Internervous Plane | Femoral Nerve at Risk | Extensile for Acetabular Access
- Internervous plane between tensor fasciae latae (superior gluteal nerve) and sartorius (femoral nerve) — a true internervous plane, safe for extensive dissection.
- The lateral femoral cutaneous nerve crosses the field and is the structure most often injured, producing meralgia paraesthetica in 10–20% of cases.
- An extensile approach — it can be extended with the iliofemoral extension for full 360-degree acetabular access.
- Supine positioning allows simultaneous bilateral procedures, easier anaesthesia, and no hip precautions after THA.
- The femoral nerve and vessels lie medial to sartorius — excessive medial retraction risks a stretch neuropraxia.
When & Why
What it exposes. The Smith-Petersen anterior approach gives direct access to the anterior hip capsule, femoral neck and acetabular rim, and — with the iliofemoral extension — to the entire acetabulum (anterior column, anterior wall, quadrilateral plate and superior dome). It is the workhorse exposure for anterior and both-column acetabular fractures, periacetabular osteotomy (PAO) and paediatric hip reconstruction, and underpins the direct anterior approach (DAA) for total hip arthroplasty. Why anterior. It is the only approach to the hip that uses a true internervous plane, so it tolerates extensive dissection without denervating muscle. Supine positioning is a major practical advantage: better respiratory mechanics for anaesthesia, the option of simultaneous bilateral procedures, easy C-arm access without repositioning, and — after DAA THA — no hip precautions. Historical context. Marius Nygaard Smith-Petersen described the approach in 1917 for hip arthrodesis. It was used through the mid-20th century for acetabular fractures and complex reconstruction, and was revived from the 2000s as the DAA for minimally invasive THA (the same interval, historically also termed the Hueter approach). Position & landmarks. The patient is supine on a radiolucent table (a specialised DAA traction table is optional for THA; a standard table suffices for acetabular work). Palpate and mark the anterior superior iliac spine (ASIS) — the primary landmark — the iliac crest, the greater trochanter laterally, and the femoral pulse medially. The incision is planned lateral to the femoral pulse; mark the pulse before draping and never deviate medially, where the femoral neurovascular bundle lies. The C-arm comes from the contralateral side for AP, and inlet/obturator-oblique views when needed.
- Indication strength
- Preferred by some surgeons
- Key advantage
- Muscle-sparing, faster early recovery
- Main risk
- Learning curve, LFCN injury
- Indication strength
- Gold standard with extension
- Key advantage
- Full acetabular visualization
- Main risk
- Heterotopic ossification
- Indication strength
- Standard approach
- Key advantage
- Acetabular reorientation access
- Main risk
- Protect LFCN in children
- Indication strength
- Historical indication
- Key advantage
- Wide exposure for fusion
- Main risk
- Rarely performed today
- Key feature
- Curved incision from ASIS toward greater trochanter
- Primary use
- Acetabular fractures, PAO
- Key feature
- Longitudinal incision between ASIS and greater trochanter
- Primary use
- Total hip arthroplasty
- Key feature
- More medial interval emphasis
- Primary use
- THA (historical)
- Key feature
- Proximal extension along the iliac crest
- Primary use
- Complex acetabular fractures
The Exposure
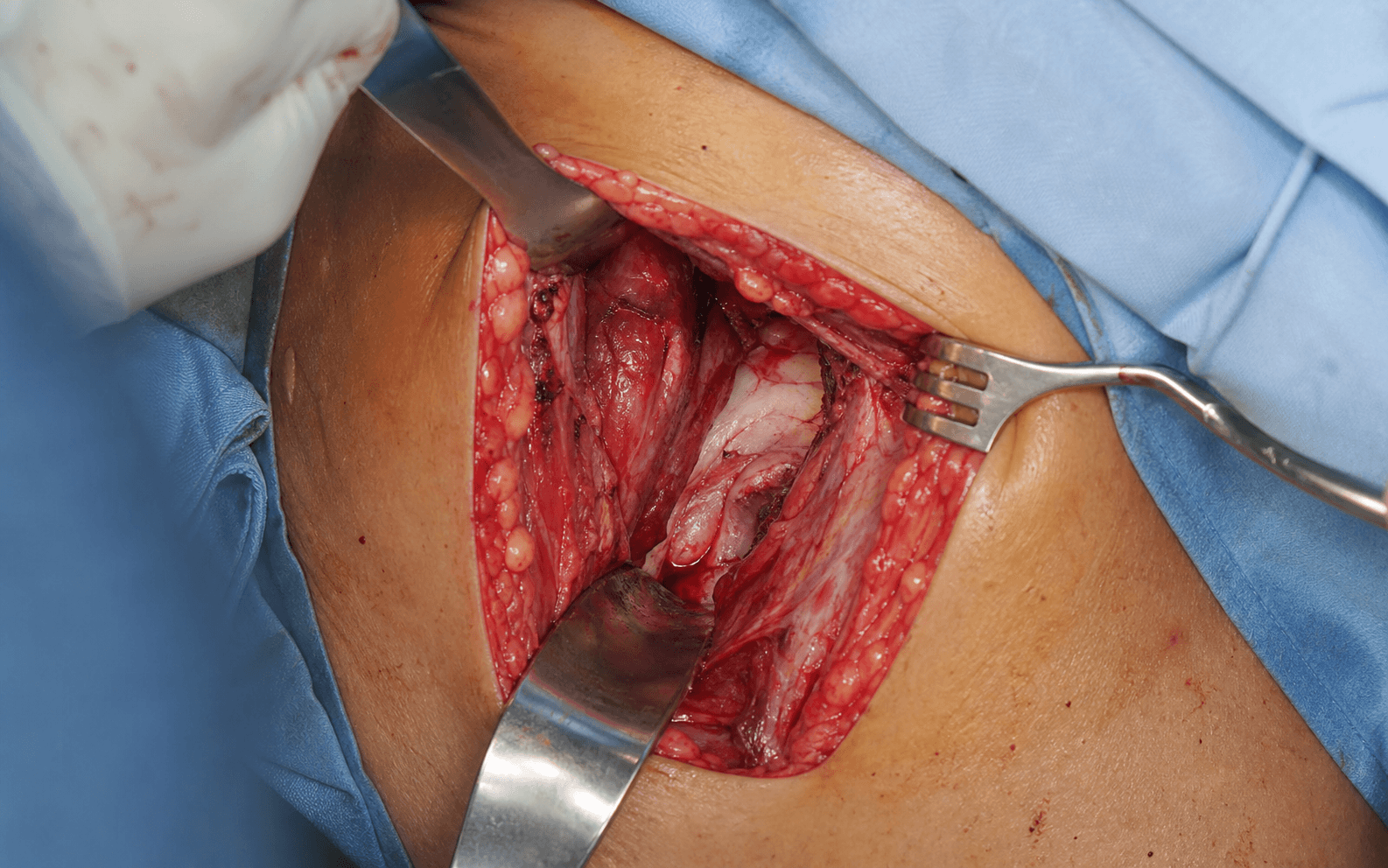
The exposure is built on a true internervous plane and developed layer by layer, protecting the lateral femoral cutaneous nerve superficially and the femoral nerve medially, then ligating the ascending branch of the lateral circumflex femoral artery before opening the capsule.
The internervous plane — the anatomical basis. The approach exploits the interval between the tensor fasciae latae (superior gluteal nerve) and sartorius (femoral nerve). A second, deeper internervous plane lies between rectus femoris (femoral nerve) medially and gluteus medius/minimus (superior gluteal nerve) laterally. Both are true internervous planes, which is what makes the approach safe for extensile dissection.
- Nerve supply
- Superior gluteal nerve (L4–S1)
- Position
- Lateral border of interval
- Function
- Hip flexion, abduction, internal rotation
- Nerve supply
- Femoral nerve (L2–L3)
- Position
- Medial border of interval
- Function
- Hip flexion, external rotation (longest muscle)
- Nerve supply
- Femoral nerve (L2–L4)
- Position
- Deep, between TFL and sartorius
- Function
- Hip flexion, knee extension (two heads: straight from AIIS, reflected from superior acetabular rim)
Exposure sequence
- Palpate the ASIS, the greater trochanter and the femoral pulse (marking the neurovascular bundle medially).
- Classic Smith-Petersen: start about 2 cm distal and lateral to the ASIS and curve distally toward the greater trochanter, 10–15 cm, staying lateral to the femoral pulse.
- DAA variant: a longitudinal incision of 8–10 cm between the ASIS and the greater trochanter, centred over the palpable interval.
- The LFCN runs in the subcutaneous layer from lateral to medial, usually 1–2 cm distal to the ASIS, passing under, through or lateral to the inguinal ligament.
- Either identify and retract it medially to preserve it, or — if it is tented across the field — divide and bury the proximal end.
- Anatomy is highly variable; counsel every patient about meralgia paraesthetica (10–20%).
- Incise the fascia lata over the tensor in line with the skin incision.
- Palpate the interval between the TFL laterally (taut, band-like) and sartorius medially (softer), and mark it.
- Bluntly develop the plane between TFL (superior gluteal nerve) and sartorius (femoral nerve) — a true internervous plane.
- Extend proximally to just below the inguinal ligament; place hand-held or cautious self-retaining retractors.
- The rectus femoris lies deep in the interval, with a straight head (from AIIS) and a reflected head (from the superior acetabular rim).
- For THA, retract rectus medially together with iliopsoas; for acetabular work, the reflected head may be released for better visualisation.
- The ascending branch of the LCFA runs between rectus and TFL and is a consistent bleeder if not addressed.
- Identify and ligate or clip it early for haemostasis; avoid diathermy close to the nerve.
- Retract TFL laterally and sartorius with rectus medially to expose the anterior hip capsule.
- THA: T-shaped or inverted-L capsulotomy (longitudinal along the femoral neck, transverse along the acetabular rim). Acetabular: limited capsulotomy/capsulectomy to the anterior column and rim. Paediatric DDH: a superiorly-based capsular flap, preserved for closure.
- Identify the femoral neck, acetabular rim, transverse acetabular ligament and labrum.
The femoral nerve lies medial to the operative field, deep to sartorius. Excessive medial retraction or prolonged retractor pressure causes a stretch neuropraxia presenting as postoperative quadriceps weakness and loss of knee extension. Use self-retaining retractors cautiously, place them lateral to the neurovascular bundle, and release them periodically.
This is the only true internervous plane approach to the hip. Both the superficial plane (TFL versus sartorius) and the deep plane (rectus femoris versus gluteus medius/minimus) are internervous, so extensive dissection — including the iliofemoral extension for 360-degree acetabular access — can be performed without motor denervation.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Lateral femoral cutaneous nerve (crosses field; 10–20% injury)
- Protection
- Incise lateral to the femoral pulse; identify and protect or divide with consent; counsel about meralgia paraesthetica
- Structure at risk
- Ascending branch of the lateral circumflex femoral artery
- Protection
- Identify and ligate early for haemostasis
- Structure at risk
- Femoral nerve and vessels
- Protection
- Avoid excessive medial retraction; place retractors lateral to the bundle; release periodically
- Structure at risk
- Superior gluteal nerve (to TFL)
- Protection
- Stay superficial to the muscle; avoid aggressive deep lateral retraction
Lateral femoral cutaneous nerve variability (cadaveric). The LFCN is highly variable and cannot always be preserved. Across cadaveric series it crosses the DAA skin incision in roughly 42–65% of specimens (Sugano 42%; Ukai 64.9%; Giang 50%); shortening the proximal extent of the incision lowers the crossing rate.
- Description
- Posterior branch thicker than or equal to anterior (Sugano)
- Reported frequency
- ~63% (Sugano, n=64 thighs)
- Surgical implication
- Branches fan toward TFL — higher chance of crossing the incision
- Description
- Thicker anterior branch along the medial border of TFL
- Reported frequency
- ~37% (Sugano)
- Surgical implication
- Often medial to the incision — more protectable
- Description
- Multiple divergent branches below the inguinal ligament
- Reported frequency
- ~40% (Giang, n=30 hips)
- Surgical implication
- Multiple branches cannot all be protected
- Description
- Branch crossing over or through the sartorius region
- Reported frequency
- ~37% (Giang)
- Surgical implication
- Crosses the field — moderate risk
Complications
- Incidence
- 10–20%
- Prevention / management
- Careful lateral dissection; identify/protect; counsel preoperatively; most recover over 6–12 months
- Incidence
- 1–3% (usually temporary)
- Prevention / management
- Avoid excessive medial retraction; release retractors periodically
- Incidence
- Common (manageable)
- Prevention / management
- Identify and ligate the ascending branch early
- Incidence
- 1–2% (learning-curve dependent)
- Prevention / management
- Careful broaching, fluoroscopy, avoid varus; extend wound if difficult
- Incidence
- 10–20%
- Prevention / management
- Indomethacin prophylaxis or radiation; minimise soft-tissue stripping
- Incidence
- 1–2% (THA), 5–10% (trauma)
- Prevention / management
- Standard prophylaxis; minimise tissue trauma
- Incidence
- 2–5%
- Prevention / management
- Careful haemostasis; consider a drain for trauma cases
LFCN injury management. Most injuries are neuropraxic and recover over 6–12 months; permanent numbness occurs in only 5–10% and is usually well tolerated. Neuropathic pain may need gabapentin or pregabalin; surgical exploration is rarely indicated. Always distinguish LFCN injury (sensory only) from a femoral nerve injury (quadriceps weakness). Extensile option — the iliofemoral extension. For full acetabular access, extend the incision proximally along the iliac crest, detach the abdominal wall muscles (external oblique, internal oblique, transversus) from the crest, and reflect the iliacus subperiosteally from the inner table working lateral to medial. This exposes the pelvic brim, quadrilateral plate and anterior column and gives 360-degree acetabular visualisation. Both-column fractures can often be fixed through this single approach, because stabilising both columns to the intact ilium secures the fracture without a posterior approach. Closure. Repair the capsule (always, for fracture and paediatric cases; surgeon preference for THA), close the TFL–sartorius fascial interval if opened widely (absorbable suture), close dead space with attention to haemostasis (a drain is favoured for acetabular trauma), and close skin with a subcuticular suture or staples.
Procedures Through This Approach
- Total hip arthroplasty via the direct anterior approach (DAA) — the principal elective operation; muscle-sparing, supine, and no hip precautions postoperatively. Femoral exposure is the limiting factor (hardest in muscular or obese patients, BMI over 35).
- Acetabular fracture ORIF — anterior column, anterior wall, both-column and anterior column/posterior hemitransverse patterns (Judet-Letournel). Elementary types: anterior wall, anterior column, posterior wall, posterior column, transverse. Associated types: both-column (the commonest associated pattern, ~25%), T-shaped, transverse + posterior wall, anterior column/posterior hemitransverse, anterior wall/posterior hemitransverse. Postoperatively: touch weight-bearing for 6 weeks and heterotopic ossification prophylaxis (indomethacin 75 mg daily for 3 weeks, or a single 700 cGy radiation dose).
- Periacetabular osteotomy (PAO), Pemberton osteotomy and DDH open reduction — standard exposure for acetabular reorientation and paediatric hip reconstruction.
- Hip arthrodesis — Smith-Petersen's original 1917 indication; rarely performed today.
- Iliopsoas tenotomy — for symptomatic iliopsoas impingement after THA, via lesser trochanter access.
- Anterior hip arthroscopy portal placement — uses the same landmarks and internervous plane.
Unlike the posterior approach, anterior approach THA does not require hip precautions — patients may flex, adduct and internally rotate without restriction, which supports faster early recovery (the advantage narrows to equivalence by one year).
Viva & Exam Focus
SARTORSARTOR — the anterior interval
LFCNLFCN — the structure at risk
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the anterior approach to the hip (Smith-Petersen). What is the internervous plane and what structures are at risk?”
“During a primary THA via the direct anterior approach, after the femoral neck osteotomy you cannot access the femoral canal because of a muscular thigh. What are your options?”
“A patient returns two weeks after anterior approach THA with anterolateral thigh numbness and dysesthesia. What is the likely diagnosis and how do you manage it?”
Key anatomy
- Internervous plane: TFL (superior gluteal) vs sartorius (femoral)
- LFCN crosses the field — 10–20% injury rate (meralgia paraesthetica)
- Femoral nerve lies medial — protect from stretch injury
- Rectus femoris lies deep between TFL and sartorius
- Ascending branch of the lateral circumflex femoral artery — ligate early
Indications
- THA via DAA — muscle-sparing, faster recovery
- Acetabular fractures — anterior column, both-column with extension
- Paediatric hip — DDH, PAO, Pemberton osteotomy
- Extensile with iliofemoral extension for full acetabular access
Positioning and setup
- Supine position — allows bilateral procedures, easier anaesthesia
- C-arm from the contralateral side
- Incision: ASIS toward greater trochanter region
- Mark the femoral pulse — stay lateral to the neurovascular bundle
Surgical steps
- Step 1: Incise 2 cm distal-lateral to ASIS, curving toward the greater trochanter
- Step 2: Identify and protect the LFCN in the subcutaneous layer
- Step 3: Open fascia between TFL (lateral) and sartorius (medial)
- Step 4: Develop the internervous plane bluntly
- Step 5: Identify rectus femoris deep in the interval
- Step 6: Ligate the ascending branch of the LCFA
- Step 7: Expose the anterior capsule and perform the capsulotomy
Complications
- LFCN injury: 10–20%, causes meralgia paraesthetica
- Femoral nerve stretch: 1–3%, causes quadriceps weakness
- Proximal femoral fracture: 1–2% (THA), limited femoral visualisation
- LCFA bleeding: consistent if not ligated early
- Heterotopic ossification: 10–20% in trauma cases
Key evidence
- Smith-Petersen 1917: original description for hip arthrodesis
- True internervous plane: safe for extensive dissection
- DAA meta-analysis: faster early recovery, no long-term difference
- LFCN injury: consistent 10–20% across studies
- Letournel: gold standard for anterior acetabular access
References
Approach data across major joint registries (side by side)
- Region
- England, Wales, Northern Ireland
- Relevant finding
- Posterior remains the most common approach; no clinically meaningful difference in revision between anterior and posterior at medium term
- Region
- Australia
- Relevant finding
- Rapidly rising DAA utilisation; tracks higher early revision during the learning curve
- Region
- United States
- Relevant finding
- Largest growth in DAA utilisation internationally; approach-specific outcome tracking
- Region
- Sweden / Norway
- Relevant finding
- Long implant survivorship data; surgeon and unit volume are strong outcome predictors
Named-society guidance and global practice. AAOS (US) and NICE / BOA (UK) do not mandate a single surgical approach for primary THA — approach choice rests on surgeon expertise and patient factors, with equivalent long-term outcomes emphasised. AO Foundation / Letournel-Judet principles underpin the Smith-Petersen, iliofemoral and anterior intrapelvic approaches for anterior column and both-column acetabular fractures. Informed consent should specifically cover LFCN injury and meralgia paraesthetica, the learning-curve risk (intraoperative femoral fracture within the first roughly 30–50 cases), and the possibility of wound extension or approach conversion for difficult femoral exposure. Specialised DAA traction tables and femoral elevators are used in some centres; a standard radiolucent table is adequate for the classic Smith-Petersen and for acetabular work, and the underlying internervous anatomy is identical worldwide.
Smith-Petersen Original Description (historical)
- Original description of the anterior approach to the hip for arthrodesis
- Defined the internervous interval between tensor fasciae latae and sartorius
- Established the anatomical foundation for the modern direct anterior approach (DAA)
- Subsequently popularised as the Hueter anterior interval for THA
DAA vs Posterior Approach THA — Meta-analysis of RCTs
- Meta-analysis of randomised controlled trials, 932 patients (467 DAA, 465 posterior)
- Markedly higher LFCN injury with DAA (RR 38.97, 95% CI 7.89–192.57)
- Less early postoperative pain with DAA (WMD -0.65)
- Earlier cessation of walking aids with DAA; more cups within the Lewinnek safe zone
- No significant difference in operative time, hospital stay or intraoperative blood loss
DAA vs Mini-Posterior THA — Randomised Trial at 7.5 Years
- RCT of DAA versus mini-posterior approach, 93 of 101 patients reviewed at mean 7.5 years
- Similar Harris Hip, SF-12 and HOOS scores between groups
- No clinical outcome reached the minimal clinically important difference
- Few complications in each group (DAA: 1 revision for femoral loosening; MPA: 3 dislocations)
- Early functional advantages of DAA did not translate into meaningful midterm differences
LFCN Anatomy and Crossing of the DAA Incision (cadaveric)
- Cadaveric study of 37 hemipelves comparing DAA and anterolateral supine incisions
- 64.9% of DAA incisions crossed the LFCN versus 27% for the anterolateral supine incision
- LFCN lay significantly closer to the DAA incision (median 10 mm vs 27 mm)
- DAA crossed the LFCN most often at the proximal third of the incision
- Shortening the proximal incision by 10 mm reduced crossing by ~25%
LFCN Branching Patterns and Injury Risk in DAA (cadaveric)
- 64 thighs from 45 cadavers studied for LFCN branching relative to the DAA
- Posterior-dominant branching in 63%, anterior-dominant in 37%
- LFCN crossed the planned skin incision along the midline of TFL in 42% of thighs
- Highly variable branching means the nerve cannot always be protected
- Defines a relative safe zone for the DAA skin incision