Subaxial C3–C7 access for laminoplasty, laminectomy and lateral-mass instrumentation, with vertebral-artery and C5-root protection
- The posterior approach gives comprehensive access to the subaxial spine (C3–C7) for decompression (laminoplasty, laminectomy) and instrumentation (lateral mass screws C3–C6, pedicle screws C7, C2 pars/pedicle screws) in multilevel stenosis, OPLL and subaxial trauma.
- The vertebral artery ascends through the transverse foramina (C6 up to C2) anterior to the lateral mass; in cadaveric study neither the Magerl nor the Roy-Camille trajectory threatened it (Heller 1991), and large clinical series report VA injury well under 1 percent (0 percent in Heller's 654-screw series). It is endangered chiefly by excessive anterior screw depth or an anterolateral entry.
- Magerl lateral mass screw: entry 1 mm medial to the lateral mass centre, trajectory 25 degrees lateral and 25–45 degrees cephalad, about 14 mm bicortical, aimed away from the foramen. Roy-Camille is more straight-lateral and slightly cephalad; in cadaveric study neither breached the VA (Heller 1991).
- C5 nerve root palsy is the characteristic neurological complication — pooled incidence about 4.6 percent (range 4.6–11 percent), with no significant difference between laminoplasty and anterior decompression and fusion (Sakaura 2003). It presents 1–7 days postoperatively as deltoid and biceps weakness with preserved hand function; most recover but a minority remain weak.
- Laminoplasty preserves the posterior tension band and reduces the kyphosis seen after laminectomy without fusion (post-laminoplasty kyphosis about 10 percent — Ratliff and Cooper 2003). Posterior decompression is preferred for high-canal-occupancy OPLL, where anterior dural manipulation is hazardous.
- Axial neck and shoulder pain affects about 60 percent after laminoplasty versus about 19 percent after anterior fusion (Hosono 1996); preserving the posterior extensor complex (start dissection at C3 to spare the C2 semispinalis cervicis insertion, protect facet capsules) is used to reduce this burden. C7 is the most reliable subaxial pedicle-screw level.
When & Why
What it exposes. The posterior approach provides 360-degree access to the subaxial spine (C3–C7) for three purposes: decompression (laminectomy or laminoplasty for multilevel stenosis and OPLL), instrumentation (lateral mass screws C3–C6, pedicle screws C7, C2 pars/pedicle screws), and fusion (posterior wiring, facet fusion, instrumented posterolateral fusion). It is ideal for multilevel cervical stenosis (3 levels or more), ossification of the posterior longitudinal ligament (OPLL), and subaxial trauma needing posterior stabilisation. Indications - Degenerative — multilevel stenosis with myelopathy or radiculopathy resistant to conservative care; OPLL with high canal occupancy (posterior decompression avoids hazardous anterior dural manipulation); adjacent-segment disease after ACDF (extend posteriorly through unscarred tissue); posterior ligamentous injury (facet dislocation).
- Trauma — facet fracture-dislocation (posterior open reduction and lateral mass fixation); burst fracture with posterior ligamentous injury (360-degree fusion); unstable Hangman's fracture (C2 pars screws or C1–C3 fusion).
- Tumour or infection — metastatic epidural cord compression (laminectomy plus instrumented fusion for structural support); intradural tumour (laminectomy or laminoplasty for access).
- Deformity — post-laminectomy kyphosis (posterior instrumented fusion with lordotic contouring); ankylosing-spondylitis chin-on-chest deformity (posterior cervical osteotomy at C7–T1 plus instrumentation). Contraindications - Absolute — active infection (discitis or osteomyelitis): treat the infection first; unstable fracture needing anterior column reconstruction (isolated posterior fixation is insufficient for burst fractures with greater than 50 percent anterior comminution).
- Relative — severe osteoporosis (T-score less than minus 3.0, poor screw purchase); prior posterior cervical surgery (obliterated planes, higher dural-tear risk of 5–10 percent versus 1–2 percent primary); prior cervical radiation (fusion 70–80 percent irradiated versus 92–96 percent non-irradiated — Emery 1994); single-level disease (ACDF is preferred — shorter recovery, no posterior muscle dissection). Position and landmarks. Prone on chest rolls with the arms tucked and axillae free. Head fixation is a Mayfield 3-pin skull clamp (gold standard; one pin frontal above the eyebrow avoiding the supraorbital nerve, two pins occipital avoiding the transverse sinus) or a padded horseshoe. The neck is held neutral — flexion increases epidural venous bleeding and extension narrows the canal and risks cord injury. SSEP and MEP monitoring are used throughout (a sustained 50 percent drop in MEP amplitude signals cord compromise). Palpate the inion, the prominent C2 spinous process and the non-bifid C7 vertebra prominens for level confirmation. Laminoplasty versus laminectomy plus fusion. For multilevel stenosis the choice turns on cervical alignment and stability. Laminoplasty preserves the posterior tension band and motion; laminectomy plus fusion corrects deformity and stabilises instability.
- Laminoplasty
- Preserved — lamina hinged open, ligamentum flavum and interspinous ligaments kept on the hinge side
- Laminectomy plus fusion
- Violated — lamina removed, posterior ligaments disrupted
- Preferred
- Laminoplasty (preserves biomechanics, less instrumentation)
- Laminoplasty
- About 5–10 percent (tension band preserved — Ratliff and Cooper 2003)
- Laminectomy plus fusion
- High progressive kyphosis if laminectomy is done without fusion; fusion prevents or corrects it
- Preferred
- Laminoplasty or laminectomy with fusion (avoid laminectomy alone)
- Laminoplasty
- Common (about 60 percent, Hosono 1996, vs about 19 percent after anterior fusion); muscle-sparing exposure aims to reduce this
- Laminectomy plus fusion
- Also significant (posterior muscle dissection, facet violation, hardware prominence)
- Preferred
- Either — minimise by sparing the posterior extensor complex
- Laminoplasty
- About 4.6–11 percent (traction on the short C5 root — Sakaura 2003)
- Laminectomy plus fusion
- Also occurs; pooled review found no significant difference versus anterior decompression and fusion (Sakaura 2003)
- Preferred
- Comparable — mitigate with prophylactic C4/C5 foraminotomy (Katsumi 2012)
- Laminoplasty
- 50–60 percent of preoperative flexion–extension maintained (no fusion)
- Laminectomy plus fusion
- Zero motion at fused levels (rigid construct)
- Preferred
- Laminoplasty (motion preservation)
- Laminoplasty
- 10–15 percent at 10 years (motion preserved reduces adjacent stress)
- Laminectomy plus fusion
- 25–30 percent at 10 years (rigid fusion increases adjacent stress — Hilibrand 1999)
- Preferred
- Laminoplasty (about half the adjacent segment disease)
- Laminoplasty
- Not applicable — no fusion intended; lamina heals to the hinge-side graft over 6–12 months
- Laminectomy plus fusion
- High fusion rates with lateral mass screw fixation (Heller 1995)
- Preferred
- Laminectomy with fusion when stability is required
- Laminoplasty
- 120–180 minutes (hinge creation, graft placement, no instrumentation)
- Laminectomy plus fusion
- 180–240 minutes (laminectomy plus lateral mass screws plus fusion)
- Preferred
- Laminoplasty (30–40 minutes shorter)
- Laminoplasty
- 150–300 mL (lamina osteotomy, less muscle stripping)
- Laminectomy plus fusion
- 300–500 mL (lateral mass exposure, facet decortication, instrumentation)
- Preferred
- Laminoplasty (40–50 percent less)
- Laminoplasty
- Multilevel stenosis (3 levels or more) with maintained lordosis, OPLL with high canal occupancy, younger active patients
- Laminectomy plus fusion
- Stenosis with kyphosis greater than 10 degrees, instability (facet dislocation, ligamentous injury), older patients
- Preferred
- Depends on cervical alignment and instability
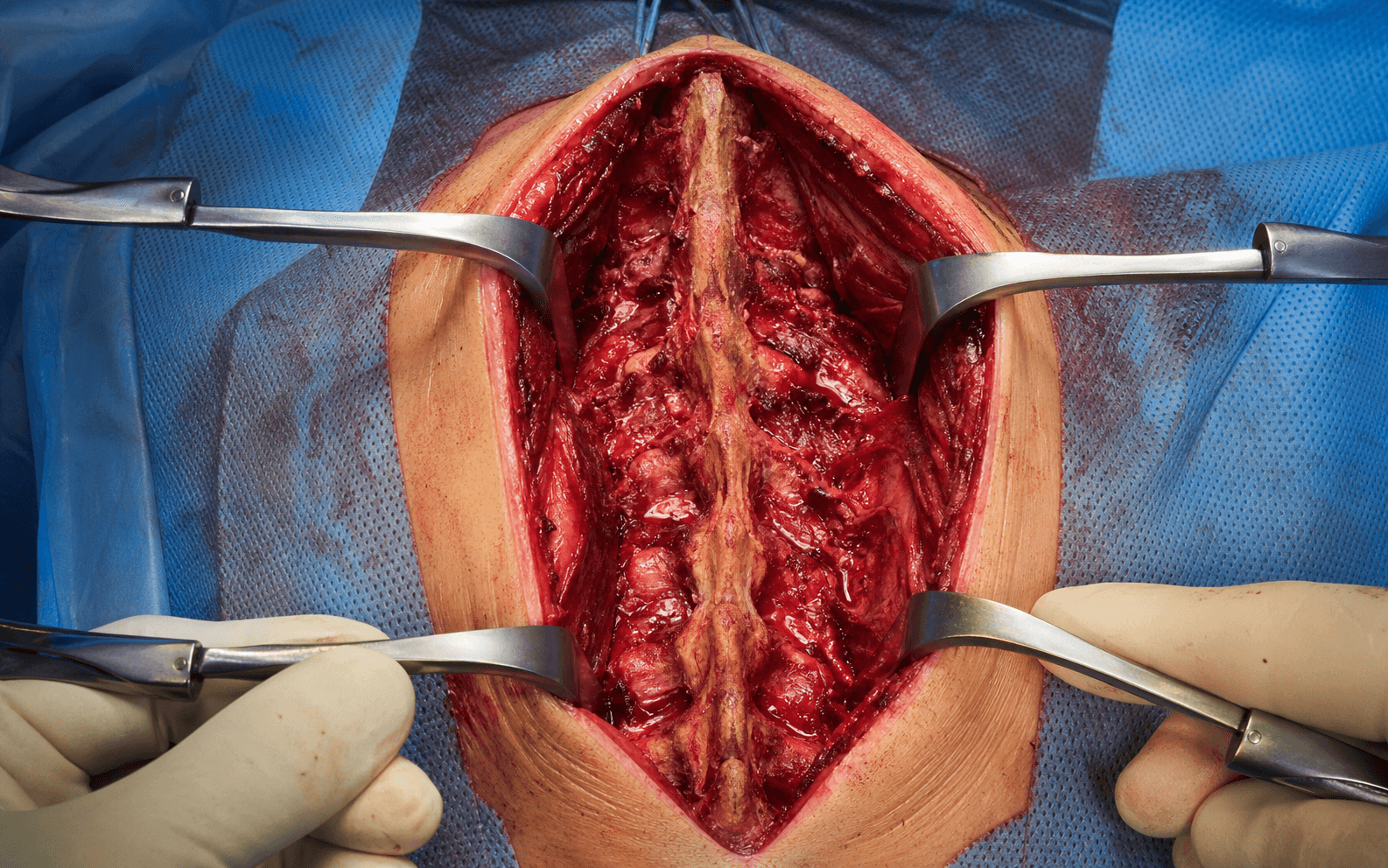
The Exposure
Work down the midline in a subperiosteal plane from C3 to C7, preserving the C2 muscle insertion, then proceed to decompression (laminoplasty or laminectomy) and lateral-mass instrumentation on the exposed posterior elements.
Posterior cervical exposure — step by step
- General anaesthesia with endotracheal intubation; SSEP and MEP monitoring set up for the cord.
- Mayfield 3-pin clamp: one pin frontal above the eyebrow, two pins occipital (avoiding the transverse sinus and auricular nerve); patient prone on chest rolls with axillae free.
- Hold the neck neutral — flexion increases epidural venous bleeding, extension narrows the canal and risks cord injury. Pad elbows, iliac crests, knees and toes.
- Palpate the inion, the prominent C2 spinous process and the non-bifid C7 vertebra prominens to confirm levels.
- A midline incision over the spinous processes from C2 to C7 (extend to the occiput only if occipito-cervical fusion is planned).
- Divide the ligamentum nuchae in the midline avascular raphe between the left and right trapezius with electrocautery — this plane avoids denervating the trapezius (spinal accessory nerve).
- Begin subperiosteal dissection on the spinous processes and laminae starting at C3, not C2 — this preserves the semispinalis cervicis insertion on the C2 spinous process, which is the key muscle-sparing manoeuvre that limits postoperative axial pain.
- Carry the dissection laterally to the medial border of the lateral mass, leaving the facet capsule intact until instrumentation.
- Expose C2 only if C2 instrumentation is needed: detach semispinalis from the inferior C2 spinous process only if unavoidable and undercut the C2 lamina from inferior, preserving the superior muscle attachments.
- Place Taylor or Scoville self-retaining retractors on the laminae, maintaining the subperiosteal plane to minimise muscle bleeding.
- Hinge side (typically left): with a high-speed burr create a trough at the lamina–lateral mass junction, 3–4 mm wide, to the inner cortex only (leave a thin shell for a greenstick hinge; do not violate the dura).
- Open side (right): perform a complete osteotomy through both cortices at the same levels; sharply divide the ligamentum flavum so the lamina can swing open.
- Open the door 4–5 mm — the canal diameter rises from 10–12 mm (stenotic) to 14–17 mm — and hold it open with a 5–7 mm bone block or ceramic/titanium spacer secured with a microplate or a suture through a drill hole in the lateral mass.
- Place morselised bone graft at the hinge to promote lamina-to-lateral-mass fusion over 6–12 months and prevent hinge fracture.
- For laminectomy, rongeur away the spinous processes and remove the lamina piecemeal with Kerrison rongeurs from the inferior edge up, working to the medial edge of the facet (preserve the capsule). The dura should be pulsatile at the end.
- Separate the ligamentum flavum from the dura with a micro-dissector before removing it to avoid a dural tear.
- For radiculopathy, add a foraminotomy: resect the medial 50 percent of the inferior articular process with a burr to unroof the root, then clear compressive disc or osteophyte. Never resect more than 50 percent of the facet — it causes iatrogenic instability.
- Identify the lateral mass borders (medial ridge at the lamina junction, facet capsule laterally, superior and inferior articular processes).
- Start point: 1 mm medial and 1 mm superior to the lateral mass centre (targets the thickest bone, avoids the anterolateral corner where the vertebral artery courses).
- Trajectory: 25 degrees lateral (diverges from midline, away from the foramen) and 25 degrees cephalad (parallel to the facet, away from the exiting root).
- Drill 2.5 mm to 12–14 mm with constant bone resistance — sudden loss of resistance means cortical perforation into the transverse foramen: abort. Tap 3.5 mm and insert a 3.5 by 14–16 mm cortical screw for bicortical purchase, torqued to 4–6 Nm.
- C7 alternative (pedicle screw): entry 1 mm lateral to the lateral mass centre, 25–30 degrees medial and 5–10 degrees caudad, depth 25–30 mm — C7 is the most reliable subaxial pedicle site (largest pedicle).
- Contour a 3.5 mm titanium rod to the cervical lordosis (10–20 degrees over C3–C7), seat it and tighten the set screws to 6–8 Nm; apply compression across levels if deformity correction is needed.
- Prepare the fusion bed: decorticate the facet joints and lateral mass surfaces to bleeding bone, and pack autograft (30–40 cc available from the removed spinous processes and laminae) ± cancellous allograft. rhBMP-2 is off-label in the cervical spine and reserved for high-risk non-union (smokers, diabetics, irradiated beds — Vaccaro 2008).
- Haemostasis with bipolar to the muscle edges and haemostatic agents to the epidural venous plexus; place a closed-suction subfascial drain (remove when output is less than 30 mL per day).
- Re-approximate muscle to the midline ligamentum nuchae raphe and close the fascia (0-Vicryl), then subcuticular 3-0 Monocryl or staples.
- Hard collar for 6–12 weeks after laminectomy plus fusion; laminoplasty is intrinsically stable and needs at most short symptomatic collar use with early range-of-motion. Ambulate on day 1, no lifting greater than 5 kg for 12 weeks.
The vertebral artery is the most feared vascular structure during posterior cervical instrumentation, yet clinically VA injury is rare (0 percent in Heller's 654-screw series; large pooled estimates remain well under 1 percent — Heller 1995). The VA ascends through the transverse foramina (C6 up to C2) anterior to the lateral mass, and in cadaveric study neither the Magerl nor the Roy-Camille trajectory breached it (Heller 1991) — it is endangered chiefly by excessive anterior screw depth or an anterolateral entry. Safeguards: use a lateral and cephalad (Magerl) trajectory aimed away from the foramen; start 1 mm medial to the lateral mass centre; keep screws to safe bicortical length (about 14 mm); obtain preoperative CT angiography for any C1–C2 work or a suspected anomalous VA; and insist on constant bone "feel" while drilling. If the artery is breached, do NOT remove the screw (it tamponades the laceration) — pack bone wax, obtain a CT angiogram, and involve vascular or interventional specialists.
Start the subperiosteal dissection at C3, not C2, to preserve the semispinalis cervicis insertion on the C2 spinous process. Detaching this insertion is the principal driver of the high axial-pain burden after laminoplasty (about 60 percent versus about 19 percent after anterior fusion — Hosono 1996). Protect the facet capsules at the same time.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Direct trauma (Kerrison or burr), compression (haematoma), ischaemia (hypotension) — cord injury 0.2–0.5 percent
- Protection
- SSEP and MEP monitoring (a 50 percent MEP drop signals compromise), keep MAP greater than 85 mmHg, meticulous piecemeal technique
- Structure at risk
- Anterior screw over-penetration or anterolateral entry at C3–C6; high-riding VA at C2 (10–15 percent)
- Protection
- Magerl trajectory aimed away from the foramen, bicortical-but-short screws (about 14 mm), preoperative CTA for C1–C2; if breached, leave the screw in and pack bone wax
- Structure at risk
- Traction on the short, tethered C5 root as the cord drifts posteriorly (pooled about 4.6 percent)
- Protection
- Prophylactic C4/C5 foraminotomy reduces palsy from 6.4 percent to 1.4 percent (Katsumi 2012); avoid resecting more than 50 percent of the facet
- Structure at risk
- CSF leak (1–3 percent), nerve-root injury during foraminotomy
- Protection
- Separate the ligamentum flavum from the dura before removing it; primary repair of any dural tear with 5-0 Prolene and a sealant
- Structure at risk
- Axial neck and shoulder pain (about 60 percent if C2 is detached, versus about 19 percent after anterior fusion — Hosono 1996)
- Protection
- Start subperiosteal dissection at C3 to spare the C2 semispinalis cervicis insertion; preserve the facet capsules
- Structure at risk
- Brisk venous bleeding during laminectomy (valveless Batson's plexus)
- Protection
- Tamponade with haemostatic agents (Surgicel, thrombin-soaked gelfoam); bipolar on low settings to avoid thermal cord injury
C5 palsy is the characteristic neurological complication of cervical decompression, with a pooled incidence of about 4.6 percent (range 4.6–11 percent) and, importantly, no significant difference between laminoplasty and anterior decompression and fusion, or between open-door and French-door laminoplasty (Sakaura 2003). It presents 1–7 days postoperatively as deltoid and biceps weakness (typically MRC 2–3/5) with preserved hand function. The leading mechanism is traction on the short C5 root as the cord drifts posteriorly after decompression; a competing theory is a segmental cord reperfusion injury. Prevention: prophylactic bilateral C4/C5 foraminotomy reduced palsy from 6.4 percent to 1.4 percent in a prospective study (Katsumi 2012) without adding instability or neck pain at two years. Management is supportive — early physiotherapy to prevent a frozen shoulder and EMG at three weeks for a baseline; there is no role for steroids or for surgical re-exploration of an isolated palsy without a compressive lesion. About 70 percent recover to MRC 4/5 by 6–12 months; roughly 30 percent are left with permanent MRC 3/5 weakness.
Vertebral artery course by level. The screw trajectory is safe only if the artery's position at each level is respected.
- VA position relative to the lateral mass
- Curves posteriorly around the C2 lateral mass in the sulcus arteriosus; only 2–3 mm from C2 pars/pedicle screws
- Clinical implication for screws
- High-riding VA in 10–15 percent — obtain CTA preoperatively; C2 pars (5–8 mm) safer than pedicle (3–5 mm)
- VA position relative to the lateral mass
- Transverse foramen anterior to the lateral mass, 3–5 mm from the trajectory
- Clinical implication for screws
- Magerl 25 degrees lateral and 25 degrees cephalad maintains the safety margin
- VA position relative to the lateral mass
- Transverse foramen anterior to the lateral mass, 3–5 mm
- Clinical implication for screws
- Safe level for lateral mass screws
- VA position relative to the lateral mass
- Transverse foramen anterior to the lateral mass, 3–5 mm
- Clinical implication for screws
- Safe level for lateral mass screws
- VA position relative to the lateral mass
- VA enters the foramen from anterior; 4–6 mm, more anterior at the entry level
- Clinical implication for screws
- Keep screws under 16 mm to avoid the anterior cortex and the VA entry zone
- VA position relative to the lateral mass
- VA may not traverse the foramen (passes anterior to C7 in about 10 percent)
- Clinical implication for screws
- Pedicle screws are safe; C7 is the most reliable subaxial pedicle-screw site
Extensile options. Extend cephalad to the occiput for occipito-cervical fusion, and to C1–C2 for a Harms/Goel construct (use C2 pars or pedicle screws with preoperative CTA for a high-riding VA). Extend caudad across the cervico-thoracic junction to T1 for posterior osteotomy (Smith-Petersen or pedicle-subtraction osteotomy for ankylosing-spondylitis chin-on-chest deformity). Convert from lateral mass to pedicle screws at C7 where the pedicle is largest and most consistent. Complications at a glance - Neurological — C5 palsy 4.6–11 percent (Sakaura 2003); spinal cord injury 0.2–0.5 percent (direct trauma, haematoma, hypotension; high-dose methylprednisolone is no longer recommended — NASCIS II/III showed no proven benefit); recurrent laryngeal nerve palsy 0.1–0.2 percent (prone hyperextension traction).
- Hardware — vertebral artery injury 0.2–0.5 percent (lateral mass) up to 2–5 percent (C2 pedicle); screw loosening 3–5 percent; hardware prominence 5–10 percent.
- Fusion — pseudarthrosis 4–8 percent (higher with smoking, diabetes, 4 levels or more); adjacent-segment disease 25–30 percent at 10 years (Hilibrand 1999).
- Wound — superficial infection 2–3 percent, deep infection 0.5–1 percent; CSF leak or pseudomeningocele 1–3 percent (small leaks treated with bed rest and acetazolamide, large leaks with primary repair and a lumbar drain).
- Deformity — post-laminectomy kyphosis: 5–10 percent after laminoplasty but 50–60 percent after laminectomy without fusion (loss of the posterior tension band — Ratliff and Cooper 2003). Prevent with laminoplasty, or with fusion if preoperative kyphosis is greater than 10 degrees.
Procedures Through This Approach
- Posterior cervical laminectomy plus fusion and posterior cervical laminectomy — decompression with or without instrumented fusion for multilevel stenosis with kyphosis or instability.
- Laminoplasty (open-door Hirabayashi) — motion-preserving decompression for multilevel stenosis with maintained lordosis and high-canal-occupancy OPLL.
- Lateral mass screw fusion (C3–C6) with C7 pedicle and C2 pars/pedicle screws — the workhorse subaxial construct; pedicle screws at C7 where the pedicle is largest.
- Posterior cervical foraminotomy — unroofing the root for radiculopathy (resect the medial 50 percent of the inferior articular process).
- C1–C2 posterior fusion (Harms/Goel) — C1 lateral mass and C2 pars/pedicle screws (CTA first for a high-riding VA).
- Occipito-cervical and cervico-thoracic extension — extend the construct cephalad to the occiput or caudad across C7–T1 for tumour, trauma or rheumatoid instability.
- Posterior cervical osteotomy (Smith-Petersen or pedicle-subtraction osteotomy at C7–T1) — correction of ankylosing-spondylitis chin-on-chest deformity.
Viva & Exam Focus
MAGERLMAGERL — lateral mass screw technique
C5-P-A-L-S-YC5 PALSY — risk factors for post-laminoplasty C5 palsy
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old man has a C3–C6 open-door laminoplasty for multilevel stenosis with myelopathy (OPLL 55 percent canal occupancy). On day 3 he reports left shoulder weakness: deltoid 2/5, biceps 3/5, with preserved triceps and hand function and intact sensation. How do you manage him?”
“You are placing a right C4 lateral mass screw with the Magerl technique during posterior cervical fusion. After drilling you notice pulsatile bleeding from the hole, with about 200 mL ongoing loss. How do you manage this intraoperatively?”
“A 63-year-old man has C3–C6 multilevel stenosis with myelopathy (mJOA 12/17, clumsy hands, gait instability), T2 cord signal change, maintained C2–C7 lordosis of 15 degrees, and no instability. He asks about the motion-preserving option versus fusion. How do you counsel him?”
Vertebral artery and lateral mass screw safety
- VA ascends through the transverse foramina (C6 up to C2), lying anterior to the lateral mass screw trajectory
- Magerl: lateral plus cephalad, entry medial to the lateral mass centre, aimed away from the foramen; diverges from the root but crosses the facet
- Roy-Camille: more straight-lateral, slightly cephalad, entry at the lateral mass centre; more parallel to the facet but nearer the root
- Cadaveric study: neither technique threatened the VA (Heller 1991)
- C2 high-riding or medialised VA in roughly 10–20 percent — obtain preoperative CT angiography for C1–C2 work
- C7 is the most reliable subaxial pedicle-screw level (largest, most consistent pedicle)
C5 palsy — mechanism, risk, prevention
- Pooled incidence about 4.6 percent (4.6–11 percent); no significant difference laminoplasty versus anterior fusion (Sakaura 2003)
- Mechanism: posterior cord shift (3–5 mm) tethers the short, relatively tethered C5 root
- Presentation: deltoid and biceps weakness (MRC 2–3/5), preserved hand function, onset 1–7 days
- Recovery: about 70 percent reach MRC 4/5 by 6–12 months; about 30 percent have permanent MRC 3/5
- Prevention: prophylactic C4/C5 foraminotomy reduces palsy from 6.4 percent to 1.4 percent (Katsumi 2012)
C2 muscle preservation and axial pain
- Semispinalis cervicis inserts on the C2 spinous process; its detachment drives axial pain
- Axial neck and shoulder pain: about 60 percent after laminoplasty versus about 19 percent after anterior fusion (Hosono 1996)
- Muscle-sparing technique: start the subperiosteal dissection at C3, undercut the C2 lamina from inferior
- Preserve the facet capsules; expose C2 only if C1–C2 instrumentation is needed
Positioning and exposure
- Prone, Mayfield 3-pin head fixation (one pin frontal, two occipital), neutral neck
- Avoid flexion (increases epidural bleeding) and extension (narrows the canal, risks cord injury)
- SSEP and MEP monitoring — a 50 percent drop in MEP amplitude signals cord compromise
- Midline incision C2–C7 over the spinous processes; split the ligamentum nuchae in the avascular raphe
- Subperiosteal dissection to the lateral mass medial border; keep the facet capsule intact until instrumentation
Laminoplasty technique (open-door Hirabayashi)
- Hinge side: burr a trough at the lamina–lateral mass junction to the inner cortex only (greenstick)
- Open side: complete osteotomy through both cortices; release the ligamentum flavum
- Open the door 4–5 mm — canal diameter rises from 10–12 mm (stenotic) to 14–17 mm
- Hold the opening with a 5–7 mm bone block or ceramic spacer, secured with a microplate or suture
- Bone graft at the hinge promotes lamina-to-lateral-mass fusion over 6–12 months
Lateral mass screw — Magerl steps
- Start point 1 mm medial and 1 mm superior to the lateral mass centre (thickest bone)
- Trajectory 25 degrees lateral (away from the VA) and 25 degrees cephalad (parallel to the facet)
- 2.5 mm drill to 12–14 mm with constant bone resistance — sudden loss means perforation, abort
- 3.5 mm by 14–16 mm cortical screw, bicortical, torque 4–6 Nm
- C7 pedicle alternative: 25–30 degrees medial, 5–10 degrees caudad, 25–30 mm depth
Complications and rates
- C5 palsy 4.6–11 percent (Sakaura 2003); spinal cord injury 0.2–0.5 percent
- Vertebral artery injury 0.2–0.5 percent (lateral mass) up to 2–5 percent (C2 pedicle); 0 percent in Heller's 654-screw series
- Screw loosening 3–5 percent; hardware prominence 5–10 percent
- Pseudarthrosis 4–8 percent; adjacent-segment disease 25–30 percent at 10 years (Hilibrand 1999)
- Infection superficial 2–3 percent, deep 0.5–1 percent; CSF leak 1–3 percent
- Post-laminectomy kyphosis: 5–10 percent after laminoplasty, 50–60 percent after laminectomy without fusion
Exam traps and high-yield
- Roy-Camille (centre, straight-lateral, near the root) versus Magerl (medial, divergent, away from the root) — neither threatens the VA (Heller 1991)
- Never remove a screw after VA injury — it tamponades; pack bone wax and get a CTA
- No surgical re-exploration for an isolated C5 palsy without a compressive lesion
- Never laminectomy without fusion for multilevel stenosis — post-laminectomy kyphosis
- Spare the C2 semispinalis insertion and facet capsules to limit axial pain (Hosono 1996)
References
C5 Palsy After Decompression Surgery for Cervical Myelopathy — Systematic Review
- Systematic review of the literature (papers published 1986-2002) on postoperative C5 palsy after surgery for cervical compression myelopathy. Pooled mean incidence of C5 palsy was 4.6% across all decompressive procedures. Critically, there were NO significant differences in C5 palsy incidence between anterior decompression and fusion versus laminoplasty, between unilateral open-door and French-door (double-door) laminoplasty, or between cervical spondylotic myelopathy and OPLL. Two competing pathogenetic theories are discussed: (1) nerve root injury (tethering/traction of the short C5 root with posterior cord drift, with or without foraminal stenosis), and (2) segmental spinal cord disorder (reperfusion injury to the C5 anterior horn). Neither hypothesis was consistently supported. Foraminotomy combined with laminoplasty had been proposed to prevent/treat C5 palsy but at the time required further study. Prognosis for functional recovery was generally good, but severely paralysed cases required significantly longer recovery.
Anatomic Comparison of the Roy-Camille and Magerl Techniques for Lower Cervical Screw Placement
- Cadaveric study comparing the Roy-Camille (entry at lateral mass centre, straight lateral, 10° cephalad) and Magerl (entry 1mm medial/cephalad to centre, 25° lateral, 30-45° cephalad parallel to facet) lateral mass screw techniques under simulated operating-room conditions by three surgeons of differing experience, assessed by anatomic dissection and radiographs. KEY RESULT: the spinal cord and vertebral arteries were NOT threatened (no breach) by EITHER technique. The Roy-Camille technique carried LESS risk of nerve root injury and fewer 'zone' placement errors; the Magerl technique carried LESS risk of facet joint violation (its trajectory aims away from the foramen but across the facet). A learning curve was observed - after the surgeons gained experience, differences between techniques were no longer statistically significant. Aiming accuracy was equal in the axial plane but consistently less accurate in the sagittal plane for Magerl screws because of cervicothoracic-junction prominence.
Complications of Posterior Cervical Plating — Clinical Series of Lateral Mass Fixation
- Retrospective clinical review of 78 consecutive patients (mean age 52.9 years, mean follow-up 2 years) treated with posterior cervical lateral mass plating; 654 screws inserted (mean 8.4 per patient), with complex reconstructions in 70.5%. Complication rates PER SCREW: nerve root injury 0.6%, facet violation 0.2%, broken screw 0.3%, screw avulsion 0.2%, screw loosening 1.1%, and vertebral artery injury 0% (no VA injuries occurred). Complication rates PER CASE: spinal cord injury 2.6%, iatrogenic foraminal stenosis 2.6%, broken plate 1.3%, lost reduction 2.6%, adjacent-segment degeneration 3.8%, infection 1.3%, pseudarthrosis 1.4%. The authors emphasise that observed clinical complication rates were CONSIDERABLY LOWER than the theoretical anatomic risks predicted by prior cadaveric work.
Neck and Shoulder (Axial) Pain After Laminoplasty — A Noticeable Complication
- Retrospective study of 98 patients operated for cervical spondylotic myelopathy: 72 underwent laminoplasty and 26 underwent anterior interbody fusion. Postoperative axial (neck and shoulder) symptoms were SIGNIFICANTLY more common after laminoplasty than after anterior fusion: 60% versus 19% (P less than 0.05). In 18 laminoplasty patients (25%) the chief complaint was severe axial pain persisting more than 3 months, whereas NO anterior-fusion patient reported such severe persistent pain. The authors highlight that axial symptoms after laminoplasty are more prevalent and more disabling than previously believed and should be counted when judging surgical outcome, attributing them in part to disruption of the posterior cervical extensor musculature and facet/capsular structures during the posterior exposure.
Prophylactic Bilateral C4/C5 Foraminotomy Prevents C5 Palsy After Open-Door Laminoplasty
- Prospective comparative study of 282 patients with cervical myelopathy. 141 consecutive patients (2009-2010) underwent open-door laminoplasty WITH prophylactic bilateral C4/C5 microforaminotomy (foraminotomy group, FG); 141 consecutive patients (2006-2008) underwent laminoplasty WITHOUT foraminotomy (non-foraminotomy group, NFG). Incidence of postoperative C5 palsy was 1.4% (2/141) in the FG versus 6.4% (9/141) in the NFG (P less than 0.05). Mean operative time was longer with foraminotomy (129 vs 102 minutes, P less than 0.05) but there were no significant differences in blood loss or number of decompressed levels. Two patients still developed C5 palsy despite foraminotomy, suggesting a minor additional spinal-cord (segmental) mechanism. A 2-year follow-up study from the same group (Ohashi et al, Spine 2014, PMID 24503687) confirmed C5 palsy 1.7% (FG) vs 7.0% (NFG) with no adverse effect on C2-C7/C4-C5 lordosis, range of motion, hinge-fracture or non-union rates and unchanged neck-pain scores.