Medial parapatellar arthrotomy — the workhorse exposure for total knee arthroplasty
- The medial parapatellar arthrotomy is the standard, most versatile exposure for total knee arthroplasty.
- It is not a true internervous plane — the arthrotomy passes through or adjacent to the vastus medialis obliquus (VMO) insertion on the patella.
- The patella is everted laterally to display the whole joint; a lateral retinacular release is added only if eversion is tight.
- The saphenous nerve and great saphenous vein are at risk with distal extension along the medial tibia — stay anterior to them.
- The pes anserinus (Sartorius, Gracilis, Semitendinosus) is the key distal landmark, marking access to the MCL.
When & Why
What it exposes. The anteromedial approach gives broad, familiar access to the entire knee joint — the distal femur, proximal tibia and patella — plus the medial compartment, the medial collateral ligament (MCL) and the medial meniscus. Its medial parapatellar variant is the gold-standard exposure for total knee arthroplasty (TKA), primary and revision. Why this approach. The medial parapatellar arthrotomy is reproducible, extensile in both directions, and gives excellent visualisation for component placement; it allows patellar eversion and tolerates the stiff, obese or revision knee better than the muscle-sparing alternatives. The muscle-sparing subvastus and midvastus variants trade some exposure for theoretical early-recovery benefit (see The Exposure). Indications. - Total knee arthroplasty — primary and revision (the dominant use)
- Unicompartmental (medial) knee arthroplasty via a mini-medial parapatellar incision
- Medial tibial plateau fractures — ORIF of Schatzker I to IV (extended anteromedial)
- MCL repair or reconstruction — acute or chronic
- ACL reconstruction — hamstring graft harvest, tibial and femoral tunnel drilling
- Open medial meniscus repair or meniscectomy
- Tibial eminence fracture fixation in adults
- Loose body removal from the medial compartment
- Arthrotomy for infection — irrigation and debridement
- Synovectomy for inflammatory arthropathy Anteromedial mini-incision vs medial parapatellar. The small anteromedial (mini) incision stays lateral to the VMO and gives limited exposure — it is used for arthroscopy portals, meniscal surgery and ACL work. The medial parapatellar (standard TKA) incision extends through the VMO tendon, allows patellar eversion, and gives full joint exposure for arthroplasty: more extensile, but it disrupts the VMO insertion. Position & landmarks. Supine, with the knee flexed to 90 degrees over the edge of the table or in a leg holder; the foot of the bed is dropped so the hip and ankle move freely, and a bump under the hip holds neutral rotation. A thigh tourniquet at 250 to 300 mmHg gives a bloodless field. Palpate and mark the patella, the patellar tendon, the tibial tubercle (the distal extent of the incision), the medial femoral condyle, the medial joint line (level with the inferior pole of the patella) and the VMO muscle belly superomedially.
The Exposure
Work from skin to capsule along the medial border of the patella, complete the medial parapatellar arthrotomy, then evert the patella laterally to deliver the joint. This is not a true internervous plane — the arthrotomy deliberately passes through or adjacent to the VMO insertion.
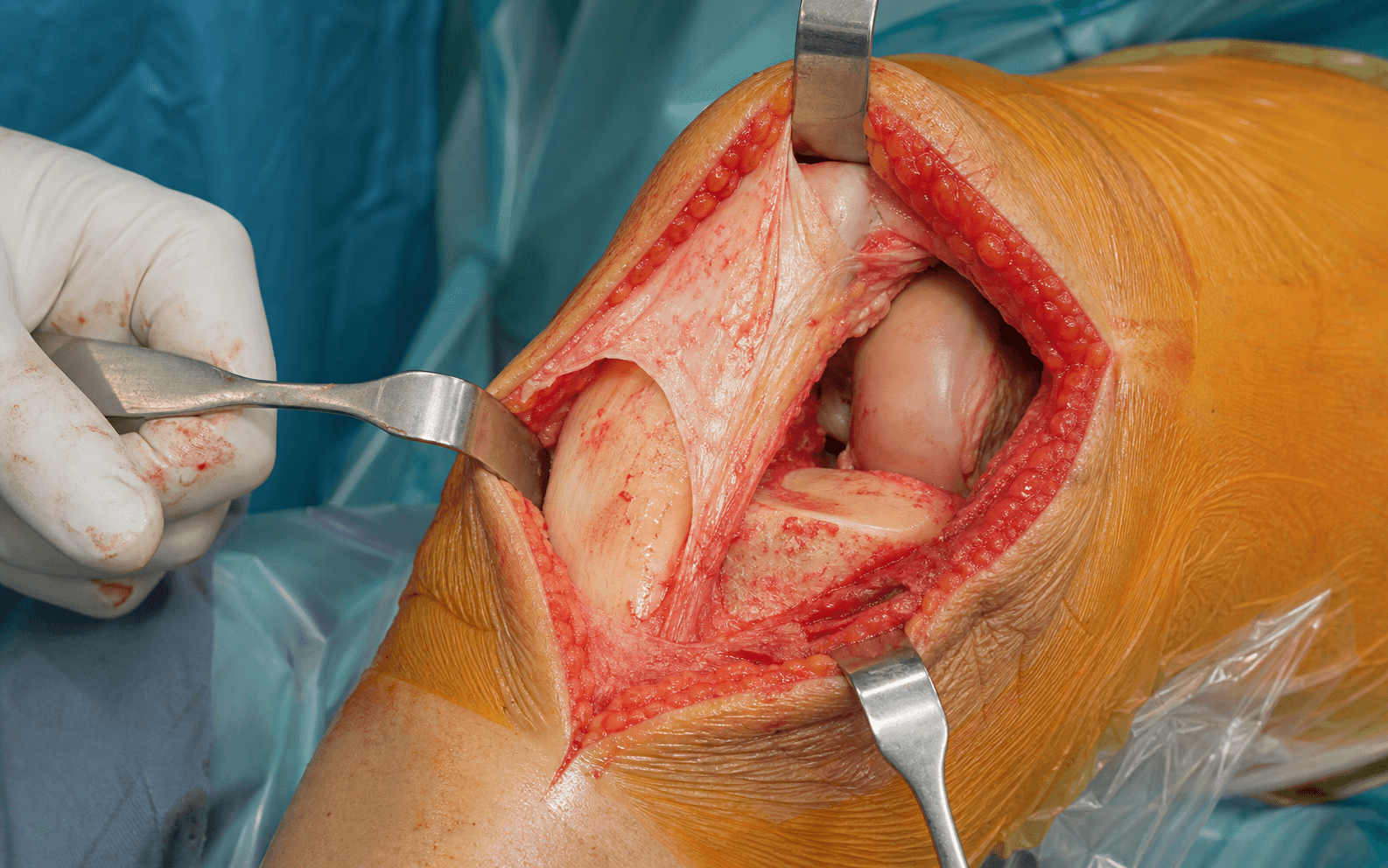
Medial parapatellar arthrotomy — dissection sequence
- A midline or slightly medial (anterior midline) skin incision from about 5 cm above the patella down to the tibial tuberosity.
- Mark the patella borders before incision; raise full-thickness flaps to avoid devascularising thin skin.
- Through subcutaneous fat (saphenous vein branches, prepatellar bursa) to the quadriceps tendon and medial retinaculum.
- Define the medial border of the patella and the patellar tendon — the line of the arthrotomy.
- Incise the capsule starting proximally in the quadriceps tendon (this may split the VMO near its insertion on the patella), continue along the medial border of the patella, then medial to the patellar tendon down to the tibial tubercle — the classic "quad tendon, medial patella, medial to patellar tendon" path.
- Protect the patellar tendon throughout; partial excision of the infrapatellar fat pad improves exposure.
- Release the soft-tissue attachments and evert the patella laterally, then flex the knee to 90 degrees to present the joint.
- If the patella will not evert comfortably, perform a lateral retinacular release; avoid forceful eversion (patellar tendon avulsion risk).
- Partial fat pad excision, lateral retinacular release for a tight extensor mechanism.
- For the stiff or revision knee, escalate to a proximal quadriceps snip (oblique incision in the VMO/quad tendon) or a tibial tubercle osteotomy rather than force exposure.
- Repair the capsule and VMO/quadriceps tendon meticulously with heavy suture (number 1 Vicryl or Ethibond), deep dermis with 2-0 Vicryl, and skin with staples, subcuticular or Monocryl.
- Test patellar tracking with the trial components — there must be no lateral subluxation in extension before final closure; drain only if there is significant ooze.
- Description
- Standard TKA arthrotomy through or near the VMO insertion
- Best indication
- Primary and revision TKA (gold standard)
- Description
- Dissects beneath the VMO off the intermuscular septum — muscle-sparing
- Best indication
- TKA in selected (thin, good ROM) patients
- Description
- Splits the VMO — a compromise between exposure and muscle sparing
- Best indication
- TKA where moderate exposure suffices
- Description
- Limited anteromedial exposure, stays lateral to VMO
- Best indication
- UKA, selected TKA, meniscal surgery
- Description
- Arthroscopic portal at the joint line, just medial to the patellar tendon
- Best indication
- Arthroscopy, ACL reconstruction
- Description
- Distal extension along the subcutaneous border of the tibia
- Best indication
- Medial plateau fractures, MCL work
- Medial parapatellar
- Disrupted
- Subvastus
- Preserved
- Midvastus
- Partially preserved
- Medial parapatellar
- Excellent
- Subvastus
- Limited
- Midvastus
- Moderate
- Medial parapatellar
- Easiest
- Subvastus
- Most difficult
- Midvastus
- Intermediate
- Medial parapatellar
- N/A
- Subvastus
- Higher (5 to 15 percent)
- Midvastus
- Lower
- Medial parapatellar
- Suitable
- Subvastus
- Difficult
- Midvastus
- Limited
- Medial parapatellar
- Excellent
- Subvastus
- Excellent
- Midvastus
- Excellent
The infrapatellar branch of the saphenous nerve crosses the field about 2.8 cm distal to the inferior pole of the patella and is encountered in essentially every standard medial parapatellar arthrotomy — transection is near-universal, leaving a usually well-tolerated numb patch anterolateral to the incision (counsel preoperatively). The patellar tendon can avulse if the patella is forcefully everted in a stiff knee. With distal extension, the saphenous nerve and great saphenous vein are at risk along the medial tibia.
In a stiff, obese or revision knee, resistance to eversion is the moment the patellar tendon avulses (0.17 to 1.0 percent of primary TKAs). A lateral retinacular release, then a quadriceps snip, then a tibial tubercle osteotomy is the safe escalation — convert exposure before you convert a complication.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Saphenous vein branches
- Protection
- Careful haemostasis; full-thickness flaps
- Structure at risk
- Infrapatellar branch of saphenous nerve (crosses about 2.8 cm distal to the inferior pole)
- Protection
- Stay close to the patella; expect transection — counsel the patient preop
- Structure at risk
- Medial inferior genicular artery (along the medial joint line)
- Protection
- Coagulate as encountered during capsulotomy
- Structure at risk
- Patellar tendon (avulsion at the inferior pole)
- Protection
- Never force eversion; snip or osteotomise instead
- Structure at risk
- Saphenous nerve and great saphenous vein (run together, posteriorly)
- Protection
- Stay anterior; identify and protect before deep work
- Structure at risk
- MCL superficial fibres; pes anserinus tendons
- Protection
- Controlled distal extension; protect during MCL/plateau work
Extensile options. - Distally — extend along the subcutaneous border of the medial tibia for medial plateau ORIF and MCL exposure. The saphenous nerve accompanies the great saphenous vein posteriorly, so stay anterior; the pes anserinus is the landmark and the MCL can be exposed from epicondyle to tibial insertion.
- Proximally — extend in the line of the quadriceps tendon.
- Quadriceps snip — an oblique incision in the VMO/quadriceps tendon for the stiff or revision knee; lengthens the extensor mechanism to gain eversion without avulsion.
- Tibial tubercle osteotomy — a flat osteotomy of the tubercle (with its distal periosteal hinge or as a free fragment fixed with screws) for severe stiffness or exposure in complex revision; the planned salvage for a knee that will not evert. Closure. Meticulous repair of the capsule and quadriceps mechanism (number 1 Vicryl or Ethibond) restores the extensor mechanism and patellar tracking; the medial meniscus and coronary ligament are respected, and the fat pad is only partially excised. A subcuticular or stapled skin closure over a drain (if ooze is significant) completes the case. Complications.
- Incidence / detail
- 30 to 70 percent symptomatic; branch transected in about 100 percent of standard arthrotomies
- Prevention or management
- Usually well-tolerated — counsel every patient preop
- Incidence / detail
- 0.17 to 1.0 percent of primary TKAs (higher in stiff, RA, revision)
- Prevention or management
- Never force eversion; snip or osteotomise; immediate repair if it occurs
- Incidence / detail
- 2 to 5 percent
- Prevention or management
- Lateral release, meticulous VMO repair, test tracking with trial
- Incidence / detail
- 3 to 7 percent
- Prevention or management
- Physiotherapy, manipulation under anaesthesia if needed
- Incidence / detail
- 1 to 2 percent
- Prevention or management
- Careful tension-free closure, no thin flaps
- Incidence / detail
- 2 to 3 percent
- Prevention or management
- Meticulous haemostasis; drain if ooze
- Incidence / detail
- 1 to 2 percent each (with prophylaxis)
- Prevention or management
- Aseptic technique, antibiotics, VTE prophylaxis protocol
- Incidence / detail
- 1 to 5 percent
- Prevention or management
- Stay anterior during distal extension
Procedures Through This Approach
- Total knee arthroplasty (primary and revision) — the principal operation; revision may need a quadriceps snip or tibial tubercle osteotomy for exposure.
- Unicompartmental (medial) knee arthroplasty through a mini-medial parapatellar incision.
- Medial tibial plateau fracture ORIF (Schatzker I to IV) via the extended anteromedial variant.
- MCL repair or reconstruction, and multiligament reconstruction combined with an anterolateral approach.
- ACL reconstruction — hamstring graft harvest and tibial/femoral tunnel drilling (anteromedial portal or small incision).
- Open medial meniscus repair or meniscectomy (coronary ligament release aids meniscal access).
- Tibial eminence fracture fixation, loose body removal, synovectomy and arthrotomy for infection.
Viva & Exam Focus
SGSPes anserinus — superficial to deep
Hook:Say Grace before Tea (Sartorius, Gracilis, SemiTendinosus)
Standard TKA arthrotomy. Incision through or adjacent to the VMO insertion on the patella, then along the medial patellar border and medial to the patellar tendon. Familiar, reproducible and extensile.
For TKA the patella is everted laterally to expose the joint. Add a lateral retinacular release only if tight. Subvastus and midvastus avoid splitting the quadriceps mechanism.
At risk with distal medial extension. The saphenous nerve accompanies the great saphenous vein along the medial knee and leg — stay anterior. Injury causes medial leg numbness.
The approach gives access to the medial collateral ligament for repair or imbrication. The pes anserinus (Sartorius, Gracilis, Semitendinosus) is the distal landmark.
The arthrotomy uses the interval between the medial border of the patellar tendon and the VMO, from the medial patellar margin along the medial patellar tendon border to the tibial tubercle; the medial retinaculum and capsule are incised to enter the joint, and the coronary ligament may be released for meniscal access. The medial inferior genicular artery runs along the medial joint line, and the MCL superficial fibres are divided in some approaches.
Placed just medial to the patellar tendon at the joint line with the knee flexed 90 degrees; transillumination helps avoid vessels. It gives working access to the medial compartment, ACL graft passage, a good tibial-tunnel angle and meniscal suture placement, but visualisation is more limited than the lateral portal and the infrapatellar branch is at risk.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the medial parapatellar approach to the knee for total knee arthroplasty.”
“You are performing a TKA via the subvastus approach in a 62-year-old man (BMI 34, ROM 0-125 degrees). After dissecting under the VMO and entering the joint, the patella will only partially evert and you cannot safely position your femoral cutting guides; a lateral retinacular release does not help. How do you proceed?”
“During a primary TKA via the medial parapatellar approach in a 71-year-old woman with only 75 degrees of preoperative flexion, you apply traction to evert a tight patella (despite a lateral retinacular release) and feel a 'give': the patellar tendon has avulsed from the inferior pole of the patella with a small bone fragment, 20 minutes into the case before any bone cuts. How do you manage this?”
Medial parapatellar arthrotomy
- Quad tendon, medial patella, medial to patellar tendon
- Through or near the VMO insertion
- Evert patella laterally; lateral release if tight
- Not a true internervous plane
Variations
- Subvastus: under VMO, muscle-sparing
- Midvastus: splits VMO
- Mini: lateral to VMO for UKA/portal work
Structures at risk
- Infrapatellar branch of saphenous nerve (often transected, about 2.8 cm distal to pole)
- Saphenous nerve and great saphenous vein with distal extension
- Patellar tendon (avulsion if forced)
- Medial inferior genicular artery at the joint line
Extensile options
- Distal extension along medial tibia (stay anterior to saphenous)
- Quadriceps snip for the stiff/revision knee
- Tibial tubercle osteotomy for severe stiffness
Pes anserinus (SGS)
- Sartorius (superficial)
- Gracilis (middle)
- Semitendinosus (deep)
References
Subvastus vs medial parapatellar approach: systematic review and meta-analysis of RCTs
- 20 RCTs, 1893 primary TKRs pooled
- Subvastus gave earlier active straight-leg raise (mean 1.7 days sooner), lower day-1 pain and greater early ROM
- Subvastus required fewer lateral retinacular releases and slightly less blood loss but added ~10 min operative time
- No difference in Knee Society Score at 6 weeks or 1 year, and no difference in infection, DVT or stiffness
Mini-subvastus vs medial parapatellar approach in primary TKA: meta-analysis
- 14 RCTs, 1172 patients pooled
- Mini-subvastus gave higher total Knee Society Score, fewer days to straight-leg raise and less blood loss
- Better ROM at 4-6 weeks, 3 months and 6 months with mini-subvastus
- No difference in functional KSS, length of stay, wound complications, DVT or PE
Mini-midvastus vs mini-medial parapatellar approach in TKA: meta-analysis
- 5 RCTs, 190 mini-midvastus vs 189 mini-medial parapatellar knees
- No significant difference in Knee Society Score at 1 and 2 years
- No difference in ROM, incision length or lateral retinacular release rate
- Statistically (but not clinically) less blood loss and shorter surgery favouring mini-midvastus
Incidence of encountering the infrapatellar branch of the saphenous nerve during a midline TKA approach
- 73 patients (76 knees) undergoing primary TKA via standard medial parapatellar arthrotomy
- Infrapatellar branch identified in 100% of knees
- Mean 2.82 cm distal to the inferior pole of the patella where it crossed the patellar tendon
- Location not predicted by sex, height or BMI - it lies within the typical arthrotomy
Knee replacement for osteoarthritis (review of outcomes and dissatisfaction)
- TKR is highly effective for end-stage knee OA with excellent reoperation and cost-effectiveness data
- A significant minority of patients remain dissatisfied despite a technically sound replacement
- Patient factors and expectations strongly influence perceived outcome
- Outcome should be measured with patient-reported as well as clinical scores