Reroutes the EHL from the distal phalanx to the first metatarsal neck, with concomitant IP fusion, to correct a claw hallux and augment weak ankle dorsiflexion · Charcot-Marie-Tooth cavovarus foot
- The Jones transfer reroutes the EHL from its insertion on the distal phalanx to the first metatarsal neck. With the interphalangeal joint fused at the same sitting, it both abolishes the deforming claw force and augments weak ankle dorsiflexion.
- Classic indication: a claw hallux WITH weak tibialis anterior, classically the Charcot-Marie-Tooth cavovarus foot, where a single functioning EHL can be sacrificed to support dorsiflexion.
- The IP joint is ALWAYS fused at the same sitting. Without it, the transferred EHL would simply recreate IP hyperextension (the claw).
- Prerequisites: a FUNCTIONING EHL (the donor must work) and a SUPPLE MTP joint. A fixed MTP deformity needs an osteotomy, not a transfer; a non-functioning EHL means no donor.
- Two dorsal incisions that are NEVER connected (skin-bridge necrosis). Tension is set at ankle neutral and rechecked with the knee both extended and flexed to remove the gastrocnemius effect.
When & Why
Indication. A symptomatic claw hallux (flexible IP hyperextension with MTP flexion) occurring together with weak ankle dorsiflexion — most commonly the Charcot-Marie-Tooth (CMT) cavovarus foot, but also anterior compartment syndrome sequelae or any partial tibialis anterior weakness — where a single functioning EHL can be sacrificed. Flexible hallux IP hyperextension greater than about 20 degrees causing painful callosities is the typical trigger. Why this transfer works. By moving the EHL insertion from the distal phalanx to the first metatarsal neck, the tendon's pull now dorsiflexes the ankle (and the first ray) instead of hyperextending the IP joint. Fusing the IP joint removes the deforming force entirely. One tendon therefore corrects two problems: the claw, and the weak dorsiflexion. Contraindications. A fixed MTP deformity (address with an osteotomy first), a non-functioning EHL (no donor tendon — consider a Bridle procedure or AFO), or normal tibialis anterior power with an isolated claw (use EHL lengthening or an EHL-to-MTP capsule transfer instead — see below). The Jones transfer is also only a partial dorsiflexion substitute and is inadequate for a complete anterior compartment palsy. The decision: which claw-hallux operation? Match the procedure to the deformity and to the tibialis anterior power.
- Indication
- Mild flexible claw, normal tibialis anterior
- Notes
- Preserves IP motion; no dorsiflexion augmentation
- Indication
- Isolated claw, normal tibialis anterior
- Notes
- Maintains some extension function
- Indication
- Claw hallux WITH tibialis anterior weakness
- Notes
- Gold standard for the CMT foot; augments dorsiflexion
- Indication
- Rigid claw, strong tibialis anterior
- Notes
- No dorsiflexion augmentation
- Indication
- Partial tibialis anterior weakness
- Notes
- Augments dorsiflexion; also corrects claw hallux
- Indication
- Complete tibialis anterior palsy
- Notes
- Tibialis posterior plus peroneus longus routed to the TA insertion; stronger dorsiflexion
- Indication
- Complete anterior compartment loss
- Notes
- Tendon transfer for full palsy
- Indication
- Non-surgical candidate or temporising
- Notes
- External support
In the CMT foot the Jones transfer is one component of a multi-level reconstruction, staged as needed: a Dwyer calcaneal osteotomy for hindfoot varus, a peroneus longus-to-brevis transfer for first-ray plantarflexion, the Jones transfer for the claw hallux and dorsiflexion, and lesser-toe flexor-to-extensor (Girdlestone-Taylor) transfers for claw toes. Counselling must stress that CMT is progressive — the operation balances the foot, it does not cure the neuropathy. Setup. Supine with a sandbag under the ipsilateral hip, foot at the end of the table for access; thigh tourniquet. Mark both incisions with the foot held in the corrected position before exsanguination, as the landmarks become harder to palpate once the limb is bloodless.
The Operation
The goal: through two dorsal incisions that are never connected, harvest the EHL off the distal phalanx, fuse the IP joint, create a bone tunnel through the first metatarsal neck, pass the EHL through it, and set the tension at ankle neutral so the hallux rests corrected and dorsiflexion is augmented. The exposure and the tensioning are the two steps that decide whether the operation works.
Operative sequence
- Supine with a sandbag under the ipsilateral hip, foot at the end of the table.
- Mark BOTH incisions and the skin bridge with the foot held corrected before exsanguination: incision 1 is a 2-3 cm longitudinal dorsal incision over the hallux IP joint; incision 2 is a 3-4 cm longitudinal dorsal incision over the first metatarsal neck.
- Thigh tourniquet, exsanguinate, inflate to 250-300 mmHg.
- Before committing, confirm a functioning, palpable EHL and a supple MTP joint on the table — both are prerequisites for the transfer to work.
- Never connect the two incisions: a single continuous wound devascularises the skin bridge.
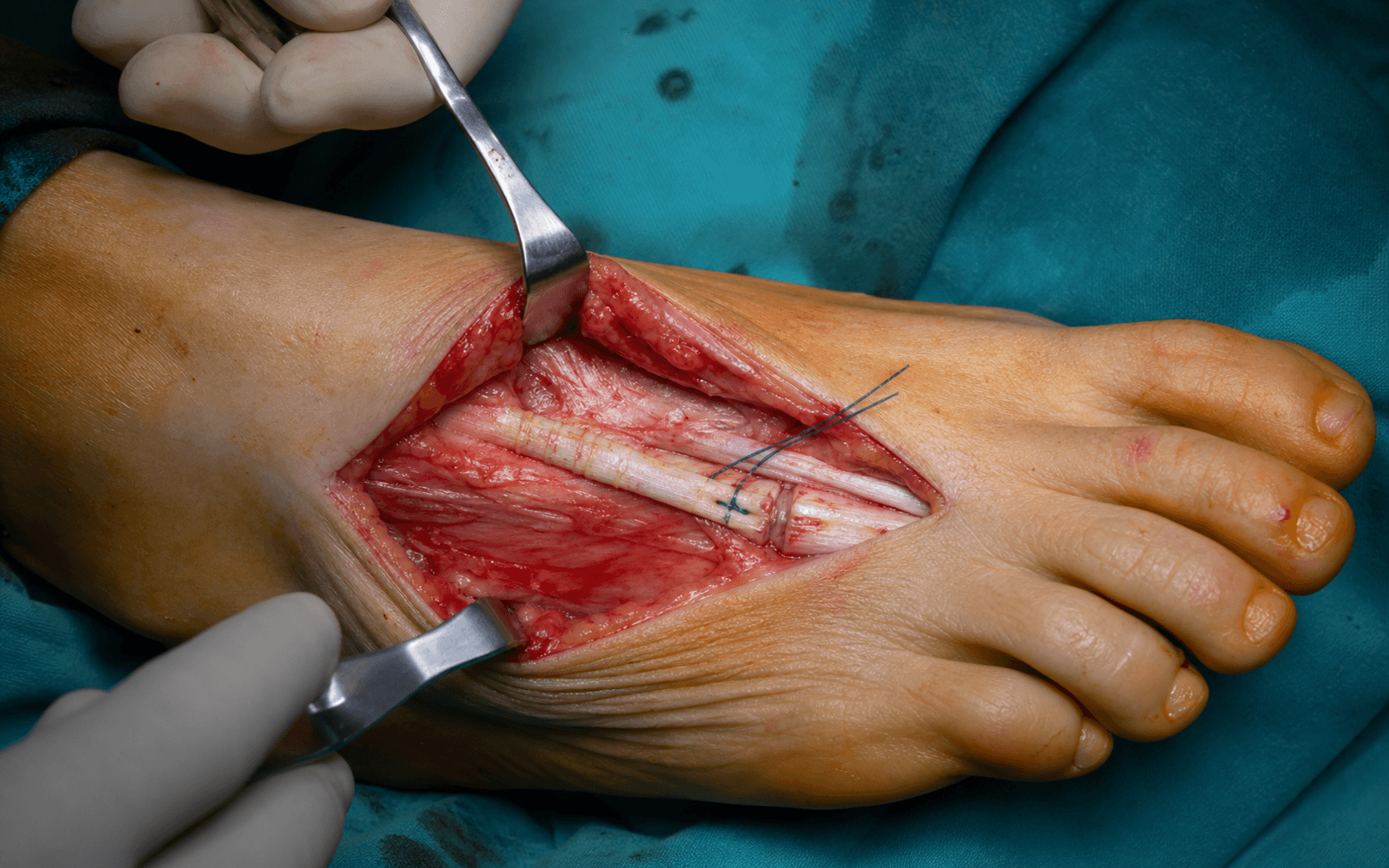
- Deepen the distal incision through subcutaneous tissue; the EHL lies immediately deep as a white, glistening tendon.
- Identify and protect the dorsal digital nerves, which run 2-3 mm medial and lateral to the tendon, before opening the sheath.
- Open the sheath longitudinally and trace the EHL distally to its insertion on the base of the distal phalanx.
- Detach the tendon sharply off the distal phalanx, harvesting it as long as possible — a short remnant compromises the later bone-tunnel weave.
- Place the whipstitch (2-0 non-absorbable, Krackow or locking) into the cut end BEFORE releasing the last fibres, so the tendon cannot retract proximally into the leg.
- With the EHL detached and retracted, expose the IP joint capsule and open it longitudinally.
- Remove all articular cartilage from the proximal phalanx head and distal phalanx base with a small rongeur or curette, creating congruent surfaces (head slightly concave, base flat-to-convex).
- Fish-scale or fenestrate the subchondral bone to promote bleeding and fusion; irrigate away all debris.
- The IP fusion is the non-negotiable companion to the transfer — without it, the EHL pull simply recreates IP hyperextension (the claw).
- Limit bone-resection depth to about 1 cm to avoid injuring the flexor hallucis longus plantarly and to avoid shortening the hallux.
- Position the hallux in 10-15 degrees of plantarflexion, with neutral varus-valgus and neutral rotation, so the pulp loads flat in the shoe.
- Insert a 1.6 mm K-wire from the tip of the distal phalanx, retrograde across the fusion site into the proximal phalanx, as guide and temporary fixation.
- Definitive fixation: ream over the K-wire with a 3.0-3.5 mm reamer and insert a 3.5 mm cannulated compression screw, burying the head. Crossed K-wires are an acceptable fallback but carry higher nonunion and pin-track rates.
- A single axial compression screw across congruent cancellous surfaces is the most reliable construct — a fibrous gap from convex-on-convex contact is the commonest reason this fusion fails.
- Measure screw length carefully to avoid plantar cortex penetration.
- Make a 3-4 cm longitudinal dorsal incision over the first metatarsal neck, centred about 3-4 cm proximal to the MTP joint.
- Stay strictly on the dorsal surface: the deep peroneal nerve and dorsalis pedis artery run about 2-3 cm medial to the tunnel site, so avoid any medial dissection.
- Raise a short subperiosteal flap over the dorsal MT neck and, with a 3.5-4.0 mm drill bit, create a dorsal-to-plantar tunnel at the neck, angled slightly from distal-dorsal to proximal-plantar.
- Place the tunnel through the metatarsal NECK, not the diaphysis — neck cancellous bone heals the tendon better and the more distal pull line gives a stronger dorsiflexion lever. Ream the edges smooth and confirm position with fluoroscopy.
- Avoid plantar cortex blowout, which weakens the tunnel and irritates the plantar soft tissues.
- Return to the distal incision and divide the EHL proximally at the MTP joint level, ensuring adequate length for the transfer (it can be harvested to the mid-dorsum of the foot if needed).
- Create a subcutaneous tunnel between the two incisions with a large haemostat or tendon passer — never convert this into a single continuous wound, which is what threatens the skin bridge.
- Pass the EHL proximally from distal to proximal through the subcutaneous tunnel, then through the metatarsal bone tunnel from dorsal to plantar using a curved clamp, until the whipstitch emerges at the plantar exit.
- Mark the tendon with a longitudinal ink line before passage so you can confirm it has not spiralled before fixation.
- Set the tension with the ANKLE IN NEUTRAL dorsiflexion and the first ray supported in slight dorsiflexion relative to the lesser metatarsals.
- Pull the tendon tight through the tunnel until the hallux MTP rests neutral to barely extended; secure it to itself or to plantar periosteum with multiple 2-0 non-absorbable sutures (FiberWire or Ethibond) in a wrap-around weave, or use a suture anchor in the plantar cortex.
- Recheck tension with the KNEE BOTH EXTENDED AND FLEXED to remove the gastrocnemius tethering effect — tensioning with the knee flexed alone leaves the transfer too tight in stance.
- Intra-operative check: passively dorsiflex the ankle and the MTP should extend slightly; plantarflex and it should flex slightly.
- Over-tensioning (the commonest error) causes MTP cock-up, transfer metatarsalgia and a painful gait; under-tensioning gives no functional benefit and the transfer elongates over time.
- Release the tourniquet and secure haemostasis with bipolar BEFORE closure — a dorsal haematoma over a thin skin bridge is a direct route to wound breakdown.
- Close the periosteum over the MT tunnel where possible (2-0 absorbable), then the subcutaneous layer (3-0 absorbable) and skin (4-0 nylon interrupted or 4-0 subcuticular) for both incisions.
- Apply a well-padded below-knee cast with the ANKLE IN NEUTRAL (never equinus), the hallux MTP in slight plantarflexion (10-15 degrees) and the IP fusion protected; the cast extends to the toes.
- Keep the toes visible for neurovascular monitoring; instruct the patient to elevate for 48-72 hours and to report increasing pain (compartment syndrome) or toe colour change (vascular compromise).
- Non-weight-bearing in the cast for 2 weeks; wound check and re-cast at 2 weeks if well healed.
- Progressive weight-bearing in the cast from weeks 2-6; radiographs at 6 weeks assess the IP fusion.
- If fusion is progressing, transition to a CAM boot and begin gentle ankle and MTP range of motion (the IP stays fused); progressive weight-bearing in the boot from weeks 6-10.
- Confirm IP fusion radiographically at 10-12 weeks; move into a supportive, stiff-soled shoe with physiotherapy for dorsiflexion strengthening, gait training and proprioception.
- Protect the construct, not just the fusion — the transfer needs roughly 6 weeks of immobilisation to incorporate into the bone tunnel before active dorsiflexion loading; premature active EHL firing against an un-incorporated tunnel is a classic cause of silent transfer elongation and recurrent drop foot.
- Obtain AP and lateral fluoroscopic images: confirm IP screw position (central, not prominent plantarly), an intact bone tunnel and acceptable foot alignment.
- Document the hallux position (IP fused in 10-15 degrees of plantarflexion, MTP neutral) and record the tendon transfer path and the tension setting — documenting the tension setting is a key medicolegal point.
- Note tendon and bone quality and the neurovascular status; take intra-operative photographs of the fusion hardware and tendon passage for the record.
- Dorsal digital nerves — 2-3 mm medial and lateral to the EHL at the distal incision. Identify them early in the subcutaneous plane and retract gently; injury (5-10 percent incidence) causes a painful neuroma. If transected, repair primarily with 8-0 or 9-0 nylon under magnification.
- Deep peroneal nerve and dorsalis pedis artery — about 2-3 cm medial to the proximal tunnel. Stay strictly on the dorsal surface of the first metatarsal; do not dissect medially from the MT neck.
- Flexor hallucis longus — plantar to the IP joint. Limit cartilage and bone resection depth to about 1 cm during fusion preparation; do not penetrate the plantar cortex aggressively.
- The skin bridge between the incisions — never connect the two incisions; pass the tendon through a subcutaneous tunnel only.
- The plantar cortex at the metatarsal tunnel — avoid blowout, which weakens fixation and causes plantar prominence and tendon irritation.
Set the tension with the ankle at neutral and the first ray supported, aiming for the hallux MTP to sit neutral to barely extended at rest. Always recheck with the knee both extended and flexed to remove the gastrocnemius tethering effect. With the ankle at neutral, the hallux MTP should be neutral; dorsiflex the ankle and the MTP should extend slightly.
The skin bridge between the dorsal IP and MT-neck incisions is the most vulnerable soft tissue in the case. Connecting the incisions devascularises it and leads to necrosis and wound breakdown. Pass the tendon through a clean subcutaneous tunnel on a curved clamp, and confirm a functioning EHL and a supple MTP joint on the table before committing — both are prerequisites for the transfer.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0-2 weeks | Below-knee cast, ankle neutral, hallux in 10-15 degrees plantarflexion, non-weight-bearing | Toe mobilisation only; elevation 48-72 hours | | 2 | 2-6 weeks | Cast, progressive weight-bearing | Wound check at 2 weeks; nothing active | | 3 | 6-10 weeks | CAM boot if IP fusion progressing on 6-week radiograph | Gentle ankle and MTP range of motion; IP stays fused | | 4 | 10-16 weeks+ | Stiff-soled shoe; night splint if needed | Dorsiflexion strengthening, gait training, proprioception | Most patients return to regular shoes at 3-4 months and to full unrestricted activity at 4-6 months once IP fusion is confirmed. Expect a permanent IP fusion (no IP motion), improved ankle dorsiflexion and a corrected claw deformity. CMT patients need yearly follow-up to monitor disease progression. If IP fusion is not evident at 12 weeks, consider a bone stimulator, prolonged immobilisation, or revision fusion with bone graft. Complications
- Recognition
- Persistent IP motion, pain at the fusion site, lucency on radiograph at 3+ months
- Prevention
- Adequate cartilage debridement, fenestrate subchondral bone, rigid compression fixation, non-weight-bearing 6 weeks
- Management
- Bone stimulator, revision fusion with bone graft and compression screw, prolonged immobilisation
- Recognition
- Hallux MTP hyperextension on weight-bearing, transfer metatarsalgia, painful gait
- Prevention
- Correct tensioning at ankle neutral; test with knee extended and flexed
- Management
- Severe: revision with tendon lengthening or release at the MT tunnel; mild: orthotic offload
- Recognition
- Progressive loss of ankle dorsiflexion, return of drop foot, no resistance on testing
- Prevention
- Secure fixation at the MT tunnel (wrap-around, multiple sutures); adequate 6-week immobilisation
- Management
- Revision transfer with tendon shortening, or alternative transfer (Bridle) if tissue insufficient
- Recognition
- Numbness medial or lateral to the hallux, painful neuroma at the incision, hyperaesthesia
- Prevention
- Identify nerves early in the subcutaneous plane, gentle retraction, mark preoperatively
- Management
- Desensitisation therapy, pregabalin; neuroma excision and transposition if symptomatic
- Recognition
- Dehiscence, skin-bridge necrosis, delayed healing, infection
- Prevention
- Do NOT connect incisions; gentle soft-tissue handling; meticulous haemostasis
- Management
- Local wound care; skin grafting if needed; secondary intention for small defects
- Recognition
- Recurrent cavovarus, progressive hindfoot varus, new toe deformities
- Prevention
- Address all components of the deformity initially; counsel on the progressive nature of CMT
- Management
- Additional procedures (Dwyer osteotomy, peroneus longus transfer); triple arthrodesis if severe
Viva & Exam Focus
JONESJONES — indications for the transfer
TUNNELTUNNEL — transfer technique
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 25-year-old with Charcot-Marie-Tooth disease presents with bilateral claw hallux deformity and foot drop. How would you assess and manage this patient?”
“Describe the key technical aspects of the Jones tendon transfer and how you ensure correct tensioning.”
“What alternative procedures exist for claw hallux and drop foot, and when would you choose them over the Jones transfer?”
Indications
- Claw hallux WITH weak tibialis anterior (the classic CMT indication)
- Drop foot from anterior compartment weakness (partial TA function)
- Cavovarus reconstruction (usually multi-level)
- Anterior compartment syndrome sequelae with residual weakness
- Contraindicated with: fixed MTP deformity, non-functioning EHL, normal TA power
Critical steps
- Two dorsal incisions - NEVER connected (skin bridge)
- Harvest the EHL with a whipstitch, detach from the distal phalanx
- IP fusion - remove cartilage, fenestrate, screw in 10-15 degrees plantarflexion
- Proximal incision over MT neck - 3.5-4.0 mm tunnel, dorsal to plantar
- Pass tendon subcutaneously then through the tunnel; tension at ankle neutral
Five danger zones
- Dorsal digital nerves: 2-3 mm from the EHL at the distal incision
- Deep peroneal nerve and dorsalis pedis: 2-3 cm medial to the MT tunnel
- Flexor hallucis longus: plantar to the IP joint - limit resection depth
- Skin bridge between incisions: NEVER connect the incisions
- Plantar cortex at the MT tunnel: avoid blowout and prominence
Tensioning
- Ankle at neutral (90 degrees) for tensioning
- Hallux MTP neutral to slightly extended
- Test: dorsiflex the ankle - the MTP should extend slightly
- Test with the knee BOTH extended and flexed (gastrocnemius effect)
- Over-tension = cock-up deformity; under-tension = no benefit
Combined CMT procedures
- Dwyer calcaneal osteotomy for hindfoot varus greater than 10 degrees
- Peroneus longus to brevis transfer for first ray plantarflexion
- Girdlestone-Taylor transfers for lesser toe clawing
- Plantar fascia release for flexible cavus
- Triple arthrodesis for rigid severe deformity
Key complications
- IP nonunion: linked to inadequate fixation and early weight-bearing
- MTP cock-up: over-tensioning, may need revision
- Dorsal digital nerve injury (5-10 percent): painful neuroma
- Transfer failure: under-tensioning or inadequate fixation
- Disease progression: CMT is progressive, may need revision
Rehabilitation
- 0-2 weeks: non-weight-bearing, below-knee cast
- 2-6 weeks: progressive weight-bearing in cast
- 6 weeks: radiograph to confirm IP fusion, transition to CAM boot
- 6-10 weeks: ankle and MTP range of motion
- 3-4 months: regular shoes; 4-6 months: full activity
Exam tips
- Know the CMT pathophysiology: 'dying-back' pattern, peroneal weakness
- Coleman block test to assess hindfoot flexibility
- Two incisions - NEVER connect (skin-bridge necrosis)
- IP fusion is always performed - corrects the claw AND anchors the tendon
- Alternatives: Bridle for complete drop foot, EHL lengthening for mild claw
Background & Evidence
Pathoanatomy of the CMT cavovarus foot. Charcot-Marie-Tooth disease is a hereditary motor sensory neuropathy (HMSN type I most common) with progressive distal weakness in a "dying-back" pattern. The selective muscle imbalance produces the classic cavovarus triad: hindfoot varus (tibialis posterior relatively preserved and unopposed), first-ray plantarflexion (peroneus longus preserved while peroneus brevis weakens, so the longus is unopposed), and claw hallux and lesser toes (intrinsic weakness). Peroneal weakness (tibialis anterior and EHL) produces the drop foot and the hallux clawing that the Jones transfer addresses. Tibialis posterior is relatively spared, which is why it can be harvested for a Bridle procedure in complete palsy. The EHL: anatomy and why it is expendable. The extensor hallucis longus arises from the middle two-fourths of the anterior fibula and adjacent interosseous membrane, is innervated by the deep peroneal nerve (L5), and inserts on the dorsal base of the distal phalanx of the hallux. Its primary action is IP extension, with secondary MTP extension and weak ankle dorsiflexion. The tendon is round in the leg, flattens distally, and runs between extensor digitorum brevis medially and extensor digitorum longus laterally on the dorsum of the foot. Once the IP joint is fused, the EHL's IP extension function is sacrificed without functional loss, the MTP and ankle extension is preserved by EDL and EDB, and moving the insertion to the metatarsal neck actually augments ankle dorsiflexion — which is precisely what makes it a suitable donor. Assessment — the Coleman block test. Flexibility is decisive. The Coleman block test assesses whether the hindfoot varus is driven by the plantarflexed first ray (flexible — the hindfoot corrects when the first ray is blocked) or is fixed. A Jones transfer is a soft-tissue-balancing operation suited to a flexible, correctable deformity; a rigid foot needs osteotomies or arthrodesis. Published outcomes. The Jones procedure is almost always reported as one component of a combined flexible-cavovarus reconstruction rather than in isolation, so outcome data reflect the package (plantar release, first metatarsal dorsiflexion osteotomy, peroneus longus-to-brevis transfer, and EHL-to-metatarsal transfer with IP fusion). The figures below are taken directly from the cited PubMed-verified studies. - Faldini, Giannini et al. (2015) — 24 feet in 12 CMT patients, mean follow-up 6 years: combined plantar fasciotomy, midtarsal osteotomy, Jones EHL transfer and first metatarsal dorsiflexion osteotomy in flexible feet. Maryland Foot Score improved from 72 to 86 (excellent in 50 percent, good in 42 percent, fair in 8 percent); Meary angle corrected from 25 degrees to 2 degrees and was maintained. The authors attribute the only modest score gain to residual motor imbalance, not loss of correction.
- Ward, Dolan et al. (2008) — 25 patients, 41 feet, mean follow-up 26.1 years: the longest follow-up of an EHL-to-first-metatarsal-based reconstruction. Cavus correction was well maintained; some radiographic recurrence of hindfoot varus was common but no patient required triple arthrodesis. Seven patients (8 feet) needed at least one further foot or ankle operation, with lower reoperation and degenerative-change rates than historical triple-arthrodesis series; smoking strongly predicted worse pain and disability scores.
- Sammarco and Taylor (2001) — 21 feet in 15 patients with neuromuscular cavovarus: a joint-sparing osteotomy strategy (calcaneal plus metatarsal) with which the Jones transfer is frequently combined. AOFAS ankle-hindfoot improved from 46 to 91 and midfoot from 41 to 89; all patients became brace-free; nonunion in 3 of 66 metatarsal osteotomies. The consistent message. In a flexible, arthritis-free CMT foot, the Jones transfer combined with joint-sparing osteotomies gives durable deformity correction and supports a joint-preserving, soft-tissue-balancing strategy over early arthrodesis — but it balances the foot, it does not cure the progressive neuropathy.
References
Surgical treatment of cavus foot in Charcot-Marie-Tooth disease: a review of twenty-four cases (AAOS exhibit selection)
- 24 flexible cavus feet (12 CMT patients) treated with plantar fasciotomy, midtarsal osteotomy, Jones EHL-to-first-metatarsal transfer and first metatarsal dorsiflexion osteotomy; mean follow-up 6 years
- Maryland Foot Score improved from 72 to 86; excellent in 50 percent, good in 42 percent, fair in 8 percent
- Meary angle corrected from 25 degrees to 2 degrees and was well maintained; only patients with a flexible deformity and a reducible Coleman-Andreasi test were included
Long-term results of reconstruction for treatment of a flexible cavovarus foot in Charcot-Marie-Tooth disease
- 25 patients (41 feet) treated with first metatarsal dorsiflexion osteotomy, peroneus longus-to-brevis transfer, plantar fascia release and EHL-to-first-metatarsal transfer; mean follow-up 26.1 years
- Cavus correction was well maintained with no patient requiring triple arthrodesis; some radiographic hindfoot varus recurrence was common
- Lower degenerative-change and reoperation rates than historical triple-arthrodesis series; smoking strongly predicted worse pain and disability scores
Cavovarus foot treated with combined calcaneus and metatarsal osteotomies
- 21 feet (15 patients), predominantly neuromuscular cavovarus, treated with lateralising and elevating calcaneal osteotomy plus dorsolateral closing-wedge metatarsal osteotomies
- AOFAS ankle-hindfoot improved from 46 to 91 and midfoot from 41 to 89; all patients became brace-free and motion was preserved
- Nonunion occurred in 3 and delayed union in 2 of 66 metatarsal osteotomies
Charcot-Marie-Tooth disease and the cavovarus foot
- Reviews the muscle-imbalance mechanics that drive the CMT cavovarus foot, including weak tibialis anterior and peroneus brevis with relatively preserved tibialis posterior and peroneus longus
- Emphasises early, flexible-stage soft-tissue balancing (including EHL transfer) before fixed bony deformity develops
- Frames surgical planning around the underlying progressive neuropathy rather than the static deformity alone
Neuromuscular issues in cavovarus foot
- Outlines the principles of soft-tissue release, bony correction and tendon rebalancing required to prevent recurrence in the neuromuscular cavovarus foot
- Highlights first-ray overload, claw toes and drop-foot gait as the presenting features the Jones transfer and adjuncts are designed to address
- Stresses muscle balancing to optimise residual strength and prevent deformity recurrence
Further reading 1. Jones R. The soldier's foot and the treatment of common deformities of the foot. BMJ 1916;1:749-753. 2. Hansen ST. Functional reconstruction of the foot and ankle. Lippincott Williams and Wilkins; 2000. 3. Holmes JR, Hansen ST. Foot and ankle manifestations of Charcot-Marie-Tooth disease. Foot Ankle 1993;14:476-486. 4. Schwend RM, Drennan JC. Cavus foot deformity in children. J Am Acad Orthop Surg 2003;11:201-211. 5. Chan G, Sampath J, Miller F, et al. The role of the dynamic pedobarograph in assessing treatment of cavovarus feet in children with Charcot-Marie-Tooth disease. J Pediatr Orthop 2007;27:510-516.