Limited Muscle-Splitting TKA | VMO Longitudinal Split | Balanced Exposure
- The midvastus approach is a muscle-splitting modification of the medial parapatellar approach: the distal 3-4cm of the vastus medialis obliquus (VMO) is separated in line with its oblique fibres from the superomedial patella, avoiding any cut through the quadriceps tendon (Engh, RCT 1997).
- VMO fibres run obliquely (roughly 50-55 degrees to the femoral long axis) from the adductor magnus tendon down to the superomedial patella; the split follows this line, separating WITH the fibres rather than cutting across them.
- Pooled RCT evidence (Alcelik 2011, 18 trials, 1040 patients) shows modest early gains — better first-week flexion (mean about 9 degrees), lower early pain, and fewer lateral retinacular releases than the medial parapatellar approach — with quadriceps strength and clinical scores equalising by 3-6 months.
- Exposure is adequate for most primary TKAs in patients of normal to moderate build; the proximal apex of the split limits extensile capacity compared with a full medial parapatellar arthrotomy.
- Best suited to primary TKA with reasonable preoperative flexion (at least 70-80 degrees) and standard deformity (less than 20 degrees) in a patient of suitable build (BMI less than 35).
- The muscle-sparing claim is only partial: EMG data (Parentis 1999) show VMO denervation in about 43 percent of vastus-splitting knees, and biochemical data (Huang 2012) show no reduction — sometimes an increase — in creatine kinase.
When & Why
What it exposes. The midvastus approach exposes the knee for primary total knee arthroplasty through a muscle-splitting variant of the medial parapatellar arthrotomy. Instead of incising the quadriceps tendon, the distal 3-4cm of the vastus medialis obliquus is separated bluntly in line with its oblique fibres, beginning at the superomedial corner of the patella. It is the most versatile of the muscle-preserving knee approaches — broader in applicability than subvastus, with faster early recovery than a full medial parapatellar arthrotomy. Why choose it (the middle ground). Conceptually it sits between subvastus and the standard medial parapatellar approach: it disturbs some muscle, but leaves the quadriceps tendon intact and is easier to expose through than subvastus while still showing early benefits over medial parapatellar (better first-week flexion, lower early pain, fewer lateral retinacular releases in pooled RCT data). The medial parapatellar arthrotomy remains the default, universally taught approach; the midvastus is a recognised muscle-splitting variant rather than a mandated competency, because the standard parapatellar arthrotomy is adequate and extensile for all cases. Best indications (primary TKA). - Most primary TKAs in normal to mildly overweight patients (BMI less than 35).
- Standard deformity correction (varus or valgus less than 20 degrees).
- Reasonable preoperative ROM (flexion at least 70-80 degrees).
- Primary osteoarthritis or inflammatory arthritis.
- Patients prioritising faster recovery, and bilateral staged TKA where a balance of recovery and versatility is wanted. Contraindications. - Absolute: revision TKA (needs extensile exposure); previous open knee surgery with significant scarring.
- Relative: severe obesity (BMI greater than 35 — difficult exposure); severe deformity (greater than 20 degrees — may need extensive releases); severe stiffness (flexion less than 60 degrees — hard to expose); patella baja (low patella difficult to evert); inflammatory arthritis with severe bone loss. Position and landmarks. Supine on the OR table with a leg holder or side post at the thigh (allowing 90-degree flexion and aiding patellar eversion — pad carefully to protect the common peroneal nerve), and a proximal-thigh tourniquet (recommended for a bloodless field and easier VMO fibre identification; deflate before closure). A bump under the hip is optional. Palpable landmarks are the patella, the medial femoral epicondyle, the adductor tubercle, the tibial tubercle and the medial joint line.
- Midvastus
- Limited VMO split (3-4cm distal fibres)
- Subvastus
- None (VMO elevated)
- Medial parapatellar
- Full VMO and retinaculum cut
- Midvastus
- Good (adequate for most cases)
- Subvastus
- Limited (challenging in some)
- Medial parapatellar
- Excellent (gold standard)
- Midvastus
- Broad (most primary TKAs)
- Subvastus
- Narrow (thin, good ROM only)
- Medial parapatellar
- Universal (all TKAs)
- Midvastus
- Earlier SLR and less early pain than parapatellar (RCT data)
- Subvastus
- Tends to be the earliest, but evidence limited
- Medial parapatellar
- Slowest early SLR of the three
- Midvastus
- Early flexion benefit; equalises by 3-6 months
- Subvastus
- Early benefit reported; equalises long term
- Medial parapatellar
- Slower early, equivalent long term
- Midvastus
- Lower than parapatellar in pooled RCTs
- Subvastus
- Lower than parapatellar (better tracking)
- Medial parapatellar
- Reference / highest
- Midvastus
- Present in a minority (abnormal EMG ~43%, Parentis)
- Subvastus
- Lowest (muscle elevated, not split)
- Medial parapatellar
- Quadriceps tendon cut; VMO belly spared
- Midvastus
- Moderate
- Subvastus
- Steep
- Medial parapatellar
- Standard
- Midvastus
- Possible but limited
- Subvastus
- Contraindicated
- Medial parapatellar
- Standard approach
- Midvastus
- Good for routine primary TKA; limited extensile reach
- Subvastus
- Narrower indications (build, ROM, deformity)
- Medial parapatellar
- Most versatile; extensile and revision-capable
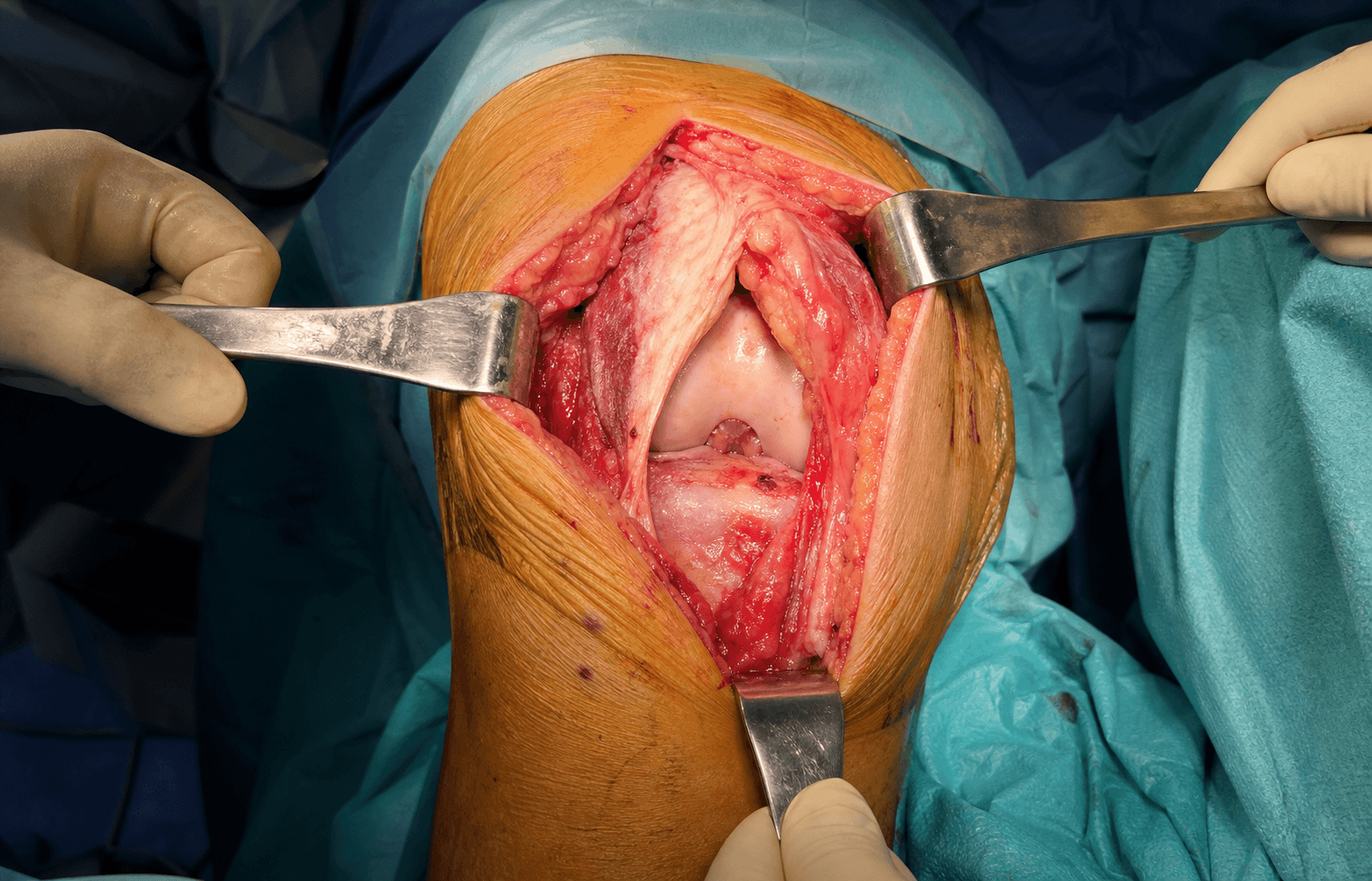
The Exposure
The midvastus split succeeds or fails on one principle: separate the distal VMO in line with its oblique fibres from the superomedial patella, keeping the split short and distal to spare the VMO motor nerve. Understanding the surgical anatomy is what makes that safe. VMO nerve supply — the key constraint. The VMO is supplied by the most distal branch of the nerve to vastus medialis (from the femoral nerve, posterior division), which runs on the deep surface of the muscle alongside branches of the descending genicular vessels and typically enters the VMO from its deep, proximal aspect. Keeping the split short and distal aims to spare this pedicle — but cadaveric and EMG data show the nerve can run more distally than assumed, so even a limited distal split can denervate part of the VMO (Parentis 1999 found abnormal postoperative EMG in 43 percent of vastus-splitting knees). The anatomic principle is therefore to keep the split limited (around 3-4cm) and distal, avoid extending the apex proximally into the thicker, more densely innervated muscle belly, and accept that the muscle-sparing benefit is partial rather than absolute. The muscle you are splitting. The oblique distal VMO fibres arise from the adductor magnus tendon proximally and run obliquely (roughly 50-55 degrees to the femoral long axis) downward and laterally to insert on the superomedial border of the patella. Separating in line with these fibres is far less traumatic than cutting transversely across the muscle belly.
Exposure sequence
- A midline or slightly medial incision beginning 5-6cm proximal to the superior pole of the patella and extending to the tibial tubercle (about 2cm distal to it); typical length 10-15cm.
- Develop a medial subcutaneous flap to the patellar border to expose the VMO muscle belly, with haemostasis by electrocautery.
- Palpate the VMO muscle belly medial to the patella and identify its fibre direction — oblique, roughly 50-55 degrees to the femoral long axis, running from the adductor magnus tendon proximally to the superomedial patella distally.
- Plan the split line from the superomedial corner of the patella, continuous with the medial arthrotomy, angling proximally and medially parallel to the fibres; the proximal apex should sit about 3-4cm above the superior pole of the patella — do not extend further.
- Begin at the superomedial corner of the patella, continuous with the medial arthrotomy, and separate the VMO fibres bluntly (finger or scissors) in line with the fibre direction, angling proximally and medially.
- Reserve electrocautery for haemostasis of crossing vessels — not for cutting through the muscle belly.
- Carry the blunt separation proximally for about 3-4cm to the apex; separate WITH the fibres — never transect the muscle across its fibres.
- Stay distal: the more proximal the apex, the greater the risk to the VMO motor branch; coagulate small intramuscular bleeders as they are encountered.
- Continue the incision through the medial retinaculum from the VMO split down to the tibial tubercle as a standard medial arthrotomy.
- The proximal split extends through the joint capsule along the same oblique line as the VMO split.
- Flex the knee to 90 degrees and evert the patella laterally.
- Eversion is easier than subvastus (better exposure) but harder than a full medial parapatellar arthrotomy (some VMO remains intact).
- The femoral condyles and tibial plateau should be visualised adequately; if exposure is tight, extend the VMO split a little more proximally (rare).
- Through the exposure, perform the tibial resection and the femoral cuts (distal, anterior, posterior, chamfer), with sizing and rotation assessment.
- Balance flexion and extension gaps with soft-tissue releases as needed, then trial, cement and implant components (CR or PS femoral, tibial baseplate and insert, patellar button), and resurface the patella by standard technique.
- Re-approximate the split VMO fibres side-to-side with 3-4 interrupted #1 absorbable (Vicryl) sutures through the muscle belly.
- Close the medial capsule and retinaculum in a watertight layer (#1 Vicryl, continuous or interrupted), then the fascia over the VMO (2-0 Vicryl), the subcutaneous layer (2-0 Vicryl) and skin (3-0 Monocryl or staples).
- Consider an intra-articular drain, removed when output is less than 30mL per shift.
The midvastus split must follow the VMO fibre direction (obliquely, roughly 50-55 degrees to the femoral long axis). Cutting transversely across the fibres causes more damage and erodes the muscle-preserving rationale. The other avoidable harm is over-splitting: extending the apex too far proximally threatens the VMO motor branch (the distal branch of the nerve to vastus medialis) and is the source of the EMG-documented denervation seen in a substantial minority of patients. Think "separate with the grain", and keep the apex limited and distal, around 3-4cm above the superior pole of the patella.
Although the split was limited to 3-4cm and followed the fibres, proper side-to-side repair of the VMO at closure optimises muscle healing and function and guards against dehiscence. Do not simply close the capsule and ignore the split muscle.
Dangers & Extensions
The danger structure of this approach is the VMO motor nerve — the distal branch of the nerve to vastus medialis (femoral nerve) — together with the descending genicular / intramuscular vessels crossed during the split, and the extensor mechanism generally. Most pitfalls flow from a split that is too long, too proximal, or made across the fibres.
- Problem
- Inadequate exposure (obese, stiff or severely deformed knee)
- Prevention / management
- Extend the VMO split a little more proximally (accepting greater muscle/nerve risk); if still inadequate, convert to a standard medial parapatellar arthrotomy through the quadriceps tendon
- Problem
- VMO damage from over-splitting or splitting across fibres
- Prevention / management
- Limit the split to 3-4cm; follow the fibre direction; do not extend into the proximal VMO (critical innervation)
- Problem
- Bleeding from the vascular VMO
- Prevention / management
- Cauterise crossing vessels as you split; direct pressure, cautery, rarely suture ligation
- Problem
- Quadriceps weakness / VMO denervation
- Prevention / management
- EMG studies show a notable minority develop denervation (Parentis: abnormal EMG 43%); early flexion still favours midvastus, strength equalises by 3-6 months
- Problem
- VMO dehiscence
- Prevention / management
- Secure side-to-side approximation of the split muscle and capsule at closure
- Problem
- Wound complications (haematoma, delayed healing, infection)
- Prevention / management
- Broadly similar to other anterior knee approaches; meticulous haemostasis and layered closure
- Problem
- Extensor lag
- Prevention / management
- Possible if VMO significantly denervated or repair inadequate; pooled data show no consistent difference vs medial parapatellar
- Problem
- Patellar maltracking
- Prevention / management
- Check trial tracking before final implantation; lateral release only if needed (fewer required than with parapatellar)
- Problem
- Standard TKA complications (loosening, instability, stiffness, periprosthetic fracture)
- Prevention / management
- No consistent difference from other approaches in long-term outcomes
Extensile options. If exposure is inadequate, the options are sequential: first extend the VMO split a little more proximally (accepting greater muscle and nerve risk), and if that is still insufficient, convert to a standard medial parapatellar arthrotomy by completing the incision through the quadriceps tendon. The midvastus apex fundamentally limits proximal extensile reach, which is why revision TKA and the difficult primary knee favour the standard parapatellar approach from the outset. Postoperative management and recovery. Enhanced-recovery protocols dominate the early course: sit the patient at the bedside on Day 1 and ambulate on Day 1-2; straight-leg raise tends to be achieved earlier than with the medial parapatellar approach (exact day varies with patient, anaesthesia and rehab protocol). Use multimodal analgesia with an adductor canal block (which preserves quadriceps function) preferred over a femoral nerve block — a femoral block delays quad recovery and defeats the purpose of a quadriceps-sparing approach. Weight-bearing is as tolerated from Day 1 (walker or crutches for 2-4 weeks, cane by 4-6 weeks), with ROM goals of 90 degrees by Week 1-2 and 0-110 degrees by 6 weeks. Typical return to activity: ADLs 2-4 weeks, driving and sedentary work 4-6 weeks, labour 8-12 weeks, full activities 12-16 weeks.
Procedures Through This Approach
- Primary total knee arthroplasty — the principal operation done through this exposure, in suitable patients (BMI less than 35, flexion at least 70-80 degrees, deformity less than 20 degrees).
- Muscle-sparing TKA within an enhanced-recovery pathway, where the early functional gains (better first-week flexion, earlier straight-leg raise, fewer lateral releases) are prioritised.
- Bilateral staged primary TKA, where a balance of recovery and versatility is wanted. Inadequate exposure or a more complex knee (revision, severe deformity, marked obesity, stiffness, patella baja) is managed by extending the split or converting to a standard medial parapatellar arthrotomy.
Viva & Exam Focus
MIDVASTUSMIDVASTUS — approach selection criteria
VMO SPLITVMO SPLIT — midvastus technique principles
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman (BMI 32) with primary knee OA needs a TKA. She has 80 degrees of flexion and a 10-degree varus deformity, and asks which surgical approach you will use. You are considering a midvastus approach — is she suitable, and how do you perform it?”
“A resident asks: why split the vastus medialis at all in the midvastus approach, rather than going under it as in subvastus, which preserves all the muscle?”
Key decision points
- Midvastus = muscle-splitting modification of the medial parapatellar approach (VMO split, quadriceps tendon spared)
- Suited to primary TKA with reasonable flexion and standard deformity in a patient of suitable build
- Choose medial parapatellar for: revision, marked obesity, severe deformity, stiff knee, patella baja
- Choose subvastus when full muscle preservation is the priority in a favourable knee
- If exposure is inadequate, extend proximally or convert to a full medial parapatellar arthrotomy
Technical pearls
- Separate the distal VMO about 3-4cm in line with the muscle fibres (roughly 50-55 degrees to the femoral long axis)
- Start at the superomedial corner of the patella, extending to the medial patellar insertion
- Split WITH the fibres (like splitting wood) — not across them
- Limited to the distal VMO (preserves proximal VMO innervation)
- Repair the split VMO at closure with 3-4 interrupted #1 Vicryl sutures
Complication avoidance
- Do not over-split: limit to 3-4cm of distal VMO only (avoid the proximal dense innervation)
- Follow the fibre direction: oblique, not transverse
- Secure the VMO repair at closure (prevents dehiscence)
- Use an adductor canal block, not a femoral block (preserves quad function)
- Extend the split proximally if exposure is inadequate — do not force it
Viva preparation
- VMO fibres run obliquely (roughly 50-55 degrees to the femoral long axis) from the adductor magnus tendon to the superomedial patella
- Evidence-based advantages: better early flexion, lower early pain, fewer lateral releases vs parapatellar
- Honest caveats: muscle-sparing claim is partial — VMO denervation on EMG and no reduction in creatine kinase in some studies
- Long-term outcomes equalise with medial parapatellar by 3-6 months
- Know the comparison: medial parapatellar vs midvastus vs subvastus
Key evidence points
- Engh 1997 (RCT): original description; excellent exposure, equivalent quad strength and patellar stability
- Alcelik 2011 (meta-analysis, 18 RCTs, 1040 patients): better week-1 flexion and VAS, fewer lateral releases
- Parentis 1999 (RCT): abnormal postoperative EMG in 43 percent of vastus-splitting knees (denervation)
- Huang 2012: mini-midvastus showed higher creatine kinase — no muscle-sparing superiority
- Benefits are early and modest; they disappear by 3-6 months
References
Guidelines, registries and global practice The medial parapatellar arthrotomy remains the default, universally taught approach to the knee for primary and revision TKA across all major training systems (advanced orthopaedic practice Tr and Orth, advanced orthopaedic practice, DNB/MS). The midvastus approach is taught as a recognised muscle-splitting variant rather than a mandated competency, because the standard parapatellar arthrotomy is adequate and extensile for all cases. | Source / body | Position relevant to the midvastus approach | |---|---| | Pooled RCT evidence (Alcelik 2011; Liu and Yang 2011) | Modest early benefit over medial parapatellar — better week-1 flexion, less early pain, fewer lateral releases; outcomes equalise by 3-6 months | | Biochemical / EMG data (Parentis 1999; Huang 2012) | The muscle-sparing claim is partial: VMO denervation on EMG in a minority, and creatine kinase not reduced (sometimes higher) than parapatellar | | Enhanced Recovery After Surgery (ERAS) consensus | Approach choice is secondary to multimodal analgesia, opioid-sparing protocols and early mobilisation; favours quadriceps-sparing regional blocks | National arthroplasty registries (NJR for England and Wales, AOANJRR in Australia and NZ, AJRR in the USA, the Swedish and Norwegian registries) record implant survivorship and revision but do not generally stratify outcomes by surgical approach, and there is no registry signal that approach selection affects long-term implant survival. Approach choice is therefore an early-recovery and surgeon-preference decision, not a survivorship one. In lower-resource settings the standard medial parapatellar approach predominates because it is reliable, extensile, and does not depend on optimal patient selection; muscle-splitting variants are more often used in high-volume elective arthroplasty practice and within enhanced-recovery pathways where early functional gains are prioritised. Perioperative principles applied globally: antibiotic prophylaxis with a first- or second-generation cephalosporin (e.g. cefazolin) within 60 minutes of incision, weight-adjusted, per surgical-site-infection prevention guidance (WHO, AAOS, NICE); multimodal opioid-sparing analgesia with an adductor canal block preferred over a femoral nerve block to preserve quadriceps strength (particularly relevant when the rationale for the approach is faster quadriceps recovery); and early mobilisation with quadriceps activation within enhanced-recovery protocols.
A midvastus muscle-splitting approach for total knee arthroplasty
- Prospective RCT of 118 consecutive primary TKAs (single surgeon), medial parapatellar vs midvastus muscle-splitting
- Original description: the VMO is separated in line with its fibres beginning at the superior pole of the patella
- The midvastus approach provided excellent exposure to all knees
- Patellar stability and quadriceps strength were equivalent between the two approaches
A comparison of the midvastus and paramedian approaches for total knee arthroplasty
- Prospective, double-blinded RCT in 24 patients undergoing simultaneous bilateral TKA (each patient as own control)
- Midvastus side offered an early advantage of less pain and earlier return to function
- No significant complications associated with the midvastus approach
- Authors recommend the approach be part of the knee surgeon's armamentarium
Comparing the mid-vastus and medial parapatellar approaches in total knee arthroplasty: a meta-analysis of short term outcomes
- Meta-analysis of 18 randomised and quasi-randomised trials, 1040 patients
- Midvastus gave significantly better first-week flexion (mean difference about 8.9 degrees) and lower first-week VAS pain
- Significantly fewer lateral retinacular releases were required with midvastus
- No increase in complication rates compared with the medial parapatellar approach
A comparison of the vastus splitting and median parapatellar approaches in total knee arthroplasty
- Prospective RCT of 51 knees in 42 patients with pre- and post-operative electromyography
- No significant difference in strength, ROM, knee scores, tourniquet time or proprioception between approaches
- Vastus-splitting group had fewer lateral releases and less blood loss
- Abnormal postoperative EMG (VMO denervation) in 9 of 21 (43 percent) vastus-splitting knees vs none in the parapatellar group
Comparison of the minimally invasive and standard medial parapatellar approaches for total knee arthroplasty: systematic review and meta-analysis
- Systematic review and meta-analysis of minimally invasive subvastus (SV) and midvastus (MV) vs standard medial parapatellar (MP)
- Days to straight-leg raise were significantly longer after MP than after either MV or SV
- MV was associated with better range of motion than MP in the first 6 months postoperatively
- Quadriceps strength recovered more slowly after MP than after SV
Mini-midvastus versus medial parapatellar approach in TKA: muscle damage and inflammation markers
- Prospective controlled trial of 60 unilateral TKAs (30 mini-midvastus, 30 medial parapatellar)
- Serum creatine kinase was significantly higher in the mini-midvastus group (postoperative days 2 and 3, and cumulatively)
- C-reactive protein and interleukin-6 were higher in the parapatellar group
- Authors concluded the mini-midvastus approach has no muscle-sparing superiority and may cause more muscle damage