True internervous plane | Sciatic nerve at risk | Capsular repair reduces dislocation
- True internervous plane between the superior gluteal nerve (gluteus medius) and the inferior gluteal nerve (gluteus maximus) — the only hip approach with a true internervous plane.
- Sciatic nerve runs approximately 1cm medial to the greater trochanter and posterior to the acetabulum — protect it throughout the case.
- Piriformis can be divided (Moore) or preserved (Southern) — both are acceptable provided the capsule and short externals are repaired.
- Posterior soft-tissue repair (capsule plus short external rotators) cuts dislocation roughly 8-fold (Kwon meta-analysis: 4.46% to 0.49%).
- Flexion, adduction and internal rotation is the dislocation position — educate the patient post-operatively.
When & Why
What it exposes. The posterior (Moore/Southern) approach gives versatile, extensile access to the hip joint — the femoral head and neck, the acetabulum (with particularly good exposure of the posterior wall and column), and the proximal femur. It is the workhorse exposure for primary total hip arthroplasty, hemiarthroplasty for femoral neck fracture, and many revision procedures, and it remains the most commonly used approach to the hip worldwide. The eponyms. The approach was popularised by Austin Moore in the 1950s (and the eponymous Austin Moore prosthesis); the "Southern" name derives from the Southern General Hospital, Glasgow. The two terms are used interchangeably for the same exposure. Why posterior. The decisive advantage is the only true internervous plane of any hip approach — between gluteus maximus (inferior gluteal nerve) and gluteus medius (superior gluteal nerve) — so no muscle is denervated and abductor function is preserved. It is extensile in both directions, gives superb posterior-column exposure for trauma and revision, and avoids abductor takedown. Its chief weaknesses are posterior instability if the soft tissues are not repaired, and the sciatic nerve lying in the field.
- Posterior approach
- Excellent — true internervous plane, familiar
- Alternative
- Lateral or anterior also acceptable
- Key pearl
- Commonest THA approach worldwide; equivalent revision rates in major registries
- Posterior approach
- Best choice — direct posterior access
- Alternative
- No good alternative
- Key pearl
- Superior posterior column and wall exposure
- Posterior approach
- Excellent — extends proximally and safely
- Alternative
- Lateral approach limited proximally by the superior gluteal nerve
- Key pearl
- No proximal nerve danger with the posterior approach
- Posterior approach
- Acceptable if posterior soft tissues are repaired
- Alternative
- Consider the anterior approach (lower native dislocation)
- Key pearl
- Posterior soft-tissue repair is mandatory — reduces dislocation roughly 8-fold
Position and landmarks. Lateral decubitus with the operative hip uppermost. The single most important factor is the pelvis perpendicular to the floor — any tilt causes an equivalent error in cup anteversion (check with fluoroscopy: obturator foramina symmetric, coccyx midline). Pad well (an axillary roll, and padding between the knees), flex the lower knee 90 degrees for comfort, and leave the operative leg free to move through the full flexion-adduction-internal-rotation arc needed for dislocation and trial reduction. Mark the greater trochanter and the posterior border of the femur to guide the incision.
- Consequence
- Cup falsely appears more anteverted than it is (false security)
- Consequence
- Cup falsely appears more retroverted (may over-correct)
- Consequence
- Eases posterior exposure but introduces anteversion error
- Consequence
- Pressure injuries and nerve compression
Always state the pelvic position when describing this approach. A pelvis rolled forward makes the cup falsely appear anteverted; a pelvis rolled back makes it falsely appear retroverted. Examiners expect you to know that pelvic tilt — not the approach itself — is the commonest cause of cup malposition.
Global utilisation. Major registries (UK NJR, AOANJRR, NZJR, Swedish/SHAR) all show the posterior approach is the most frequently used exposure for primary THA, with the direct lateral and anterior approaches making up most of the remainder. Crucially, no clinically meaningful difference in long-term revision rate exists between the three approaches in registry data — the approach influences dislocation and abductor-related complications more than overall survival.
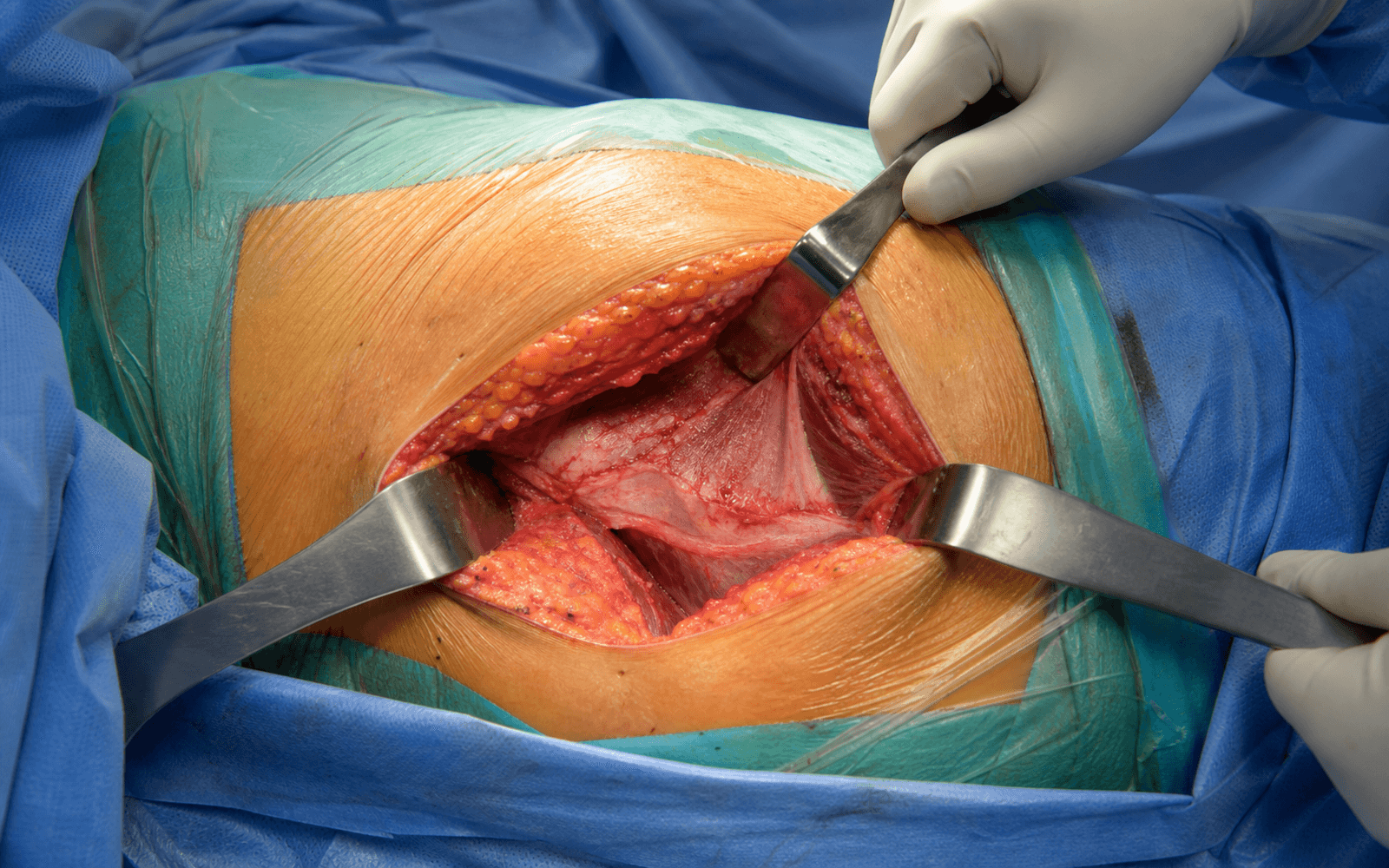
The Exposure
Work straight down through the layers from skin to capsule: split gluteus maximus on its internervous plane, use the piriformis as the guide to the short external rotators, and finish with a transosseous repair of the posterior soft tissues — the step that defines a modern posterior approach.
Dissection sequence
- Lateral decubitus, operative hip up, pelvis perpendicular to the floor.
- A curved incision centred on the posterior border of the greater trochanter: start 6-8cm proximal to the trochanter and curve posteriorly toward the posterosuperior iliac spine, then run straight distally along the posterior femoral shaft for 10-15cm.
- Incise skin and subcutaneous fat down to the fascia lata.
- Open the fascia lata in line with its fibres over the trochanter; this opens onto gluteus maximus posteriorly and the vastus lateralis ridge anteriorly.
- Bluntly split gluteus maximus in the line of its fibres — this is the only true internervous plane to the hip: gluteus maximus (inferior gluteal nerve) on the posterior leaf and gluteus medius (superior gluteal nerve) anteriorly.
- Take careful haemostasis of the branches of the inferior gluteal artery within the muscle.
- With the leg internally rotated, identify the piriformis tendon at the superior border of the short external rotators.
- The sciatic nerve runs immediately below the piriformis, about 1cm medial to the greater trochanter — visualise or palpate it gently and protect it throughout. Internal rotation relaxes the nerve and swings the short externals into view.
- Place stay sutures in each tendon before division, for later repair.
- Moore: divide the piriformis and all short external rotators close to their trochanteric insertion.
- Southern: preserve the piriformis, dividing only the gemelli and obturator internus.
- Either is acceptable provided the capsule and short externals are repaired. The medial femoral circumflex artery runs along quadratus femoris — keep the dissection close to bone and leave quadratus intact where possible.
- Reflect the divided short externals back to expose the posterior capsule.
- Place stay sutures in the capsule, then make a longitudinal or T-shaped capsulotomy, preserving tagged flaps for later repair.
- With the capsule open, flex, adduct and internally rotate the hip to dislocate posteriorly.
- Perform the femoral neck osteotomy at the templated level and remove the head. The acetabulum and femur are now exposed for preparation and implantation.
- After implantation, perform a transosseous tendon-to-bone repair of the capsule and short external rotators to the greater trochanter through bone tunnels, using heavy non-absorbable suture.
- This single step reduces dislocation roughly 8-fold (Kwon: 4.46% without repair to 0.49% with repair) and is now standard of care for the posterior approach.
The sciatic nerve is the primary structure at risk. It exits the pelvis below the piriformis (in 85% of patients), runs about 1cm medial to the greater trochanter, and lies posterior to the short external rotators and posterior capsule. It is most at risk during posterior retractor placement, acetabular reaming, and leg lengthening. Protect it by keeping retractors anterior to the intact short externals, internally rotating the leg, and avoiding excessive lengthening (under 4cm). Transient palsy occurs in roughly 0.5-2% and permanent injury in 0.1-0.5% of cases — so always document the pre-operative nerve examination.
The feature that distinguishes a modern posterior approach is the posterior soft-tissue repair. Transosseous tendon-to-bone repair of the capsule and short external rotators restores a mechanical barrier to posterior translation, allows early mobilisation often without strict precautions, and lowers dislocation to a rate comparable with the anterior approach.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Sciatic nerve (1cm medial to GT, below piriformis)
- Protection
- Internal rotation, retractors anterior to the short externals, avoid over-lengthening
- Structure at risk
- Superior gluteal nerve (emerges 3-5cm above the GT)
- Protection
- Limit proximal dissection to under 5cm above the trochanter
- Structure at risk
- Inferior gluteal artery branches within gluteus maximus
- Protection
- Careful haemostasis during the muscle split
- Structure at risk
- Medial femoral circumflex artery along quadratus femoris
- Protection
- Stay close to bone; preserve quadratus where possible
- Structure at risk
- First perforating artery (profunda femoris)
- Protection
- Careful distal dissection along the femur
Moore versus Southern
- Moore
- Divided
- Southern
- Preserved
- Moore
- All divided
- Southern
- Gemelli and obturator internus only
- Moore
- Slightly better
- Southern
- Slightly less
- Moore
- Less (piriformis divided)
- Southern
- More (piriformis intact)
- Moore
- Common
- Southern
- Less common
Current consensus: capsular repair is more important than piriformis preservation for preventing dislocation. Either variant is acceptable provided the posterior capsule and short external rotators are repaired. Component position and the safe zone
- Target
- 40 degrees
- Safe range
- 30-50 degrees
- Target
- 15-20 degrees
- Safe range
- 5-25 degrees
- Target
- 30-40 degrees
- Safe range
- 25-40 degrees safe
- Mechanism
- Retractor pressure, traction
- Prognosis
- Good (60-80% recovery)
- Mechanism
- Stretch, compression
- Prognosis
- Variable (months to years)
- Mechanism
- Laceration, transection
- Prognosis
- Poor (often permanent)
- Sciatic or motor nerve palsy: roughly 0.5-2% transient, 0.1-0.5% permanent. Risk factors: revision surgery, DDH, lengthening over 4cm, direct trauma. Only about 36% of complete palsies recover fully (Farrell), so prognosis is guarded; manage with an ankle-foot orthosis, physiotherapy, and exploration if progressive or a compressive cause is found.
- Heterotopic ossification: 20-40% radiographic, 5-10% symptomatic. Risk: male gender, DISH, hypertrophic OA, prior HO. Prevent with indomethacin or single-dose radiation (7 Gy); excise if symptomatic after maturation (12 months or more). Extensile options. Extend proximally along the ilium for high-riding DDH or posterior column work (stay under 5cm above the trochanter to protect the superior gluteal nerve); extend distally along the posterior femur for shaft fracture or revision femoral work. The same incision becomes the Kocher-Langenbeck approach for posterior wall and column acetabular fractures. Closure. Re-attach the capsule and short external rotators to the greater trochanter through transosseous tunnels with heavy non-absorbable suture (tendon-to-bone is the most effective technique), close the gluteal split and fascia lata, and close the skin in layers. With a secure repair, many enhanced-recovery pathways use reduced or no hip precautions.
Procedures Through This Approach
- Primary total hip arthroplasty — the principal operation done through this exposure.
- Posterior approach THA (Kocher-Langenbeck modified) — the standard workhouse THA.
- Minimally invasive posterior THA and SuperPATH tissue-sparing posterior — posterior-based, abductor-sparing variants.
- Revision THA (acetabular component) — direct access to the posterior column and wall.
- Hemiarthroplasty for displaced femoral neck fracture.
- Posterior wall and column acetabular fracture fixation (the Kocher-Langenbeck variant).
- Compatible with ceramic bearings, dual-mobility cups and cemented or cementless femoral stems for stability and fixation strategy.
Viva & Exam Focus
The only hip approach with a true internervous plane: gluteus maximus (inferior gluteal nerve) and gluteus medius (superior gluteal nerve). No muscle is denervated when the approach is performed correctly.
The sciatic nerve runs about 1cm medial to the greater trochanter, below the piriformis, and posterior to the acetabulum. It is at highest risk during posterior retractor placement, acetabular exposure, and leg lengthening. Injury causes foot drop.
Posterior soft-tissue repair (capsule plus short external rotators) reduces dislocation roughly 8-fold — Kwon found 4.46% without repair versus 0.49% with repair (relative risk 8.21). Now standard of care, using transosseous tendon-to-bone repair with heavy non-absorbable suture.
Post-operative dislocation occurs with combined flexion, adduction and internal rotation — getting out of a low chair, tying shoes, picking up objects. Patient education for the first 6-12 weeks is critical.
POSTERIORPOSTERIOR — surgical steps
SCIATICSCIATIC — nerve protection
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Walk me through the posterior approach to the hip for THA. What is the internervous plane and what structures are at risk?”
“A 72-year-old woman undergoes primary THA via a posterior approach. In recovery she has complete foot drop and numbness over the lateral leg and dorsum of the foot. How do you assess and manage this?”
“A 65-year-old man has had three posterior dislocations in 6 months following primary THA via a posterior approach, each closed reduced successfully. How do you manage this?”
Key anatomy
- True internervous plane: gluteus maximus (inferior gluteal) versus gluteus medius (superior gluteal)
- Sciatic nerve: about 1cm medial to the GT, below the piriformis (85%)
- Short external rotators (superior to inferior): piriformis, superior gemellus, obturator internus, inferior gemellus, quadratus femoris
- Posterior capsule: primary restraint to posterior dislocation
Surgical steps
- Lateral decubitus, pelvis perpendicular to the floor
- Curved incision from PSIS to GT, then straight distally along the femur
- Split gluteus maximus bluntly in line with its fibres
- Identify the piriformis (landmark for the sciatic nerve)
- Tag and divide the short externals (Moore) or preserve the piriformis (Southern)
- Tag the capsule and perform the capsulotomy
- Femoral neck osteotomy, then proceed with the THA
- Critical: repair the capsule and short externals with heavy non-absorbable suture
Structures at risk
- Sciatic nerve (about 1cm medial to GT): internal rotation, careful retractors, avoid over-lengthening
- Superior gluteal nerve if extended proximally: limit dissection to under 5cm above the GT
- Inferior gluteal artery: haemostasis during the gluteal split
- Medial femoral circumflex artery: at risk near quadratus femoris
- First perforating artery: near the distal exposure
Advantages versus disadvantages
- Pro: the only true internervous plane to the hip
- Pro: extensile proximally for DDH, distally for femoral fracture
- Pro: excellent posterior column and wall exposure for revision and trauma
- Con: higher dislocation if the capsule is not repaired (addressed by modern repair)
- Con: sciatic nerve at risk (0.5-2% palsy)
- Con: requires lateral positioning (cannot be done supine)
Complications
- Dislocation: roughly 0.5% with repair versus 4-5% without (Kwon); position is flexion, adduction, internal rotation
- Sciatic or motor nerve palsy: roughly 0.5-2%; complete palsies often recover incompletely (about 36% full recovery, Farrell)
- Heterotopic ossification: 20-40% radiographic; prevent with indomethacin or single-dose radiation
- Posterior soft-tissue repair reduces dislocation roughly 8-fold (Kwon, relative risk 8.21) — standard of care
Key pearls
- Posterior soft-tissue repair is mandatory (transosseous tendon-to-bone, heavy non-absorbable suture)
- Risk position: flexion, adduction, internal rotation
- Piriformis is the landmark (sciatic nerve runs just below it)
- Commonest THA approach worldwide; equivalent revision rates across approaches
- Fully compatible with enhanced-recovery pathways when the soft tissues are repaired
References
Registry and society guidance. The posterior approach is the most commonly used approach for primary THA across major registries (UK NJR, AOANJRR, NZJR, SHAR), with no clinically significant difference in long-term revision between posterior, direct lateral and anterior approaches. AAOS (US) and NICE / BOA (UK) both emphasise accurate component position, adequate head size and posterior soft-tissue repair to minimise instability; AO Foundation and arthroplasty consensus recommend transosseous tendon-to-bone repair when a posterior approach is used.
Does surgical approach affect total hip arthroplasty dislocation rates? (Posterior soft-tissue repair meta-analysis)
- Meta-analysis of 5 studies directly comparing the posterior approach with and without posterior soft-tissue repair
- Dislocation rate with repair 0.49% versus without repair 4.46%
- Posterior approach without repair carried 8.21 times the relative risk of dislocation (95% CI 4.05 to 16.67)
- With soft-tissue repair, dislocation rates for anterolateral, direct lateral and posterior approaches were comparable (0.70%, 0.43%, 1.01%)
Dislocations after total hip-replacement arthroplasties (the Lewinnek safe zone)
- Series of 300 total hip replacements with precise measurement of acetabular cup orientation
- Dislocation rate 1.5% when the cup lay within anteversion 15 plus or minus 10 degrees and lateral opening (inclination) 40 plus or minus 10 degrees
- Dislocation rate 6.1% when the cup lay outside this safe range
- Greatest dislocation risk in the first 30 days and in hips with prior surgery; anterior dislocation associated with increased cup anteversion
Soft tissue repair as a hip dislocation preventive strategy after posterior/posterolateral THA (scoping review)
- Systematic scoping review of 13 studies of posterior/posterolateral THA for osteoarthritis
- Preserving or repairing the external rotators consistently reduced dislocation rates
- Tendon-to-bone repair was the most effective soft-tissue technique identified
- Authors recommend tailoring preventive strategy to individual dislocation risk factors
Motor nerve palsy following primary total hip arthroplasty
- Retrospective review of 27,004 primary THAs (1970-2000); 47 motor nerve palsies (0.17%)
- Independent risk factors: posterior approach, limb lengthening, cementless femoral fixation, and a diagnosis of developmental dysplasia or post-traumatic arthritis
- Peroneal division most commonly affected (30 of 47 palsies)
- Only 36% of complete palsies recovered fully (mean 21 months); most deficits, complete or incomplete, did not fully resolve
Named-society guidance on elective primary THA (NICE/BOA, AAOS)
- Approach selection (posterior, lateral, anterior) should be based on surgeon training and patient anatomy; registries show no clear difference in revision between approaches
- Routine pharmacological VTE prophylaxis after elective THA, commonly continued for up to roughly 35 days, with mechanical prophylaxis and early mobilization
- Dislocation is minimized by accurate component position, adequate femoral head size and posterior soft-tissue repair when a posterior approach is used
- Patient-specific risk assessment guides head size, dual-mobility and precaution decisions