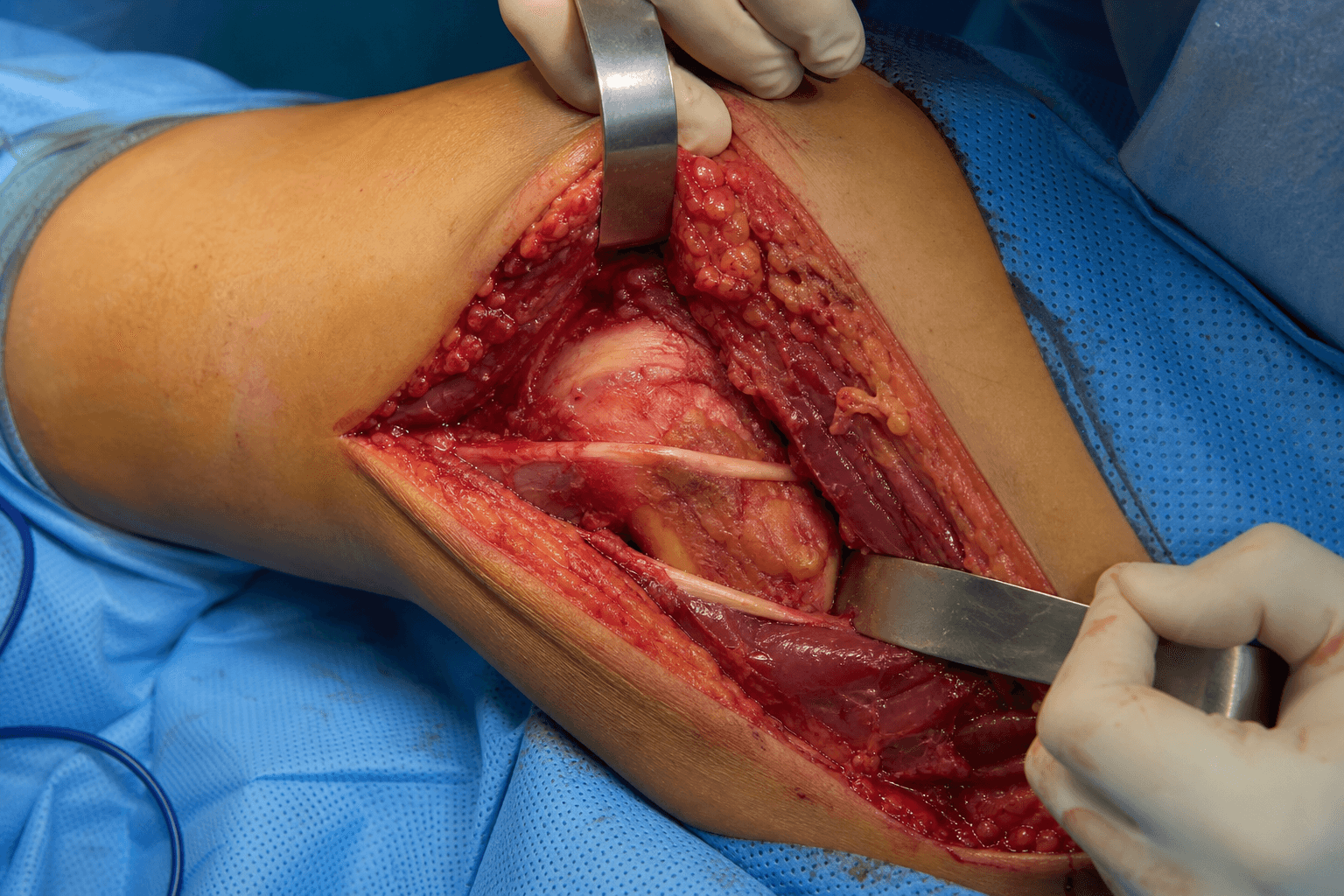
CPN at the fibular neck - LCL, popliteus and PFL reconstruction - posterolateral corner repair
- What the approach exposes: the fibular head, LCL, popliteus tendon, popliteofibular ligament (PFL), biceps femoris insertion and the common peroneal nerve.
- Golden rule - protect the CPN first: identify and protect the common peroneal nerve before any dissection around the fibular head. It crosses the fibular neck roughly 2cm distal to the head apex, closely applied to bone.
- PLC static stabilizers: LCL (primary varus restraint), popliteus tendon (primary external rotation restraint) and the popliteofibular ligament (secondary external rotation restraint and primary restraint to posterior translation of the lateral tibial plateau - Shahane 1999). The LCL and popliteus complex together resist varus and external rotation (Gollehon 1987).
- Injury patterns are usually combined: isolated PLC tears are uncommon - the majority occur with ACL and/or PCL injury in the multiligament-injured or dislocated knee, so maintain a high index of suspicion.
- Clinical examination: dial test at 30° and 90° (greater than 10° asymmetry is positive), varus stress at 0° and 30° (greater than 10mm opening is Grade III), external rotation recurvatum and the posterolateral drawer.
- Operative indications: Grade III PLC injury (varus laxity greater than 10mm at 30°, external rotation asymmetry greater than 10° on the dial test) and chronic PLC insufficiency with functional instability.
When & Why
What it exposes. The posterolateral approach to the knee gives direct access to the fibular head and the structures of the posterolateral corner (PLC) for repair or reconstruction of the lateral collateral ligament (LCL), the popliteus tendon and the popliteofibular ligament (PFL). The common peroneal nerve is the highest-risk structure: it crosses the fibular neck roughly 2cm distal to the fibular head apex, closely applied to bone. The single most important principle of the approach is to identify and protect the common peroneal nerve before any dissection around the fibular head. Why this approach. It is the workhorse exposure for anatomic PLC reconstruction and the only approach that simultaneously controls the fibular head, the LCL femoral and fibular attachments, the popliteus and the PFL while keeping the common peroneal nerve under direct vision throughout. PLC injuries are rarely isolated - the majority occur with ACL and/or PCL tears in multiligament knee injuries - and modern practice favours anatomic reconstruction of all torn structures performed concurrently with cruciate reconstruction rather than repair plus staged cruciate surgery (Geeslin 2015). Indications. - PLC reconstruction (primary indication): Grade III PLC injury (varus laxity greater than 10mm at 30°, dial test greater than 10° asymmetry), and chronic PLC insufficiency with a varus thrust gait or recurrent giving way.
- Combined ligament injuries (the majority): ACL plus PLC (varus hyperextension), PCL plus PLC (dashboard injury), and ACL plus PCL plus PLC (knee dislocation). Reconstruct all torn structures concurrently with the cruciate(s) - acute repair plus staged cruciate reconstruction fails far more often (about 38%) than concurrent reconstruction of all torn structures (about 9%, Geeslin 2015).
- Fibular head fractures: avulsion of the LCL or biceps insertion displaced greater than 5mm (ORIF), and comminuted fractures as part of a Schatzker IV tibial plateau injury.
- Common peroneal nerve exploration: iatrogenic injury with immediate postoperative foot drop and intact preoperative function, traumatic palsy at presentation, or a delayed palsy with no recovery by 4-6 months on EMG.
- Varus opening at 30°
- Less than 5mm
- Dial test
- Less than 10° asymmetry
- Management
- Non-operative: hinged brace, quadriceps and hamstring rehabilitation
- Varus opening at 30°
- 5-10mm
- Dial test
- Less than 10° asymmetry
- Management
- Non-operative: hinged brace, rehabilitation
- Varus opening at 30°
- Greater than 10mm
- Dial test
- Greater than 10° asymmetry
- Management
- Operative: anatomic PLC reconstruction (LaPrade)
Position & landmarks. Supine with a bump or sandbag under the ipsilateral hip to roll the knee into internal rotation and bring the posterolateral corner up; a leg holder or post at the medial thigh allows flexion and varus stress for exposure. Lateral decubitus is an alternative for isolated PLC work but is awkward when combining with ACL or PCL reconstruction. A proximal-thigh tourniquet at 250-280mmHg is optional - many surgeons avoid it so a nerve stimulator can be used if the nerve is hard to find. Palpate the fibular head (prominent lateral landmark) and the biceps femoris tendon (cord inserting on the fibular head, with the nerve along its posteromedial border), and centre the incision over and just posterior to the fibular head.
The Exposure
Work down through the layers posterior to the fibular head, identifying and protecting the common peroneal nerve before any bony work, then expose the PLC structures from superficial to deep.
Exposure sequence
- Supine with a bump under the ipsilateral hip to bring the posterolateral corner up; a medial thigh post allows flexion and varus stress for exposure.
- Lateral decubitus is an alternative for isolated PLC surgery but is awkward for combined ACL or PCL reconstruction.
- A proximal-thigh tourniquet at 250-280mmHg is optional - many surgeons omit it so a nerve stimulator can be used.
- Palpate the fibular head and the biceps femoris tendon; the common peroneal nerve runs along the posteromedial border of the biceps.
- Mark a longitudinal incision centred over and just posterior to the fibular head, from roughly 8-10cm proximal to the head (for the LCL femoral attachment) to 4-5cm distal (for the fibular neck and nerve crossing), typically 12-15cm.
- Centre the incision posteriorly, not directly lateral, so the nerve can be identified along the biceps before any bony work.
- Incise skin and subcutaneous tissue; identify the iliotibial band (ITB) anteriorly as a thick fascial layer and the biceps femoris tendon posteriorly as a palpable cord.
- Develop the plane between the ITB (retracted anteriorly) and the biceps (retracted posteriorly) to reach the underlying LCL and lateral joint capsule.
- Before any dissection around the fibular head, palpate the common peroneal nerve as a cord-like structure crossing the fibular neck roughly 2cm distal to the fibular head apex.
- Roll it under the fingers - firm and mobile, like an electrical cord. In an obese or scarred knee where it cannot be felt, use a nerve stimulator at low current (0.5-1.0mA); stimulation produces foot dorsiflexion.
- Identify the nerve along the posteromedial border of biceps femoris and trace it distally to the fibular neck, where it lies closely applied to the periosteum.
- Free it from the fibular neck with blunt dissection only (finger or Kittner) - sharp dissection risks transection.
- Encircle it with a vessel loop or rubber drain.
- Gently retract the nerve anteriorly away from the fibular head using the vessel loop.
- Minimise retraction time and release it periodically (every 20-30 minutes) - the nerve is sensitive to ischaemia from prolonged traction.
- With the nerve protected, identify the biceps femoris and LCL insertions on the fibular head; the LCL inserts posterior to the biceps.
- Subperiosteally elevate soft tissues from the fibular head where drilling is needed (for example a biceps or LCL avulsion repair, or the fibular tunnel).
- The LCL runs from the lateral femoral epicondyle to the fibular head; assess its integrity for a midsubstance tear, femoral avulsion or fibular avulsion.
- Locate the popliteal hiatus (the opening in the lateral capsule posterior to the LCL); the popliteus tendon emerges here and runs to the popliteal sulcus on the lateral femoral condyle.
- Expose the popliteus by blunt dissection only - sharp capsular work risks capsular violation and fluid extravasation.
- Identify the popliteofibular ligament from the popliteus musculotendinous junction to the fibular styloid. In acute injuries it may be merged with haematoma, so define it by finding the fibular styloid insertion and tracing proximally.
The common peroneal nerve is the single most vulnerable structure in this approach and the most commonly injured nerve in PLC trauma and surgery. It crosses the fibular neck roughly 2cm distal to the fibular head apex, closely applied to bone. Identify and loop it along the posterior border of the biceps before any fibular head work, free it with blunt dissection only, retract it anteriorly, release retraction every 20-30 minutes, keep electrocautery at least 1cm away, and never drill blind into the fibular head.
At the level of the fibular neck the common peroneal nerve lies anterior to the biceps femoris tendon. Dissecting along the posterior border of the biceps keeps you away from the nerve, and centring the incision just posterior to the fibular head lets you find the nerve along the biceps before any bony work.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Common peroneal nerve at the fibular neck (crosses roughly 2cm distal to the head, closely applied to bone)
- How to protect it
- Identify first; palpate as a cord; blunt dissection only; loop with a vessel loop; retract anteriorly; no blind drilling; no electrocautery within 1cm
- Structure at risk
- Popliteal artery and vein (roughly 15-20mm medial to the fibular head)
- How to protect it
- Stay lateral to the biceps-hamstring interval; fluoroscopy for any posterior tibial tunnel; blunt dissection near the posterior capsule
- Structure at risk
- LCL and biceps femoris conjoined insertion on the fibular head
- How to protect it
- Subperiosteal elevation; protect the conjoined insertion during drilling and fixation
- Structure at risk
- Popliteus tendon at the popliteal hiatus
- How to protect it
- Blunt exposure only; avoid sharp capsular work that risks fluid extravasation
Common peroneal nerve injury classification and recovery. The common peroneal nerve is the most common complication of this surgery. Mechanisms include drill penetration through the fibular head into the nerve roughly 2cm distal to the apex, direct trauma while freeing it from the fibular neck, excessive retractor traction and thermal injury from electrocautery.
- Pathology
- Conduction block; axon intact; no Wallerian degeneration
- Mechanism
- Compression, traction, blunt trauma (retractor)
- Recovery
- 90-95% complete recovery by 6-9 months
- Pathology
- Axon disrupted; endoneurial tube intact; Wallerian degeneration
- Mechanism
- Severe crush, stretch or thermal injury
- Recovery
- 60-70% functional recovery by 12-18 months
- Pathology
- Complete transection; axon and sheath disrupted; neuroma
- Mechanism
- Sharp laceration, drill penetration
- Recovery
- No spontaneous recovery; primary repair 60%, nerve graft 40%
The popliteal artery and vein lie roughly 15-20mm medial to the fibular head. They are not at risk in a standard posterolateral dissection as long as you stay lateral to the biceps-hamstring interval and use fluoroscopy for any posterior tibial tunnel - but they are injured in high-energy trauma, so check pulses and the ankle-brachial index in every knee dislocation.
Extensile options. Extend proximally along the femur (8-10cm) to expose the LCL femoral attachment on the lateral epicondyle; extend distally along the fibular shaft to follow the fibular neck and the course of the common peroneal nerve. A straight lateral approach (between the ITB and biceps, anterior to the biceps) is used for Schatzker I-III tibial plateau fractures and is distinct from the posterolateral approach, which is more posterior (posterior to the biceps) for the PLC structures and the fibular head. Closure. Layered closure over the reconstructed PLC; the lateral capsule and ITB-biceps interval are repaired. A haematoma drain is used at the surgeon's discretion. The knee is splinted or braced in extension.
Procedures Through This Approach
- Anatomic PLC reconstruction (LaPrade) - the principal operation done through this exposure.
- Fibular head fracture ORIF - lag screws, a plate or suture anchors for an avulsion fragment.
- Common peroneal nerve exploration - neurolysis, primary repair or nerve grafting. Anatomic PLC reconstruction (LaPrade technique - gold standard). Reconstruct both the LCL (femoral epicondyle to fibular head) and the popliteofibular ligament (popliteus to fibular styloid), using allograft (Achilles tendon with a bone block, tibialis anterior or semitendinosus) or autograft (hamstring or quadriceps tendon). Allograft is preferred for combined ACL plus PLC so the hamstrings are preserved for an ACL autograft.
Anatomic reconstruction sequence
- Drill a 7mm tunnel at the anatomic LCL origin on the lateral femoral epicondyle, proximal and posterior to the popliteus origin.
- Drill a 7mm tunnel through the fibular head from lateral to anterior, exiting on the anterior fibular neck and avoiding the peroneal nerve roughly 2cm distal.
- Use fluoroscopy to confirm the trajectory and a drill stop or depth gauge to avoid plunging through the far cortex.
- Pass the graft (for example semitendinosus allograft) from femur to fibula and fix the femoral side with an interference screw or suspensory button.
- Tension with the knee at 30° flexion, neutral rotation and slight varus to restore the near-isometric LCL length, then fix on the fibular head.
- Drill a 7mm tunnel at the anatomic popliteus origin in the popliteal sulcus, anterior and distal to the LCL femoral origin.
- Attach the graft (a separate limb or shared with the LCL graft) to the fibular styloid with a suture anchor or bone tunnel.
- Pass it through the popliteus tunnel (posterior to the LCL graft) to recreate the popliteus course.
- Tension at 60-70° flexion and neutral rotation (the popliteus-PFL complex is tightest in flexion), then fix.
- A standalone popliteus tendon reconstruction (a tunnel from the popliteal sulcus to the posterior tibia) is rarely done in isolation and is usually combined with LCL plus PFL reconstruction.
- Anatomic reconstruction (LaPrade)
- LCL (femoral epicondyle to fibular head) PLUS popliteofibular ligament (popliteus to fibular styloid) - two structures
- Non-anatomic (historical)
- LCL only, or biceps tenodesis - single structure
- Anatomic reconstruction (LaPrade)
- Both varus (LCL) and external rotation (PFL) - complete PLC function
- Non-anatomic (historical)
- Varus only - residual rotatory deficit, dial test remains positive
- Anatomic reconstruction (LaPrade)
- About 9% when all torn structures are reconstructed concurrently (Geeslin 2015)
- Non-anatomic (historical)
- About 38% with repair plus staged cruciate reconstruction (Geeslin 2015)
- Anatomic reconstruction (LaPrade)
- IKDC subjective 29 to 82, Cincinnati 22 to 81, near-normal varus stress radiographs (Geeslin and LaPrade 2011)
- Non-anatomic (historical)
- Persistent rotatory laxity; lower return to pre-injury sport
- Anatomic reconstruction (LaPrade)
- Three bone tunnels (femoral LCL, femoral popliteus, fibular head), two graft limbs, about 180-210 minutes
- Non-anatomic (historical)
- One tunnel or biceps rerouting, about 90-120 minutes
- Anatomic reconstruction (LaPrade)
- Gold standard for Grade III PLC injuries
- Non-anatomic (historical)
- Superseded - leaves a rotatory deficit (Gollehon 1987, Shahane 1999)
Combined ACL or PCL plus PLC: reconstruct concurrently, not staged. For a combined injury, reconstruct all torn structures in a single setting with the cruciate(s). Pooled data show about 9% posterolateral failure when all torn structures are reconstructed concurrently versus about 38% with acute repair of the corner plus staged cruciate reconstruction (Geeslin 2015); the mechanism of failure is that an unaddressed or under-reconstructed PLC leaves varus and rotatory laxity that overloads the cruciate graft (Gollehon 1987). The surgical sequence is PLC first, then ACL: drill and tension the PLC grafts (LCL at 30°, popliteus-PFL at 60-70°), then tension the ACL last, because PLC laxity allows the tibia to subluxate and would over-tension the ACL graft. The exception is severe soft-tissue injury with massive swelling or blisters after a knee dislocation with vascular repair - brace for 1-2 weeks for the swelling to settle, then perform the combined reconstruction (not separate staged procedures). Common peroneal nerve exploration. Findings dictate management: a nerve in continuity (contusion or neurapraxia, the most common) needs neurolysis (about 80% functional recovery); a clean laceration needs primary repair (about 60% recovery); and a gap greater than 1cm needs a sural nerve autograft (about 40% recovery). Fibular head fracture ORIF. Fix a large avulsion fragment (LCL or biceps insertion) displaced greater than 5mm with lag screws, a small plate or suture anchors depending on fragment size. Anatomic reduction and stable fixation give about 90-95% union; peroneal nerve injury is present in about 10-15% at presentation (associated with the fracture) and is iatrogenic in about 2-5% during surgery. Post-operative protocol. Hinged knee brace locked in extension for 2 weeks; partial weight-bearing (toe-touch) for 6 weeks; range of motion 0-90° for the first 6 weeks (no deep flexion, to protect the popliteus reconstruction); full range of motion by 8-12 weeks with strengthening; return to sport at 9-12 months (longer and the ACL timeline determines return when combined).
The LCL maintains a near-constant length from 0° to 90° flexion, which makes it well suited to an anatomic graft reconstruction with the femoral tunnel at the lateral epicondyle and the fibular tunnel through the fibular head, tensioned at 30°.
Viva & Exam Focus
PLCPLC - posterolateral corner essentials
FIBULARFIBULAR - the approach and nerve protection
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old rugby player sustains a varus hyperextension injury. Examination shows varus laxity of 12mm at 30° flexion and 15° external rotation asymmetry on the dial test, with negative Lachman and posterior drawer. How do you grade this PLC injury, and what is your management?”
“A 32-year-old netball player has a positive Lachman, 12° dial test asymmetry at 30°, and 10mm varus laxity at 30°, with MRI confirming ACL, LCL and popliteofibular ligament tears. Do you reconstruct the ACL and PLC concurrently or staged, and in what order?”
“During posterolateral corner reconstruction, after drilling the fibular head tunnel, the patient develops a foot drop intraoperatively. What has happened, how do you manage it immediately, and what is the expected outcome?”
Posterolateral corner anatomy
- LCL - primary varus restraint: lateral femoral epicondyle (proximal and posterior to popliteus) to fibular head; mean length 69mm, near-isometric through ROM (Gollehon 1987)
- Popliteus tendon - primary external rotation restraint: popliteal sulcus on the lateral femoral condyle through the popliteal hiatus to the posterior tibia
- Popliteofibular ligament - secondary external rotation restraint and primary restraint to posterior translation of the lateral tibial plateau (Shahane 1999)
- Arcuate complex - Y-shaped, from fibular styloid to lateral femoral condyle and posterior capsule; present in about 80% of knees (Seebacher 1982)
- Biceps femoris and ITB are the dynamic stabilisers; the biceps shares a conjoined insertion with the LCL on the fibular head
Common peroneal nerve (primary hazard)
- Branches from the sciatic nerve at the popliteal fossa apex, runs along the medial border of biceps femoris, then crosses the fibular neck roughly 2cm distal to the fibular head apex
- Closely applied to the fibular neck periosteum with minimal intervening soft tissue - the zone of highest risk
- High sciatic bifurcation proximal to the popliteal fossa in 10-15% of patients
- Injury causes foot drop (tibialis anterior, EHL, EDL), weak ankle eversion, steppage gait and sensory loss over the dorsum of the foot
Clinical assessment of PLC injury
- Varus stress at 0° and 30°: Grade I less than 5mm, Grade II 5-10mm, Grade III greater than 10mm
- Dial test: greater than 10° asymmetry at 30° only suggests isolated PLC; at both 30° and 90° suggests combined PLC plus PCL
- External rotation recurvatum test: the affected leg hyperextends and externally rotates, suggesting combined PLC plus PCL
- Posterolateral drawer at 90° with the foot externally rotated 15°: the lateral tibial plateau subluxates posteriorly
Exposure and nerve protection
- Golden rule: identify and protect the common peroneal nerve before any dissection around the fibular head
- Longitudinal incision centred over and just posterior to the fibular head; develop the ITB-biceps interval
- Find the nerve along the posterior border of the biceps; free it from the fibular neck with blunt dissection only
- Loop it and retract anteriorly; release every 20-30 minutes; no electrocautery within 1cm; never drill blind
Anatomic reconstruction (LaPrade)
- Reconstruct both the LCL (femoral epicondyle to fibular head) and the popliteofibular ligament (popliteus to fibular styloid)
- Three 7mm tunnels: femoral LCL, femoral popliteus and fibular head (lateral to anterior, avoiding the nerve)
- Tension the LCL at 30° flexion with slight varus; tension the popliteus-PFL complex at 60-70° flexion
- Post-op: brace locked in extension for 2 weeks, partial weight-bearing for 6 weeks, ROM 0-90° for 6 weeks, return to sport 9-12 months
Combined ACL/PCL plus PLC
- Reconstruct all torn structures concurrently - about 9% PLC failure versus about 38% with repair plus staged cruciate (Geeslin 2015)
- Sequence: PLC first, then ACL tensioned last (PLC laxity would over-tension the ACL graft)
- Exception: severe swelling or vascular repair - brace 1-2 weeks, then combined reconstruction
- Acute reconstruction within 2-3 weeks is preferred, before scarring and contracture develop
Outcomes and complications
- Anatomic reconstruction: about 81% objective success for acute Grade III PLC; IKDC subjective 29 to 82, near-normal varus stress radiographs (Geeslin and LaPrade 2011)
- Common peroneal nerve injury is the most common complication: neurapraxia 90-95% recovery by 6-9 months, primary repair 60%, nerve graft 40%
- Graft failure is higher with the repair-plus-staged approach (about 38%) than concurrent reconstruction (about 9%)
- Persistent rotatory instability (10-15%) follows non-anatomic LCL-only reconstruction; stiffness (5-10%) follows prolonged immobilisation
Indications and decision-making
- Operative: Grade III PLC, combined ACL/PCL plus PLC, chronic PLC insufficiency, young pivoting athletes
- Non-operative: Grade I-II (varus less than 10mm, dial less than 10°) with a hinged brace and quadriceps or hamstring rehabilitation
- Also through this approach: fibular head ORIF (avulsion displaced greater than 5mm) and common peroneal nerve exploration
References
Anatomic 2-Graft Posterolateral Reconstruction - Biomechanical Validation & Technique
- Cadaveric study (n=10) of a 2-graft technique anatomically reconstructing the THREE primary static lateral stabilizers: fibular collateral ligament (LCL), popliteus tendon and popliteofibular ligament
- After simulated Grade III sectioning, varus stability was significantly restored by the reconstruction versus the cut state at 0°, 30°, 60° and 90° of flexion
- External rotation was significantly increased in the cut state; the reconstruction restored external rotation with NO significant difference from the intact knee at any flexion angle
- Established the femoral attachment points and tunnel geometry that underpin the modern anatomic PLC reconstruction
Role of Posterolateral & Cruciate Ligaments in Knee Stability - Biomechanical Study
- Selective ligament sectioning in 17 cadaveric specimens tested from 0° to 90° flexion with five degrees of freedom
- At ALL flexion angles, the LCL and the deep (popliteus-arcuate) complex together were the principal structures preventing varus rotation and external rotation of the tibia
- The PCL was the principal restraint to posterior translation; isolated PCL sectioning did NOT alter varus or external rotation at any flexion angle
- Combined sectioning of the LCL and deep complex, then the PCL, produced large increases in posterior translation, varus, and (beyond 30°) external rotation - confirming the PLC and PCL act together
Outcomes of Acute Grade III PLC Injuries - Prospective Case Series & Injury Patterns
- Prospective series of 29 patients (30 knees), mean age 27, with acute Grade III posterolateral knee injury treated within 6 weeks by anatomic repair and/or reconstruction of all injured structures, with concurrent reconstruction of any cruciate tears
- Injury patterns confirm PLC injury is rarely isolated: only 8/30 knees were isolated PLC; 10 had a concurrent ACL tear, 4 a PCL tear, and 8 had BOTH cruciates torn
- Side-to-side lateral compartment gap on varus stress radiographs improved from 6.2mm preoperatively to 0.1mm at final follow-up
- Cincinnati subjective score improved 21.9 to 81.4 and IKDC subjective 29.1 to 81.5; all five IKDC objective subscores improved significantly at a mean 2.4 years
Surgical Treatment of Acute Grade III PLC Injuries - Systematic Review
- Systematic review of 8 studies, 134 patients, acute Grade III PLC injuries with minimum 2-year follow-up
- Overall objective success 81%, failure 19% (varus stability on examination/stress radiographs or need for revision)
- Repair of the LCL/popliteus with STAGED cruciate reconstruction: 17 failures in 45 patients (38%)
- Reconstruction of all torn structures (or hybrid repair/reconstruction) with concurrent cruciate surgery: failure rate only 9%
- Reported IKDC range 78.1-91.3 and Lysholm range 87.5-90.3 across included studies
The Popliteofibular Ligament - Anatomical & Biomechanical Study of the PLC
- The popliteofibular ligament (PFL) was present in all 8 cadaveric knees examined
- On selective sectioning, the PFL was a significant restraint to excessive posterior translation, varus angulation, and primary/coupled external rotation
- Isolated section of the popliteus muscle belly did NOT cause significant posterolateral instability
- The LCL acted as the primary restraint to varus and a secondary restraint to external rotation and posterior displacement
- Isolated PFL reconstruction restored stability ONLY when the LCL was intact; with combined LCL disruption, isolated PFL reconstruction did not restore stability