Lateral Kocher approach (between ECU and anconeus) | Mason type 2 and reconstructable type 3 | advanced
- Displaced Mason type 2 fractures (a marginal fragment greater than 2mm displaced and greater than 30% of the articular surface) require ORIF when the fragment is reconstructable and stable fixation is achievable.
- Mason type 3 (comminuted) fractures demand a decision between ORIF and arthroplasty based on fragment size, fragment number and associated elbow instability. More than three articular fragments generally do badly with ORIF and are better replaced.
- A mechanical block to forearm rotation is an ABSOLUTE indication for surgery regardless of the displacement measured on radiographs.
- Associated elbow instability (the terrible triad, or an Essex-Lopresti injury) mandates radial head PRESERVATION by ORIF or arthroplasty. Excision is contraindicated.
- All hardware must sit within the 110° anterolateral safe zone that never articulates with the proximal radioulnar joint — hardware outside this arc impinges throughout pronation-supination.
- Keep the forearm fully supinated throughout the approach: this swings the posterior interosseous nerve (PIN) anteriorly, away from the field. Most PIN injuries follow inadvertent pronation during dissection.
- Aim for an anatomic articular reduction — less than 1mm step-off. Greater than 1mm of incongruity drives post-traumatic arthritis.
When & Why
Indication. Open reduction internal fixation is offered for a displaced radial head fracture that is reconstructable and amenable to stable fixation, that blocks forearm rotation, or that forms part of an unstable elbow injury in which the radial head must be preserved. The Mason classification drives the decision (full staging is in Background & Evidence). Absolute indications:
- Displaced Mason type 2 fractures — a marginal fragment greater than 2mm displaced and greater than 30% of the articular surface.
- Mason type 3 fractures that are comminuted but still reconstructable with stable fixation.
- A mechanical block to forearm rotation — impingement from a displaced fragment, regardless of measured displacement.
- Associated elbow instability requiring radial head preservation — the terrible triad and the Essex-Lopresti injury. Relative indications:
- A Mason type 2 fracture with 2mm displacement where the patient elects surgery.
- A radial head fracture with a concurrent MCL or LCL injury that needs the head as a lateral stabiliser.
- A marginal fracture involving greater than 25% of the head circumference. Contraindications:
- Mason type 1 fractures (less than 2mm displacement, no block to rotation) — manage non-operatively with early range of motion.
- Comminuted fractures not amenable to stable fixation — consider arthroplasty instead.
- Active infection at the surgical site, or medical comorbidities precluding surgery.
- A small fragment less than 25% of the head circumference in a stable elbow — consider excision. The one decision that matters — fix, excise, or replace? Every displaced fracture is assessed intra-operatively for reconstructability and elbow stability, then matched to one of three strategies:
For reconstructable Mason type 2 and type 3A patterns — a fragment greater than 25% of the head, three or fewer articular fragments, and good bone quality. Buried headless screws or a low-profile mini-fragment plate placed within the safe zone.
Reserved for a small fragment (less than 25%) in a thoroughly stable elbow with NO LUCL or MCL injury and NO Essex-Lopresti pattern. Never excise in an unstable elbow — it removes the lateral column and invites recurrent instability.
For a comminuted head with more than three fragments that is not reconstructable, or any fracture in an unstable elbow (terrible triad, Essex-Lopresti). A modular metal prosthesis restores radiocapitellar contact — the technical pitfall to avoid is an over-sized, overstuffed head.
Assess the whole elbow, not just the head. Before committing, exclude or plan for the associated injuries that change everything:
- The terrible triad (radial head fracture plus coronoid fracture plus elbow dislocation). All three components must be addressed in sequence — coronoid first, then the radial head, then the lateral ligament complex — to restore a concentric, stable joint.
- The Essex-Lopresti injury (radial head fracture plus interosseous membrane disruption plus DRUJ disruption). Examine the wrist in every radial head fracture: wrist pain and DRUJ instability are red flags. The radial head MUST be preserved — excision causes progressive proximal radial migration and DRUJ arthrosis.
- Associated MCL injury. Assess with valgus stress under fluoroscopy — opening greater than 3mm means MCL disruption needing repair through a separate medial approach. Consent specifically for posterior interosseous nerve (PIN) neuropraxia (transient weakness of finger and thumb extension), stiffness and loss of terminal rotation, heterotopic ossification, painful or prominent hardware requiring later removal, loss of reduction, and post-traumatic arthritis. Setup. Supine with the arm across the chest or on a hand table, or lateral decubitus if other injuries demand it. The position must allow full elbow flexion-extension and full forearm pronation-supination for intra-operative assessment, with the shoulder abducted less than 90° to avoid brachial plexus traction. General or regional anaesthesia; upper-arm tourniquet; image intensifier available.
The Operation
The goal is to expose the radial head through the lateral Kocher interval, protect the PIN by keeping the forearm supinated, restore the articular surface to within 1mm, place all fixation within the non-articulating safe zone, and repair the lateral ligamentous stabilisers so the elbow is concentric and stable through a full arc. The exposure — the Kocher approach between ECU and anconeus — is the heart of the operation and is laid out in the first steps below (in depth on the Kocher approach to the elbow page).
Operative sequence
- Supine, arm across the chest or on a hand table (lateral decubitus if other injuries require it). Shoulder abducted less than 90° to avoid brachial plexus traction.
- Confirm before draping that you can achieve full elbow flexion-extension AND full forearm pronation-supination — both are needed for intra-operative stability assessment and PIN protection.
- Apply valgus stress under fluoroscopy: medial opening greater than 3mm indicates MCL injury requiring repair.
- Perform the posterolateral rotatory test: subluxation indicates LUCL injury.
- Test forearm rotation: a mechanical block indicates impingement from a displaced fragment — an absolute indication for surgery.
- Stability assessment here drives the decision between ORIF, excision and arthroplasty — an unstable elbow mandates radial head preservation.
- Palpate the lateral epicondyle, the radial head (which rotates with the forearm) and the ulna.
- Mark a 6 to 10cm lateral incision centred over the radial head, beginning at the lateral epicondyle and extending distally; it may curve slightly posterior to follow the Kocher internervous plane.
- Palpate the radial head while rotating the forearm to confirm the level before incising — prevents an approach that is too proximal or too distal.
- The PIN enters the supinator about 1 to 2cm distal to the radial head in pronation but rotates anteriorly, away from the field, in full supination.
- Maintain full supination throughout the approach and the deep dissection. Have an assistant hold it. Most PIN injuries follow inadvertent pronation during the critical steps.
- Incise skin and subcutaneous tissue and identify the internervous plane between the anconeus posteriorly and extensor carpi ulnaris (ECU) anteriorly.
- Both muscles are supplied by the posterior interosseous nerve, so this is a true internervous plane and is safe for the PIN, which remains anterior in supination.
- Bluntly separate the anconeus from ECU with a finger or blunt instrument.
- Identify the lateral ulnar collateral ligament (LUCL) running from the lateral epicondyle to the supinator crest — the primary restraint to posterolateral rotatory instability. Preserve it, or tag it for repair if detached.
- Incise the lateral capsule longitudinally to expose the radial head and neck, keeping the forearm supinated.
- Use minimal periosteal elevation to reduce the risk of heterotopic ossification and radioulnar synostosis.
- Inspect the articular surface, count the fragments and gauge their size. Stable fixation needs a fragment greater than 25% of the head circumference.
- If there are more than three articular fragments, or poor bone quality, or the pattern is not amenable to stable fixation, convert to arthroplasty rather than attempt doomed fixation.
- Clear haematoma and debris with irrigation under direct vision.
- Reduce the fragments to restore the spherical radial head contour, using a dental pick or freer elevator to lever them into place.
- Check the reduction from anterior, lateral and posterior views. Accept less than 1mm of step-off — greater incongruity leads to post-traumatic arthritis.
- Hold the reduction with 0.9 to 1.0mm K-wires placed outside the definitive safe zone (to be removed later), or with small pointed reduction forceps.
- Confirm with fluoroscopy (AP and lateral) and by direct visualisation of articular congruity. Provisional fixation is far easier to adjust than definitive screws.
- With the arm at the side and the forearm supinated, mark the lateral aspect of the radial head under fluoroscopy — this is the centre of the safe zone.
- The safe zone extends approximately 55° anterior and 55° posterior of that mark — an arc of roughly 90 to 110° that never articulates with the lesser sigmoid (radial) notch of the ulna through full rotation.
- Mark the boundaries with K-wires or methylene blue. All definitive hardware must stay within this arc.
- Buried headless compression screws (2.0 to 2.4mm), countersunk beneath the articular cartilage, for simple fragment patterns — minimal hardware, no prominence, but need a fragment greater than 25%.
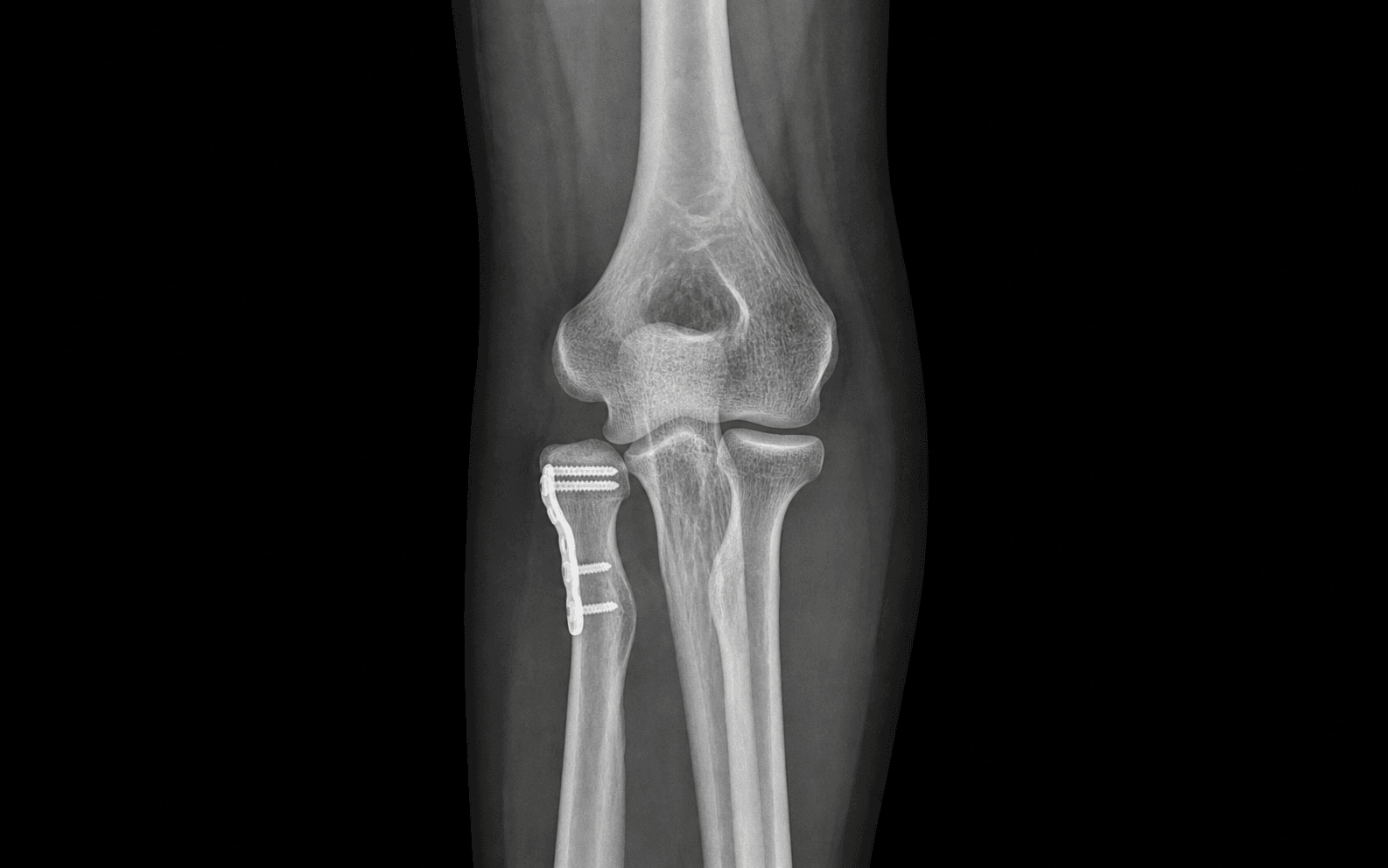
- Mini-fragment plate (2.0 to 2.4mm), anatomically contoured to the radial head and placed within the safe zone, for comminuted patterns needing a more stable column construct.
- Use at least two screws for a fragment greater than 25%. A plate for the main fracture line and lag screws for additional fragments is a useful combination.
- Remove the provisional K-wires and rotate the forearm through full pronation and supination while palpating the radial head — motion should be smooth, with no crepitus or catching and no hardware prominence.
- Confirm with fluoroscopy in pronation and supination that no hardware impinges on the proximal radioulnar joint. Revise before closure if anything catches.
- If the annular ligament was incised to expose the fracture, repair it with absorbable 2-0 suture in a side-to-side fashion to restore PRUJ stability.
- Avoid over-tightening, which restricts rotation. Test forearm rotation after repair — it should be smooth through the full arc.
- Under fluoroscopy repeat the valgus stress test (medial opening greater than 3mm means MCL injury) and the posterolateral rotatory test (subluxation means LUCL injury).
- If the LUCL is injured, repair it to its footprint on the lateral epicondyle with two or three suture anchors, passing sutures through the LUCL and common extensor origin and tying with the elbow reduced.
- In a terrible triad, address the coronoid fracture here if not already done. Document a concentric, stable reduction through the full arc with fluoroscopy.
- Irrigate thoroughly (pulse lavage) and achieve meticulous haemostasis — haematoma drives heterotopic ossification; consider a drain if dissection was extensive. Avoid thermal injury to the PIN from cautery near the supinator.
- Repair the lateral capsule with absorbable 2-0 suture to create a soft-tissue envelope over the head, testing range of motion before tying so the closure does not restrict rotation.
- Close the Kocher interval (anconeus-ECU), subcutaneous layer (3-0 absorbable) and skin (monofilament or staples) with gentle, tension-free handling.
- Apply a soft dressing and a posterior elbow splint at 90° flexion, forearm neutral, with generous padding.
- Splint for comfort and soft-tissue rest for 48 to 72 hours ONLY — not for fracture stability. Splinting that is too tight risks compartment syndrome or nerve compression, and prolonged immobilisation is the enemy after elbow trauma.
Before any deep dissection, confirm and MAINTAIN full forearm supination. The posterior interosseous nerve enters the supinator 10 to 20mm distal to the radial head and lies anterior to the radial neck in supination; pronation swings it into the operative field. Stay proximal to 2cm distal to the radial head, avoid placing retractors into the supinator or anterior to the radial head, and keep the forearm supinated throughout. The radial nerve proper runs 20 to 30mm anterior to the skin incision — avoid any dissection anterior to the capsular incision. A post-operative PIN palsy (weakness of thumb and finger extension with preserved wrist extension and no sensory loss) is usually a neuropraxia observed for 3 to 6 months.
The radial head articulates with the lesser sigmoid notch of the ulna across roughly 280° of its circumference during rotation — that entire articulating arc is forbidden territory for hardware. The non-articulating safe zone is only the 90 to 110° anterolateral arc. Identify it with the arm at the side and the forearm supinated, marking the lateral radial head under fluoroscopy, then confirm by rotating the forearm under fluoroscopy before closure. Hardware outside this zone causes pain, mechanical catching and loss of rotation.
If the head has more than three articular fragments, poor bone quality, or cannot take stable fixation, abandon ORIF and convert to a modular metal arthroplasty — the cardinal error of arthroplasty is an over-sized, overstuffed head that erodes the capitellum.
The five danger structures of the lateral elbow — know the location and the protection for each:
Enters the supinator 10 to 20mm distal to the radial head and lies anterior to the radial neck in supination. Protect it by maintaining full forearm supination throughout, staying proximal to 2cm distal to the head, and avoiding retractors in the supinator.
Runs anterior to the lateral epicondyle and radiocapitellar joint, about 20 to 30mm anterior to the skin incision, dividing into the PIN and superficial sensory branch at the radiocapitellar joint. Protect it by staying within the Kocher interval and avoiding anterior dissection beyond the capsular incision.
Runs from the lateral epicondyle to the supinator crest and is the primary restraint to posterolateral rotatory instability. Identify and preserve it during the Kocher interval, or tag and repair it at closure.
Encircles the radial neck from the anterior to the posterior margin of the sigmoid notch and stabilises the proximal radioulnar joint. Minimise dissection around the neck, avoid circumferential stripping, and repair the ligament if it was incised for exposure.
The anterior bundle runs from the medial epicondyle to the sublime tubercle of the coronoid and is the primary valgus restraint. Assess it with valgus stress under fluoroscopy and repair it through a separate medial approach if the joint opens greater than 3mm.
Aftercare & Complications
Rehabilitation — early active motion is the principle; the elbow stiffens quickly. | Phase | Timing | Splint / motion | Therapy focus | |-------|--------|-----------------|---------------| | 1 | 0 to 2 days | Posterior splint at 90° for comfort only | Remove splint for gentle active ROM 3 to 4 times daily | | 2 | Week 1 to 2 | Splint off for exercise | Aggressive active elbow ROM; begin forearm rotation | | 3 | Week 4 to 6 | — | Progressive strengthening; active motion only | | 4 | Week 6 onward | — | Continue ROM; avoid passive stretching for the first 6 weeks | Avoid passive stretching for the first 6 weeks — it inflames the joint and increases heterotopic ossification risk. Give indomethacin 25mg three times daily for 6 weeks to patients at high risk of heterotopic ossification (associated head injury, burns, extensive dissection, prior HO). Complications
- Recognition
- Post-op weakness of thumb and finger extension (EPL, EDC, EIP, EPB, APL) with preserved wrist extension (ECRL/ECRB branch proximal to PIN) and no sensory loss; EMG at 3 to 4 weeks confirms neuropraxia vs axonotmesis
- Prevention
- Full forearm supination throughout; stay proximal to 2cm distal to the head; no retractors in the supinator or anterior to the head
- Management
- Usually neuropraxia — observe 3 to 6 months with therapy; repeat EMG at 3 months; primary repair if transected intra-op; explore at 4 to 6 months if no recovery
- Recognition
- Progressive loss of forearm rotation with a firm endpoint; radiographs show bone bridging proximal radius to ulna; CT confirms extent
- Prevention
- Minimise periosteal stripping of radius and ulna; gentle handling of the interosseous membrane; early ROM; maintain the ECU-anconeus plane
- Management
- Synostosis takedown after maturation (6 to 12 months) with post-op indomethacin for 6 weeks and 700cGy radiation within 72 hours
- Recognition
- Progressive stiffness weeks to months post-op with pain on ROM and palpable hard masses; radiographs show periarticular calcification; alkaline phosphatase is raised during active formation
- Prevention
- Gentle soft-tissue handling; minimal periosteal stripping; early ROM within 48 hours; meticulous haemostasis; indomethacin or single-dose 700cGy radiation within 72 hours if high risk
- Management
- Observe if asymptomatic; excise after maturation (12 to 18 months, no radiographic progression for 3 to 6 months and normal alkaline phosphatase); post-excision indomethacin and radiation
- Recognition
- Pain and mechanical catching with forearm rotation, point tenderness over hardware, loss of terminal rotation; fluoroscopy during rotation shows PRUJ impingement
- Prevention
- Bury screws beneath cartilage (countersink); low-profile plates within the 110° safe zone; intra-op rotation testing with fluoroscopy before closure
- Management
- Hardware removal once union confirmed (minimum 6 to 12 months); warn that stiffness may not fully resolve after removal
- Recognition
- Recurrent mechanical symptoms, loss of ROM; radiographs show displacement, hardware loosening or breakage, articular step-off on CT
- Prevention
- Adequate fragment size (greater than 25% of head); stable construct (plate for comminution, minimum two screws); protected active motion only; bone graft for comminution or bone loss
- Management
- Revision ORIF if early (less than 6 weeks) and reconstructable; excision if late with a small fragment and a stable elbow; arthroplasty if late, unstable, or Essex-Lopresti
- Recognition
- Loss of flexion-extension (normal 0 to 145°) or forearm rotation (normal 75° pronation, 85° supination) with a firm capsular endpoint; radiographs may show HO
- Prevention
- Anatomic reduction (less than 1mm step-off); stable fixation allowing early motion; brief splinting (48 to 72 hours maximum); active ROM from week 1 to 2; no passive stretching for 6 weeks
- Management
- Continue active ROM and stretching for at least 6 months; static progressive splinting after 3 months if plateau; arthroscopic or open capsular release and HO excision after 6 to 12 months if severe (functional arc less than 30 to 100°)
- Recognition
- Chronic pain with use, mechanical catching, crepitus, loss of motion; radiographs show joint-space narrowing, osteophytes, subchondral sclerosis, articular collapse
- Prevention
- Anatomic articular reduction (less than 1mm step-off); stable fixation; early motion; screws buried beneath cartilage; address all instability
- Management
- Non-operative first (NSAIDs, activity modification, therapy, steroid injection); isolated radial head arthritis in a stable elbow — excision; arthritis with instability — arthroplasty; pan-elbow arthritis in a low-demand patient — total elbow arthroplasty
Viva & Exam Focus
My Surgeon Makes ArthroplastyMASON — the four types and their management
RaCe CoLTERRIBLE TRIAD — the three components
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 32-year-old presents with a terrible triad injury. Walk me through your management. What is the terrible triad and how do you manage it?”
“You have fixed a Mason type 2 radial head fracture with a plate. Post-operatively the patient complains of pain with forearm rotation and mechanical catching. What is your differential and management?”
“A patient presents with a radial head fracture and wrist pain. On examination the DRUJ is unstable. What injury pattern are you concerned about and how does this change your management?”
Indications
- Mason type 2: displaced greater than 2mm, greater than 30% surface, reconstructable
- Mason type 3: comminuted but reconstructable with stable fixation
- Block to forearm rotation — absolute indication regardless of displacement
- Associated instability (terrible triad, Essex-Lopresti) — radial head preservation mandatory
Key anatomy
- PIN enters the supinator 10 to 20mm distal to the head; anterior in supination
- Safe zone: 110° anterolateral arc with no PRUJ articulation; identify with arm at side, forearm supinated
- LUCL: lateral epicondyle to supinator crest — primary posterolateral restraint
- Kocher interval: ECU (anterior) and anconeus (posterior), both PIN-supplied — true internervous plane
Critical steps
- Stability assessment under anaesthesia: valgus stress (MCL), posterolateral rotatory test (LUCL)
- Full forearm supination throughout the approach — protect the PIN
- Anatomic reduction to less than 1mm step-off — prevents post-traumatic arthritis
- Safe-zone identification: mark the lateral radial head under fluoroscopy (forearm supinated, arm at side)
- Rotation testing with fluoroscopy before closure — confirm no hardware impingement
Danger structures
- PIN: anterior in supination; injured if the forearm pronates or dissection goes greater than 2cm distal to the head
- Radial nerve proper: about 20 to 30mm anterior to the incision — avoid anterior dissection
- LUCL: identify and preserve or tag for repair
- Annular ligament: repair if incised — PRUJ stability
- MCL: assess with valgus stress, repair if it opens greater than 3mm
Technique pearls
- Supination is the key to PIN protection — most injuries follow inadvertent pronation
- Safe zone critical: hardware outside it causes PRUJ impingement and pain
- Headless screws for simple patterns — bury beneath cartilage
- Plate for comminution — low-profile and within the safe zone
- Terrible triad sequence: coronoid, then radial head, then LUCL, then assess MCL
Complications
- PIN injury (1 to 5%): usually neuropraxia; observe 3 to 6 months
- Stiffness (10 to 30%): early ROM essential; splint maximum 48 to 72 hours
- HO (5 to 15%): indomethacin 25mg TDS for 6 weeks if high risk
- Hardware prominence (10 to 20%): safe-zone placement and rotation testing prevent it
- Post-traumatic arthritis (15 to 30%): anatomic reduction to less than 1mm is critical
Post-op protocol
- Splint at 90° flexion for 48 to 72 hours only — comfort, not stability
- Day 1 to 2: remove splint for active ROM 3 to 4 times daily
- Week 2: aggressive active ROM including forearm rotation
- Week 4 to 6: progressive strengthening
- Avoid passive stretching for the first 6 weeks — increases HO risk
- Indomethacin 25mg TDS for 6 weeks if high HO risk (head injury, burns)
Exam tips
- Know Mason cold: type 1 non-op, type 2 ORIF if reconstructable, type 3 ORIF vs arthroplasty, type 4 with dislocation
- Terrible triad: address all three components (radial head + coronoid + ligaments)
- Essex-Lopresti: radial head excision contraindicated — causes proximal migration
- Safe zone concept and how to identify it: 110° anterolateral arc, mark under fluoroscopy
- Early ROM is critical to prevent stiffness — the biggest complication after elbow trauma
Background & Evidence
Epidemiology. Radial head fractures are among the most common fractures about the elbow, classically resulting from a fall onto an outstretched hand with the elbow extended and the forearm pronated; they peak in young and middle-aged adults and show a female predominance in many series (Kaas, 2010). Mason classification (1954) — the most widely used system and the basis of the management decision:
- Description
- Undisplaced or minimally displaced (less than 2mm), no block to rotation
- Typical management
- Non-operative — splint for comfort, early ROM, NSAIDs
- Description
- Displaced greater than 2mm, usually greater than 30% of the articular surface, possible mechanical block
- Typical management
- ORIF if reconstructable; excision only if a small fragment in a stable elbow
- Description
- Comminuted with multiple fragments
- Typical management
- ORIF if reconstructable; arthroplasty if not; excision only in a stable elbow
- Description
- Radial head fracture with associated elbow dislocation
- Typical management
- Address every component of instability (radial head, coronoid, ligaments)
Hotchkiss modification (1997) refines the surgical decision: type 1 non-displaced or minimally displaced; type 2 displaced greater than 2mm but reconstructable; type 3A comminuted but reconstructable; type 3B comminuted and not reconstructable; type 4 associated with elbow dislocation. The terrible triad — pathoanatomy. A posterolateral rotatory force with axial load causes sequential failure: Stage 1 LUCL disruption with posterolateral subluxation; Stage 2 coronoid fracture (usually the tip or anteromedial facet); Stage 3 radial head fracture; Stage 3B MCL rupture with complete dislocation. Management in sequence: coronoid fixation first (the foundation for valgus stability), then radial head ORIF or arthroplasty (lateral column), then LUCL repair (posterolateral stability), then MCL repair only if valgus instability persists. The Essex-Lopresti injury — longitudinal radioulnar dissociation. The three components are a radial head fracture, interosseous membrane disruption (the central band is the primary restraint to proximal migration), and DRUJ disruption. Clinical signs: a radial head fracture with wrist pain, DRUJ tenderness and instability, a positive DRUJ stress test (piano-key sign), and proximal radial migration on an AP forearm radiograph. The radial head MUST be preserved; excision is contraindicated. The DRUJ is assessed and repaired if unstable; interosseous membrane reconstruction is considered in the acute setting. Post-op splinting holds the forearm supinated with the wrist neutral. Key evidence. Ring, Quintero and Jupiter (2002) reviewed 56 intra-articular radial head fractures treated with ORIF: all 15 isolated non-comminuted type 2 fractures had a satisfactory result, but 13 of 14 type 3 fractures with more than three articular fragments had an unsatisfactory result — ORIF is best reserved for fractures with three or fewer fragments and minimal comminution. Ring, Jupiter and Zilberfarb (2002) showed that in the terrible triad every satisfactory result retained the radial head and all four patients managed with radial head resection redislocated — excision is contraindicated in the unstable elbow. Pugh et al. (2004) validated the sequenced protocol for the terrible triad (radial head fixation or replacement, coronoid fixation, lateral ligament repair, selective medial repair) with a mean Mayo Elbow Performance Score of 88 and concentric stability in 34 of 36 elbows. Doornberg et al. (2007) showed that a modular metal spacer reliably restores stability when the head is too comminuted for ORIF, the pitfall being an over-sized (overstuffed) head. Smith, Morrey and Steinmann (2007) described low-profile buried-screw fixation that minimises hardware in the constrained PRUJ region.
References
Open reduction and internal fixation of fractures of the radial head
- Retrospective series of 56 intra-articular radial head fractures treated with ORIF, mean 48-month follow-up (30 Mason type 2, 26 Mason type 3)
- All 15 isolated non-comminuted type 2 fractures had a satisfactory result; 13 of 14 type 3 fractures with more than three articular fragments had an unsatisfactory result
- Associated fracture-dislocation of elbow or forearm compromised forearm rotation even in less comminuted patterns
Standard surgical protocol to treat elbow dislocations with radial head and coronoid fractures
- 36 consecutive terrible triad injuries treated with a sequenced protocol: radial head fixation or replacement, coronoid fixation where possible, lateral ligament repair, with selective MCL repair and hinged external fixation
- Mean Mayo Elbow Performance Score 88 (15 excellent, 13 good); concentric stability restored in 34 of 36 elbows; mean flexion-extension arc 112 degrees and forearm rotation 136 degrees
- Eight reoperations (two synostoses, one recurrent instability, four hardware removal/release, one infection)
Posterior dislocation of the elbow with fractures of the radial head and coronoid
- 11 terrible triad elbows, minimum 2-year follow-up; 7 of 11 had an unsatisfactory result and 7 of 10 retained elbows developed advanced ulnohumeral arthrosis
- All four patients managed with radial head resection redislocated; every satisfactory result had retained the radial head
- Coronoid fractures were unrepaired and lateral collateral ligament repaired in only three patients - underscoring why incomplete reconstruction fails
Radial head arthroplasty with a modular metal spacer to treat acute traumatic elbow instability
- 27 patients with comminuted radial head fractures and traumatic instability treated with a modular metal head; stability restored in all 27 elbows
- Mean flexion-extension to 131 degrees (20-degree contracture), pronation 73 degrees, supination 57 degrees; 22 of 27 good or excellent on the Mayo index at mean 40 months
- Stem lucency around an intentionally loose stem and minor capitellar changes were common but clinically inconsequential; overstuffing with an oversized head caused problems
Low profile fixation of radial head and neck fractures: surgical technique and clinical experience
- Describes obliquely oriented buried screws driven from the radial head into the shaft to avoid distal soft-tissue dissection and hardware adjacent to the annular ligament and lateral ligaments
- Technique is most suited to axially stable fractures with no or minimal neck comminution
- Minimises hardware in the constrained PRUJ region, addressing the forearm-rotation loss associated with prominent plates
Further reading 1. Mason ML. Some observations on fractures of the head of the radius with a review of one hundred cases. Br J Surg. 1954;42(172):123-132. doi:10.1002/bjs.18004217203 2. Hotchkiss RN. Displaced fractures of the radial head: internal fixation or excision? J Am Acad Orthop Surg. 1997;5(1):1-10. doi:10.5435/00124635-199701000-00001 3. Mathew PK, Athwal GS, King GJ. Terrible triad injury of the elbow: current concepts. J Am Acad Orthop Surg. 2009;17(3):137-151. doi:10.5435/00124635-200903000-00002 4. Guitton TG, Ring D, Science of Variation Group. Interobserver reliability of radial head fracture classification: two-dimensional compared with three-dimensional CT. J Bone Joint Surg Am. 2011;93(21):2015-2021. doi:10.2106/JBJS.J.00711 5. Grewal R, MacDermid JC, King GJ. Open reduction internal fixation versus excision of radial head fractures: a systematic review. J Hand Surg Am. 2009;34(10):1861-1869. doi:10.1016/j.jhsa.2009.09.007 6. Struijs PA, Smit G, Steller EP. Radial head fractures: effectiveness of conservative treatment versus surgical intervention. A systematic review. Arch Orthop Trauma Surg. 2007;127(2):125-130. doi:10.1007/s00402-006-0240-9 7. Kaas L, van Riet RP, Vroemen JP, Eygendaal D. The epidemiology of radial head fractures. J Shoulder Elbow Surg. 2010;19(4):520-523. doi:10.1016/j.jse.2009.10.015