutaneously, not anteriorly
- Reserve for complex revision cases only
Critical anatomy
- L5/lumbosacral trunk crosses the sacral ala about 2cm medial to the joint (highest-risk structure); the joint is lateral to the nerve
- Iliac vessels lie in the operative field and must be mobilised and protected
- Lumbosacral plexus at risk during deep medial dissection over the ala
- SI joint runs oblique (superior-medial to inferior-lateral); ala medial, ilium lateral
- Access via the lateral window of the ilioinguinal approach or a modified Stoppa
Surgical steps
- Modified ilioinguinal incision (ASIS to pubic tubercle)
- Elevate iliacus off the inner table; mobilise the iliac vessels medially in the field
- Identify and protect the lumbosacral trunk on the ala, medial to the joint
- Expose the anterior SI joint lateral to the nerve; keep dissection off the ala
- Joint preparation (curette cartilage, bone graft) if fusion
- Anterior plate ilium-to-sacrum, or iliosacral screws
Complications (high risk - quote as ranges)
- L5/lumbosacral trunk injury: foot drop; commonly a recoverable traction neuropraxia
- Iliac vessel injury: uncommon but potentially life-threatening haemorrhage
- Lumbosacral plexus injury: multiple nerve deficits possible
- Nonunion/malreduction: outcome driven by quality of reduction
- Infection: higher than percutaneous techniques
- Chronic pain: common after revision arthrodesis (guarded prognosis)
Post-operative care
- ICU monitoring (high-risk case)
- Neurological checks every 2 hours for 24 hours (L5, S1 function)
- Toe-touch weight bearing 6-8 weeks
- Full weight bearing at 10-12 weeks if healing
- Fusion assessment: CT at 6-12 months
- Realistic expectations: outcome driven by quality of reduction
References
Internal fixation of pelvic ring fractures
- Four-year comparison of skeletal traction/sling, anterior external fixation and internal fixation for unstable pelvic ring injuries
- Reduction and stable fixation promoted union in a satisfactory position and improved clinical results
- Foundational description of operative reduction and fixation of the pelvic ring, including open anterior exposures
- Established that displaced posterior ring injuries benefit from anatomic reduction and stable fixation
Techniques for reduction and posterior fixation through the anterior approach
- Describes open reduction and fixation of the SI joint through an anterior (iliac) approach
- Stated absolute indication: posterior SI joint disruption, with or without iliac wing fracture, that cannot be reduced by closed techniques
- Anterior fixation allows accurate, stable reduction while avoiding the soft-tissue wound problems of posterior open approaches
- Two-hole or three-hole anterior plates applied across the joint from ilium to sacral ala provide direct visual reduction
Iliosacral screw fixation: early complications of the percutaneous technique
- Prospective consecutive series of 177 patients with unstable pelvic ring disruptions treated with percutaneous iliosacral screws
- No posterior infections and minimal blood loss; complications were due to imaging quality, surgeon error and fixation failure
- Five screws were misplaced by surgeon error; one misplaced screw caused a transient L5 neuropraxia
- Two sacral nonunions required debridement, grafting and repeat fixation; quality triplanar fluoroscopy is essential for safe screw placement
Anterior pelvic plating and sacroiliac joint fixation in unstable pelvic ring injuries
- 32 patients with unstable pelvic ring injuries, mean follow-up 51 months
- Functional results: 16 excellent, 10 good, 4 moderate, 2 poor; 2 poor results had residual neurologic symptoms after moderate reduction
- Radiological reduction: 16 anatomic, 9 nearly anatomic, 7 moderate; all healed except 3 pubic ramus nonunions
- Complications: 3 screw loosenings, 2 anterior plate breakages, 1 postoperative infection