A functional inter-nervous interval giving direct access to the medial and anterior femoral shaft for MIPO, medial plating and revision around previously operated lateral tissue
- The interval is between sartorius and vastus medialis — both innervated by the femoral nerve, so this is a FUNCTIONAL (not true) internervous plane; it is safe because the two muscles have distinct functions (sartorius is a hip flexor, vastus medialis a knee extensor) and their nerve branches enter from different directions.
- Subsartorial (Hunter's) canal boundaries: sartorius forms the roof, vastus medialis the lateral wall, adductor longus and magnus the medial wall. It carries the femoral artery, femoral vein, saphenous nerve and the nerve to vastus medialis.
- The saphenous nerve is the structure most often injured — it pierces the fascial roof of the canal at mid-thigh to become subcutaneous. Identify and protect it with a vessel loop whenever the canal is opened.
- NAVEL — lateral to medial at the base of the femoral triangle: Nerve, Artery, Vein, Empty space, Lymphatics.
- MIPO preserves the fracture hematoma and periosteal perfusion — never strip or directly expose the fracture site; insert the plate submuscularly beneath vastus medialis.
- MIPO for distal femur fractures achieves around 93 percent union without bone grafting (Kregor LISS series, 96 of 103 fractures).
When & Why
What it exposes. The anteromedial approach is a versatile corridor giving direct access to the medial and anterior aspects of the femoral shaft through the interval between sartorius (medial) and vastus medialis (lateral). It is the workhorse exposure for minimally invasive plate osteosynthesis (MIPO) of the distal femur, medial plate fixation of the shaft, bone grafting of nonunions, and revision work where the lateral side has already been operated on. Why anteromedial (and not lateral). Both sartorius and vastus medialis are innervated by the femoral nerve, so the interval is technically a functional rather than a true internervous plane. It is nevertheless safe: the nerve branches enter from different directions (sartorius from its deep surface, vastus medialis from its lateral surface) and the muscles have distinct functions, so dissection between them denervates nothing of consequence. The approach has grown in popularity for modern MIPO techniques and is especially attractive when the lateral femur is scarred, comminuted, or unsuitable for fixation — it offers a superficial, relatively avascular plane and virgin medial tissue. The critical structure at risk is the femoral neurovascular bundle. In the femoral triangle the arrangement lateral-to-medial is remembered as NAVEL (Nerve, Artery, Vein, Empty space, Lymphatics). In the mid-thigh these structures run through the subsartorial (Hunter's) canal, bounded by vastus medialis laterally, adductor longus and magnus medially, and sartorius superficially.
- Typical scenario
- Middle-third shaft fracture needing medial plating; MIPO of distal femur; periprosthetic Vancouver/UCS B1
- What the approach gives you
- Direct medial corridor; medial plate fixation; submuscular plate insertion
- Typical scenario
- Atrophic nonunion with medial bone loss; previous lateral surgery
- What the approach gives you
- Virgin medial tissue plane; direct access to the defect for grafting
- Typical scenario
- Benign or malignant medial femoral lesion
- What the approach gives you
- Biopsy or wide excision corridor with neurovascular control
- Typical scenario
- Lateral side previously operated or scarred; ipsilateral vascular injury
- What the approach gives you
- Alternative virgin plane; shared field for combined orthopaedic-vascular repair
Position & landmarks. Position the patient supine on a radiolucent table (essential for fluoroscopy); a standard fracture table is generally not required. Place a bump under the ipsilateral hip to tilt the pelvis and bring the medial thigh anteriorly. Position the limb with the hip abducted 15 to 20 degrees and externally rotated 10 to 15 degrees, and the knee flexed 10 to 20 degrees on a sterile bump to relax the quadriceps. The C-arm comes from the contralateral side. Palpate and mark the ASIS and pubic tubercle (defining the inguinal ligament), the mid-inguinal point (midway between ASIS and pubic symphysis — the femoral artery), the adductor tubercle on the medial femoral condyle (distal landmark), and the oblique course of sartorius. The incision is centred between the ASIS and the adductor tubercle. Contraindications. Active infection in the surgical field (cellulitis, abscess, open contaminated medial wound) is an absolute contraindication to elective use — stage with debridement and temporary external fixation in trauma. Relative contraindications are massive medial soft-tissue loss (wound-healling and coverage concern — consider a lateral route or flap) and morbid obesity (deep field, difficult retraction). Threatened limb viability from vascular insufficiency is usually a contraindication — except that an acute vascular injury needing combined repair turns it into an indication. Assess high-risk limbs with ankle-brachial indices and CT angiography. Anaesthesia. General anaesthesia is preferred for optimal muscle relaxation, but neuraxial blockade suits elderly patients with cardiopulmonary comorbidity. For MIPO, an adductor canal or femoral nerve block gives targeted analgesia while preserving motor function — coordinate timing with the surgeon, as a pre-operative femoral block can blur landmark identification.
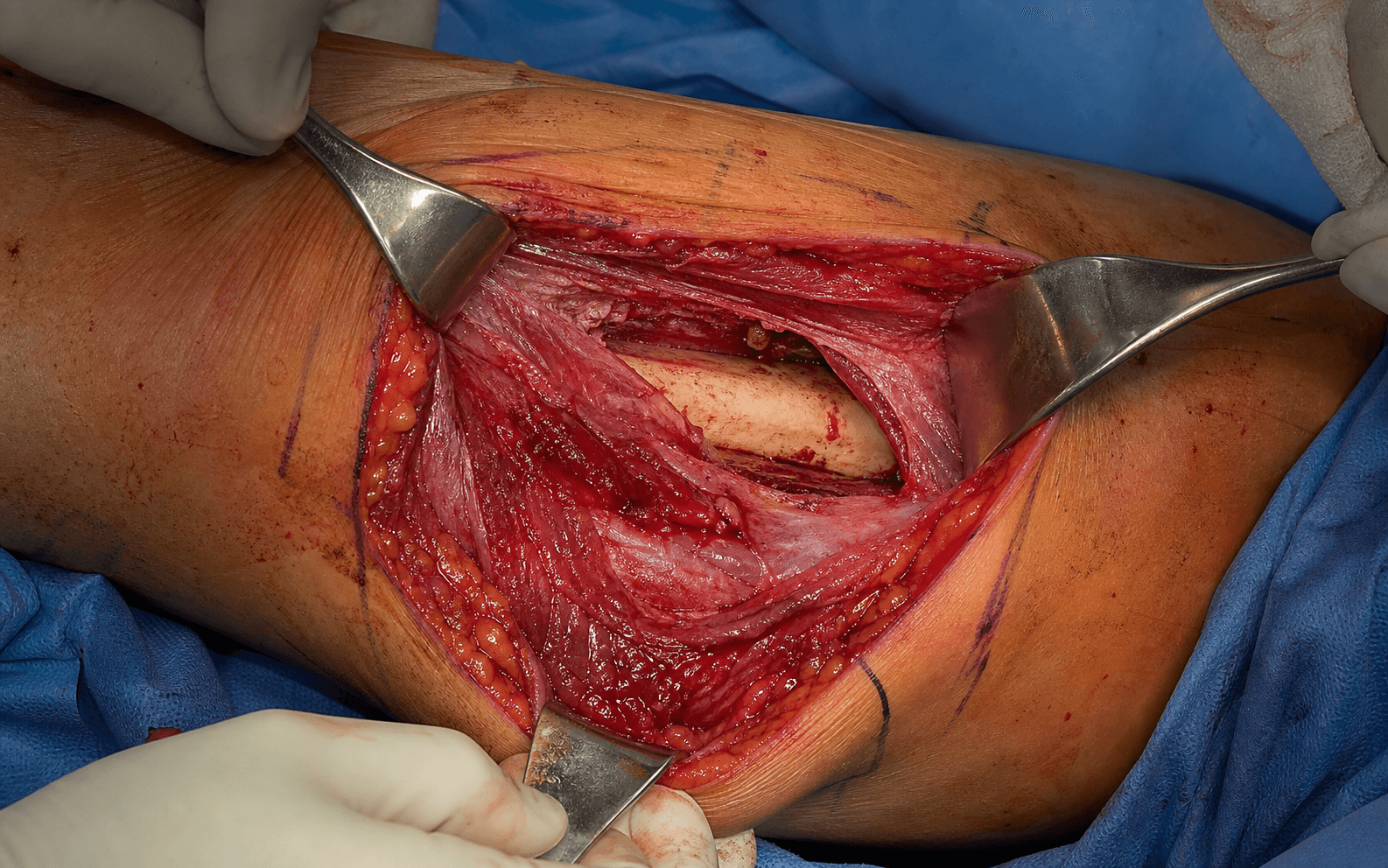
The Exposure
Work down through the medial thigh in layers: incise over the sartorius–vastus medialis interval, open the subsartorial canal carefully to find and protect the femoral vessels and saphenous nerve, then elevate vastus medialis subperiosteally off the shaft.
Exposure sequence
- A longitudinal incision over the medial thigh, centred between the ASIS proximally and the adductor tubercle distally — typically beginning about 8 to 10 cm distal to the ASIS and extending 15 to 20 cm as exposure demands (a shorter 8 to 10 cm incision suffices for MIPO).
- Place the incision slightly posterior to the anterior midline of the medial thigh to avoid the great saphenous vein running along the more anterior aspect.
- Incise the fascia lata in line with the skin incision to reveal the strap-like, obliquely-running sartorius beneath.
- Identify sartorius by its strap-like appearance and oblique course from lateral-proximal to medial-distal, and vastus medialis lateral to it as a bulkier muscle with vertical fibres.
- Develop the interval between them and retract sartorius medially (anteriorly) with a handheld or self-retaining retractor, exposing vastus medialis and the roof of the subsartorial canal.
- With sartorius retracted, identify the fascial roof of the subsartorial (Hunter's) canal — a distinct layer spanning between sartorius superficially and the adductors medially.
- Incise it carefully under direct vision with Metzenbaum scissors, because the femoral artery and vein lie immediately deep to it.
- Once opened, identify the femoral vessels and mobilise them gently medially by blunt dissection.
- The saphenous nerve lies lateral to the femoral artery in the canal; it is the most commonly injured structure in this approach.
- Identify it early, mobilise it carefully and protect it with a vessel loop; alongside it protect the nerve to vastus medialis.
- Place retractors under direct vision and reposition them frequently to avoid compression injury.
- With the neurovascular structures protected, elevate vastus medialis subperiosteally from the medial femur using a Cobb or Key elevator, working at the medial lip of the linea aspera.
- Strip only what the planned procedure requires — in fracture cases, excessive circumferential stripping devascularises fragments and impairs healing.
- For MIPO, create a submuscular tunnel by elevating vastus medialis from the shaft without exposing the fracture, extending the tunnel proximally and distally from the limited incision.
- Reduce indirectly with traction and manipulation under fluoroscopy, then pass a locking plate from distal to proximal beneath vastus medialis, holding its soft-tissue attachments.
- Place distal screws through the incision under direct vision and proximal screws percutaneously; aim for at least three to four bicortical screws each side of the fracture.
The saphenous nerve is the commonest and most troublesome structure injured in this exposure, with a reported injury rate of roughly 5 to 15 percent (usually a temporary neuropraxia but occasionally a painful neuroma causing medial-leg numbness). It is at risk when the fascial roof of the subsartorial canal is opened and during distal extension. Identify it lateral to the artery the moment the canal is opened, loop it, avoid self-retaining retractors on it, and release retraction regularly.
The approach is safe even though both muscles share femoral-nerve innervation because the nerve branches enter from different directions, the muscles have different functions (sartorius flexes the hip, vastus medialis extends the knee), and medial elevation of vastus medialis preserves its lateral nerve entry. Calling it a "functional internervous plane" — and explaining why it is safe — is exactly what the examiner wants to hear.
The whole point of MIPO is biology. Preserve the fracture hematoma and periosteal attachments, reduce indirectly, and pass the plate submuscularly. Stripping the fracture site converts a biological fixation into an open one and forfeits the healing advantage.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Great saphenous vein; saphenous nerve branches
- Protection
- Incise slightly posterior to the anterior midline; identify the nerve early under direct vision
- Structure at risk
- Femoral artery and vein (immediately deep to the roof)
- Protection
- Open the fascial roof carefully with scissors; mobilise vessels medially by gentle blunt dissection
- Structure at risk
- Saphenous nerve and nerve to vastus medialis
- Protection
- Identify the saphenous nerve lateral to the artery; loop it; reposition retractors frequently
- Structure at risk
- Perforating arteries from profunda femoris (first perforator largest, about 5 to 7 cm distal to the lesser trochanter)
- Protection
- Coagulate or ligate as encountered; control prevents haematoma without compromising limb perfusion
- Structure at risk
- Thigh compartment syndrome; fracture-fragment devascularisation
- Protection
- Limit periosteal stripping to what is needed; release retractors periodically
Complications. Saphenous nerve injury (5 to 15 percent, usually neuropraxia) causes medial-leg numbness or a painful neuroma — prevent it as above; a refractory neuroma may need excision and proximal-stump burial. Femoral vessel injury is the most serious risk — arterial injury presents with pulsatile bleeding, an expanding haematoma or loss of distal pulses; manage with immediate direct pressure, proximal and distal control, and urgent vascular surgery (primary repair with 5-0 or 6-0 Prolene if a clean laceration and help is delayed). Haematoma is minimised by meticulous haostasis, a drain where indicated, a compression dressing, and delaying the first chemoprophylaxis dose 6 to 12 hours; tranexamic acid may help in high-risk patients. Surgical site infection occurs in about 1 to 3 percent — superficial cases respond to antibiotics, deep cases need debridement and sometimes hardware removal. Thigh compartment syndrome is rare but a surgical emergency — pain with passive stretch demands urgent four-compartment fasciotomy. Extensile options. Extend proximally along the radial border of sartorius toward the femoral triangle to reach the femoral vessels for proximal control or to address proximal-shaft pathology. Extend distally along the medial border of the patella toward the adductor tubercle for the distal femur and for MIPO submuscular plate insertion — this distal extension is where the saphenous nerve is most vulnerable. Closure. Achieve meticulous haemostasis and inspect the canal to confirm the vessels are intact. Close the fascia lata with 0 or 1 absorbable suture; the subsartorial canal roof need not be formally closed (it is thin and closure may compress the bundle). Let sartorius fall back over the vessels to provide soft-tissue cover, then close subcutaneous tissue (2-0 or 3-0 absorbable) and skin (staples, subcuticular suture or adhesive) over a sterile compression dressing.
Procedures Through This Approach
- MIPO / submuscular locked plating of distal femur fractures — the principal modern use, achieving high union without grafting.
- Medial plate fixation of middle-third femoral shaft fractures — when the lateral side is comminuted, has bone loss, or is unsuitable for fixation.
- Periprosthetic Vancouver/UCS B1 fractures around a well-fixed hip stem — medial plating avoids the scarred lateral tissue and abductors; distinguishing B1 (fix the fracture) from B2/B3 (revise the stem) is the decision pivot.
- Bone grafting of atrophic nonunions — direct medial access to the defect plus medial plating for stability, avoiding a previously operated lateral plane.
- Corrective osteotomy for femoral malunion and biopsy or excision of medial femoral tumours (benign and, with limb-salvage reconstruction, malignant).
- Combined orthopaedic-vascular procedures for ipsilateral femoral fracture with vascular injury — a single shared medial field.
Viva & Exam Focus
At a glance. The anteromedial approach reaches the medial femoral shaft through the interval between sartorius (medial) and vastus medialis (lateral) — both femoral-nerve innervated, making this a functional but not true internervous plane. Key uses are MIPO of the distal femur (around 93 percent union without grafting), medial plating, nonunion grafting, and revision where the lateral side is scarred. The subsartorial (Hunter's) canal carries the femoral vessels and must be identified to avoid catastrophic injury; its boundaries are sartorius (roof), vastus medialis (lateral) and the adductors (medial). The saphenous nerve exits the canal at mid-thigh and is the most commonly injured structure (5 to 15 percent). Position supine with the hip slightly abducted and externally rotated.
MEDIALMEDIAL — the approach steps
NAVELNAVEL — femoral triangle contents (lateral to medial)
Both sartorius and vastus medialis are innervated by the femoral nerve. The interval is still functionally safe because sartorius is primarily a hip flexor while vastus medialis is a knee extensor, and their nerve branches enter from different directions, so dissection between them causes minimal functional deficit.
Lateral wall: vastus medialis. Medial wall: adductor longus (proximally) and adductor magnus (distally). Roof: sartorius with its fascial covering (the vastoadductor membrane). Contents: femoral artery, femoral vein, saphenous nerve and the nerve to vastus medialis.
The saphenous nerve. It exits the subsartorial canal at mid-thigh by piercing the fascial roof to become subcutaneous. It must be identified and protected during proximal dissection; injury causes sensory loss over the medial leg and can produce a painful neuroma.
NAVEL — Nerve (femoral), Artery (femoral), Vein (femoral), Empty space, Lymphatics. The femoral nerve lies most lateral under the iliacus fascia; the lymphatics lie most medial in the femoral canal, the site of a femoral hernia.
Femoral-vessel injury from failing to identify subsartorial canal anatomy; saphenous nerve damage during proximal dissection without identification; thigh compartment syndrome from over-retraction of vastus medialis; fracture devascularisation from circumferential periosteal stripping.
Subsartorial (Hunter's) canal: vastus medialis (lateral wall), adductor longus and magnus (medial wall), sartorius and fascial roof (anterior). The saphenous nerve exits at mid-thigh by piercing the fascial roof. Femoral vessels enter the canal proximally at the apex of the femoral triangle.
Why is this not a true internervous plane? Both muscles are femoral-nerve innervated but functionally distinct. What is at risk? Femoral vessels, saphenous nerve, perforating vessels. When choose medial over lateral? Previous lateral surgery, medial pathology, MIPO, combined vascular procedures.
Position supine with the hip slightly abducted and externally rotated. Incise skin and fascia over the medial thigh. Identify sartorius and retract it medially to expose vastus medialis. Open the subsartorial roof to identify and protect the femoral vessels. Elevate vastus medialis laterally to expose the medial shaft.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old builder has a painful six-month atrophic nonunion of the middle-third femoral shaft after intramedullary nailing done through a lateral approach, with medial bone loss. He wants to return to work. How would you achieve union?”
“You are planning MIPO fixation of a distal femur fracture (AO 33-A3, extra-articular supracondylar) in a 78-year-old woman with osteoporosis who takes rivaroxaban for atrial fibrillation; the fracture is shortened with medial comminution. Walk me through your approach and fixation.”
“During an anteromedial approach to plate a femoral shaft fracture you inadvertently injure the femoral artery with a retractor, causing pulsatile bleeding. The on-call vascular surgeon is 30 minutes away. Talk me through your immediate management.”
Anatomy rapid fire
- Interval: sartorius (femoral) and vastus medialis (femoral) — NOT a true internervous plane
- Subsartorial canal: sartorius (roof), vastus medialis (lateral), adductor longus/magnus (medial)
- NAVEL — Nerve, Artery, Vein, Empty space, Lymphatics (lateral to medial)
- Saphenous nerve exits the canal at mid-thigh by piercing the fascial roof
- Perforating arteries from profunda femoris pierce adductor magnus posteriorly
Indications — high yield
- Femoral shaft fractures needing medial plate fixation
- MIPO for distal femur fractures — submuscular locked-plate insertion
- Periprosthetic femur fractures (Vancouver/UCS B1) when medial fixation is planned
- Revision where the lateral approach was previously used
- Combined orthopaedic-vascular procedures
Critical surgical steps
- Position: supine, hip abducted and externally rotated, knee flexed 10 to 20 degrees
- Incision: longitudinal over the medial thigh, slightly posterior to the midline
- Develop the interval — retract sartorius medially, vastus medialis laterally
- Open the subsartorial canal roof carefully — vessels lie immediately deep
- Identify and protect the saphenous nerve with a vessel loop
- Elevate vastus medialis from the shaft by subperiosteal dissection
Examiner trap questions
- Why NOT a true internervous plane? Both muscles femoral-nerve innervated, but functionally distinct
- MIPO vs traditional plating? Preserves fracture hematoma, submuscular insertion, indirect reduction
- Femoral artery injury management? Direct pressure, proximal/distal control, vascular surgery
- Assess rotation in MIPO? Clinical comparison with the contralateral limb plus fluoroscopy
- Subsartorial canal boundaries? Sartorius (roof), vastus medialis (lateral), adductors (medial)
Guidelines, registries & global practice
- Prophylaxis (AAOS/NICE/BOA/AO consensus): cefazolin 2 g IV within 60 min; vancomycin for true allergy or MRSA
- Registries (NJR, AOANJRR, AJRR, SHAR): periprosthetic fracture a rising revision indication, higher with cementless stems
- Vancouver/UCS B1 = well-fixed stem = FIX; B2/B3 = loose stem = REVISE (the decision pivot)
- Vascular surgery backup is the key system requirement — defer or transfer if unavailable
- Femoral shaft fracture incidence roughly 10 to 21 per 100,000 per year, bimodal distribution
Complications
- Saphenous nerve injury: 5 to 15 percent rate, usually temporary neuropraxia
- Femoral vessel injury: direct pressure, vascular surgery consult, primary repair or grafting
- Compartment syndrome: pain with passive stretch — urgent four-compartment fasciotomy
- Haematoma: meticulous haemostasis, consider a drain
- Infection: SSI rate 1 to 3 percent; deep infection may need hardware removal
References
Epidemiology. Femoral shaft fractures occur worldwide at roughly 10 to 21 per 100,000 person-years with a classic bimodal distribution: high-energy injuries in young men and low-energy fragility fractures in older women. Periprosthetic femoral fractures around hip stems are a fast-growing burden across all major registries as arthroplasty volumes and patient age rise. Vancouver/UCS type B fractures (around the stem) are the commonest periprosthetic pattern; type B1 (well-fixed stem) is the subgroup managed by fixation rather than revision and is therefore the principal indication for plating via this corridor. Registry evidence — periprosthetic femoral fractures
- Region
- UK
- Signal
- Periprosthetic fracture a rising indication for revision; cementless stems carry higher early periprosthetic fracture risk than cemented
- Region
- Australia
- Signal
- Periprosthetic fracture among leading reasons for revision after primary THR; risk elevated with cementless fixation, especially in older women
- Region
- USA
- Signal
- Periprosthetic fracture an increasing share of revision burden as primary volumes grow
- Region
- Sweden / Scandinavia
- Signal
- Cementless stems and female sex associated with higher early periprosthetic fracture rates
- First-line
- Cefazolin 2 g IV (3 g if over 120 kg) within 60 min of incision
- Beta-lactam allergy / MRSA
- Vancomycin 15 mg/kg or clindamycin
- First-line
- Cephalosporin at induction per local protocol
- Beta-lactam allergy / MRSA
- Glycopeptide for MRSA risk or allergy
- First-line
- First-generation cephalosporin within 60 min
- Beta-lactam allergy / MRSA
- Vancomycin for MRSA-endemic settings
Global practice variation. Vascular surgery availability is the key system-level determinant for this approach. In tertiary trauma centres with on-site vascular cover, combined orthopaedic-vascular procedures can be undertaken safely. In resource-limited or remote settings without immediate vascular backup, a high-risk anteromedial dissection is best deferred to scheduled lists with full teams present, or an alternative approach selected; damage-control external fixation and transfer to a centre with vascular capability is the safe default for the acutely injured limb with vascular concern.
MIPO for Distal Femur Fractures (LISS)
- 103 distal femur fractures (OTA 33 and distal 32) treated with the submuscular Less Invasive Stabilization System (LISS)
- 96 of 103 fractures (93%) healed WITHOUT autogenous bone grafting
- Low acute infection rate (3 of 103, 3%) and zero loss of distal condylar fixation
- Malreduction in only 6% despite 35 open fractures and 30 patients over age 65
Blood Supply Preservation with MIPO
- Ten paired fresh cadaver femora: conventional lateral open plating versus percutaneous submuscular MIPO (silicone arterial dye injection)
- All MIPO specimens retained intact perforating and nutrient arteries; conventional plating disrupted them variably
- MIPO preserved periosteal perfusion in every specimen and medullary perfusion in 70%
- Provides the biologic rationale for submuscular plate insertion in femoral shaft and distal femur fractures
Risk Factors for Locked Plate Failure
- 335 distal femur fractures (OTA 33A/C, 33% open) treated with lateral locked plates across three trauma centres
- 64 of 335 (19%) required reoperation to promote union, including 30 planned staged bone grafts for open-fracture defects
- Independent risk factors for reoperation and deep infection: open fracture and diabetes
- Independent risk factors for proximal implant failure: open fracture, smoking, higher BMI and SHORTER plate length
Unified (Vancouver) Classification of Periprosthetic Femoral Fractures
- International field test of the Unified Classification System (UCS) for periprosthetic fractures of the pelvis and femur around total hip replacement
- Substantial inter-observer agreement for the femur (kappa 0.81 experts, 0.73 trainees)
- Almost perfect intra-observer agreement for the femur (kappa 0.92 experts)
- Confirms reproducibility of the B1/B2/B3 distinction that drives fix-versus-revise decision-making