Interval between TFL and gluteus medius | Superior gluteal nerve at risk | Workhorse for primary THA
- Not a true internervous plane - tensor fascia lata and gluteus medius are both supplied by the superior gluteal nerve.
- Superior gluteal nerve crosses the interval about 5 cm proximal to the greater trochanter tip; dissection or retraction beyond this risks denervation of the abductors and a Trendelenburg gait.
- Muscle-sparing modification (current standard) splits TFL longitudinally and reflects gluteus medius posteriorly without detaching it, reducing Trendelenburg gait from 15 to 20 percent toward under 5 percent.
- Can be performed supine or lateral decubitus - surgeon preference and familiarity drive the choice.
- Abductor preservation is the key principle - avoid detachment, protect the nerve, and repair any inadvertent tears.
- Described by Watson-Jones in 1936 for hip arthrodesis and fracture management.
When & Why
What it exposes. The Watson-Jones anterolateral approach gives direct access to the hip joint, the femoral neck and the acetabulum through the interval between tensor fasciae latae (anterior) and gluteus medius (posterolateral). It is a workhorse exposure for primary total hip arthroplasty and femoral neck fracture management, and can be performed with the patient supine or lateral decubitus. Why anterolateral (and not anterior or posterior). It is frequently confused with the anterior (Smith-Petersen) approach - a common exam trap. Watson-Jones uses the TFL–gluteus medius interval (both supplied by the superior gluteal nerve, so NOT internervous), whereas Smith-Petersen uses the TFL–sartorius interval (superior gluteal versus femoral nerve, a TRUE internervous plane). Versus the posterior approach, anterolateral preserves the posterior capsule and short external rotators, giving a lower dislocation rate at the cost of higher abductor risk. Historical context. Sir Reginald Watson-Jones described the approach in 1936 for hip arthrodesis and fracture management. It was popular through the 1950s to 1970s, fell from favour in the 1980s to 1990s due to abductor complications, and was revived in the 2000s with muscle-sparing modifications (the Röttinger/OCM intermuscular variant) that split TFL rather than detaching it. Indications.
- Indication strength
- Common approach choice
- Key advantage
- Familiar anatomy, supine or lateral positioning
- Main risk
- Superior gluteal nerve if dissection too proximal
- Indication strength
- Good option for fracture work
- Key advantage
- Quick access, less bleeding than posterior
- Main risk
- Abductor damage if hasty dissection
- Indication strength
- Useful for acetabular exposure
- Key advantage
- Better acetabular visualization
- Main risk
- Limited femoral exposure for complex femoral revisions
- Indication strength
- Familiar corridor if scoped first
- Key advantage
- Same interval as anterolateral portal
- Main risk
- Iatrogenic labral or cartilage damage
Contraindications. - Relative: severe obesity (BMI over 40) - difficult exposure and higher complication rate; prior anterolateral surgery with known abductor damage; pre-existing superior gluteal nerve palsy; severe osteoporosis (fracture risk with retraction).
- Active infection is a general contraindication to elective arthroplasty. Position & landmarks. Supine (with a bump under the ipsilateral hip, allowing 20 to 30 degrees of pelvic tilt) suits trauma, permits bilateral procedures and eases anaesthesia. Lateral decubitus (pelvis held perpendicular to the floor with anterior and posterior supports) gives better acetabular exposure as gravity assists. Palpate and mark the greater trochanter (primary landmark), the ASIS and the iliac crest, and plan a curvilinear incision centred over the trochanter. The defining concept: not a true internervous plane. The interval lies between TFL and gluteus medius, but both are supplied by the superior gluteal nerve (L4 to S1), so this is an intranervous interval rather than an internervous one. The superior gluteal nerve exits the pelvis through the greater sciatic notch superior to piriformis, divides into a superior branch (to gluteus medius and minimus) and an inferior branch (to TFL), and crosses the interval about 5 cm proximal to the greater trochanter tip - the origin of the 5 cm rule that governs proximal dissection.
- Nerve supply
- Superior gluteal nerve (L4 to S1)
- Position
- Anterior border of interval
- Function
- Hip flexion, abduction, internal rotation
- Nerve supply
- Superior gluteal nerve (L4 to S1)
- Position
- Posterolateral border of interval
- Function
- Hip abduction (primary), pelvic stabilization in gait
- Nerve supply
- Superior gluteal nerve (L4 to S1)
- Position
- Deep to gluteus medius
- Function
- Hip abduction; anterior fibres internally rotate
Deep structures encountered: the hip joint capsule (accessed after splitting TFL and reflecting gluteus medius), the reflected head of rectus femoris from the superior acetabular rim, the iliofemoral ligament (strongest hip ligament, anterior capsule), and the ascending branch of the lateral circumflex femoral artery running deep, which requires ligation.
The Exposure
Work from skin down to capsule along the TFL–gluteus medius interval, protecting the superior gluteal nerve and the abductors at every step. The muscle-sparing modification is the modern standard - split TFL rather than detach it.
Exposure sequence
- Landmarks: greater trochanter (primary), ASIS (anterior reference); the incision follows the line from ASIS toward the lateral GT.
- Classic Watson-Jones: start about 5 cm distal and posterior to the ASIS, curve distally toward and over the greater trochanter, then continue distally along the femoral shaft; total length 10 to 15 cm, centred on the TFL–GM interval.
- Muscle-sparing variant: a shorter incision of 8 to 10 cm centred over the GT with a more vertical orientation along the femoral shaft.
- Centre the incision over the GT - too anterior misses the trochanter and hampers femoral exposure; too posterior encroaches on the gluteus medius insertion.
- Deepen through subcutaneous fat with cutting diathermy; secure haemostasis of skin-edge bleeders and stay perpendicular to minimise subcutaneous stripping.
- Identify the glistening white fascia lata and iliotibial band.
- Incise the fascia in line with the skin over the GT and distally along the femoral shaft; proximally, stay within 5 cm of the GT tip to protect the superior gluteal nerve.
- Define the muscular interval: TFL anteriorly (soft, mobile) and gluteus medius posteriorly (firm, taut over the GT); release any fascial condensation between them with scissors.
- Split TFL longitudinally along its oblique fibres (5 to 8 cm) with scissors or diathermy, preserving all bony attachments - do NOT detach it from the GT (the original technique detached TFL and the anterior third of gluteus medius and is now avoided).
- Reflect gluteus medius posteriorly without bony detachment; use gentle retraction to avoid muscle damage and identify gluteus minimus lying deep to medius.
- The ascending branch of the lateral circumflex femoral artery runs deep between the muscles and the capsule.
- Identify it and ligate with ties or clips early (avoid diathermy close to the nerve) - it is a consistent bleeder and should be addressed before deeper work.
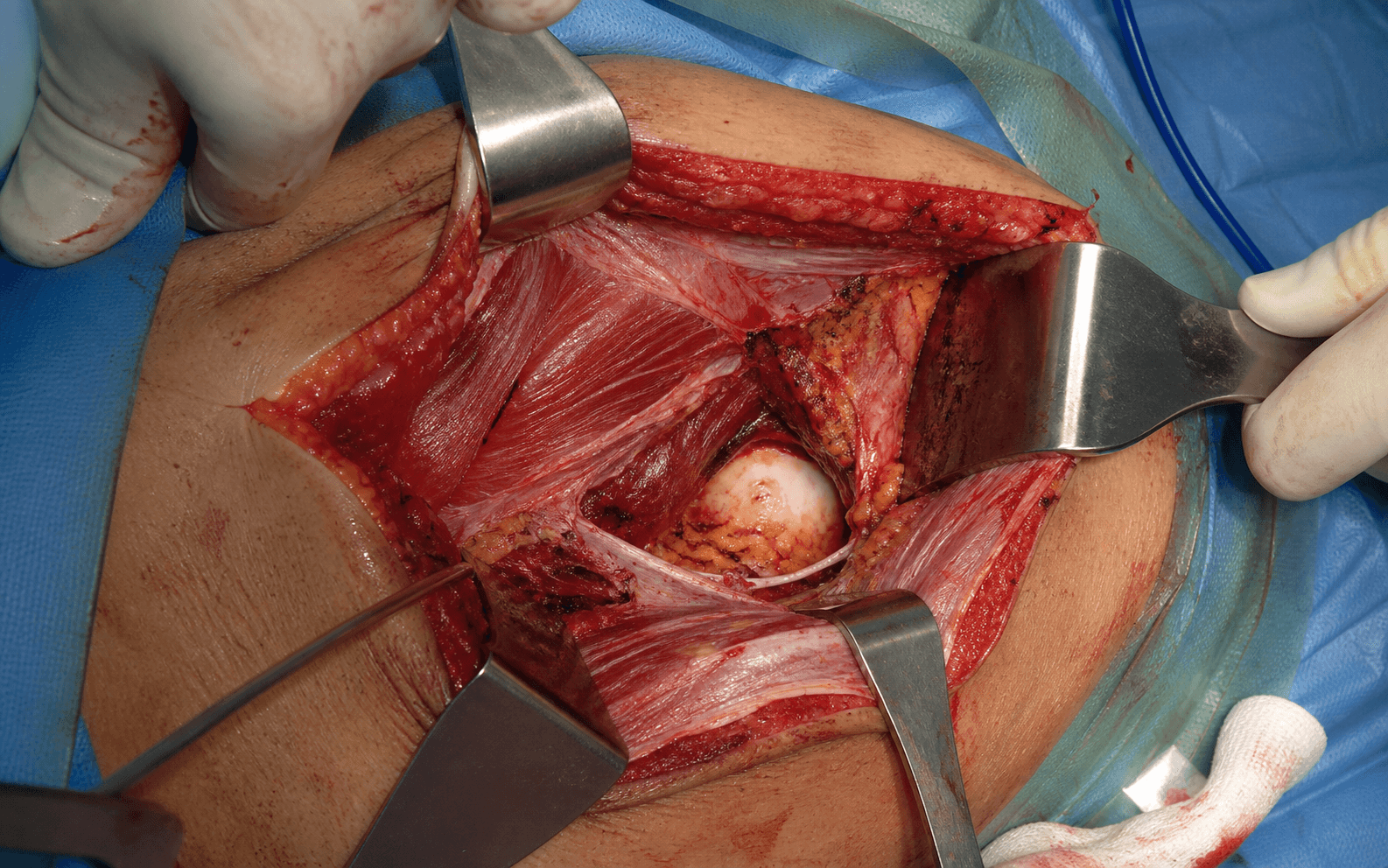
- Retract TFL anteriorly and gluteus medius posteriorly to expose the anterior and lateral hip capsule.
- Identify the reflected head of rectus femoris (superior, from the acetabular rim) and feel the femoral neck through the capsule.
- Make a T-shaped capsulotomy (longitudinal limb along the femoral neck plus transverse limb along the acetabular rim) - the common choice for THA; tag the edges with stay sutures if planning repair. An H-shaped capsulotomy or a limited capsulotomy is used for specific indications.
- Stay extracapsular until the deliberate capsulotomy, then expose the femoral neck and acetabular rim.
- Femoral neck osteotomy: flex and externally rotate the hip and cut in situ at the templated level with an oscillating saw; remove the head with a corkscrew or bone hook.
- Acetabular exposure: place retractors around the acetabular rim, excise labrum and osteophytes, ream to bleeding bone aiming for about 40 to 45 degrees inclination and 15 to 20 degrees anteversion, then implant the cup.
- Femoral preparation: extend and externally rotate the hip, deliver the proximal femur, open and broach the canal aiming for about 10 to 15 degrees anteversion.
- Trial reduction: confirm stability through range of motion, leg length, offset and absence of impingement before final implantation.
The superior gluteal nerve crosses the interval about 5 cm proximal to the tip of the greater trochanter. Do not extend the fascial incision, split TFL, or retract more than about 5 cm proximal to the GT - beyond this, dissection or retraction risks denervation of gluteus medius and minimus and a Trendelenburg gait. Cadaveric work confirms the most distal branch lies about 5.5 cm up and that a true fixed safe zone does not exist, so gentle retraction matters as much as the distance itself (Khan 2007; Zhou 2020).
Too anterior and you miss the GT, making femoral exposure difficult; too posterior and you encroach on the gluteus medius insertion and risk damage. The incision should sit squarely over the trochanter, following the TFL–GM interval.
Splitting TFL longitudinally and reflecting gluteus medius posteriorly without bony detachment preserves the abductor mechanism, reduces abductor weakness, speeds recovery, and lowers the Trendelenburg gait incidence from 15 to 20 percent toward under 5 percent. The original detach-and-reflect technique is now rarely used.
Most surgeons do NOT routinely repair the capsule after anterolateral THA (unlike the posterior approach, where capsule and short-external-rotator repair is standard). Consider repair for added stability in the trauma setting or where component position raises instability concern.
Dangers & Extensions
Structures at risk, by layer
- Location
- About 5 cm proximal to GT
- Mechanism of injury
- Proximal dissection or retraction
- Prevention
- Stay within 5 cm of GT tip; gentle retraction
- Location
- Lateral hip
- Mechanism of injury
- Retraction injury or inadvertent tears
- Prevention
- Muscle-sparing technique; repair any tears
- Location
- Deep interval
- Mechanism of injury
- Bleeding
- Prevention
- Identify and ligate early
- Location
- Femur
- Mechanism of injury
- Broaching or reaming
- Prevention
- Careful technique with adequate exposure
Complication rates. - Superior gluteal nerve injury: 1 to 5 percent, producing a Trendelenburg gait.
- Abductor muscle damage: 5 to 15 percent, technique-dependent.
- Heterotopic ossification: 10 to 20 percent overall (higher than posterior); clinically significant Brooker grade III to IV in 3 to 5 percent.
- Dislocation: under 2 percent (lower than the posterior approach).
A Trendelenburg gait after anterolateral THA - the pelvis drops on the contralateral side during single-leg stance on the affected leg - indicates abductor dysfunction from nerve injury, muscle damage, or both. Temporary in 5 to 10 percent, permanent in 1 to 3 percent; prevention (the 5 cm rule and muscle-sparing technique) is the key.
- Anterolateral
- 1 to 2%
- Posterior
- 2 to 3%
- Direct anterior
- under 1%
- Anterolateral
- 5%
- Posterior
- under 2%
- Direct anterior
- 2 to 3%
- Anterolateral
- 15%
- Posterior
- 10%
- Direct anterior
- 8%
- Anterolateral
- Equivalent
- Posterior
- Equivalent
- Direct anterior
- Equivalent
- Description
- Islands of bone in soft tissue
- Clinical impact
- Minimal
- Description
- Bone spurs from pelvis or femur with gap over 1 cm
- Clinical impact
- Minimal
- Description
- Bone spurs with gap under 1 cm
- Clinical impact
- May limit motion
- Description
- Apparent bony ankylosis
- Clinical impact
- Severe ROM limitation
- Pathology
- Neurapraxia (conduction block)
- Prognosis
- Complete recovery in weeks
- Pathology
- Axonotmesis (axon damage)
- Prognosis
- Recovery over months
- Pathology
- Partial endoneurial damage
- Prognosis
- Variable recovery
- Pathology
- Perineurial damage
- Prognosis
- Poor without surgery
- Pathology
- Complete transection
- Prognosis
- No recovery without repair
Procedures Through This Approach
- Total hip arthroplasty - the principal operation. Acetabular targets are about 40 to 45 degrees inclination and 15 to 20 degrees anteversion; the femoral stem is set at about 10 to 15 degrees anteversion, with offset and leg length restored and stability confirmed on trial reduction.
- Femoral neck fracture - quick joint access for hemiarthroplasty or THA in the elderly, and exposure for screw fixation in the young displaced or non-displaced fracture; supine positioning suits the trauma setting.
- Revision THA (acetabular) - excellent cup and liner exposure; less suited to complex femoral revision (posterior preferred).
- Hip arthroscopy conversion - the anterolateral portal uses the same anatomical corridor, allowing conversion to open if arthroscopy cannot be completed.
- Hip arthrodesis (historical) - Watson-Jones' original indication; rarely performed in modern practice. Postoperative course. Mobilise on day 0 to 1 with full weight-bearing as tolerated (modern implants); abductor strengthening is especially important for this approach. Hip precautions after anterolateral THA are controversial - many surgeons use none, while some avoid extremes of flexion, adduction and internal rotation for 6 weeks. VTE prophylaxis follows local protocol (for example rivaroxaban 10 mg daily, enoxaparin 40 mg daily, or aspirin 100 mg daily) combined with mechanical prophylaxis and early mobilisation. Follow up at 2 weeks (wound check and staple removal), 6 weeks, 3 months, 1 year, then annually; most patients reach maximum improvement by 6 to 12 months.
Viva & Exam Focus
WATSONWATSON - key features of the approach
5CM5 CM RULE - superior gluteal nerve protection
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the Watson-Jones anterolateral approach to the hip. Is this a true internervous plane, and what structures are at risk?”
“A patient is 6 weeks post-THA via an anterolateral approach and has developed a noticeable limp with a positive Trendelenburg test. What is your assessment and management?”
“You are planning a primary THA for a 65-year-old active patient. What are the pros and cons of the anterolateral (Watson-Jones) versus the posterior approach, and how would you counsel the patient?”
Key anatomy
- Interval: TFL (anterior) versus gluteus medius (posterolateral)
- NOT internervous - both supplied by the superior gluteal nerve
- Superior gluteal nerve about 5 cm above the GT tip - stay distal
- Injury causes Trendelenburg gait (gluteus medius and minimus denervation)
- Ascending branch of the lateral circumflex femoral artery - ligate
Indications
- Primary THA - popular approach in some regions
- Femoral neck fractures - hemi or THA
- Revision THA - particularly acetabular work
- Can be performed supine or lateral
Surgical steps (muscle-sparing)
- Incision: ASIS region to GT, then along the femoral shaft
- Incise fascia lata over the GT (stay within 5 cm proximal)
- Split TFL longitudinally - preserve attachments
- Reflect gluteus medius posteriorly - no detachment
- Ligate the ascending LCFA branch
- T-shaped capsulotomy
Complications
- Superior gluteal nerve injury: 1 to 5% (Trendelenburg gait)
- Abductor muscle damage: 5 to 15%
- Trendelenburg gait: 5 to 10% temporary, 1 to 3% permanent
- Heterotopic ossification: 10 to 20% (higher than posterior)
- Dislocation: under 2% (lower than posterior)
Muscle-sparing versus traditional
- Traditional: detach TFL and anterior gluteus medius from the GT
- Muscle-sparing: split TFL, reflect gluteus medius, preserve attachments
- Muscle-sparing reduces Trendelenburg from 15 to 20% toward under 5%
- Modern standard: always use the muscle-sparing technique
- Repair any inadvertent tears in gluteus medius
Key evidence and exam points
- Watson-Jones 1936: original description
- NOT internervous plane (common exam mistake)
- 5 cm rule: superior gluteal nerve protection
- Dislocation 1.4% (lower than posterior 2.9%)
- Trendelenburg 5% (higher than posterior under 2%)
- Surgeon experience is more important than approach choice
References
Guidelines, registries and global practice. - Global practice variation: the anterolateral (Watson-Jones or Röttinger) interval is used worldwide but is less common than the posterior and direct lateral approaches in most national registries; it is more popular in parts of continental Europe (where the Röttinger/OCM muscle-sparing variant originated) than in the UK or North America. Surgeon training and familiarity, rather than country, drive approach choice.
- Registry evidence (approach and outcomes): major arthroplasty registries (NJR for England, Wales and Northern Ireland; AJRR in the US; AOANJRR in Australia; the Swedish and Norwegian registries) record surgical approach and track approach-specific revision and dislocation. Across registries, primary THA implant survival is broadly equivalent between approaches when performed by experienced surgeons; differences in early dislocation and revision-for-instability are the main approach-related signals. Abductor-based approaches show a lower dislocation risk but a higher loosening and abductor-deficiency signal than the posterior approach in pooled data.
- Named-society guidance (side by side): AAOS (US) and NICE or BOA (UK) do not mandate a specific approach for primary THA and emphasise surgeon experience and audited outcomes; AO Foundation and EFORT (Europe) recognise the muscle-sparing anterolateral interval as a valid exposure for primary THA and displaced femoral neck fracture. All major societies agree that informed consent must include approach-specific risks.
- Informed consent (approach-specific): superior gluteal nerve injury and Trendelenburg gait (temporary versus permanent weakness), heterotopic ossification and the role of prophylaxis in high-risk patients, and documentation of the discussion.
- Venous thromboembolism prophylaxis: follow current national society guidance (for example AAOS, NICE or equivalent); combine mechanical and pharmacological prophylaxis with early mobilisation. Agents include aspirin, low-molecular-weight heparin, or a direct oral anticoagulant per local protocol and individual risk.
Watson-Jones Original Description
- Original description of the anterolateral approach for hip arthrodesis
- Described the interval between TFL and gluteus medius
- Noted both muscles are supplied by the superior gluteal nerve
- Emphasized the need to preserve the abductor mechanism
- Established the approach for the pre-arthroplasty era of hip surgery
Superior Gluteal Nerve Damage in Anterolateral/Lateral Hip Exposure (Cadaveric)
- Cadaveric dissection of 44 hips after a lateral or abductor-splitting exposure
- Inferior division of the superior gluteal nerve damaged in 3 of 44 (6.8%)
- Authors conclude a true anatomical safe zone does NOT exist
- Nerve injury depends largely on the individual branching pattern of the SGN
- The inferior division is the main motor supply to the abductors
Anterolateral Mini-Incision THA: A Modified Watson-Jones Approach
- Describes the intermuscular plane between gluteus medius and tensor fasciae latae (Röttinger or OCM technique)
- Avoids splitting the anterior gluteus medius and minimus used in traditional lateral exposures
- Aims to spare the abductors and the superior gluteal nerve and to keep the posterior capsule intact
- Reported reduced abductor weakness, limp and faster rehabilitation versus muscle-detaching approaches
- Provides adequate exposure for both acetabular and femoral preparation through a small incision
THA Approach Complication Rates: Systematic Review and Meta-analysis
- 69 studies, 283,036 patients, comparing posterior, anterior, anterolateral and direct lateral approaches
- Versus posterior, dislocation risk significantly lower for anterolateral (RR 0.50, 95% CI 0.32 to 0.77)
- Anterior (RR 0.66) and direct lateral (RR 0.74) also had lower dislocation than posterior
- Anterolateral and lateral approaches had HIGHER risk of implant loosening than posterior (anterolateral RR 1.89)
- Overall GRADE quality low to very low; no approach proven definitively superior
Anatomy of the Gluteus Medius Split and Superior Gluteal Neurovascular Bundle
- Cadaveric and skeletal study (20 hips) measuring the abductor split safe limit
- Most distal branch of the superior gluteal nerve lay a mean 5.70 plus or minus 0.66 cm from the greater trochanter reference point
- Corresponding artery lay a mean 6.33 plus or minus 0.56 cm proximal
- Authors recommend limiting the proximal gluteus medius split to about 5.5 cm
- Confirms the neurovascular bundle, not just the nerve, defines the proximal limit
Anterolateral Minimally Invasive (Röttinger) vs Hardinge THA: RCT
- Randomised controlled trial of 79 primary THAs
- Röttinger anterolateral MIS (n equals 42) versus standard lateral transgluteal Hardinge (n equals 41)
- The anterolateral MIS group had longer operative time but lower blood loss
- Similar complication rates, analgesia use, length of stay and gait analysis
- Harris and SF-36 scores, implant position, HO and loosening equivalent at 1 year