Posterior Cruciate Ligament · Dashboard injury · Grade III laxity
- Dashboard injury: a posteriorly directed force on the proximal tibia of a flexed knee is the classic mechanism (knee striking the dashboard in a motor-vehicle collision).
- The PCL is the thickest and strongest intra-articular ligament of the knee, providing roughly 95% of the restraint to posterior tibial translation; it is tightest (and the dominant posterior restraint) at 60–90° of flexion.
- Posterior drawer test and the sag sign are diagnostic; the medial tibial step-off is lost compared with the other side.
- Grade III (greater than 10mm translation) is the principal surgical indication — the tibia sits posterior to the medial femoral condyle.
- A Grade III injury mandates a deliberate search for posterolateral corner injury and a (spontaneously reduced) knee dislocation — a combined PCL plus posterolateral corner reconstruction done in isolation will fail.
- Transtibial or tibial inlay are the two tibial-side techniques; the transtibial 'killer turn' can abrade the graft, and Achilles tendon allograft is the common graft choice.
When & Why
Indication. Surgical reconstruction is reserved for Grade III (greater than 10mm posterior translation) isolated PCL injuries, combined multiligament injuries — especially PCL plus posterolateral corner (PLC), symptomatic Grade II injuries that have failed structured non-operative care, high-demand athletes, and bony tibial PCL avulsions (which are fixed by open or arthroscopic fixation rather than reconstructed when the fragment is adequate). Isolated Grade I–II injuries, and low-demand patients without associated injuries, are managed non-operatively. Mechanism. Three patterns produce a PCL injury: - Dashboard injury — the classic mechanism. A flexed knee takes a posteriorly directed force on the proximal tibia, as when the knee strikes a dashboard in a motor-vehicle collision.
- Hyperflexion — a non-contact fall onto a flexed knee with the foot plantarflexed, a common sporting mechanism.
- Hyperextension — a hyperextension force can injure both cruciates and, when severe, threatens the popliteal neurovascular bundle. PCL injuries are frequently part of a multiligament pattern, especially with the posterolateral corner. Any high-grade (Grade III) PCL injury mandates a deliberate search for associated injury and for a knee dislocation that has spontaneously reduced. The one decision that matters. Every reconstruction begins by confirming the grade and excluding associated injury; the operative choice then turns on what is injured and how it is fixed:
Isolated Grade I–II. Quadriceps strengthening is the key (it reduces the posterior tibial sag). Add a brace, activity modification and range-of-motion work. Many isolated PCL injuries function well this way.
Greater than 10mm posterior translation in isolation. Achilles tendon allograft via a transtibial or tibial inlay technique, single- or double-bundle.
Both structures must be reconstructed together — reconstructing either in isolation overloads the single repair and fails. The PLC is usually reconstructed first.
Graft choice. Achilles tendon allograft is the most common — a large cross-section, strong, no donor-site morbidity, and useful bulk in multiligament knees. Alternatives are the quadriceps tendon, hamstring (semitendinosus with or without gracilis) autograft, and bone-patellar tendon-bone. Consent specifically for residual posterior laxity (the most common functional shortfall), loss of flexion or stiffness after prolonged bracing, the small but serious risk of popliteal neurovascular injury, graft failure or stretching, deep vein thrombosis, anterior knee pain, and progression of post-traumatic osteoarthritis (which reconstruction does not reliably prevent). Setup. Supine with a thigh tourniquet; a lateral post or leg holder allows a figure-of-four position to reach the posteromedial knee. Standard anterolateral and anteromedial arthroscopy portals with an accessory posteromedial portal. Prone positioning is used when a formal open tibial inlay is planned.
The Operation
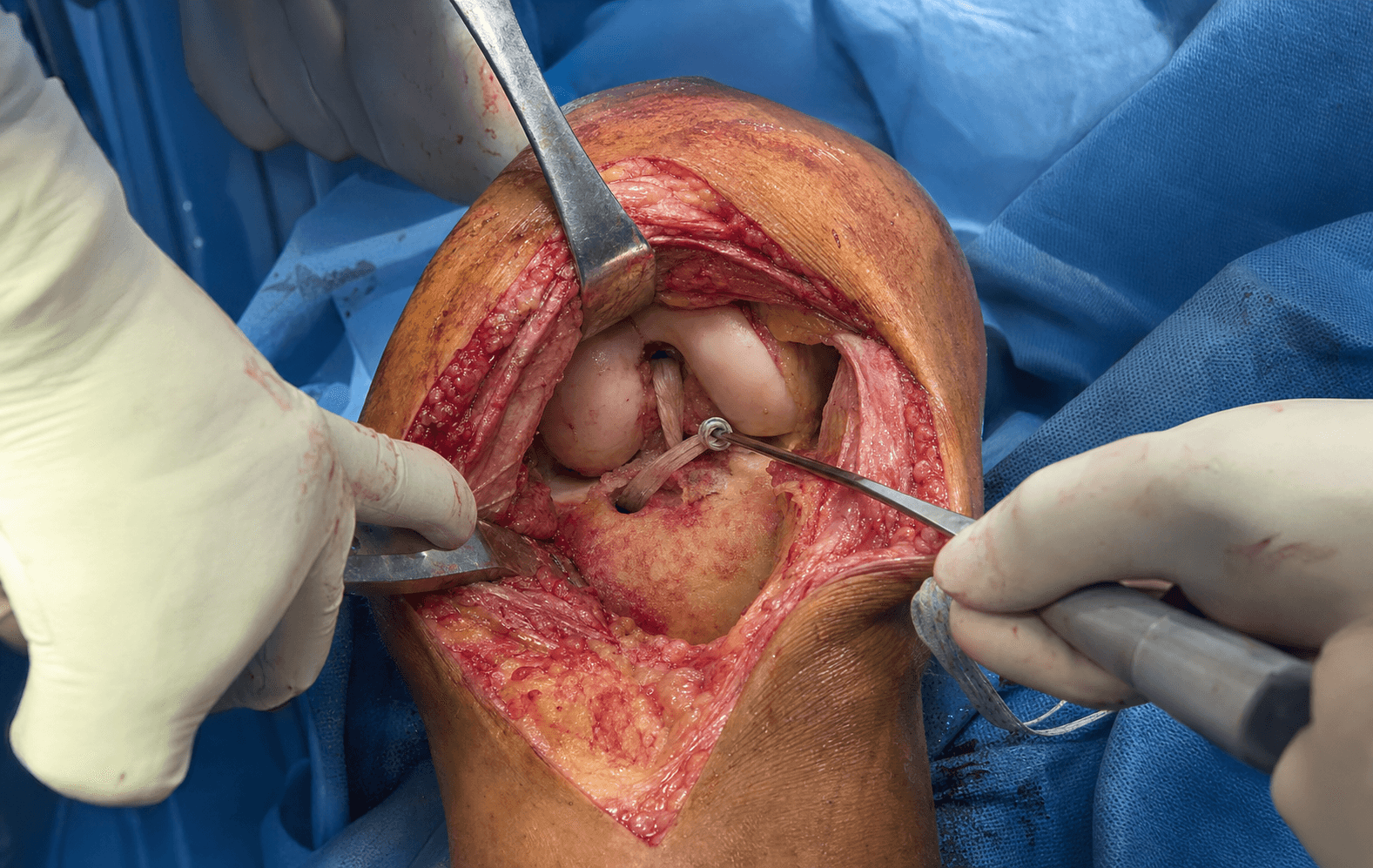
The goal: reconstruct the dominant anterolateral bundle (and, in double-bundle cases, the posteromedial bundle) across anatomic footprints, while protecting the popliteal neurovascular bundle that lies directly behind the tibial insertion. The exposure — the posteromedial interval behind the PCL, or the open posteromedial approach for an inlay — is laid out in full below and is the heart of the operation.
Operative sequence
- Supine, thigh tourniquet, lateral post or leg holder for figure-of-four access to the posteromedial knee.
- Establish anterolateral and anteromedial portals plus an accessory posteromedial portal to visualise the PCL tibial footprint directly.
- If a formal open tibial inlay is planned, position the patient prone.
- Confirm the PCL tear, grade the laxity, inspect the meniscofemoral ligaments (Humphrey anterior, Wrisberg posterior) and assess the articular surfaces.
- Address meniscal and chondral injury; in a combined case, plan the PLC/ACL reconstruction — the PLC is reconstructed first.
- Prepare an Achilles tendon allograft (typically 10–11 mm with a bone block); alternatives are quadriceps tendon, hamstring (semitendinosus with or without gracilis) or bone-patellar tendon-bone.
- From the anteromedial portal, elevate the posteromedial capsule off the posterior tibia with a curved elevator, working the interval between the medial femoral condyle and the PCL.
- Create a posteromedial capsular window and place a posterior retractor (a curved curette or spoon) to shield the neurovascular bundle — the single most important safety step in the transtibial technique.
- The PCL tibial footprint (the fovea) sits on the flat posterior tibial surface about 1–1.5 cm below the joint line.
- For the open tibial inlay, a formal posteromedial approach (medial gastrocnemius retracted laterally) exposes the flat posterior tibia directly; the popliteus and neurovascular bundle are protected behind the lateral gastrocnemius.
- Through the anteromedial or accessory posteromedial portal, drill the femoral tunnel in the anatomic PCL footprint on the lateral wall of the medial femoral condyle.
- The anterolateral-bundle centre sits anterior and proximal within the footprint; an over-anterior tunnel compromises graft function.
- Single-bundle reconstructs the dominant anterolateral bundle; double-bundle adds a separate posteromedial-bundle tunnel.
- Transtibial (tunnel) technique — the most common. Pass a guide pin from the anteromedial tibia to the PCL fovea with a curved PCL tibial guide; the posterior retractor or curette protects the vessels; the final reaming passes are done by hand under arthroscopic and fluoroscopic control. The acute angle where the graft turns out of the back of the tunnel is the 'killer turn', which can abrade and thin the graft over repeated flexion–extension cycles and contribute to gradual stretching and failure.
- Tibial inlay technique — through the open posteromedial approach, cut a flat trough on the posterior tibial surface and inset the graft bone block, fixing it with a screw and spiked washer or suture anchors. This eliminates the killer turn and gives robust posterior fixation, at the cost of the posterior approach; it is favoured by many for revision and multiligament cases.
- Pass the graft from the tibia (through the tunnel for transtibial, or up from the inlay) into the femoral tunnel, smoothing the tunnel edges to reduce abrasion.
- For a double-bundle reconstruction, pass each bundle into its own femoral socket.
- Tension and fix the graft at about 70–90° of knee flexion while an anterior drawer force is applied to the tibia — this reduces the posterior sag and restores the normal medial tibial step-off.
- Femoral fixation with an interference screw; tibial fixation with an interference screw plus a supplementary cortical button, post or staple.
- Cycle the knee through flexion–extension to confirm isometry and a stable step-off before final fixation.
- Confirm restoration of the medial tibial step-off and a negative posterior sag; recheck the neurovascular status of the limb.
- Close the portals or the posteromedial approach in layers and apply a hinged knee brace locked in extension.
The popliteal artery and vein lie directly posterior to the proximal tibia, about 1–2 cm behind the PCL tibial insertion. During transtibial tunnel drilling the guide pin and reamer must be protected — use a curved tibial guide, a posterior retractor or curette, fluoroscopic or arthroscopic control, and ream the final passes by hand. The same vessels are at risk during the posterior inlay dissection. If a vascular injury is recognised: direct pressure, call for vascular help, and repair primarily where possible. The common peroneal nerve is additionally at risk when a posterolateral corner reconstruction is performed and must be identified and protected throughout.
Tension and fix the graft at 70–90° of flexion while applying an anterior drawer to the tibia. The endpoint is restoration of the normal medial tibial step-off (the tibia 1 cm anterior to the medial femoral condyle) and abolition of the posterior sag — confirm it before final fixation, then cycle the knee to check isometry.
In a combined PCL plus posterolateral corner injury, reconstruct the PLC first, then the PCL. Posterolateral instability complicates PCL tunnel placement and graft tensioning; stabilising the corner first gives a stable platform. Reconstructing either structure in isolation will fail, because the unopposed forces overload the single repair.
Aftercare & Complications
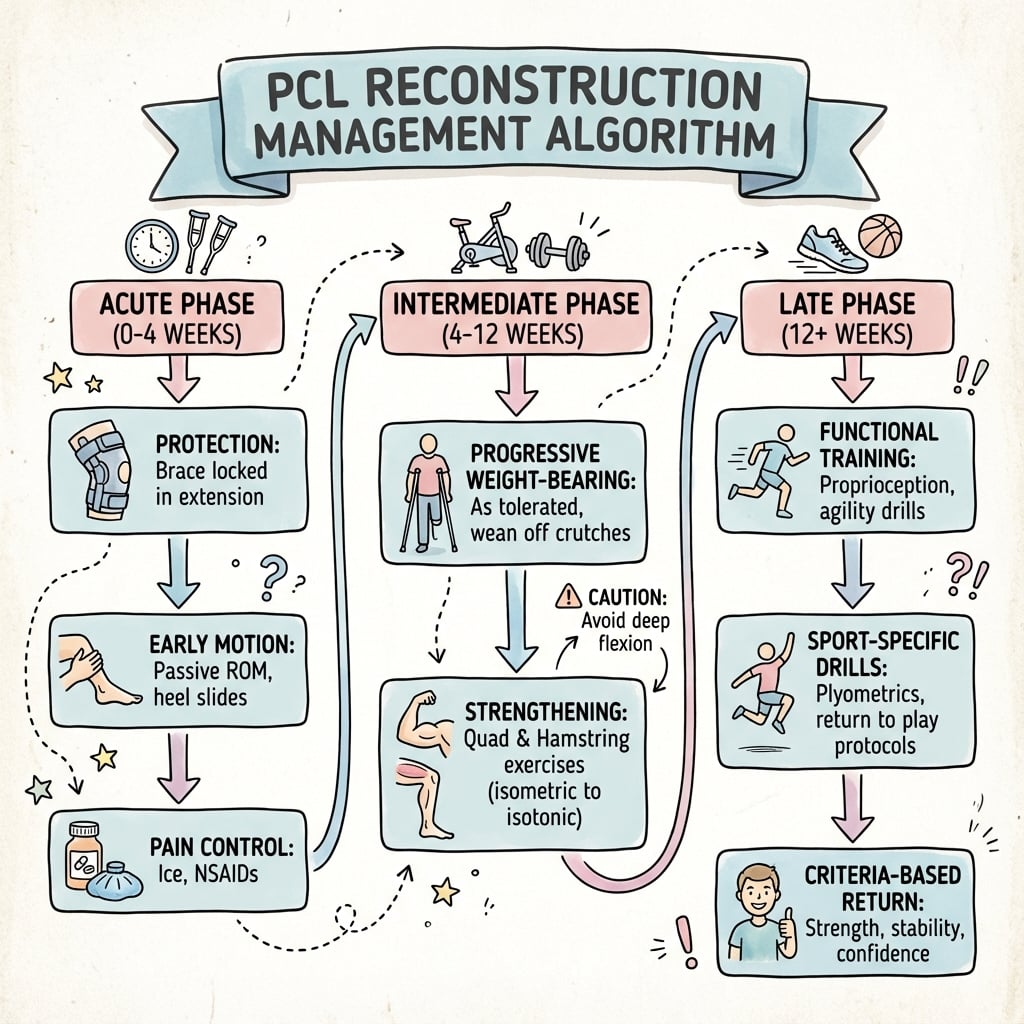
Rehabilitation | Phase | Timing | Immobilisation / brace | Therapy focus | |-------|--------|------------------------|---------------| | 1 | 0–2 weeks | Hinged brace locked in extension | Quadriceps sets, straight-leg raises, wound healing | | 2 | 2–6 weeks | Brace; flexion limited to 60–70° | Progressive flexion within the limit; patellar mobilisation | | 3 | 6–12 weeks | Brace unlocked, then weaned | Full flexion by 12 weeks; closed-chain quadriceps work | | 4 | 3–6 months | Functional brace for high demand | Hamstring strengthening from 8–10 weeks (delayed to protect the graft); running from 4–6 months | | 5 | 6–9+ months | None | Pivoting and cutting from 9–12 months; return to sport when strength is at least 90% of the other side | The early restriction of flexion (to 60–70° for the first six weeks) protects the graft, which is under maximal tension in flexion; external-rotation and varus loading are avoided for three months when a PLC reconstruction has also been performed. Quadriceps strengthening is critical throughout, because a strong quadriceps actively counters the posterior tibial sag. Complications
- Recognition / risk
- Bleeding in the field; distal ischaemia; expanding calf haematoma
- Prevention
- Posterior retractor/curette; curved guide; hand-ream final passes; fluoro control
- Management
- Direct pressure, vascular help, primary repair; check distal perfusion
- Recognition / risk
- Foot drop; dorsiflexion weakness (PLC reconstruction)
- Prevention
- Identify and protect the nerve throughout the posterolateral exposure
- Management
- Neurolysis or exploration if no recovery; ankle-foot orthosis
- Recognition / risk
- Persistent posterior drawer / sag — the most common functional shortfall
- Prevention
- Anatomic tunnels; tension at 70–90° with anterior drawer; avoid killer-turn abrasion
- Management
- Quadriceps rehab and brace; revision if symptomatic and grade III
- Recognition / risk
- Flexion contracture after prolonged extension bracing or combined reconstruction
- Prevention
- Early motion within restrictions; avoid over-bracing
- Management
- Gentle passive flexion; manipulation or arthrolysis if refractory
- Recognition / risk
- Recurrent instability months to years out; attenuated high-T2 graft on MRI
- Prevention
- Avoid killer turn (inlay for revision); graft maturation before pivoting (18–24 months)
- Management
- Revision reconstruction (tibial inlay, Achilles allograft preferred)
- Recognition / risk
- Infection, DVT, anterior knee pain, fixation failure
- Prevention
- Aseptic technique, prophylaxis, secure fixation
- Management
- Standard management; revision fixation if hardware fails
Outcomes. Reconstruction reliably improves objective stability and function for Grade III and multiligament injuries, but residual laxity is common and reconstruction has not been shown to reliably prevent later osteoarthritis (see the Shelbourne natural-history comparison in the evidence base). Isolated low-grade injuries frequently do well with quadriceps-focused rehabilitation.
Viva & Exam Focus
DASHPCL Injury Features
Hook:DASH = Dashboard, Anterior sag, Step-off lost, Higher grades need surgery!
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old man has posterior tibial sag and a positive posterior drawer with greater than 10mm translation. How do you manage him?”
“A 28-year-old motorcyclist is referred 6 weeks after a dashboard-type knee injury. He has a Grade III posterior drawer (greater than 10mm), a positive sag, and the dial test shows 15° increased external rotation at both 30° and 90°, with varus opening at 30°. MRI confirms complete tears of the PCL, LCL and popliteus. He is a firefighter who wants to return to sport and work. How do you counsel him and what is your surgical plan?”
“A 32-year-old former college rugby player presents 3 years after a transtibial hamstring-autograft PCL reconstruction for an isolated Grade III injury. He did well initially and returned to rugby at 12 months, but over the past 12-18 months has developed progressive posterior instability with 'giving way' on decelerating or descending stairs, plus medial and patellofemoral pain. He has stopped rugby. Examination shows a Grade III posterior drawer (10-12mm), positive sag, mild quadriceps atrophy and patellofemoral crepitus; dial test is negative; range of motion is full. Radiographs show mild patellofemoral and medial compartment degenerative change; MRI shows an attenuated, high-T2 graft with posterior tibial translation and early medial and patellar cartilage damage. What went wrong and how do you manage him?”
Diagnosis
- Posterior drawer test positive
- Sag sign (tibia drops posteriorly)
- Quadriceps active test
- Step-off lost vs contralateral
Grading
- Grade I: 1-5mm (anterior to condyle)
- Grade II: 6-10mm (flush)
- Grade III: greater than 10mm (posterior)
Surgical Indications
- Grade III
- Multiligament injury (PCL + PLC)
- Symptomatic Grade II failing conservative care
- Bony tibial avulsion (fix, not reconstruct)
Technique
- Transtibial (killer turn risk)
- Tibial inlay (posterior approach)
- Single or double bundle
- Achilles allograft common
Background & Evidence
Anatomy and biomechanics. The posterior cruciate ligament is the primary restraint to posterior tibial translation, contributing roughly 95% of the restraining force, and is the thickest and strongest intra-articular ligament of the knee — its cross-sectional area exceeds that of the ACL, with a reported ultimate tensile load around 1600–2000 N for the intact ligament. It has two functional bundles: the larger anterolateral (AL) bundle is tightest in flexion and is the dominant posterior restraint at 70–90°, while the smaller posteromedial (PM) bundle is tightest in extension; the bundles are named by their femoral origin and tibial insertion. The femoral origin is a broad fan-shaped footprint on the lateral wall of the medial femoral condyle (AL anterior and proximal, PM posterior and distal). The tibial insertion is the posterior tibial fovea, about 1–1.5 cm below the joint line and immediately anterior to the popliteal vessels. The meniscofemoral ligaments — Humphrey (anterior) and Wrisberg (posterior) — run alongside the PCL, provide secondary posterior restraint, and can be mistaken for PCL fibres at arthroscopy. Clinical assessment. Diagnosis rests on: - Posterior drawer test — at 90° flexion, stabilise the foot and push the tibia posteriorly; positive when there is increased laxity.
- Sag sign (Godfrey's test) — with 90° hip and knee flexion, the tibia sags posteriorly compared with the other side.
- Quadriceps active test — at 90° flexion with the foot fixed, quadriceps contraction pulls a PCL-deficient tibia anteriorly from its posteriorly subluxed position.
- Dial test — to assess the posterolateral corner; increased external rotation at 30° only suggests isolated PLC injury, while asymmetry at both 30° and 90° indicates combined PCL plus PLC injury. Grading of posterior translation (the posterior drawer) determines management:
- Translation
- 1–5mm
- Tibia vs medial femoral condyle
- Still anterior to the condyle
- Typical management
- Non-operative — quadriceps-led rehabilitation
- Translation
- 6–10mm
- Tibia vs medial femoral condyle
- Flush with the condyle
- Typical management
- Non-operative first; reconstruction if symptomatic and failing
- Translation
- greater than 10mm
- Tibia vs medial femoral condyle
- Posterior to the condyle
- Typical management
- Surgical reconstruction
Single versus double bundle. Single-bundle reconstruction recreates the dominant anterolateral bundle and is biomechanically sound. Double-bundle reconstruction additionally recreates the posteromedial bundle and reduces residual laxity biomechanically, though randomised clinical data show comparable patient-reported outcomes (see the evidence base). Guidelines, registries and global practice. | Theme | Global consensus position | |-------|---------------------------| | Isolated Grade I–II | Non-operative, quadriceps-led rehabilitation is first-line across AAOS, BOA and European practice | | Grade III / multiligament | Reconstruction favoured; combined PCL plus posterolateral corner injury requires addressing both structures | | Bony tibial avulsion | Fixation (open or arthroscopic) preferred over reconstruction where the fragment is adequate | | Tunnel vs inlay | No technique proven superior in pooled data; inlay favoured for revision and to avoid the killer turn | | Single vs double bundle | Double-bundle improves biomechanical laxity control; randomised clinical outcomes comparable | Practice variation is driven largely by graft availability — allograft is freely available in some health systems and restricted or costly in others, shifting graft choice toward autograft — and by surgeon experience with the posterior approach, rather than by national guideline differences.
References
A Comprehensive Meta-analysis of Clinical and Biomechanical Outcomes Comparing Double-Bundle and Single-Bundle Posterior Cruciate Ligament Reconstruction Techniques
- Pooled 15 biomechanical and 13 clinical comparative studies
- Double-bundle gave significantly less posterior tibial translation at both 30 and 90 degrees of flexion and less external rotation laxity at 90 degrees
- Double-bundle showed higher odds of normal/near-normal objective IKDC grades and higher subjective IKDC scores
- No difference in Lysholm, Tegner, or major complication rate between techniques
Single-Bundle versus Double-Bundle Posterior Cruciate Ligament Reconstruction: A Meta-Analysis of Randomized Controlled Trials
- Meta-analysis restricted to 4 randomized controlled trials
- No significant difference in Lysholm, Tegner, side-to-side laxity, or IKDC objective grade at final follow-up
- Both single- and double-bundle restored knee stability and function
- Authors conclude higher-quality RCTs are still needed to settle superiority
Posterior Cruciate Ligament Reconstruction With Transtibial or Tibial Inlay Techniques: A Meta-analysis of Biomechanical and Clinical Outcomes
- Pooled 5 biomechanical and 5 clinical studies comparing transtibial versus tibial inlay
- No significant difference in posterior tibial translation at 90 degrees or after cyclic loading
- No difference in Lysholm, Tegner, side-to-side difference, or posterior drawer at final follow-up
- Transtibial tended toward fewer perioperative complications than tibial inlay
The Multiple-Ligament Injured Knee: Evaluation, Treatment, and Results
- Systematic framework for the dislocated/multiligament knee, emphasising mandatory vascular assessment
- Arthroscopically assisted combined ACL/PCL reconstruction is reproducible and improves objective stability
- Combined PCL plus posterolateral corner injury is best treated with reconstruction, not isolated repair alone
- Strong allograft (Achilles, BPTB) preferred for these large grafts with no donor-site morbidity
Optimal Management of Posterior Cruciate Ligament Injuries: Current Perspectives
- Compared a 14.3-year natural-history cohort of isolated PCL tears against operative and nonoperative series
- Subjective and objective outcomes of nonoperative management compared favourably with reconstruction
- Osteoarthritis was reported across both groups (17-88% nonoperative, 13-63% operative)
- Reducing posterior laxity alone did not reliably prevent later osteoarthritis