Two-stage cell therapy for large focal cartilage defects — hyaline-like repair with durable 10–20 year results
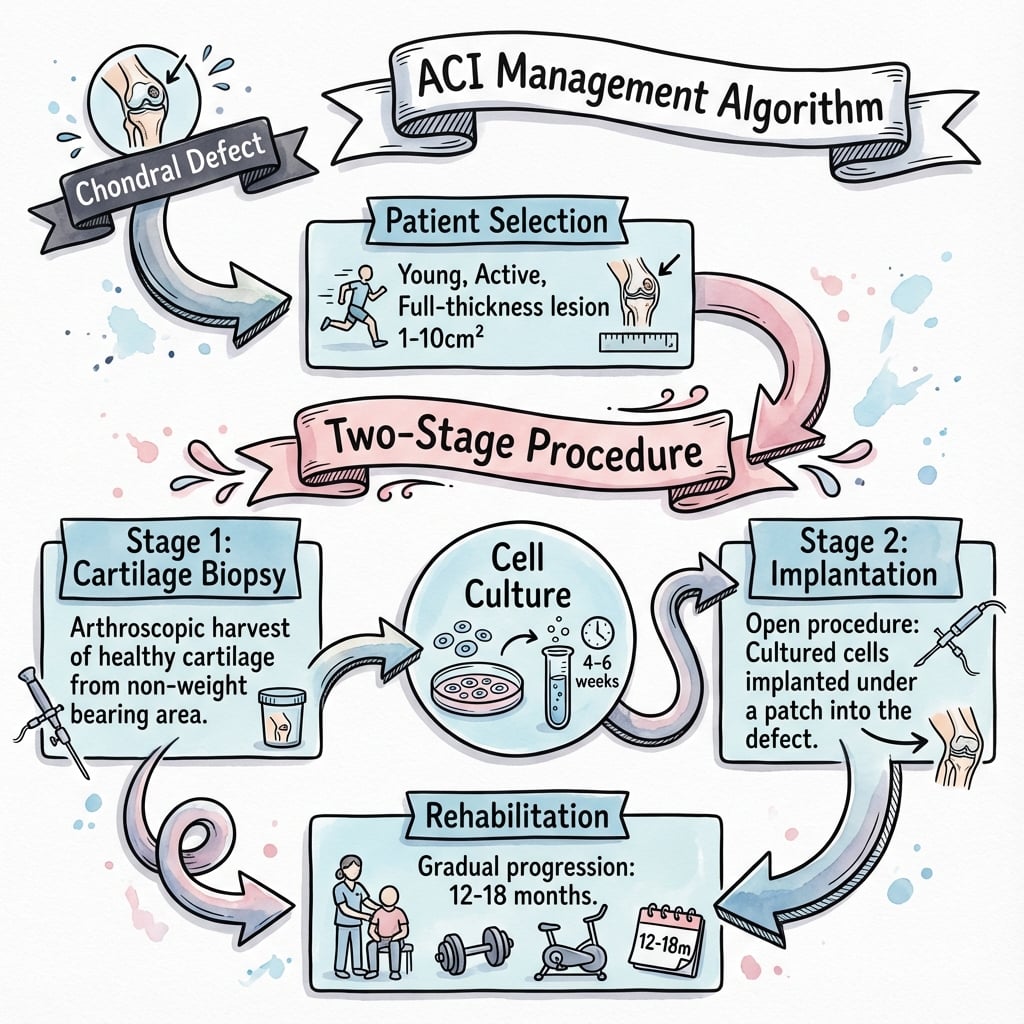
- Two-stage procedure — Stage 1 biopsy, 4–6 weeks of cell culture, then Stage 2 implantation
- ACI/MACI produces hyaline-like cartilage with predominantly Type II collagen, biomechanically superior to microfracture fibrocartilage
- Minimal donor morbidity — only a small (200–300mg) biopsy from a non-weight-bearing area
- Durable long term — benefit maintained at 10–20 years, unlike microfracture which deteriorates at 2–5 years
- MACI (third generation) is the current standard — cells seeded on a collagen scaffold, fixed with fibrin glue, no suturing
When & Why
Indication. ACI/MACI is the biological cartilage repair of choice for large focal chondral or osteochondral defects, typically over 2cm², where marrow stimulation (microfracture) gives poor durability and osteochondral transfer (OATS) is limited by donor capacity. The classic candidate is a young, active patient (typically under 45–50) with a symptomatic full-thickness (ICRS grade 3–4) lesion of the femoral condyle or trochlea, intact subchondral bone, and an otherwise healthy joint, who has failed or is unsuited to simpler options.
- Large lesions over 2cm² (especially over 4cm²) - Failed prior microfracture or OATS - Young, active patients (typically under 45) - Single or multiple focal defects - Full-thickness cartilage damage (ICRS grade 3–4)
- Diffuse osteoarthritis - Inflammatory arthropathy - Uncorrected malalignment - Meniscal deficiency (unless addressed) - Kissing (bipolar) lesions — relative - Age over 55 — relative
ACI/MACI is the gold standard for large cartilage lesions (over 2cm²) where microfracture outcomes are poor and OATS donor capacity is limited. Knowing the generations of ACI, the two-stage nature, and the long-term outcomes is high-yield for examination.
Clinical assessment. Take a focused history of prior cartilage surgery (failed microfracture or OATS), symptom duration, mechanical symptoms (catching, locking), activity level and sport demands, and crucially the patient's willingness to commit to two operations and a 12–18 month rehabilitation. On examination look for effusion, compartment-localised tenderness, crepitus, limb alignment, and ligament and meniscal integrity — every concurrent problem that could jeopardise the graft must be identified and planned for. Investigations.
Work-up before ACI
- Weight-bearing AP, lateral, Rosenberg (PA flexed) and skyline views
- Assess alignment, joint-space narrowing and established OA — diffuse disease excludes ACI
- Map every lesion: size, location and depth
- Assess subchondral bone status
- Identify associated meniscal and ligament pathology
- Full-length standing films to quantify the mechanical axis
- Plan a concurrent or staged osteotomy if deviation is significant
MRI identifies all cartilage lesions for treatment planning. Unlike OATS — limited by donor supply — ACI can address multiple lesions at one implantation, so every defect that needs treating should be mapped now.
Treatment selection by lesion size. Defect size is the single biggest driver of technique choice.
- First choice
- Microfracture
- Alternative
- OATS
- Notes
- ACI is usually unnecessary
- First choice
- OATS or ACI
- Alternative
- Either is reasonable
- Notes
- Patient factors decide
- First choice
- ACI / MACI
- Alternative
- Osteochondral allograft (OCA)
- Notes
- OATS donor limit exceeded
- First choice
- ACI / MACI
- Alternative
- Staged OATS
- Notes
- ACI can treat all lesions at once
Correct everything that will fail the graft. Malalignment, ligament instability and meniscal deficiency must be corrected — concurrently or staged — or the repair will fail. When malalignment is present, the staging matters:
- Timing
- HTO or DFO, then ACI after 6–12 months
- Rationale
- Lets the correction heal; simpler staged procedures
- Timing
- Both at one surgery
- Rationale
- One anaesthetic, but technically demanding
- Timing
- Biopsy during HTO, implant later
- Rationale
- Reduces total operations to two
ACI requires real commitment: two operations, a 4–6 week wait for cell culture, and a 12–18 month rehabilitation. Confirm the patient understands and accepts this timeline before offering it; non-compliant patients are poor candidates.
The Operation
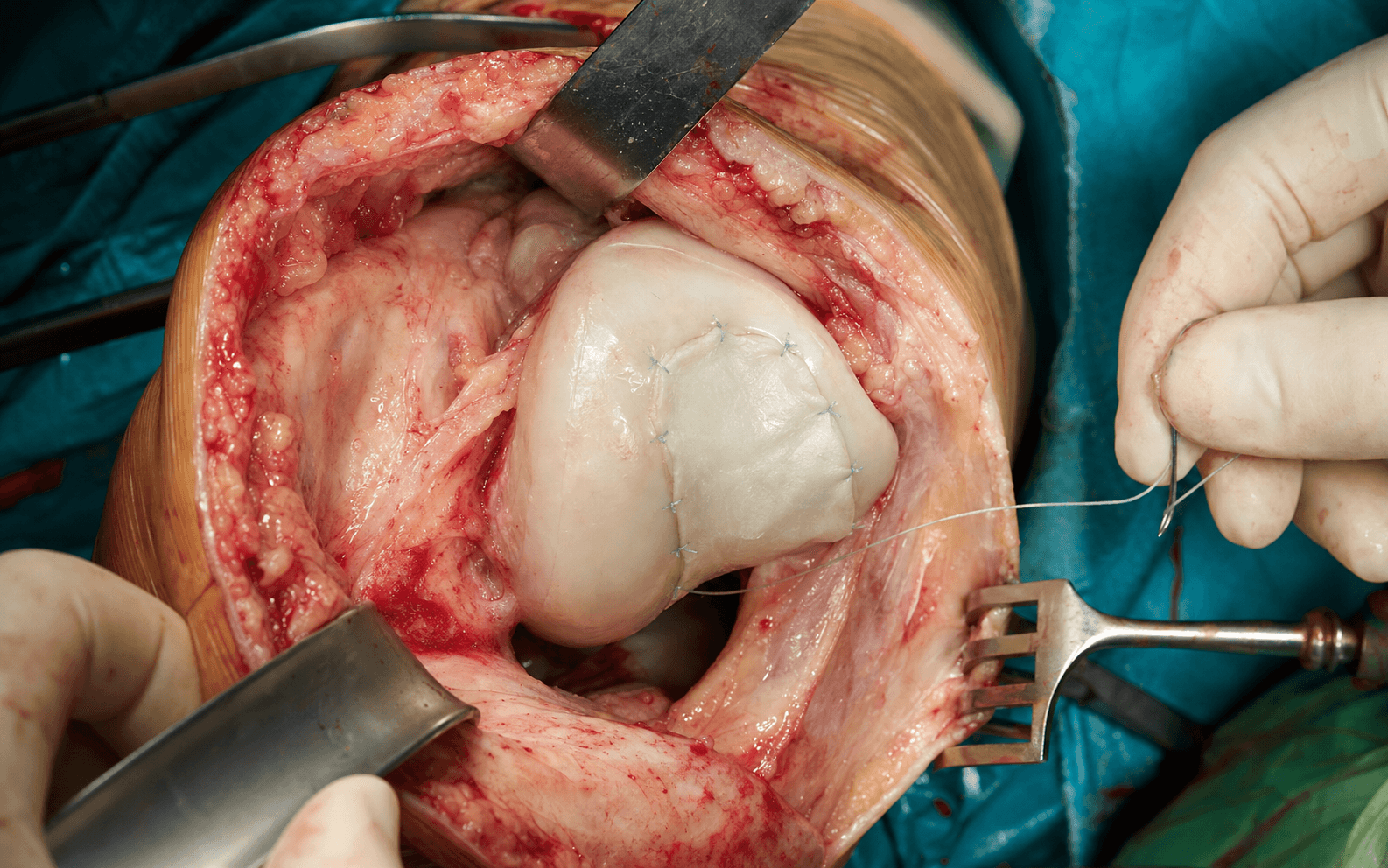
ACI is a two-stage biological repair. Stage 1 harvests a small cartilage biopsy, which is expanded in culture for 4–6 weeks; Stage 2 implants the expanded cells — most often as a cell-seeded collagen scaffold (MACI) — into the prepared defect. The implantation stage is where the operative craft lives: a clean exposure, a contained defect with stable shoulders, an exactly templated scaffold placed cell-side down, and fibrin-glue fixation confirmed stable through a full range of motion.
How ACI compares with the alternatives.
- ACI / MACI
- Two
- Microfracture
- One
- OATS
- One
- ACI / MACI
- Hyaline-like (Type II)
- Microfracture
- Fibrocartilage (Type I)
- OATS
- Hyaline (Type II)
- ACI / MACI
- Over 2cm²
- Microfracture
- Under 2cm²
- OATS
- 1–4cm²
- ACI / MACI
- Minimal (small biopsy)
- Microfracture
- None
- OATS
- 10–15%
- ACI / MACI
- High (cell culture)
- Microfracture
- Low
- OATS
- Moderate
Why the biology matters. ACI produces hyaline-like cartilage with predominantly Type II collagen and an organised matrix — biomechanically superior to the fibrocartilage (Type I) of microfracture, which is why ACI results hold up where microfracture deteriorates.
ACI produces hyaline-like cartilage with predominantly Type II collagen and organised matrix structure; biopsy studies show over 80 percent hyaline tissue at 2 years. This is biomechanically superior to the fibrocartilage (Type I) of microfracture — the basis of ACI's superior long-term durability.
- ACI / MACI (hyaline-like)
- Type II (over 80%)
- Microfracture (fibrocartilage)
- Type I
- ACI / MACI (hyaline-like)
- Organised
- Microfracture (fibrocartilage)
- Disorganised
- ACI / MACI (hyaline-like)
- Columnar
- Microfracture (fibrocartilage)
- Random
- ACI / MACI (hyaline-like)
- Variable
- Microfracture (fibrocartilage)
- Fibrous
- ACI / MACI (hyaline-like)
- Maintained 10–20 years
- Microfracture (fibrocartilage)
- Degrades at 2–5 years
- Harvest — 200–300mg cartilage biopsy - Enzymatic digestion releases the chondrocytes - Expansion over 4–6 weeks in culture - Result — 12–48 million cells ready to implant - MACI — cells seeded onto a collagen scaffold
- 3 months — soft repair cartilage - 6 months — increasing firmness - 12 months — near-normal stiffness - 18–24 months — full maturation - Rehabilitation mirrors this timeline
Operative sequence — Stage 1 biopsy through Stage 2 MACI implantation
- Arthroscopic or mini-open approach to the knee
- Locate a non-weight-bearing area of healthy cartilage for harvest
- Typical sites: superior margin of the intercondylar notch, superomedial trochlear margin, or the peripheral edge of the lesion itself
- Use a curette or gouge to take 200–300mg of full-thickness cartilage
- Usually 2–3 pieces, roughly 4–5mm each
- Enough healthy tissue to yield viable chondrocytes for expansion
- Place the biopsy in specialised transport medium and send it to the cell-culture laboratory; cells must stay viable in transit
- Now assess the index lesion fully — measure its size and map any additional defects for the Stage 2 plan
- Stage 1 is a minor procedure; the patient recovers quickly and waits for culture
- The biopsy is enzymatically digested and the chondrocytes expanded in a GMP-grade facility to 12–48 million cells
- For MACI, the expanded cells are seeded onto a collagen scaffold, arriving as a ready-to-implant membrane
- Confirm culture success and book Stage 2
- Mini-arthrotomy (medial or lateral parapatellar, depending on the lesion) or an arthroscopic approach, chosen for access to the whole defect
- Evert or sublux the patella and flex the knee as needed to see the lesion — adequate visualisation of the entire defect is essential before any work begins
- Trochlear lesions often need a mini-arthrotomy because of the sulcus contour
- Debride unstable cartilage back to stable, vertical shoulders
- Create a well-contained defect
- Curette away the calcified cartilage layer
- Preserve the subchondral plate — do not violate it excessively
- Make a template of the defect with sterile foil
- Trace the exact defect shape
- Cut the MACI scaffold to match the template precisely
- Dry the defect base, then apply fibrin glue to it
- Orient the scaffold correctly — the cell-seeded side faces DOWN toward the subchondral bone, the smooth membrane side faces the joint
- Place the scaffold into the defect and apply additional fibrin glue around the edges
- Ensure secure attachment with no gaps and no fluid undercutting the scaffold
- Cycle the knee through a full range of motion several times
- Confirm the scaffold stays put and does not delaminate, and that the edges stay sealed
- No sutures are typically needed with MACI
- Close in layers
The MACI scaffold carries cells on one side only. The cell-seeded side must face the subchondral bone (down), with the smooth membrane side facing the joint. Incorrect orientation compromises the entire procedure.
- Maintain a watertight seal if using a membrane technique - Cut the MACI scaffold to the exact defect size - Apply fibrin glue to a dry surface - Confirm scaffold stability through range of motion - Protect the subchondral plate
- Violate the subchondral bone excessively - Leave gaps at the scaffold edges - Allow fluid to track under the scaffold - Place the scaffold cell-side up - Allow early unprotected loading
Aftercare & Complications
Rehabilitation reflects cartilage maturation. ACI repair tissue is soft and vulnerable for months and takes 12–18 months to fully mature, so the protocol is slower than after OATS or microfracture.
Weight-bearing progression
- Toe-touch weight-bearing only, with crutches and a brace for protection
- Lets early cartilage maturation occur without load
- Progress weight-bearing from 25 percent up to 75 percent
- Wean the brace; crutches until comfortable
- Full weight-bearing without aids
- No impact activities; low-load exercises only
ACI cartilage takes 12–18 months to fully mature. Early on the tissue is soft and vulnerable, so weight-bearing and activity advance more slowly than after OATS or microfracture.
Return to activity
- Swimming, aqua jogging, stationary cycling
- No impact
- Jogging progression
- Light sport-specific drills
- Return to sport if MRI and clinical criteria are met
- Longer timeline than OATS or microfracture
Long-term outcomes.
- Design
- Case series, n=23
- Follow-up
- 2–3 yr
- Key finding
- First ACI series; 14 of 16 femoral condylar cases good-to-excellent
- Design
- Case series, n=224
- Follow-up
- 10–20 yr, mean 12.8
- Key finding
- 74% same or better; 92% would repeat ACI
- Design
- RCT, n=144
- Follow-up
- 5 yr
- Key finding
- MACI superior to microfracture (P=0.022)
- Design
- RCT, n=60
- Follow-up
- 2 yr
- Key finding
- MACI superior on Lysholm and Tegner
The SUMMIT RCT (Level 1, lesions 3cm² or larger) showed MACI clinically and statistically superior to microfracture, with benefit maintained at 5 years and fewer treatment non-responders (12.5% versus 31.9% at 2 years). Where microfracture results deteriorate at 2–5 years, MACI maintains improvement — most markedly for larger lesions.
Complications.
- Incidence
- 5–20% (highest with first-gen)
- Risk factors
- Periosteal ACI
- Prevention and management
- Use MACI; arthroscopic debridement if symptomatic
- Incidence
- 5–10%
- Risk factors
- Malalignment, poor technique
- Prevention and management
- Correct alignment; meticulous surgery
- Incidence
- Around 5%
- Risk factors
- Trauma, early loading
- Prevention and management
- Protected rehab; gradual return
- Incidence
- Around 5%
- Risk factors
- Prolonged immobilisation
- Prevention and management
- Early range-of-motion protocol
- Incidence
- Under 1%
- Risk factors
- Standard surgical risk
- Prevention and management
- Sterile technique
First-generation ACI under a periosteal flap had 20–30% hypertrophy rates needing secondary debridement. MACI has markedly reduced this complication; when hypertrophy does occur, arthroscopic debridement is usually effective.
Viva & Exam Focus
ACIACI — the core concept
Hook:ACI = your own cells, cultured, then implanted — Autologous, Cultured, Implanted.
MACIMACI — the modern standard
Hook:MACI adds a Matrix to ACI — cells delivered on a collagen scaffold.
Two stages. Stage 1 is a cartilage biopsy for cell harvest; cells are cultured for 4–6 weeks; Stage 2 is implantation of the expanded cells. This two-stage requirement is the key disadvantage versus single-stage OATS.
12–48 million cells. The initial 200–300mg biopsy holds roughly 200,000–300,000 chondrocytes, which culture expands to 12–48 million for implantation.
Matrix-induced Autologous Chondrocyte Implantation. Third-generation ACI, in which cells are seeded on a collagen scaffold — eliminating periosteal harvest and watertight membrane suturing.
First-generation (periosteal ACI), with 20–30% hypertrophy. This fell sharply with second-generation collagen membranes and further with MACI.
10–20 years (Peterson, AJSM 2010; mean 12.8 years). In 224 patients, 74% rated their knee the same or better than in previous years and 92% would have ACI again — but bipolar (kissing) lesions did worse than multiple unipolar defects.
Viva scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old female athlete has persistent symptoms 2 years after microfracture for a 3cm² medial femoral condyle lesion. MRI shows incomplete fill with subchondral changes. What are your options?”
“Describe the MACI implantation technique for a 4cm² trochlear lesion.”
“A 52-year-old man with a 2cm² medial femoral condyle lesion asks about ACI. His MRI also shows grade 2 patellofemoral changes and mild medial joint-space narrowing. Is he a candidate?”
Definition
- Two-stage cell-based cartilage repair
- Patient's own chondrocytes expanded in culture
- Hyaline-like cartilage formation
- MACI = cells on a collagen scaffold (current standard)
Generations
- First-gen — periosteal flap (hypertrophy 20–30%)
- Second-gen — collagen membrane
- Third-gen — MACI scaffold (current standard)
Key numbers
- Over 2cm² — typical lesion indication
- 4–6 weeks — cell culture duration
- 12–48 million — cells implanted
- 74% same or better at 10–20 years (Peterson)
- 12–18 months — full cartilage maturation
Two-stage process
- Stage 1 — biopsy of 200–300mg cartilage
- Culture — 4–6 weeks of expansion
- Stage 2 — MACI scaffold implantation
- Fibrin-glue fixation, no sutures
Advantages
- Hyaline-like cartilage (Type II collagen)
- Durable 10–20 year results
- Minimal donor morbidity (small biopsy only)
- Can treat large and multiple lesions
- MACI simpler than the periosteal technique
Disadvantages
- Two-stage procedure
- High cost (cell culture)
- Extended rehabilitation (12–18 months)
- Requires intact subchondral bone
- Not for diffuse OA
Background & Evidence
Evolution of the technique. ACI has moved through three generations, each solving the main problem of the last. First-generation ACI suspended cells under a harvested periosteal flap; its Achilles heel was periosteal hypertrophy. Second-generation ACI replaced the periosteum with a collagen membrane. Third-generation MACI seeds the cells onto a collagen scaffold in the lab, delivering a ready-to-implant membrane fixed with fibrin glue — no periosteal harvest, no watertight suturing, and a marked drop in hypertrophy.
- Technique
- Cells under a periosteal flap
- Advantages
- Original technique, proven long-term
- Disadvantages
- Periosteal hypertrophy (up to 30%); second incision to harvest periosteum
- Technique
- Cells under a collagen membrane
- Advantages
- No periosteal harvest, less hypertrophy
- Disadvantages
- Still needs watertight suturing
- Technique
- Cells seeded on a collagen scaffold
- Advantages
- No suturing, fibrin-glue fixation, less invasive
- Disadvantages
- Higher cost; needs reliable cell adherence
Guidelines, regulation and global practice.
- MACI (Vericel) is an FDA-approved cell-based product (US, 2016) and licensed in several other jurisdictions; availability and reimbursement vary widely by country - NICE (UK) TA477 recommends ACI for symptomatic defects over 2cm² of the femoral condyle in patients with no prior repair surgery and minimal OA - AAOS / ICRS position cell therapy for larger or failed lesions where marrow stimulation is inadequate - All techniques need a GMP-grade, accredited cell-culture facility with full chain-of-custody tracking
- Marrow stimulation first-line for small lesions (under 2cm²); cell therapy reserved for larger or failed defects - Bipolar (kissing) and patellar lesions do worse across registries and series - Malalignment, instability and meniscal deficiency must be corrected concurrently or staged, or the repair fails - Cell therapy carries the longest rehabilitation of the cartilage procedures (return to sport 12–18 months)
Key documentation: two-stage consent explaining the biopsy, culture period and implantation; the cell-culture laboratory, batch tracking and viability confirmation; the surgical detail (scaffold orientation cell-side down, fixation method). Consent must cover the extended 12–18 month rehabilitation, two operations, and realistic sport expectations (around two-thirds return to pre-injury level). If failure occurs, documentation of correct indication and technique is protective.
References
Original ACI Technique (First-Generation)
- First clinical series of cultured autologous chondrocytes, 23 patients, lesions 1.6-6.5 cm²
- Cells cultured 14-21 days and injected under a sutured periosteal flap (first-generation ACI)
- 14 of 16 femoral condylar transplants good-to-excellent at 2 years; patellar results poorer
- Biopsy showed hyaline-like repair in 11 of 15 femoral but only 1 of 7 patellar transplants
Long-Term Durability of ACI (10-20 Years)
- 224 patients, mean follow-up 12.8 years (range 10-20 years), mean lesion 5.3 cm²
- 74% reported their knee as the same or better than previous years; 92% would have ACI again
- Lysholm improved 60.3 to 69.5 and Brittberg-Peterson pain score 59.4 to 40.9
- Bipolar ('kissing') lesions had significantly worse outcomes than multiple unipolar lesions
SUMMIT RCT - MACI vs Microfracture (5-Year)
- Level 1 RCT, 144 patients, lesions 3 cm² or larger of femoral condyle or trochlea
- Co-primary KOOS pain + function superiority of MACI over microfracture maintained at 5 years (P =.022)
- 2-year data showed fewer treatment non-responders with MACI (12.5%) than microfracture (31.9%)
- MRI defect fill improved in both arms with no significant structural difference between groups
MACI vs Microfracture RCT (Basad)
- RCT of 60 patients (40 MACI, 20 microfracture), single isolated defects 4-10 cm²
- MACI significantly superior to microfracture at 2 years on Lysholm (P =.005) and Tegner (P =.04)
- Patient- and surgeon-rated ICRS scores also favoured MACI (P =.03 and.02)
- No safety issues attributable to either technique
Prior Marrow Stimulation Compromises Later ACI
- Cohort of 321 patients (522 defects); ACI failure defined as removal of over 25% of graft
- Prior subchondral-penetrating surgery raised failure 3-fold: 26% vs 8% in untreated controls
- Failure rates similar across drilling (28%), abrasion (27%) and microfracture (20%)
- Disruption of the subchondral plate is the proposed mechanism for impaired ACI take
Return to Sport After Cartilage Repair
- Systematic review of 20 studies, 1363 patients, mean follow-up 42 months
- Overall return to sport 73%; return to pre-injury level 68%; sustained pre-injury level 65%
- Time to return 7-18 months depending on technique; ACI/MACI shows the longest timeline
- Best durability of athletic return after autologous chondrocyte transplantation