Both columns through one incision | Mandatory trochanteric osteotomy | The most extensile acetabular approach (Letournel)
- Most extensile single approach to the acetabulum — combines ilioinguinal and Kocher-Langenbeck access through one lateral incision
- Trochanteric osteotomy is mandatory — it reflects the abductor mass proximally to reach the posterior column
- Highest heterotopic ossification risk in orthopaedics (40–60% without prophylaxis) — dual prophylaxis is strongly considered
- No true internervous plane — the abductor mass stays pedicled on the superior gluteal neurovascular bundle at the greater sciatic notch
- Steep learning curve — now reserved for experienced pelvic surgeons managing select complex both-column fractures
When & Why
What it exposes. The extended iliofemoral is the most extensile approach to the acetabulum, providing 360-degree access through a single lateral incision. It exposes the anterior column (iliac wing to pelvic brim, via the lateral and inner-table windows), the posterior column (from the greater sciatic notch to the ischium, via posterior reflection of the abductors and short external rotators), and the pelvic brim and quadrilateral surface between them — the entire acetabulum in one field. Why a single incision. Described by Emile Letournel (1960s–1970s), the approach was conceived to avoid two separate incisions and the need to reposition the patient. It works the anterior column much like the ilioinguinal approach and the posterior column much like the Kocher-Langenbeck, combining both through one extensile lateral exposure. Its defining advantage remains single-position, single-incision 360-degree access. Indications (now selective). The approach is reserved for patterns that cannot be adequately reduced through a single anterior or posterior window: - Both-column (associated) fractures — complete articular dissociation from the ilium, the spur sign, significant displacement of both columns in young patients where anatomical reduction is critical (the primary indication)
- Complex T-type fractures — a transverse component plus an anterior stem, with significant displacement requiring anterior and posterior fixation
- Anterior column + posterior hemitransverse — a high anterior column component with posterior column extension
- Revision surgery after failed prior fixation where access to both columns is needed Why use has declined. Very high complication rates (HO 40–60% without prophylaxis, nerve injury 15–20%, trochanteric nonunion 5–10%), a steep learning curve, and the availability of lower-morbidity alternatives mean most modern pelvic surgeons now use it sparingly.
- Extended Iliofemoral
- Single (extensive)
- Staged Two-Incision
- Two separate (K-L + ilioinguinal)
- Preferred
- Depends on surgeon preference
- Extended Iliofemoral
- Not required (lateral position)
- Staged Two-Incision
- Required (or simultaneous)
- Preferred
- Extended iliofemoral advantage
- Extended Iliofemoral
- Extensive (abductor elevation)
- Staged Two-Incision
- Moderate (two sites)
- Preferred
- Two-incision better
- Extended Iliofemoral
- 40–60% (highest)
- Staged Two-Incision
- 20–30% (high but lower)
- Preferred
- Two-incision better
- Extended Iliofemoral
- Mandatory
- Staged Two-Incision
- Not required
- Preferred
- Two-incision better (avoids osteotomy)
- Extended Iliofemoral
- Very steep
- Staged Two-Incision
- Moderate (two familiar approaches)
- Preferred
- Two-incision more accessible
The alternatives. - Staged two-incision — Kocher-Langenbeck for the posterior column (patient lateral), then 3–7 days later an ilioinguinal or Stoppa for the anterior column (patient supine). Lower HO risk, no trochanteric osteotomy, uses two familiar approaches. Increasingly preferred.
- Simultaneous two-team — both approaches at once under a single anaesthetic; technically demanding and needs two experienced pelvic surgeons.
- Modified approaches — an anterior intrapelvic (modified ilioinguinal + Stoppa concepts) window, with selective percutaneous fixation of one column.
The extended iliofemoral retains selective indications: (1) both-column fractures in young patients where anatomical reduction is critical and the surgeon has extensive experience with the approach; (2) complex T-type fractures requiring extensive anterior and posterior exposure; (3) revision surgery after failed prior fixation where access to both columns is needed. Most surgeons now reserve it for specific cases rather than routine use.
Position & landmarks. - Lateral decubitus, affected side up, secured on a beanbag or pegboard, with the entire limb prepped and draped free for manipulation
- C-arm positioned to allow inlet, outlet and Judet views from below; the surgeon stands facing the patient's back (as for the Kocher-Langenbeck), with the assistant opposite for retraction
- Landmarks: the iliac crest (PSIS to ASIS, the anterior limb) and the greater trochanter with the femoral shaft (the posterior limb)
The Exposure
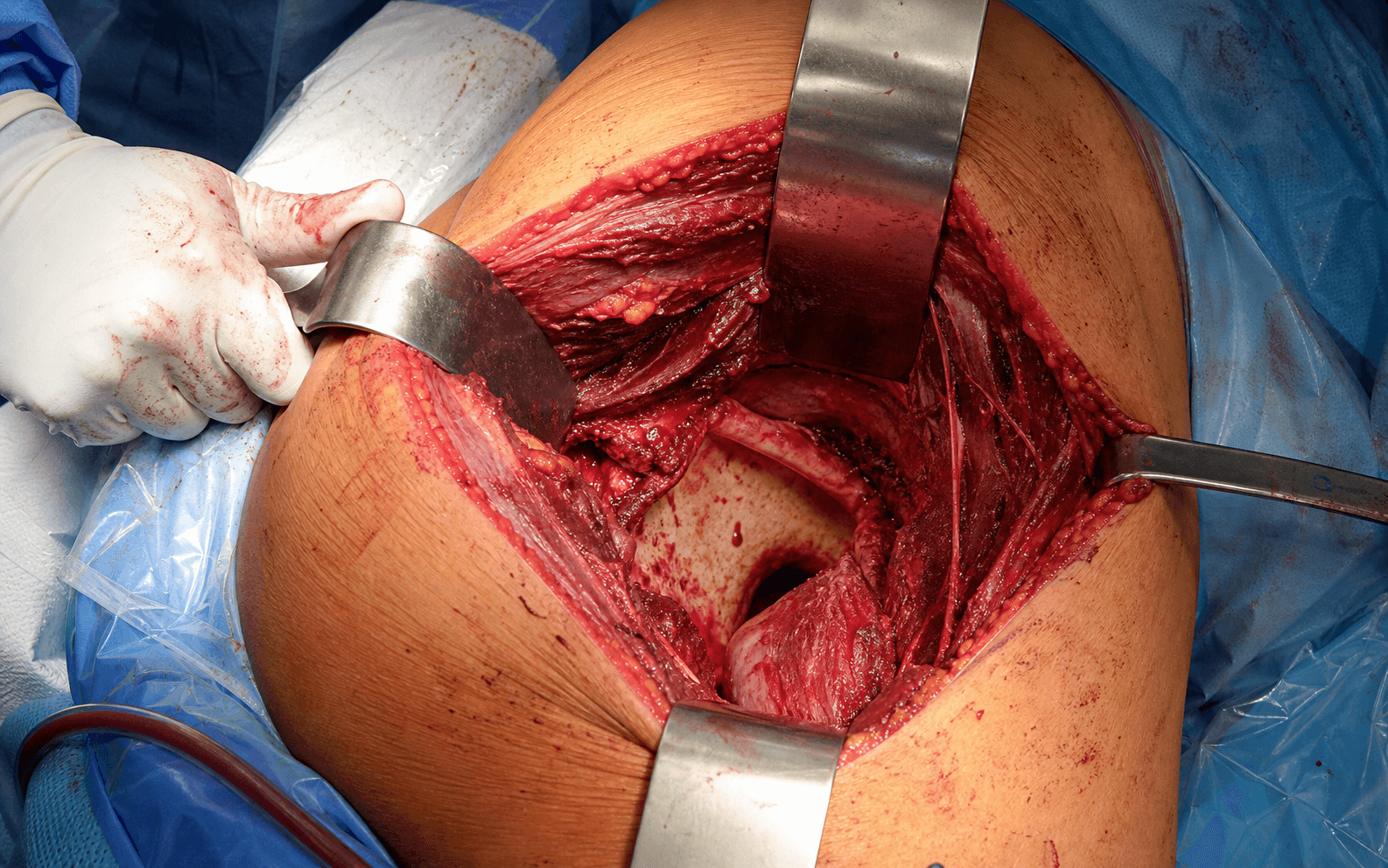
Work down through the layers in the lateral position: develop the anterior abductor interval and strip the gluteal muscles off the iliac wing, perform the trochanteric osteotomy to reflect the abductors, then open the posterior column behind them — completing a single-incision 360-degree exposure of the acetabulum.
Exposure sequence
- Lateral decubitus, affected side up; entire limb draped free for manipulation
- An extensive curved or T-shaped incision, 25–35 cm: an anterior limb along the iliac crest from PSIS to ASIS, and a posterior limb from the greater trochanter distally along the femur
- C-arm set for inlet, outlet and Judet views from below; surgeon faces the patient's back
- Develop the interval at the anterior border of the abductors — between tensor fasciae latae (superior gluteal nerve) and sartorius (femoral nerve)
- Elevate the abductor origin (gluteus medius and minimus) subperiosteally off the outer table of the iliac wing
- This exposes the iliac wing, anterior column and pelvic brim through lateral and inner-table windows
- The lateral femoral cutaneous nerve crosses near the ASIS and is often reflected or sacrificed for exposure — counsel the patient about anterolateral thigh numbness
- Plan an osteotomy that includes the vastus ridge laterally to give an adequate fixation surface; typical fragment thickness 1.5–2.0 cm, preserving the soft-tissue attachments
- Make an oblique cut with an oscillating saw from proximal-lateral to distal-medial, protecting the abductor soft tissues attached to the fragment
- Elevate the trochanter with the attached abductors and reflect them proximally — this exposes the posterior hip capsule and posterior column
- Tag the fragment for later repair; this osteotomy is what unlocks complete posterior column access
- Identify and protect the sciatic nerve as it emerges below piriformis; use intermittent retraction throughout
- Release the short external rotators (piriformis, conjoint tendon) and tag them for repair — their repair shields the nerve at closure
- Open the posterior capsule to expose the posterior column from the greater sciatic notch to the ischium
- The reflected abductor mass stays pedicled on the superior gluteal neurovascular bundle — protect it at the notch
- With both windows open, the entire acetabulum is accessible — anterior column, posterior column and pelvic brim
- Reduction can proceed on either column first, working around the circumference as the fracture dictates
- This single-position, single-incision 360-degree access is the approach's defining advantage, allowing comprehensive fracture reduction
- Fix the trochanteric osteotomy rigidly — tension band wiring, wires plus lag screws, or a cable plate system (options detailed below)
- Repair the short external rotators and piriformis to the trochanter with heavy non-absorbable suture
- Close in layers over a deep drain: fascia lata, subcutaneous tissue, skin
- Rigid fixation and rotator repair protect both the osteotomy and the sciatic nerve
Unlike the standard ilioinguinal or Kocher-Langenbeck approaches, the extended iliofemoral has no true internervous plane. Exposure depends on a trochanteric osteotomy to elevate the abductor mass (gluteus medius and minimus, supplied by the superior gluteal nerve) together with extensive soft-tissue dissection.
The working planes. The approach is fundamentally an extensile lateral exposure. Anteriorly it develops the interval at the front of the abductor mass — between tensor fasciae latae (superior gluteal nerve) and sartorius (femoral nerve) — then strips subperiosteally off the outer iliac wing. Posteriorly, after the trochanteric osteotomy reflects the abductors, the working interval runs through and beneath gluteus maximus (inferior gluteal nerve), a muscle-splitting plane rather than a true internervous one. The whole abductor mass stays pedicled on the superior gluteal neurovascular bundle at the greater sciatic notch, which is therefore the structure most at risk during proximal abductor elevation and must be protected throughout. Trochanteric fixation options. Rigid fixation of the osteotomy is essential for healing and function — nonunion or migration occurs in 5–10% even with optimal technique.
- Components
- 2–3 K-wires + figure-of-8 wire
- Advantages
- Classic technique, biomechanically sound
- Disadvantages
- Wire migration, breakage risk
- Components
- Cerclage wire + 2–3 lag screws
- Advantages
- More rigid than wires alone
- Disadvantages
- Screw fixation in thin trochanter challenging
- Components
- Cables + specialized trochanteric plate
- Advantages
- Most rigid fixation, lower failure rate
- Disadvantages
- Requires specific implants, more expensive
The trochanteric osteotomy is the maneuver that converts a lateral iliac exposure into full posterior column access. It must be large enough to include the vastus ridge laterally (giving an adequate fixation surface) and rigidly fixed at closure — nonunion or migration occurs in 5 to 10 percent even with optimal technique, causing abductor weakness and a Trendelenburg gait.
Dangers & Extensions
Structures at risk, by layer
- Location
- Posterior, below piriformis
- Risk
- 15–20% palsy (same as K-L)
- Protection Strategy
- Identify early, intermittent retraction, repair external rotators
- Location
- Above piriformis, into gluteus medius
- Risk
- 5–10% injury (higher than isolated approaches)
- Protection Strategy
- Careful dissection at the greater sciatic notch; the abductor mass is pedicled on this bundle
- Location
- Crosses the iliac crest medial to ASIS
- Risk
- Often sacrificed for exposure
- Protection Strategy
- Counsel the patient about anterolateral thigh numbness
- Location
- Lies on iliopsoas
- Risk
- Rare but devastating if injured
- Protection Strategy
- Identify and protect during the anterior dissection
Complications — the highest burden of any acetabular approach
- Extended Iliofemoral
- 40–60% (HIGHEST)
- Two-Incision Approaches
- 20–30%
- Management
- Dual prophylaxis (indomethacin + radiation); excision if severe after maturation
- Extended Iliofemoral
- 15–20%
- Two-Incision Approaches
- 15–20% (K-L component)
- Management
- Identify early, protect, repair rotators, monitor recovery
- Extended Iliofemoral
- 5–10% (higher than isolated approaches)
- Two-Incision Approaches
- 2–5% (K-L alone)
- Management
- Careful dissection at the notch; Trendelenburg gait if injured
- Extended Iliofemoral
- 5–10%
- Two-Incision Approaches
- N/A (no osteotomy)
- Management
- Rigid fixation, protected weight-bearing, revision if symptomatic
- Extended Iliofemoral
- 10–15%
- Two-Incision Approaches
- 5–10%
- Management
- Meticulous closure, drain placement, antibiotics
The extended iliofemoral approach carries the highest HO risk of any orthopaedic procedure — 40–60% without prophylaxis. Dual prophylaxis should be strongly considered: indomethacin 75 mg daily for 6 weeks plus single-dose radiation 7–8 Gy within 72 hours. In the landmark Matta-group series of 106 cases treated with indomethacin, significant HO still occurred in 30%. Even with prophylaxis, 10–20% develop some HO. Given the catastrophic impact of severe HO on hip function, some surgeons use both modalities specifically for this approach.
Recovery protocol. Rehabilitation is longer than for other acetabular approaches because both the fracture fixation and the trochanteric osteotomy must be protected.
Recovery Protocol
- Toe-touch weight bearing only (protect the osteotomy)
- Hip abduction exercises only — no active abduction
- Passive range of motion as tolerated
- Indomethacin 75 mg daily for HO prophylaxis
- X-rays to assess trochanteric healing
- Progress to partial weight bearing if healing
- Begin active abduction exercises
- Continue range-of-motion work
- Full weight bearing when fracture and osteotomy are healed
- Strengthening programme
- Gait normalisation
- Return to activities as tolerated
- Monitor for HO development (up to 18 months)
- Assess for trochanteric complications
- Consider hip arthroplasty if severe arthritis develops
Procedures Through This Approach
- ORIF of both-column (associated) acetabular fractures — the primary indication, an alternative to a staged two-incision approach
- ORIF of complex T-type fractures requiring extensive anterior and posterior exposure
- ORIF of anterior column + posterior hemitransverse fractures
- Revision acetabular surgery after failed prior fixation requiring simultaneous both-column access
- Delayed or open reduction of complex patterns where extensive exposure aids reduction
- Excision of mature heterotopic ossification through the same extensile plane
Viva & Exam Focus
EXTENDEDEXTENDED — Key Features of the Approach
OSTEOTOMYOSTEOTOMY — Trochanteric Fixation Essentials
Why is trochanteric osteotomy mandatory in the extended iliofemoral approach? The osteotomy allows the abductor muscles to be reflected proximally with the trochanter, providing access to the posterior column and posterior acetabulum. Without it the approach cannot achieve 360-degree acetabular exposure. The osteotomy must include the vastus ridge for adequate fixation.
What is the incidence of HO with the extended iliofemoral and how is it prevented? Extended iliofemoral has the highest HO risk of any orthopaedic procedure at 40–60% without prophylaxis. Prevention requires dual prophylaxis: indomethacin 75 mg daily for 6 weeks plus single-dose radiation 7–8 Gy within 72 hours. Even with prophylaxis, 10–20% develop some HO.
Extended iliofemoral vs staged two-incision for both-column fractures? Extended iliofemoral provides 360-degree acetabular access through a single incision, avoiding repositioning. However, most surgeons now prefer staged two-incision approaches due to lower complications (20–30% HO vs 40–60%, no trochanteric osteotomy, lower nerve injury). Extended iliofemoral is reserved for complex cases by experienced surgeons.
Fixation options for the trochanteric osteotomy, and why is rigid fixation important? Options: (1) tension band wiring, (2) wires plus lag screws, (3) cable plate system. Rigid fixation is critical because nonunion occurs in 5–10% despite best technique, causing abductor weakness, Trendelenburg gait and pain. Cable plate systems provide the most rigid fixation with the lowest failure rate.
Why has the use of extended iliofemoral declined? The approach has very high complication rates (40–60% HO without prophylaxis, trochanteric nonunion 5–10%, superior gluteal nerve injury 5–10%) with no improvement in fracture outcomes compared to staged two-incision approaches. Modern surgeons prefer lower-morbidity alternatives that achieve similar reduction quality. Extended iliofemoral is now reserved for select cases.
Greater trochanter osteotomy is mandatory for this approach. It must be adequately large (include the vastus ridge), rigidly fixed at closure (wires plus screws or a cable plate), and protected post-operatively to heal. Nonunion or migration occurs in 5–10% despite best technique.
Highest HO risk of any approach — historically 40–60% without prophylaxis. In the landmark Matta-group series of 106 cases with indomethacin, significant HO still occurred in 30%. Extensive abductor stripping and muscle trauma drive ectopic bone. Indomethacin and/or single-dose radiation prophylaxis is essential; severe HO can ankylose the hip.
Just as in Kocher-Langenbeck, the sciatic nerve is at significant risk (15–20%). Identify early, protect throughout, and repair the external rotators. Extended dissection increases nerve injury risk compared to an isolated K-L approach.
The main advantage is 360-degree acetabular access through one incision, avoiding the need for patient repositioning. However, this comes at the cost of extensive soft-tissue trauma, high complication rates and prolonged surgery. Most surgeons now prefer two separate approaches.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old male has a both-column acetabular fracture with significant displacement of both anterior and posterior columns. Your consultant asks whether you would use the extended iliofemoral or a staged two-incision approach. What factors guide your decision?”
“Six months after an extended iliofemoral approach, a patient returns with lateral hip pain and a limp. X-rays show the acetabular fracture has healed well, but the trochanteric osteotomy has not united and has migrated proximally 2 cm. How do you manage this?”
“Eighteen months after an extended iliofemoral approach for a both-column fracture, a patient has developed severe heterotopic ossification (Brooker Grade IV) with complete ankylosis of the hip. The acetabular fracture healed anatomically. What are the management options?”
Key Characteristics
- Most extensile acetabular approach — 360-degree access
- Single incision for both anterior and posterior columns
- Trochanteric osteotomy MANDATORY for exposure
- Combines ilioinguinal and Kocher-Langenbeck concepts
- HIGHEST complication rate of any acetabular approach
Indications (Selective)
- Both-column fractures (alternative to two-incision)
- Complex T-type fractures
- Anterior column + posterior hemitransverse
- Revision surgery requiring both-column access
- Reserved for experienced pelvic surgeons
Trochanteric Osteotomy
- Must include the vastus ridge laterally for fixation
- Allows abductor reflection for posterior exposure
- Fixation: cable plate system preferred (most rigid)
- Nonunion rate 5–10% despite optimal technique
- Requires 8–12 weeks of protected weight-bearing to heal
Complications (VERY HIGH)
- HO: 40–60% without prophylaxis (HIGHEST of any approach)
- Trochanteric nonunion: 5–10% — causes permanent limp
- Sciatic nerve palsy: 15–20% — same as K-L
- Superior gluteal nerve: 5–10% — higher than K-L alone
- Wound complications: 10–15% — large incision
HO Prophylaxis (CRITICAL)
- DUAL prophylaxis recommended: indomethacin + radiation
- Indomethacin 75 mg daily for 6 weeks starting post-op day 1
- PLUS radiation 7–8 Gy single dose within 72 hours
- Even with dual prophylaxis, 10–20% develop some HO
- Severe HO (Brooker III–IV) in 5–10% despite prophylaxis
Why Use Has Declined
- VERY high complications with no outcome advantage
- Two-incision approaches achieve similar reduction quality
- Two-incision: 20–30% HO vs 40–60%, no trochanteric issues
- Steep learning curve vs two familiar approaches
- Modern trend: reserve for complex cases by experts only
References
Guidelines, Registries and Global Practice Centralisation of complex acetabular trauma. Across major trauma systems (AO Foundation, OTA in the US, BOA/BOAST pelvic and acetabular fracture standards in the UK, and equivalent national networks), displaced acetabular fractures requiring an extensile exposure are recommended for management in high-volume Level 1 centres with subspecialty pelvic/acetabular expertise. Outcome is volume-dependent: anatomical reduction rates and complication profiles improve with surgeon and unit experience. This is the single most consistent message across guidelines worldwide. Approach selection consensus. Contemporary international practice (reflected in AO and OTA teaching) favours a single working window where one can be used, with anterior intrapelvic / modified Stoppa approaches increasingly replacing the ilioinguinal, and reserves extensile or combined exposures for patterns that cannot otherwise be reduced. The extended iliofemoral is now used selectively rather than routinely. HO prophylaxis — side-by-side evidence. There is no single global standard, and practice genuinely differs by unit: - Indomethacin (typically 75 mg daily, or 25 mg three times daily, for about 6 weeks) — first-line in most centres; cheap and effective (Moore et al RCT)
- Single-dose radiation (700 to 800 cGy within about 72 hours) — equivalent efficacy in the randomised data but roughly 200 times more expensive and logistically demanding
- Combined indomethacin plus radiation — lowest reported HO incidence (Piatek et al) and favoured by some surgeons specifically for the extended iliofemoral given its very high baseline risk Registry and outcome context. Acetabular fracture surgery is not implant-registry tracked the way arthroplasty is (NJR, AJRR, AOANJRR, Swedish/Norwegian registries), but secondary total hip arthroplasty after an acetabular fracture IS captured in those arthroplasty registries and is a recognised, higher-complexity revision burden — reinforcing the value of achieving anatomical reduction at the index operation. Blood management. Major pelvic/acetabular surgery carries significant blood-loss risk. Intraoperative cell salvage and locally available massive-transfusion / patient-blood-management protocols are standard of care internationally; tranexamic acid is widely used to reduce transfusion requirement. Rehabilitation. Extended recovery with protected (toe-touch) weight bearing for about 6 to 8 weeks to protect both the fracture fixation and the trochanteric osteotomy, then graduated loading, coordinated through specialist physiotherapy regardless of healthcare system.
Letournel — Acetabulum Fractures: Classification and Management
- Foundational paper establishing the Letournel-Judet classification (5 elementary plus 5 associated patterns) and the surgical approach algorithm still used worldwide
- Established that a perfect (anatomical) open reduction is the method of choice for displaced acetabular fractures and the principal determinant of outcome
- Both-column fractures, complex transverse and T-type patterns are the patterns for which an extensile single-incision exposure was developed
- Difficult patterns demand experienced surgeons — results deteriorate when anatomical reduction is not achieved
Griffin, Beaule, Matta — Safety and Efficacy of the Extended Iliofemoral Approach
- Single-surgeon prospective series of 106 complex acetabular fractures (60% both-column) treated via the extended iliofemoral approach, mean follow-up 6.3 years
- Anatomical reduction (0 to 1 mm) achieved in 72%; ALL fractures united; good or excellent Merle d'Aubigne-Postel result in 64%
- Significant heterotopic ossification developed in 30% and was associated with a worse functional score (mean 13.7)
- Functional outcome correlated significantly with accuracy of reduction (p less than 0.009)
Matta — Accuracy of Reduction and Clinical Results (Operative within 3 Weeks)
- 262 displaced acetabular fractures operated within 21 days; both-column was the single most common associated pattern (35%)
- Anatomical reduction achieved in 71%; rate fell with increasing fracture complexity, older age and longer injury-to-surgery interval
- Clinical result excellent or good in 76% and closely related to the radiographic reduction; excision of ectopic bone required in 5%
- Establishes the benchmark that anatomical reduction and joint congruity are the dominant predictors of hip survival
Moore, Goss, Anglen — Indomethacin vs Radiation for HO Prophylaxis (RCT)
- Prospective randomised blinded trial of 72 evaluable adults after acetabular ORIF (Kocher-Langenbeck, combined, or extended iliofemoral approaches)
- Indomethacin 25 mg three times daily for 6 weeks versus single-dose 800 cGy radiation within 3 days
- No significant difference in HO formation between the two arms; both safe and effective with no treatment-related complications
- Radiation was approximately 200 times more expensive than indomethacin and carries additional risks; the two Brooker IV cases occurred in patients who did not receive proper indomethacin dosing
Piatek et al — Combined Indomethacin plus Radiation HO Prophylaxis
- Retrospective cohort of 24 patients receiving combined single-dose radiation plus indomethacin after operative acetabular fracture, assessed at 24 months
- Only 1 of 24 patients developed heterotopic ossification with the combined regimen
- Systematic literature comparison showed combined prophylaxis had the lowest HO incidence versus radiation or indomethacin alone (significant difference)
- Supports dual modality prophylaxis for the highest-risk exposures such as the extended iliofemoral