Joint preservation · Varus correction · Unloading the medial compartment
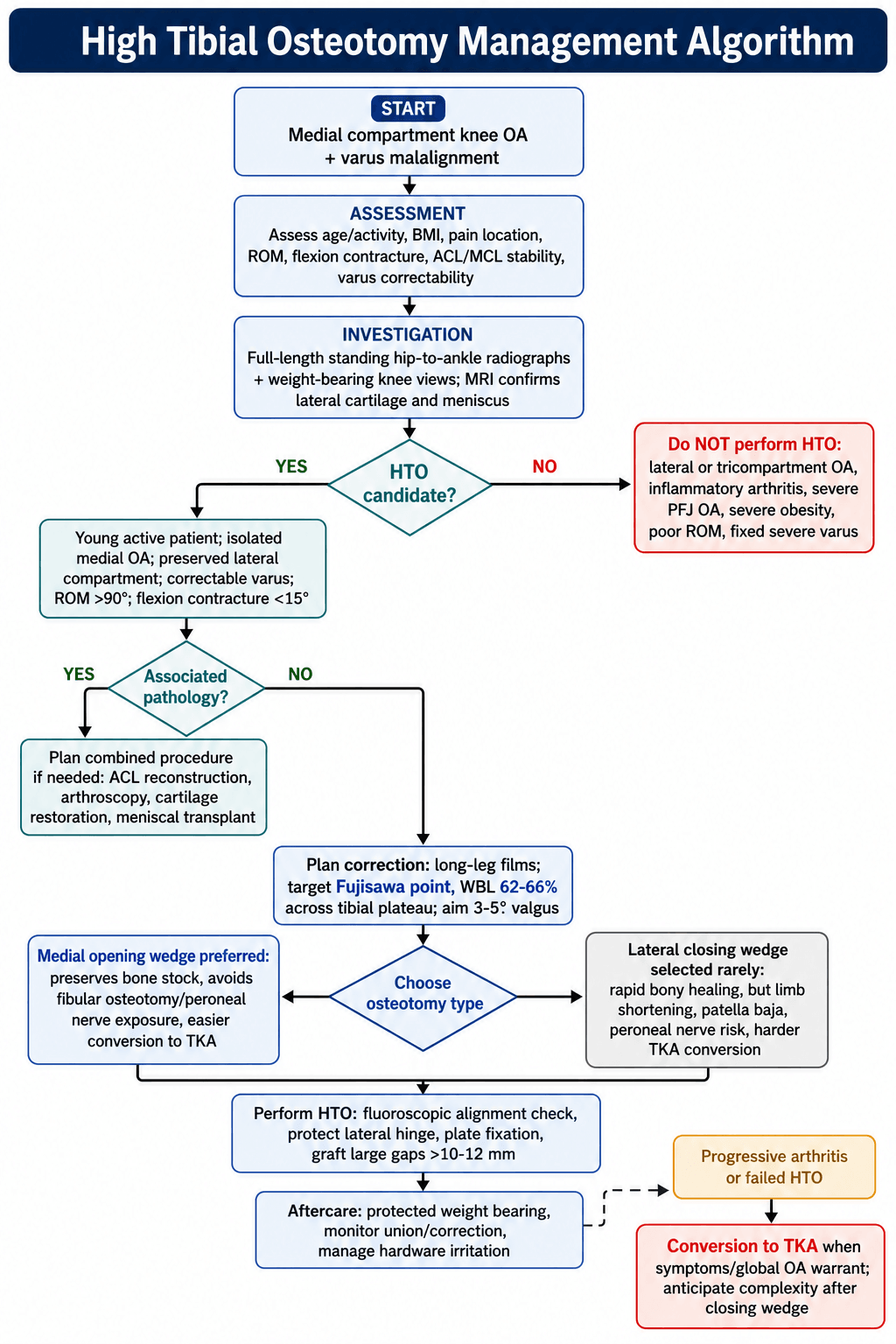
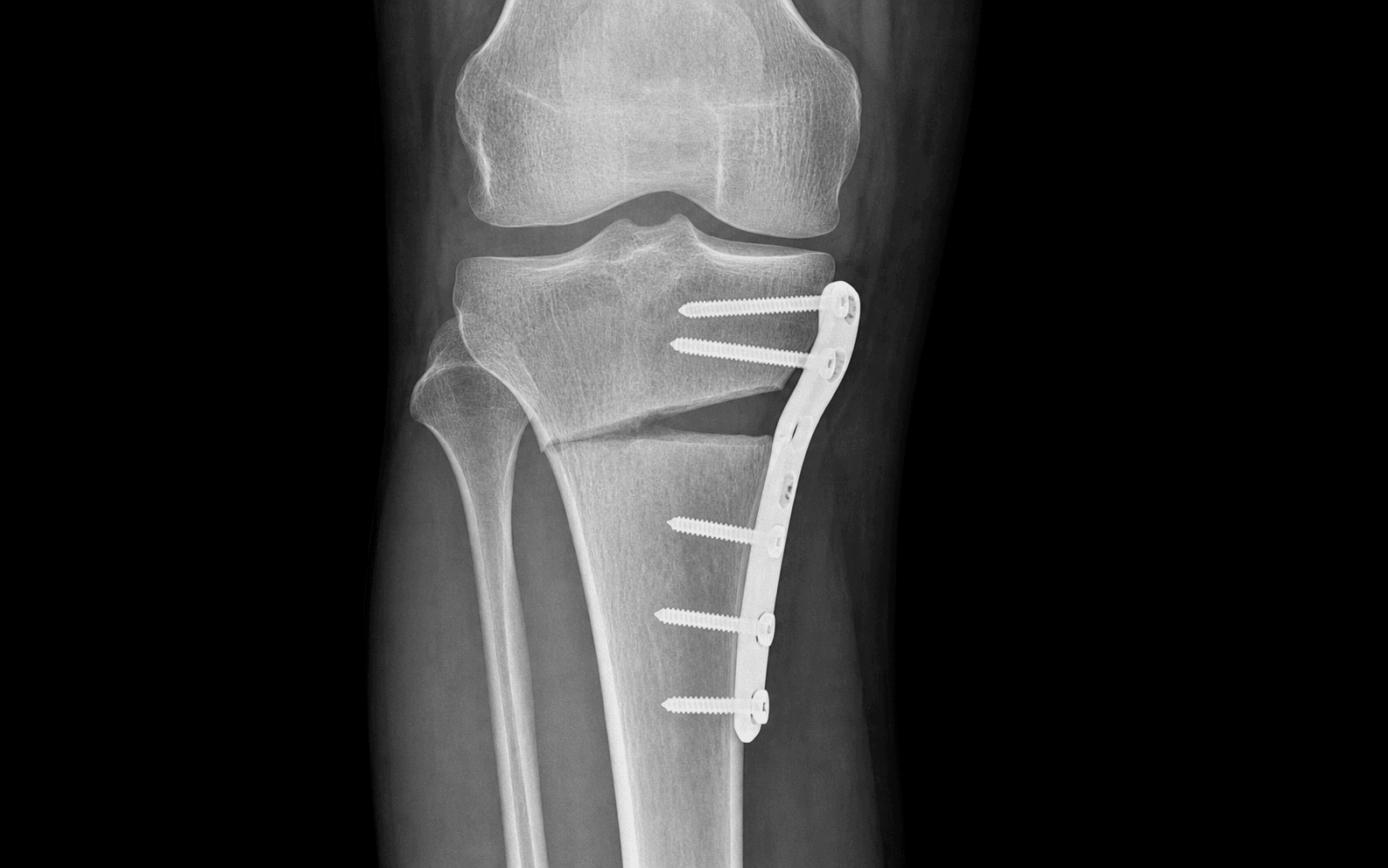
- A medial opening wedge is now the dominant technique worldwide — it preserves bone stock, avoids fibular osteotomy and peroneal-nerve risk, and is straightforward to convert to TKA later.
- The operation corrects varus by moving the mechanical axis to the Fujisawa point at 62 to 65 percent of the tibial plateau width, roughly 3 to 5 degrees of valgus overcorrection.
- The ideal patient is age 40 to 60, BMI under 30, with isolated medial OA (Ahlbäck grade 1 to 2), a pristine lateral compartment on MRI, intact cruciates and flexion over 120 degrees.
- Maximum practical opening-wedge correction is 12 to 15mm; every 5mm of opening increases the posterior tibial slope by about 2 degrees.
- With modern locking-plate fixation, routine bone-void filling does not improve union or knee scores (Mao 2022); reserve graft for larger gaps only.
- Opening- and closing-wedge HTO give equivalent patient-reported outcomes and TKA-conversion rates; opening wedge preserves bone and avoids the peroneal nerve, closing wedge better preserves slope (van Haeringen 2022).
When & Why
Indication. Symptomatic, isolated medial compartment osteoarthritis with varus malalignment in an active patient who has failed conservative management (activity modification, physiotherapy, NSAIDs, bracing and at least one intra-articular injection) and wants to preserve the joint rather than proceed to arthroplasty. The operation corrects alignment to unload the diseased medial compartment and delay TKA by a decade or more. Why correction works. In varus the mechanical axis passes medial to the knee centre, concentrating load medially. A normal knee shares load about 60:40 medial to lateral, and each degree of varus adds roughly 10 to 12 percent of medial load — driving progressive cartilage wear. HTO corrects varus to 3 to 5 degrees of valgus so the axis crosses the Fujisawa point (62 to 65 percent of the plateau width), shifting load laterally off the medial compartment.
The opening- versus closing-wedge decision. Both techniques achieve equivalent clinical results; the choice is about anatomy, bone stock and risk profile:
Add height on the medial side through a medial approach. Preserves bone stock (an advantage for a future TKA), needs no fibular osteotomy, carries almost no peroneal-nerve risk, and allows intraoperative adjustment of correction. Fixation is a medial locking plate (TomoFix); bone graft is optional. Now first-line for the varus knee worldwide.
Remove a lateral wedge through a lateral approach plus a fibular osteotomy. Union is faster and slope is better preserved, but it shortens the limb 5 to 10mm, removes bone (making later TKA harder) and carries a 5 to 10 percent peroneal-nerve palsy risk. Reserve for a valgus knee needing varus correction, severe medial soft-tissue scarring, or specific surgeon preference.
The ideal candidate, and who to turn away. Selection is the single biggest determinant of success — a wrong patient is a failed osteotomy.
- Age 40 to 60 years - BMI under 27 (up to 30 acceptable) - Isolated medial OA, Ahlbäck grade 1 to 2 - Lateral compartment pristine on MRI (Outerbridge 0 to 1) - Varus 5 to 12 degrees, stable cruciates - Flexion over 120 degrees, extension to 0 - Active, motivated, able to comply with a 6-week protected weight-bearing protocol
- Inflammatory arthritis (RA, psoriatic) - Bi- or tricompartmental OA - Ligamentous instability (ACL or PCL deficiency) - Flexion contracture over 15 degrees - ROM under 90 degrees - Active infection - Severe peripheral vascular disease
- Smoking (about a 4-fold nonunion risk) - Diabetes with HbA1c over 8 percent - Varus over 15 degrees - Symptomatic patellofemoral arthritis - Age over 65 (consider TKA) - Workers compensation or litigation
HTO or TKA? — a shared decision.
- Recommendation
- HTO preferred
- Rationale
- Delays TKA by 15-plus years, preserves bone stock, maintains activity
- Recommendation
- HTO or TKA (shared decision)
- Rationale
- HTO may last 10 years then TKA; TKA may last a lifetime. Discuss both
- Recommendation
- TKA preferred
- Rationale
- HTO unlikely to last 5-plus years and will not address PF symptoms
- Recommendation
- TKA (HTO contraindicated)
- Rationale
- Lateral disease will progress rapidly; a large correction is risky
- Recommendation
- HTO strongly preferred
- Rationale
- Too young for TKA (revision guaranteed in a lifetime); HTO buys 15 to 20 years
Consent specifically for loss of correction (5 to 10 percent), delayed or nonunion (5 percent), compartment syndrome (under 1 percent but devastating), peroneal nerve palsy (5 to 10 percent in closing wedge), and a realistic 40 percent chance of conversion to TKA within 15 years. Frame HTO honestly as joint preservation that delays rather than cures arthritis. Setup. Supine on a radiolucent table, thigh tourniquet, knee flexed 20 to 30 degrees over a bump to relax the medial soft tissues, and a C-arm set up for perfect AP and lateral views. Mark the medial joint line, tibial tubercle and pes anserinus.
The Operation
The goal is to correct varus by opening the medial tibial cortex and tilting the tibial plateau into valgus until the mechanical axis crosses the Fujisawa point — preserving a stable lateral cortical hinge, protecting the popliteal vessels posteriorly, and locking the correction with a rigid medial plate. The medial opening-wedge technique is laid out in full below; the lateral closing-wedge alternative follows.
Medial opening-wedge HTO — operative sequence
- Supine on a radiolucent (Jackson) table, thigh tourniquet at 300mmHg after exsanguination, knee flexed 20 to 30 degrees over a bump.
- Position the C-arm for a perfect AP (tibial spines centred between the femoral condyles) and a perfect lateral (femoral condyles superimposed); confirm the whole knee and proximal tibia are visible on both.
- If using the cable technique, check you can obtain a full hip-to-ankle mechanical-axis view. Mark the medial joint line, tibial tubercle and pes anserinus.
- An oblique incision 5 to 6cm long, starting about 1cm posteromedial to the tibial tubercle and 4cm distal to the joint line, running distally and anteriorly at 45 degrees toward the tibial crest.
- The line stays posterior to the superficial MCL to preserve it and allows proximal or distal extension if needed.
- Identify the pes anserinus (sartorius, gracilis, semitendinosus) on the anteromedial tibia and retract it posteriorly, protecting the sartorial branch of the saphenous nerve; some surgeons release and tag the pes for later repair.
- Stay anterior to the superficial MCL with subperiosteal dissection; place a Hohmann retractor anterolaterally beneath the patellar tendon and a posterior retractor to guard the MCL and neurovascular structures.
- Elevate along the medial and anterior tibia from 3cm to 10cm distal to the joint. The posterior periosteum is elevated carefully and a curved elevator is kept behind the tibia throughout the case to shield the popliteal vessels during sawing.
- Under fluoroscopy, insert a 2.0mm K-wire from anteromedial tibia aimed toward the superior fibular head, entering 3.5 to 4cm distal to the medial joint line, ascending 5 to 10 degrees and staying 1 to 1.5cm below the joint to avoid an intra-articular cut.
- On the lateral view the wire should lie in the anterior half of the tibia so the posterior cortex is preserved as the hinge. Place a parallel second K-wire 5mm distal as a saw guide.
- Biplanar technique (an ascending plus a descending cut) preserves the posterior cortical hinge and drops the lateral hinge-fracture rate from about 20 percent to under 10 percent.
- Ascending cut (anteromedial to posterolateral) along the proximal K-wire with an oscillating saw, stopping 1cm short of the lateral cortex; keep it parallel to the joint line.
- Descending cut (anterolateral toward posterior) perpendicular to the first, forming an L or hockey-stick shape, stopping 1cm short of the posterior cortex.
- Complete the break with a thin osteotome, gently twisting to propagate a controlled fracture of the lateral cortex while the posterior cortex stays intact as the hinge.
- Insert calibrated lamina spreaders (e.g. a Puddu spreader) and open gradually in 1 to 2mm increments; check fluoroscopy after each opening so the lateral cortex fractures and the posterior cortex bends in a controlled way.
- Cable technique: an electrocautery cable from the centre of the femoral head to the centre of the ankle should pass through the knee at 62 to 65 percent of the plateau width from the medial edge. Open or close the spreader to hit the target and record the gap. Navigation, if available, shows the mechanical axis in real time and accounts for soft-tissue laxity.
- Gap under 10mm: graft optional — modern locking plates are sufficient.
- Gap 10 to 15mm: consider graft (autograft preferred, or allograft chips).
- Gap over 15mm: graft strongly recommended (high nonunion risk); very large gaps should be avoided altogether where possible.
- Seat a TomoFix locking plate on the anteromedial tibia with the proximal end just below the joint; the first screw is a non-locking screw through the oblong hole to act as a reduction screw that seats the plate.
- Insert 3 proximal bicortical locking screws (3.5mm), measuring depth carefully to avoid penetrating far posteriorly; they must stay 5mm below the joint line.
- Insert graft into the wedge (posterior first, then anterior) if used, then the 3 distal screws (may be unicortical). Gently stress into varus to confirm stability and flex to 90 degrees to check for impingement; re-verify alignment before closure.
- Most surgeons use no drain; if one is placed, remove it at 24 hours.
- Repair the pes if released (Krackow stitch to drill holes), close periosteum and fascia over the plate to reduce hardware prominence, and close in layers.
- Apply a compressive dressing and a hinged knee brace locked in extension for early protected motion.
Keep a curved elevator behind the tibia throughout the sawing and opening. A posterior cortex breach threatens the popliteal artery — the most feared complication (under 1 percent but catastrophic). Maintain the elevator, control saw depth, use biplanar cuts that stop 1cm short of both the lateral and posterior cortices, and confirm on lateral fluoroscopy. If a breach is suspected, explore and involve vascular surgery.
- A biplanar osteotomy that preserves the posterior cortical hinge (hinge-fracture rate under 10 percent).
- Slight overcorrection to 3 to 5 degrees valgus at the Fujisawa point (undercorrection fails early).
- Rigid locking-plate fixation (loss of correction under 5 percent with modern plates). The commonest technical error is an intra-articular cut — keep the guide wire 1 to 1.5cm below the joint on the lateral view.
Opening increases the posterior tibial slope by about 2 degrees for every 5mm of opening, because the wedge is thicker anteriorly. Limit the total slope increase to under 5 degrees from baseline; excessive slope destabilises the knee and raises ACL graft tension in a reconstructed knee. Minimise it with an anterior-biased opening or a biplanar cut. Closing wedge typically maintains or slightly decreases slope.
- Closing wedge (lateral)
- Lateral incision plus a proximal fibular osteotomy 8 to 10cm distal to the head
- Closing wedge (lateral)
- Resect a lateral wedge based on the correction (1mm of base is about 1 degree), leaving a 1cm medial cortical hinge
- Closing wedge (lateral)
- Lateral locking plate or staples with compression across the osteotomy
- Closing wedge (lateral)
- Faster — weight-bearing as tolerated from day 1; union by 8 to 10 weeks
- Closing wedge (lateral)
- Peroneal nerve palsy 5 to 10 percent — prophylactic decompression of fascial bands at the fibular neck, without direct nerve dissection
Aftercare & Complications
Rehabilitation (opening wedge). Protected weight-bearing is the single most important modifiable factor — early weight-bearing before 6 weeks is the leading cause of loss of correction.
- Weight-bearing
- Toe-touch (10 to 20 pounds), crutches, brace locked in extension
- Motion and therapy
- Gentle ROM 0 to 90 degrees from day 1; DVT prophylaxis (e.g. aspirin 325mg for 4 weeks)
- Imaging
- AP and lateral at 2 weeks
- Weight-bearing
- 25 percent body weight weeks 2 to 4, then 50 percent
- Motion and therapy
- Advance to 0 to 120 degrees by week 6; isometric quads, straight-leg raises
- Imaging
- AP and lateral at 6 weeks (callus, alignment)
- Weight-bearing
- Full weight-bearing by week 8 to 10 if healing
- Motion and therapy
- Full ROM by week 12; closed-chain strengthening, proprioception
- Imaging
- AP and lateral at 12 weeks (union)
- Weight-bearing
- Full
- Motion and therapy
- Low-impact activity (cycling, swimming) from 3 months; impact sports from 4 to 6 months
- Imaging
- AP and lateral at 6 months
- Weight-bearing
- Full
- Motion and therapy
- Avoid marathon running and jumping long-term to protect durability
- Imaging
- Annual review for 3 to 5 years; hardware removal at 18 to 24 months if symptomatic
Because closing-wedge osteotomy uses compression fixation, patients may bear weight as tolerated from day 1 and typically reach 90 percent functional recovery by 4 months with union by 8 to 10 weeks. The trade-off is peroneal-nerve vigilance — any foot-drop symptoms need urgent evaluation.
Complications — recognition, prevention, management.
- Incidence
- 5 to 10 percent
- Prevention
- Rigid locking plate, protected weight-bearing, good bone quality, gap under 12mm
- Management
- Early (under 6 weeks): revision fixation with bone graft. Late: accept if asymptomatic, revise if symptomatic
- Incidence
- 5 percent overall; 10 to 15 percent in gaps over 10mm without graft
- Prevention
- Avoid large gaps, graft gaps over 10 to 15mm, stop smoking
- Management
- Observe if asymptomatic (many unite by 6 months); bone graft or exchange plating if symptomatic
- Incidence
- Up to 20 to 30 percent of opening wedge, often subclinical
- Prevention
- Biplanar technique, gradual opening, stop 1cm from the lateral cortex
- Management
- Takeuchi type I (stable): proceed with medial plate. Type II or III: protect weight-bearing, add lateral plate or lag screws
- Incidence
- 1 to 2 percent
- Prevention
- Guide wire 1 to 1.5cm below the joint on the lateral view; control saw depth
- Management
- Small (under 2mm): accept, watch for hemarthrosis. Large (over 5mm): treat as a tibial plateau fracture
- Incidence
- Under 1 percent but devastating
- Prevention
- Limit tourniquet time, release before closure, avoid excess stripping
- Management
- Clinical diagnosis — urgent four-compartment fasciotomy within 6 hours
- Incidence
- 5 to 10 percent closing wedge; rare opening wedge
- Prevention
- Fibular osteotomy 8 to 10cm distal to the head, prophylactic decompression, avoid nerve dissection
- Management
- Observe — about 80 percent recover by 12 months. AFO for foot drop; explore a complete palsy with no recovery at 3 months
- Incidence
- 2 to 3 percent
- Prevention
- Optimise glycaemia and smoking, avoid prominent hardware
- Management
- Oral antibiotics for cellulitis; washout for abscess; retain stable hardware within 3 weeks
- Incidence
- Under 1 percent
- Prevention
- Antibiotic prophylaxis, avoid prolonged surgery
- Management
- Washout, retain stable hardware within 3 weeks, 6 weeks IV antibiotics; remove hardware after union if chronic
- Incidence
- 10 to 15 percent of opening wedge (usually asymptomatic)
- Prevention
- Avoid very large corrections
- Management
- Usually asymptomatic; consider a late tibial tubercle osteotomy for symptomatic instability
- Incidence
- 40 percent by 15 years, 60 percent by 20 years
- Prevention
- Correct patient selection, achieve 3 to 5 degrees valgus
- Management
- Plan as joint preservation — HTO does not compromise later TKA outcomes
The lateral hinge fracture — Takeuchi classification. Recognising the pattern intraoperatively (a sudden loss of resistance, an audible crack, the fracture line on fluoroscopy) dictates management.
- Where the line exits
- At or proximal to the proximal tibiofibular joint (commonest, about 73 percent)
- Stability
- Stable
- Management
- Proceed with standard medial locking-plate fixation
- Where the line exits
- Distal to the proximal tibiofibular joint
- Stability
- Less stable; risks delayed union and loss of correction
- Management
- Protect weight-bearing, consider supplementary fixation
- Where the line exits
- Into the lateral tibial plateau (intra-articular)
- Stability
- Unstable
- Management
- Treat as a plateau fracture: lag screws or a lateral plate, then complete the medial fixation
After HTO, severe pain out of proportion, pain with passive stretch and a tense anterior compartment is compartment syndrome until proven otherwise. Do not delay for imaging; if uncertain, measure compartment pressures (absolute over 30mmHg, or a delta pressure — diastolic minus compartment — under 30mmHg) and perform an urgent four-compartment fasciotomy within 6 hours.
Viva & Exam Focus
ACTIVEACTIVE — the ideal HTO candidate
PAHCOPAHCO — the opening-wedge operation
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 48-year-old carpenter presents with 2 years of progressive medial knee pain. He is active, wants to continue working, and has tried physiotherapy and NSAIDs without relief. On examination he has medial joint line tenderness, ROM 0 to 130 degrees, and stable ligaments. His standing AP X-ray shows medial joint space narrowing with 8 degrees of varus alignment. What is your assessment and management plan?”
“You are performing an opening-wedge HTO on a 52-year-old patient with 10 degrees of varus. You have made your biplanar osteotomy cuts. As you begin opening the wedge with calibrated spreaders you hear an audible crack and feel a sudden loss of resistance at 8mm of opening. Fluoroscopy shows a fracture line extending from the lateral cortex posteriorly toward the tibial plateau. What has happened, how do you classify it, and what is your intraoperative management?”
“A 55-year-old patient is postoperative day 1 after an opening-wedge HTO. The nurse reports severe pain (10 out of 10) in the leg despite IV morphine, worsening with passive ankle dorsiflexion. The anterior compartment of the leg is tense and firm. What is your immediate assessment and management?”
Patient selection (ACTIVE)
- Age 40 to 60 years (the ideal window for durability)
- Compartment isolated medial (Ahlbäck 1 to 2, lateral pristine on MRI)
- Tibiofemoral stability (ACL and PCL intact — instability contraindicates)
- Inflammatory arthritis absent (RA, psoriatic progress despite HTO)
- Varus under 15 degrees (large corrections fail; undercorrection inevitable)
- Excellent ROM (flexion over 120 degrees; a flexion contracture over 15 degrees or ROM under 90 degrees predicts a poor outcome)
Preoperative planning
- Full-length standing films are MANDATORY (hip-knee-ankle for the mechanical axis)
- Target: Fujisawa point = 62 to 65 percent of the tibial plateau width from the medial edge
- Correction angle: 3 to 5 degrees of valgus overcorrection for durability
- MRI: confirm lateral compartment Outerbridge 0 to 1 (grade 2-plus predicts failure)
- Miniaci estimate: opening height (mm) is about correction angle (degrees) times 0.7
- Maximum opening 12 to 15mm (excessive slope change and nonunion risk beyond)
Opening-wedge technique
- Approach: medial, 4cm distal to the joint line, protect the pes and superficial MCL
- Biplanar osteotomy: ascending plus descending cuts preserve the posterior cortical hinge
- Guide wire: 1 to 1.5cm below the joint on the lateral view (avoid intra-articular)
- Gradual opening: 1 to 2mm increments with calibrated spreaders to the target
- Fixation: TomoFix locking plate, 3 proximal bicortical screws, 3 distal (may be unicortical)
- Graft: not needed for gaps under 10mm with modern plates; consider 10 to 15mm; recommended over 15mm
Key surgical pearls
- Biplanar technique drops the hinge-fracture rate from 20 percent to under 10 percent
- The posterior periosteal elevator MUST stay in place during sawing (protects the vessels)
- Cable technique: hip centre to ankle centre crosses 62 to 65 percent of the tibial width
- Type I hinge fracture (lateral cortex, intact posterior) = stable, proceed with the medial plate
- Type II or III hinge fracture = unstable, add a lateral plate or lag screws
- Posterior tibial slope rises about 2 degrees per 5mm of opening — limit the total increase to under 5 degrees
Complications and management
- Loss of correction 5 to 10 percent — inadequate fixation or early weight-bearing; revise if under 6 weeks
- Delayed union or nonunion 5 percent — smoking, large gap, no graft; bone graft if symptomatic at 6 months
- Compartment syndrome under 1 percent but devastating — pain out of proportion; urgent four-compartment fasciotomy
- Intra-articular fracture 1 to 2 percent — guide wire too close; if small accept, if large treat as a plateau fracture
- Peroneal nerve palsy 5 to 10 percent in closing wedge, rare in opening wedge — observe, 80 percent recover by 12 months
- Conversion to TKA 40 percent by 15 years — natural history, does NOT compromise TKA outcomes
Key evidence and outcomes
- 10-year survival about 85 to 92 percent (no conversion to TKA); open wedge about 91.6 percent versus closed wedge about 85.4 percent at 10 years (Kim 2017 meta-analysis)
- Opening versus closing wedge: equivalent PROMs and TKA-conversion risk; closing wedge preserves slope, opening wedge avoids fibular osteotomy and peroneal risk (van Haeringen 2022)
- Bone-void fillers do NOT improve union, knee scores or correction maintenance with locking-plate fixation (Mao 2022 network meta-analysis)
- Lateral hinge fracture in about a quarter of OWHTO; usually a stable type I, type II or III risk delayed union and loss of correction (Takeuchi 2011)
- TKA after a failed HTO gives good results and does not preclude later arthroplasty (Ehlinger 2017 SoFCOT series)
- Poor-outcome predictors: age over 60, BMI over 30, bicompartmental OA, undercorrection, smoking
Background & Evidence
Epidemiology. Medial compartment OA with varus malalignment is common, and HTO is most often performed in active patients aged 45 to 55 with an equal sex distribution. The procedure is more frequently used in Europe and Asia than in North America, and has seen a renaissance with modern locking-plate fixation, patient-specific planning and navigation. Around 80 to 85 percent of well-selected patients report excellent pain relief at 2 years, 60 to 70 percent return to impact activities, and median implant survival is 10 to 12 years — with about 40 percent converting to TKA by 15 years. Technique comparison.
- Approach and bone stock
- Medial; add bone. Bone stock preserved (advantage for a future TKA)
- Fixation
- Locking plate (TomoFix); bone graft optional
- Role
- Now the dominant worldwide technique, first-line for the varus knee
- Approach and bone stock
- Lateral; remove a wedge. Bone removed, shortens the limb 5 to 10mm
- Fixation
- Plate or staples; faster union, no graft
- Role
- Historical; consider for a valgus knee needing varus correction
- Approach and bone stock
- Curved multiplanar cut. Bone preserved
- Fixation
- Compression screws or plate
- Role
- Technically demanding; allows multiplanar correction. Rarely used
Ahlbäck classification of medial OA (HTO patient selection).
- Radiographic findings
- Joint space narrowing under 50 percent
- Cartilage status
- Partial-thickness cartilage loss
- HTO candidacy
- Excellent candidate; about 90 percent 10-year survival
- Radiographic findings
- Joint-space obliteration (bone on bone)
- Cartilage status
- Full-thickness loss, intact subchondral bone
- HTO candidacy
- Good candidate; about 80 to 85 percent 10-year survival
- Radiographic findings
- Bone attrition 0 to 5mm of wear
- Cartilage status
- Subchondral bone exposure, early wear
- HTO candidacy
- Relative contraindication; counsel about reduced durability
- Radiographic findings
- Bone attrition 5 to 10mm of wear
- Cartilage status
- Significant bone loss
- HTO candidacy
- Poor candidate; TKA or UKA preferred
- Radiographic findings
- Bone attrition over 10mm, subluxation
- Cartilage status
- Severe bone loss with instability
- HTO candidacy
- Absolute contraindication; HTO will fail, TKA only
Survivorship and functional outcomes.
- 2 years
- 80 to 90 percent significant improvement
- 5 to 10 years
- 70 to 80 percent sustained
- Over 10 years
- 50 to 60 percent as OA progresses
- 2 years
- 30 to 40 point gain
- 5 to 10 years
- Maintained in 70 to 80 percent
- Over 10 years
- Gradual decline
- 2 years
- 60 to 70 percent return
- 5 to 10 years
- 50 to 60 percent maintain level
- Over 10 years
- 30 to 40 percent maintain high activity
- 2 years
- 95 to 98 percent
- 5 to 10 years
- 85 to 90 percent ideal, 70 percent suboptimal
- Over 10 years
- 60 percent at 15 years, 40 percent at 20 years
Predictors of outcome. Durable results favour patients under 60 with a BMI under 30, isolated medial disease (Ahlbäck 1 to 2, pristine lateral compartment on MRI), intact menisci and cruciates, correction to 3 to 5 degrees of valgus at the Fujisawa point, a biplanar osteotomy with a stable hinge, rigid fixation and compliance with the protected weight-bearing protocol. Early failure is predicted by age over 60, BMI over 30, bicompartmental OA, undercorrection and smoking. Key evidence. Pooled data show roughly 95 percent survival at 5 years and 85 to 92 percent at 10 years, with opening wedge slightly ahead of closing wedge at 10 years (Kim 2017). Opening and closing wedge achieve equivalent patient-reported outcomes and TKA-conversion rates; closing wedge better preserves the posterior slope while opening wedge avoids fibular osteotomy and peroneal-nerve risk (van Haeringen 2022). With modern angular-stable plates, routine bone-void filling does not improve union, knee scores or correction maintenance (Mao 2022). Lateral hinge fractures occur in about a quarter of opening-wedge cases and are usually a stable Takeuchi type I (Takeuchi 2011). Conversion of a failed HTO to TKA gives good results, so HTO is a reasonable joint-preservation step that does not preclude later arthroplasty (Ehlinger 2017). Guidelines, registries & global practice.
- Pooled survival (time to TKA conversion): about 95 percent at 5 years and 85 to 92 percent at 10 years; open wedge about 91.6 percent versus closed wedge about 85.4 percent at 10 years (Kim 2017) - Best survivorship in patients under 60 with BMI under 30 and isolated medial disease - Opening wedge has become the dominant technique internationally (bone preservation, no fibular osteotomy, simpler later conversion to TKA) - Joint registries (e.g. AOANJRR, NZJR, SHAR) capture HTO in smaller volumes than arthroplasty, but reported revision-to-TKA rates are broadly consistent with the pooled literature
- AAOS, BOA or BOAST, EFORT and AO Foundation endorse HTO as a joint-preservation option for isolated medial-compartment OA with varus malalignment in appropriately selected, active patients; subspecialty or deformity training is recommended - VTE prophylaxis per institutional risk assessment (e.g. aspirin or LMWH such as enoxaparin) - Surgical antibiotic prophylaxis (commonly a first-generation cephalosporin; a glycopeptide if MRSA risk or allergy) - Documented informed consent and structured rehabilitation - Recommendations are broadly concordant across societies; differences are mainly in VTE-agent preference and rehabilitation cadence
References
Opening- vs Closing-Wedge HTO and Early Weight-Bearing: Meta-analysis
- Meta-analysis of RCTs and prospective studies comparing opening-wedge (owHTO) and closing-wedge (cwHTO) techniques, fixation, and rehabilitation
- No significant difference between owHTO and cwHTO for most pain and activity PROMs or risk of conversion to TKA
- cwHTO showed a slightly better KOOS or WOMAC pain improvement and a significantly smaller increase in posterior tibial slope
- Angular-stable (locking) plates — including TomoFix, Activmotion, 2nd-generation Puddu — showed the highest load to failure
- Early full weight-bearing was safe for small corrections without hinge fracture in non-smokers
Survival of Opening vs Closing Wedge HTO: Meta-analysis
- 23 studies pooled, survival defined as time to conversion to TKA, minimum 5-year follow-up
- 5-year survival 95.1 percent open wedge vs 93.9 percent closed wedge — no significant difference
- 10-year survival 91.6 percent open wedge vs 85.4 percent closed wedge — open wedge 6.2 percent higher
- Demonstrates durable joint preservation with both techniques into the second decade
- Most included studies were level IV, so absolute figures should be read with caution
Bone Void Fillers in Opening-Wedge HTO: Network Meta-analysis
- 25 trials (10 RCTs, 15 comparative studies), 1,420 participants, 6 filler strategies including no-graft
- No filler material was superior to leaving the gap unfilled for final Knee Society Score, WOMAC, time to union or loss of correction
- Autograft gave a higher chance of complete radiologic union at 1 year, but the overall certainty of evidence was low
- Allograft and synthetic grafts were associated with inferior complete union versus no graft in this network
- Supports omitting routine graft when stable locking-plate fixation is used
Lateral Hinge Fracture After OWHTO — Takeuchi Classification
- 104 knees; lateral cortex fractures occurred in 26 knees (25 percent) after medial opening-wedge HTO
- Classification by where the line exits: type I at or proximal to the proximal tibiofibular joint (19 of 26), type II distal to it (5 of 26), type III into the lateral plateau (2 of 26)
- No complications in any of the 19 type I fractures with standard fixation and rehabilitation
- 2 of 5 type II fractures developed delayed union with 3 and 7 degrees of loss of correction
- Defines the hinge as a key biomechanical structure and guides pattern-based management
TKA After Opening- vs Closing-Wedge HTO (SoFCOT Multicentre Series)
- 135 TKAs after prior HTO (58 opening-wedge, 77 closing-wedge), 9 centres, minimum 5-year follow-up
- Clinical results after TKA were comparable regardless of the index HTO technique
- Hardware was removed in 98.5 percent of cases — usually a single stage after opening wedge, often two-stage after closing wedge
- Most TKAs used a stemless implant (87.2 percent) and conventional technique (74.4 percent)
- Late complications (loosening, infection) were more frequent after prior closing-wedge HTO