Chronic lateral ankle instability following failed conservative management · modified Broström (anatomic repair) with Gould modification (inferior extensor retinaculum reinforcement)
- The modified Broström repairs the attenuated ATFL and CFL directly (imbrication / pants-over-vest) and the Gould modification reinforces it with the inferior extensor retinaculum (IER) — it is the anatomic, first-line operation, preserving normal kinematics.
- Operate only on mechanical instability — a positive anterior drawer and/or talar tilt on stress testing/imaging — after a minimum 3 months (often 6) of structured rehabilitation has failed. Functional instability (giving way without measurable laxity) is treated with physiotherapy, not surgery.
- Hindfoot varus greater than 5 degrees must be corrected before or at the same sitting (lateral closing-wedge calcaneal osteotomy). Reconstruction without correcting varus carries a 50–70% recurrence rate.
- Protect the superficial peroneal nerve and its dorsal intermediate/medial branches throughout the anterolateral exposure — nerve injury (5–10%) is the commonest surgical complication.
- Tension the repair with the ankle in neutral dorsiflexion and slight eversion; the Gould modification uses the inferior (not superior) extensor retinaculum. Address concomitant pathology (osteochondral lesions, peroneal tendons) in the same sitting.
When & Why
Indication. Symptomatic chronic lateral ankle instability (CLAI) — recurrent giving way, pain and functional limitation after at least one significant inversion sprain — that has failed a structured conservative programme of proprioceptive training, peroneal strengthening and activity modification (with bracing or taping) for a minimum of 3 months (extended to 6 months in low-demand patients). The decision to operate rests on three pillars, all of which must be present:
- Documented mechanical instability — a positive anterior drawer and/or talar tilt, confirmed clinically and/or on stress radiographs.
- Functional limitation that persists despite 3–6 months of compliant conservative therapy.
- No uncorrected hindfoot malalignment — varus greater than 5 degrees is corrected first or concurrently.
- A motivated patient committed to postoperative rehabilitation and activity modification.
Distinguish mechanical from functional instability first. This is the single most important pre-operative decision — surgery helps mechanical instability and does not help (and may harm) functional instability.
- Mechanical instability
- Objective ligamentous laxity with demonstrable pathologic motion
- Functional instability
- Subjective giving way without measurable laxity
- Mechanical instability
- Positive anterior drawer (greater than 10mm), talar tilt (greater than 10 degrees side-to-side difference)
- Functional instability
- Negative stress tests, normal joint excursion
- Mechanical instability
- Stress radiographs show increased talar tilt or anterior translation
- Functional instability
- Normal stress radiographs, no structural pathology
- Mechanical instability
- ATFL/CFL elongation or rupture, capsular laxity
- Functional instability
- Proprioceptive deficit, peroneal weakness, neuromuscular dysfunction
- Mechanical instability
- Surgical reconstruction indicated if conservative fails
- Functional instability
- Physiotherapy, proprioception, peroneal strengthening
- Mechanical instability
- 85–95% success with anatomic repair
- Functional instability
- Surgery not indicated; poor outcomes if performed
Look for and plan to address concomitant pathology — present in 40–70% of chronic cases and a cause of persistent symptoms if missed: - Osteochondral lesion of the talus (around 35%) — requires concurrent arthroscopic debridement/fixation.
- Peroneal tendon pathology (around 25%) — tears or subluxation.
- Sinus tarsi syndrome (around 20%) and anterior ankle impingement from osteophytes.
- Subtalar instability, which may need separate stabilisation.
- Hindfoot varus — the critical alignment issue (see below).
Hindfoot varus greater than 5 degrees must be corrected before or concurrently with lateral ligament reconstruction. An uncorrected varus position places repetitive overload on the lateral structures and carries a 50–70% recurrence rate. Correct it with a lateral closing-wedge calcaneal osteotomy (or a first metatarsal dorsiflexion osteotomy) depending on the apex of the deformity.
Contraindications. Absolute: active infection, severe peripheral vascular disease, Charcot arthropathy. Relative: uncorrected hindfoot varus (correct first), generalised ligamentous laxity (Beighton greater than 6 — favour non-anatomic reconstruction), a poor soft-tissue envelope, and unrealistic patient expectations. Consent specifically for superficial peroneal nerve injury/numbness or a painful neuroma (5–10%), wound problems or infection (3–5%), ankle or subtalar stiffness (10–15% after anatomic repair), recurrent instability (5–15%), and incomplete relief if concomitant pathology is not addressed. Setup. Supine with a bump under the ipsilateral hip, thigh tourniquet, foot over the end of the table for access. Loupe magnification helps nerve and ligament identification.
The Operation
The goal is to restore the normal lateral ligament complex anatomically — re-tension the attenuated ATFL and CFL, reinforce the repair with the inferior extensor retinaculum (Gould), and protect the superficial peroneal nerve throughout. The anterolateral exposure is laid out as the first steps below (and in depth on the anterolateral approach to the ankle page). Non-anatomic tenodesis is reserved for salvage and is described as the final operative steps.
Operative sequence — modified Broström-Gould
- Supine, sandbag under the ipsilateral hip, thigh tourniquet, foot over the end of the table for access, loupes on.
- Mark the lateral malleolus, the sinus tarsi, and the course of the superficial peroneal nerve as it crosses the dorsum (often palpable with the foot plantarflexed and inverted).
- A curvilinear incision centred over the lateral malleolus, about 7–8 cm, extending from its tip distally and anteriorly toward the sinus tarsi.
- The curve allows proximal extension along the fibula and distal extension into the sinus tarsi as needed.
- In the subcutaneous plane, identify and protect the superficial peroneal nerve and its dorsal intermediate and medial branches — they cross the field and are the structure most often injured (numbness or a painful neuroma, 5–10%).
- Develop full-thickness skin flaps down to the lateral malleolus to expose the ATFL remnant and the inferior extensor retinaculum (IER).
- Locate the ATFL remnant just anterior to the lateral malleolus — in chronic cases it is often thickened, elongated and scarred, sometimes a sheet of tissue rather than a discrete ligament.
- Identify the anatomic talar attachment of the ATFL (anterior to the lateral articular facet) and the CFL running obliquely from the malleolus to the lateral calcaneus.
- Confirm the inferior extensor retinaculum (a strong fascial band from the calcaneus to the lateral malleolus) — the structure used for the Gould reinforcement.
- Excise degenerate tissue from the ATFL and CFL remnants, leaving healthy tissue for imbrication.
- Prepare the bone at the fibular origin with a curette or rongeur to create a bleeding bed for healing.
- Place suture anchors (2.8–3.5 mm) at the anatomic ATFL and CFL origins on the lateral malleolus.
- Alternative: drill holes through the distal fibula (osseous tunnels) for suture passage.
- Use a separate anchor for the CFL if it is also incompetent.
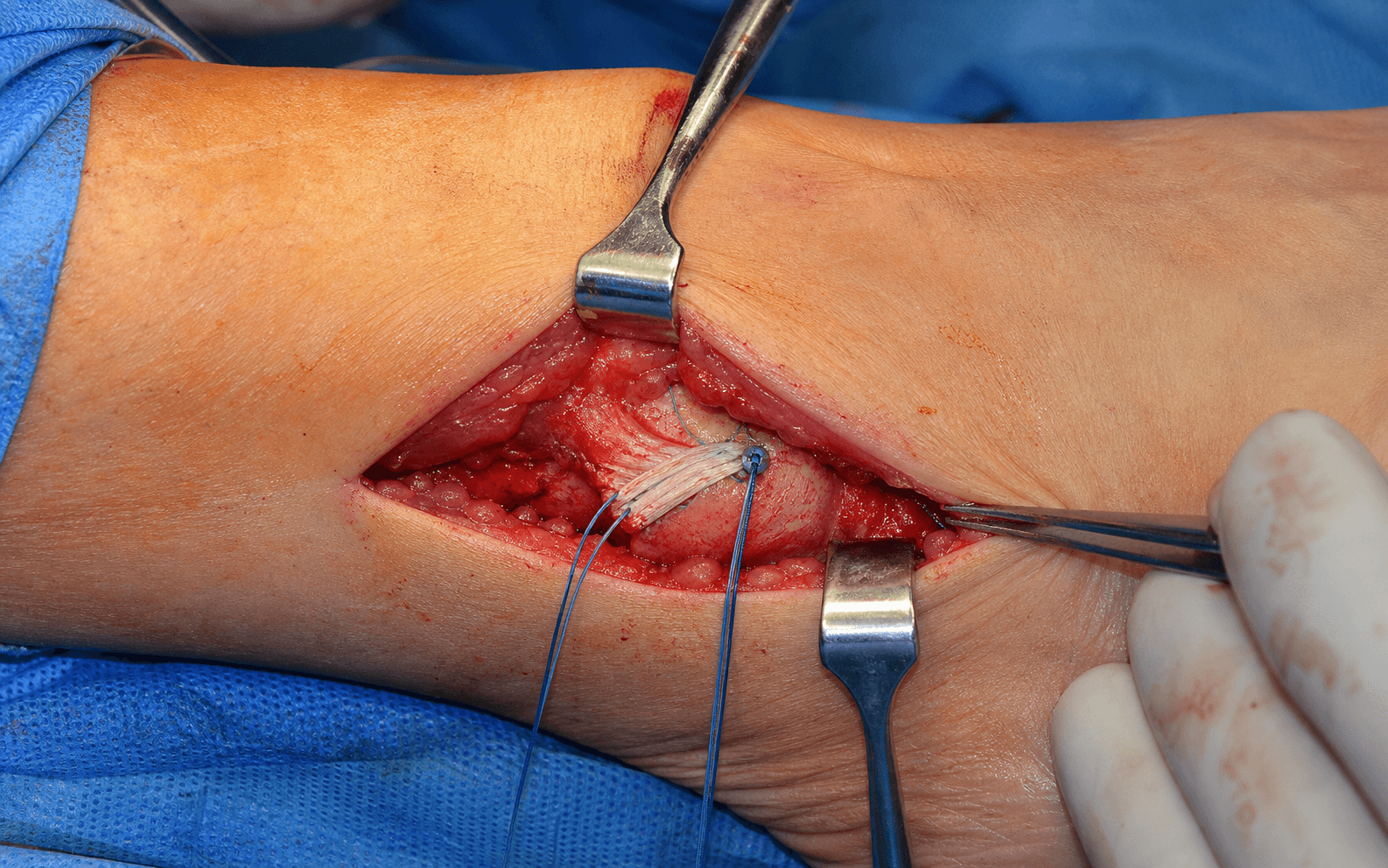
- Perform a pants-over-vest (imbrication) repair: advance the ATFL remnant anteriorly and superiorly over itself and secure it with interrupted non-absorbable sutures (0 or 2-0).
- Hold the ankle in neutral dorsiflexion and slight eversion while tying down — this sets the correct tension and avoids overtightening.
- Repeat for the CFL if involved.
- Mobilise the lateral portion of the inferior extensor retinaculum (not the superior).
- Advance and suture it over the repaired ATFL, creating a double-layer augmentation that reinforces the repair without altering the native biomechanics.
- For high-demand patients or attenuated tissue, augment the Broström-Gould with suture-tape (internal brace).
- Place one anchor at the anatomic ATFL origin on the distal fibula and a second at the talar ATFL insertion; pass the 2 mm suture tape in the anatomic (horizontal) ATFL orientation, tension with the ankle neutral, and secure — the tape lies beneath the biological repair.
- The suture tape (tensile strength 800–1200 N versus 100–150 N for the native ATFL) load-shares during healing (6–12 weeks) and protects against catastrophic early failure. It augments, not replaces, the biological repair.
Reserved for failed primary repair, generalised ligamentous laxity, or absent/poor-quality native tissue — these create a static tendon sling rather than recreating normal anatomy:
- Chrisman-Snook — splits the peroneus brevis longitudinally (distal insertion kept), routes it through the fibula then the calcaneus, reconstructing both ATFL and CFL. Sacrifices peroneal strength and may cause subtalar stiffness.
- Watson-Jones — uses the entire peroneus brevis routed through the fibula and talar neck (ATFL only); largely historical.
- Allograft reconstruction — gracilis or semitendinosus through anatomic fibular/talar/calcaneal bone tunnels; preserves native tendons, increasingly used for revision.
- Layered closure: absorbable suture to the deep tissues, then skin.
- Apply a compressive dressing with the ankle in neutral, then a posterior splint or CAM boot, non-weight-bearing.
Confirm hindfoot alignment is corrected (or being corrected) before the ligament work — varus is the commonest cause of recurrence. Through the superficial dissection, identify and protect the superficial peroneal nerve and its branches before any deep work; nerve injury is the commonest surgical complication and is largely preventable with meticulous, full-flap dissection under loupe magnification.
- Position the ankle in neutral dorsiflexion and slight eversion when tensioning the repair.
- The Gould modification uses the inferior extensor retinaculum, never the superior.
- Avoid overtightening — it causes subtalar stiffness and loss of inversion-eversion arc.
- Address concomitant pathology in the same sitting (osteochondral lesion, peroneal tendon tear, impingement osteophytes).
Anatomic Broström-Gould preserves normal ankle and subtalar kinematics and gives 85–95% good-excellent results. Non-anatomic tenodeses (Chrisman-Snook, Watson-Jones) over-constrain the subtalar joint, sacrifice a dynamic stabiliser, and carry higher stiffness rates (20–30% versus 5–10%). Reserve them for salvage — failed primary repair, absent ligament remnants, or generalised laxity.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Activity & therapy | |-------|--------|----------------|--------------------| | 1 — Protection | 0–2 weeks | Posterior splint or CAM boot, non-weight-bearing | Toe wiggling, muscle pumps; no inversion, no weight-bearing; sutures out at 10–14 days | | 2 — Early motion | 2–6 weeks | CAM boot, progress to 50% weight-bearing by week 6 | Active ankle pumps, gentle dorsiflexion/plantarflexion ROM (no inversion); therapy from week 3–4 | | 3 — Strengthening | 6–12 weeks | Lace-up brace (e.g. ASO), full weight-bearing | Progressive resistance (theraband), proprioception/balance; elliptical, bike, swimming | | 4 — Return to sport | 3–6 months | Ankle brace for sport for 12 months | Straight-line jogging, cutting drills, sport-specific; full strength and negative functional tests to return | Most patients return to sedentary work at 6–8 weeks and manual labour at 10–12 weeks. Around 85–95% return to their pre-injury activity level. Proprioceptive training is essential to prevent recurrence, and an external brace is recommended for sport for 12 months.
- No forced inversion for a minimum of 8 weeks post-operatively.
- Weight-bearing is delayed until 2 weeks after a standard Broström (may be earlier with an internal brace).
- Proprioceptive training is essential to prevent recurrence.
- External ankle support is recommended for sport for 12 months.
Complications
- Rate
- 5–10%
- Recognition
- Numbness or dysaesthesia over the dorsum; tender Tinel at the scar
- Prevention / management
- Meticulous dissection, identify and protect the nerve; usually neurapraxia settling over 3–6 months; permanent injury less than 1%
- Rate
- 3–5%
- Recognition
- Edge separation, delayed healing
- Prevention / management
- Local wound care; optimise diabetes/smoking
- Rate
- 1–2%
- Recognition
- Erythema, increasing pain, purulent discharge
- Prevention / management
- Antibiotics plus irrigation and debridement
- Rate
- 10–15% anatomic; 20–30% non-anatomic
- Recognition
- Loss of dorsiflexion (average 5–10 degrees) or subtalar motion
- Prevention / management
- Early ROM, avoid overtightening; therapy; manipulation under anaesthesia rarely needed
- Rate
- 5–15% anatomic; 15–25% non-anatomic
- Recognition
- Recurrent giving way
- Prevention / management
- Address varus, identify cause; revision reconstruction or tenodesis
- Rate
- 5–10%
- Recognition
- Pain out of keeping with a stable ankle
- Prevention / management
- Re-evaluate with MRI/CT and targeted injections — sinus tarsi, subtalar arthritis, peroneal tendinopathy, CRPS
Viva & Exam Focus
PALPAL — position-dependent function of the lateral ligaments
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old semi-professional footballer has recurrent lateral ankle sprains over 3 years with giving way several times per game, limiting play. Examination shows a positive anterior drawer (12mm) and talar tilt (18 degrees), with mild hindfoot varus. He has failed 6 months of physiotherapy and bracing.”
“A 35-year-old presents 2 years after a Broström-Gould performed elsewhere with recurrent instability. The ankle felt stable for the first 6 months then gradually loosened. Examination shows a positive anterior drawer and talar tilt; MRI shows an attenuated repair with poor tissue quality. There is no hindfoot varus.”
The Broström repair directly repairs the attenuated ATFL and CFL by imbrication/shortening. The Gould modification augments it by suturing the inferior extensor retinaculum over the repair, adding stability without sacrificing normal anatomy. It is the preferred first-line surgical treatment, with success rates greater than 85%.
Anatomic (Broström-Gould) is first-line for most patients and preserves normal mechanics. Non-anatomic tenodesis (Chrisman-Snook, Watson-Jones) is reserved for revision surgery, generalised ligamentous laxity, poor tissue quality, or high-demand athletes with absent remnants. Non-anatomic procedures sacrifice the peroneus brevis (or plantaris) and tend to over-constrain the subtalar joint.
ATFL (anterior talofibular): most commonly injured, resists inversion in plantarflexion. CFL (calcaneofibular): crosses both the ankle and subtalar joints, resists inversion in neutral/dorsiflexion. PTFL (posterior talofibular): strongest, rarely injured except in severe dislocation. The ATFL is the weakest and fails first.
A non-anatomic reconstruction using a split peroneus brevis tendon woven through the fibula and calcaneus to reconstruct both the ATFL and CFL. It sacrifices half of peroneus brevis. Indicated for revision surgery or poor tissue quality; its disadvantage is restriction of subtalar motion and weakness of eversion.
Anterior drawer assesses the ATFL — performed in slight plantarflexion (where the ATFL is the primary restraint); positive with greater than 3mm side-to-side asymmetry (absolute cutoffs often quoted around 10mm). Talar tilt (inversion stress) assesses the CFL (and ATFL) — best in neutral/dorsiflexion; positive with greater than 5 degrees asymmetry (absolute cutoffs around 10–15 degrees). Stress radiographs quantify both. Note the position dependence: ATFL tested in plantarflexion, CFL in neutral/dorsiflexion.
Immediate opener
- Lateral ligament reconstruction addresses chronic lateral ankle instability after failed conservative management
- Gold standard is Broström-Gould (anatomic repair + inferior extensor retinaculum reinforcement), 85–95% success
- Confirm mechanical instability, exclude hindfoot malalignment, identify associated pathology
Broström-Gould steps
- Curvilinear incision over the lateral malleolus, protect the superficial peroneal nerve
- Identify and excise the attenuated ATFL/CFL remnants
- Suture anchors or drill holes at the anatomic fibular origins
- Pants-over-vest repair with the ankle in neutral dorsiflexion and slight eversion
- Gould modification: advance the inferior extensor retinaculum over the repair
- Layered closure, posterior splint, non-weight-bearing
Indications vs contraindications
- Indicated: mechanical instability (anterior drawer greater than 10mm or talar tilt greater than 10 degrees difference)
- Failed 3–6 months conservative therapy including physiotherapy and bracing
- Not indicated: functional instability only (negative stress tests)
- Correct hindfoot varus greater than 5 degrees; avoid in active infection, severe PVD, Charcot
Associated pathology to identify
- Osteochondral lesion of the talus (around 35%) — treat concurrently
- Peroneal tendon pathology (around 25%) — tears or subluxation
- Sinus tarsi syndrome (around 20%), anterior impingement osteophytes
- Hindfoot varus (needs calcaneal osteotomy), subtalar instability
Complications by timeframe
- Early: superficial peroneal nerve injury (5–10%), wound problems (3–5%), infection (1–2%)
- Late: ankle stiffness (10–15% anatomic, higher non-anatomic)
- Recurrent instability (5–15% anatomic), chronic pain without instability (5–10%)
- Loss of motion, especially dorsiflexion (average 5–10 degrees)
Anatomic vs non-anatomic
- Anatomic (Broström): direct repair of ATFL/CFL, preserves biomechanics, 90–95% success, first-line
- Non-anatomic (Chrisman-Snook, Watson-Jones): tendon graft, 75–85% success, 20–30% stiffness
- Allograft (gracilis/semitendinosus) in anatomic position — increasing use for revision
Rehabilitation milestones
- 0–2 weeks: splint, non-weight-bearing, sutures out 10–14 days
- 2–6 weeks: CAM boot, progress to 50% weight-bearing, gentle ROM
- 6–12 weeks: full weight-bearing in brace, strengthening and proprioception
- 3–6 months: return to sport with functional testing, brace for sport for 12 months
High-yield viva points
- Always correct hindfoot varus (greater than 5 degrees needs osteotomy) or 50–70% failure
- Distinguish mechanical from functional instability — surgery only for mechanical
- Tension the repair in neutral dorsiflexion and slight eversion
- Gould modification uses the inferior (not superior) extensor retinaculum
- Internal brace augments — it does not replace — the biological repair
- Associated pathology present in 40–70% and drives persistent symptoms if missed
Background & Evidence
Epidemiology. Lateral ankle sprains are among the most common musculoskeletal injuries worldwide and are especially frequent in court and field sports (basketball, netball, football codes, volleyball). The ATFL is involved in the large majority of inversion sprains, and approximately 20–40% of individuals progress to chronic lateral ankle instability, generating a substantial burden in both athletic and general populations across all regions. The lateral ligament complex. Three distinct ligaments provide sequential restraint through the range of ankle motion:
Origin: anterior border of the distal fibula. Insertion: talar body, anterior to the lateral articular facet. Orientation: horizontal in neutral, vertical in plantarflexion. Primary restraint: inversion in plantarflexion and anterior talar translation. Clinical: most commonly injured ligament (around 85% of ankle sprains); the weakest of the three.
Origin: anterior aspect of the lateral malleolus. Insertion: lateral calcaneus. Orientation: oblique posteroinferior. Primary restraint: inversion in neutral and dorsiflexion, and subtalar inversion. Special feature: crosses both the ankle and subtalar joints. Second most commonly injured (around 75% when the ATFL is torn).
Origin: posterior border of the lateral malleolus (malleolar fossa). Insertion: posterior process of the talus. Orientation: nearly horizontal. Primary restraint: posterior talar translation and internal rotation. Clinical: the thickest and strongest; rarely injured except in severe trauma or dislocation.
Biomechanics. The lateral ligaments provide roughly 30–40% of total ankle stability; osseous congruity (the mortise) and the surrounding musculature provide the remainder. Functionally the ligaments work as a sequence: in plantarflexion the ATFL is vertical and the primary inversion restraint, while in dorsiflexion the ATFL relaxes and the CFL becomes the principal restraint to inversion and subtalar tilt. Because the CFL bridges both the talocrural and subtalar joints, combined ATFL plus CFL deficiency produces clinically meaningful talar tilt and subtalar instability, whereas isolated CFL insufficiency rarely causes symptomatic instability. This position dependence underpins clinical testing — the anterior drawer (ATFL) is assessed in slight plantarflexion and the talar tilt (CFL) in neutral/dorsiflexion. Anatomic repair restores this normal kinematic sequence; non-anatomic tenodeses do not, which is why they over-constrain the subtalar joint and reduce the inversion-eversion arc. Pathophysiology — acute sprain to chronic instability. An initial injury causes ligament elongation (3–5 mm) rather than complete disruption in many cases. Repetitive giving-way episodes drive progressive attenuation, capsular laxity and proprioceptive deficits, with associated pathology developing in 40–70% (osteochondral lesions around 35%, peroneal tendon pathology around 25%, sinus tarsi syndrome around 20%). Reported outcomes. The Broström-Gould achieves 85–95% good-excellent satisfaction, return to pre-injury sport in 80–90% of athletes at an average 4–6 months, and recurrence of 5–10% at 5 years (rising to 12–15% at 10 years). Non-anatomic reconstructions show lower success (75–85%) and higher stiffness (20–30%). Patient-reported AOFAS Ankle-Hindfoot scores average 88–92 postoperatively (from 55–65 preoperatively) and FAAM scores average 85–90% of maximum. Guidelines, registries and global practice. There is broad international agreement on the core principles — confirm mechanical instability, exhaust structured rehabilitation, correct hindfoot varus, and prefer anatomic repair. Genuine variation is mainly in the uptake of arthroscopic versus open repair and the threshold for suture-tape augmentation.
- Position on management
- Standardised diagnostic criteria for chronic ankle instability — a history of a significant sprain plus recurrent giving way, episodes of instability and/or self-reported functional deficits; used to standardise patient selection and research
- Position on management
- Anatomic Broström-Gould is first-line surgical treatment; arthroscopic assessment recommended to identify and treat intra-articular pathology
- Position on management
- Anatomic Broström-Gould is the reference standard; suture-tape augmentation selectively for high-demand patients or attenuated tissue; non-anatomic tenodesis reserved for salvage
- Position on management
- Minimum 3–6 months structured rehabilitation before surgery; operate for demonstrable mechanical instability; address hindfoot malalignment and concomitant pathology concurrently
Practice variation. Arthroscopic Broström is increasingly adopted in high-volume sports-medicine centres (faster weight-bearing, lower wound-complication rate) but remains technically demanding and less available in lower-resource settings, where open repair predominates. Allograft availability and regulation differ markedly by region, influencing the choice between allograft reconstruction and autograft (peroneal/hamstring) tenodesis for revision cases.
References
Suture Tape Augmentation vs Modified Broström (multicentre RCT)
- Prospective multicentre RCT, 119 patients randomised to modified Broström (n=59) or Broström plus suture-tape augmentation (n=60)
- Mean return to pre-injury activity was 13.3 weeks with suture tape vs 17.5 weeks with Broström alone (p less than 0.001)
- Complication rate 1.7% (suture tape) vs 8.5% (Broström alone); difference not statistically significant (p=0.12)
- Suture-tape augmentation supported an accelerated rehabilitation protocol without increased morbidity
Suture-Tape Augmentation vs Modified Broström — Intermediate-Term RCT
- Single-surgeon RCT, 60 young female patients with chronic lateral ankle instability, minimum 2-year follow-up
- No significant difference between suture-tape augmentation and modified Broström in FAOS, FAAM, recurrence, or stress radiographs
- Total medical cost was approximately 1.3 times higher in the suture-tape group (p less than 0.001) despite shorter operating time
Open vs Arthroscopic Broström for Chronic Lateral Ankle Instability
- Systematic review and meta-analysis of 8 comparative studies, 408 patients (193 open, 215 arthroscopic)
- Arthroscopic repair gave higher 1-year AOFAS scores (88.6 vs 80.1) and lower VAS pain scores
- Mean time to weight-bearing 9.0 weeks (arthroscopic) vs 14.25 weeks (open)
- Operative time, overall complication rate, post-op anterior drawer and talar tilt were comparable between techniques
Modified Broström-Gould vs Other Operations (RCT meta-analysis)
- Meta-analysis of 8 randomised trials, 426 patients comparing modified Broström-Gould with alternative reconstructions
- Across six functional and stability outcomes there were no clinically meaningful differences favouring more invasive procedures
- A small FAOS advantage for comparator operations (about 6.5 points) was of uncertain clinical significance
Non-Anatomic Peroneal Tenodesis (Hemi-Castaing) Long-Term Outcomes
- Retrospective cohort of hemi-Castaing peroneus brevis ligamentoplasty (uses half the peroneus brevis tendon)
- Good-to-excellent outcome in 80% (OMAS) and 65% (Karlsson); Tegner activity did not return to pre-injury level
- Long-term functional outcome was less favourable than published anatomic-repair series