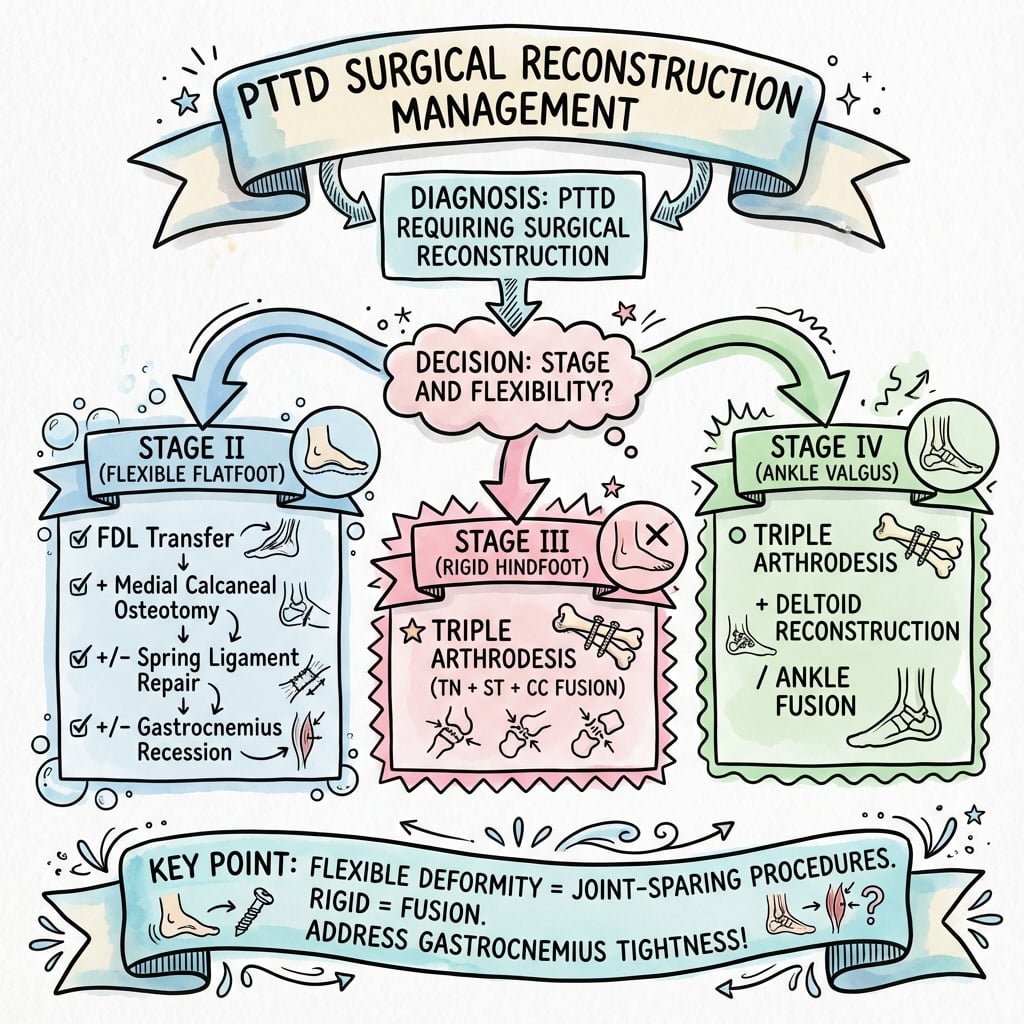
Stage-Based Surgery · FDL Transfer + MDCO Gold Standard · Flexible Versus Rigid Is the Decision
- PTTD is the most common cause of acquired adult flatfoot deformity. Untreated flexible Stage II disease progresses to rigid Stage III deformity that requires arthrodesis — the reason to operate early in Stage II.
- FDL transfer + MDCO is the gold-standard reconstruction for flexible Stage II disease, achieving 85-90% good outcomes while preserving hindfoot motion. FDL transfer alone manages only 60-70%; MDCO alone does not replace the tendon.
- The flexible (Stage II, joint-sparing) versus rigid (Stage III, arthrodesis) distinction — tested by passive correction — is the single most important surgical decision. Soft-tissue reconstruction fails in a rigid foot.
- FDL runs deep to the PTT in the tarsal tunnel; harvest it distal to the master knot of Henry. MDCO shifts the calcaneus 10-12 mm medially, shifting ground reaction force medial to the ankle and offloading the reconstructed tendon.
- Stage IV adds deltoid insufficiency with ankle valgus tilt (medial clear space over 4 mm on the mortise view). Triple arthrodesis alone fails — address the ankle with deltoid reconstruction or tibiotalocalcaneal fusion.
When & Why
Indication. Symptomatic posterior tibial tendon dysfunction (PTTD) — progressive medial ankle pain, a collapsing medial longitudinal arch, heel valgus and loss of the single heel raise — that has failed at least six months of non-operative care (a University of California Biomechanics Laboratory — UCBL — orthosis, physiotherapy with eccentric strengthening, and NSAIDs). The operation is chosen by stage and, above all, by whether the deformity is flexible or rigid.
Without intervention, flexible Stage II deformity progresses to rigid Stage III deformity requiring arthrodesis. Early surgical reconstruction with FDL transfer and MDCO in Stage II preserves hindfoot motion while correcting alignment, achieving 85-90% good outcomes in appropriately selected patients.
The one decision that matters — flexible versus rigid. Stand behind the patient and passively correct the heel valgus and arch collapse:
The deformity fully corrects passively, the subtalar and talonavicular joints are not arthritic, and the patient cannot perform a single heel raise. This is the candidate for soft-tissue reconstruction: FDL transfer plus MDCO, with lateral column lengthening or a Cotton osteotomy added as the deformity pattern demands.
The deformity cannot be fully corrected passively — the joints are fixed or arthritic. Soft-tissue reconstruction will fail. The answer is triple arthrodesis (talonavicular, subtalar and calcaneocuboid fusion), accepting loss of hindfoot motion.
Always examine the ankle in PTTD. Stage IV adds deltoid ligament incompetence with ankle valgus tilt. Palpate the deltoid, perform a valgus stress test, and obtain a mortise ankle view to measure the medial clear space (normal under 4 mm) and talar tilt. Triple arthrodesis alone will fail without addressing the ankle instability — Stage IV needs deltoid reconstruction or tibiotalocalcaneal (TTC) fusion.
Clinical assessment. Take a focused history (progressive medial ankle pain and swelling, difficulty on uneven ground and stairs, noticed flatfoot and shoe-wear changes, duration and response to orthoses) and examine from behind:
- Technique
- Patient stands on one leg and attempts to lift the heel
- Positive finding
- Unable to perform, or unable to invert the heel during the raise
- Significance
- PTTD Stage II or higher — cannot isolate heel inversion
- Technique
- Stand behind the patient, observe the feet
- Positive finding
- More than 1-2 toes visible lateral to the heel
- Significance
- Forefoot abduction (Stage IIb) — requires lateral column lengthening
- Technique
- With the patient sitting, manually correct heel valgus and arch
- Positive finding
- Deformity cannot be fully corrected
- Significance
- Rigid deformity (Stage III) — arthrodesis required
- Technique
- Apply valgus stress to the ankle with the knee flexed 30 degrees
- Positive finding
- Excessive medial opening, pain over the deltoid
- Significance
- Deltoid insufficiency (Stage IV) — address the ankle
Imaging for surgical planning. Obtain weight-bearing AP and lateral foot, and a hindfoot alignment view. Non-weight-bearing films underestimate the deformity. Key measurements: lateral talus-first metatarsal angle (normal 0-4 degrees, Stage II often 15-30 degrees), calcaneal pitch (normal 20-30 degrees, Stage II often under 15 degrees), and AP talus-first metatarsal angle (forefoot abduction when over 30 degrees). Add an ankle mortise view for Stage IV (medial clear space, talar tilt). MRI is not mandatory when the clinical and weight-bearing radiographic picture is clear, but confirms PTT pathology and spring ligament integrity when needed. Stress views confirm flexibility when the stage is uncertain.
The stage-based surgical algorithm translates the clinical and radiographic assessment into the operation:
- First-line treatment
- Conservative: UCBL orthosis, eccentric strengthening, NSAIDs for 6 months
- If conservative fails
- Debridement plus synovectomy (rare)
- Surgical goal
- Relieve tenosynovitis, prevent progression
- First-line treatment
- Orthosis and physiotherapy — most need surgery
- If conservative fails
- FDL transfer + MDCO
- Surgical goal
- Restore the tendon, correct heel valgus, preserve motion
- First-line treatment
- Conservative rarely succeeds
- If conservative fails
- FDL + MDCO + lateral column lengthening, plus Cotton osteotomy for IIc
- Surgical goal
- Correct the triplanar deformity (valgus, abduction, arch collapse)
- First-line treatment
- Accommodative orthosis, symptom control
- If conservative fails
- Triple arthrodesis
- Surgical goal
- Restore alignment, relieve pain, accept loss of hindfoot motion
- First-line treatment
- Conservative is ineffective
- If conservative fails
- Triple arthrodesis + deltoid reconstruction, OR tibiotalocalcaneal fusion
- Surgical goal
- Restore hindfoot AND ankle alignment
Consent specifically for 6 weeks of strict non-weight-bearing (the patient must have support at home), recurrent deformity in 10-15%, sural nerve injury from the lateral MDCO incision, wound problems, MDCO nonunion, and CRPS. Counsel that a long-term orthosis is usually recommended. Optimise risk factors first — weight, diabetes control, and smoking — since obesity (BMI over 35), diabetes and smoking predict failure.
The Operation
The goal of Stage II reconstruction is to replace the failed posterior tibial tendon with the FDL (active arch support) and correct the bony deformity with an MDCO (passive realignment that offloads the new tendon), adding lateral column lengthening for forefoot abduction and a Cotton osteotomy for residual forefoot varus. The medial exposure is laid out in full below (and in depth on the medial approach to the talus and navicular page).
Operative sequence — FDL transfer plus MDCO
- Supine on a standard table with a bump under the ipsilateral hip to internally rotate the leg — this brings the medial ankle and hindfoot into view and improves access to the PTT, the FDL harvest and the navicular.
- Knee flexed 30-40 degrees over padded support; sacrum, contralateral heel and all bony prominences padded.
- Thigh tourniquet to 300 mmHg (or limb occlusion pressure plus 100 mmHg) after elevation or Esmarch exsanguination; typical tourniquet time 90-120 minutes.
- Free-drape the foot to allow manipulation; position the C-arm for AP, lateral and oblique views.
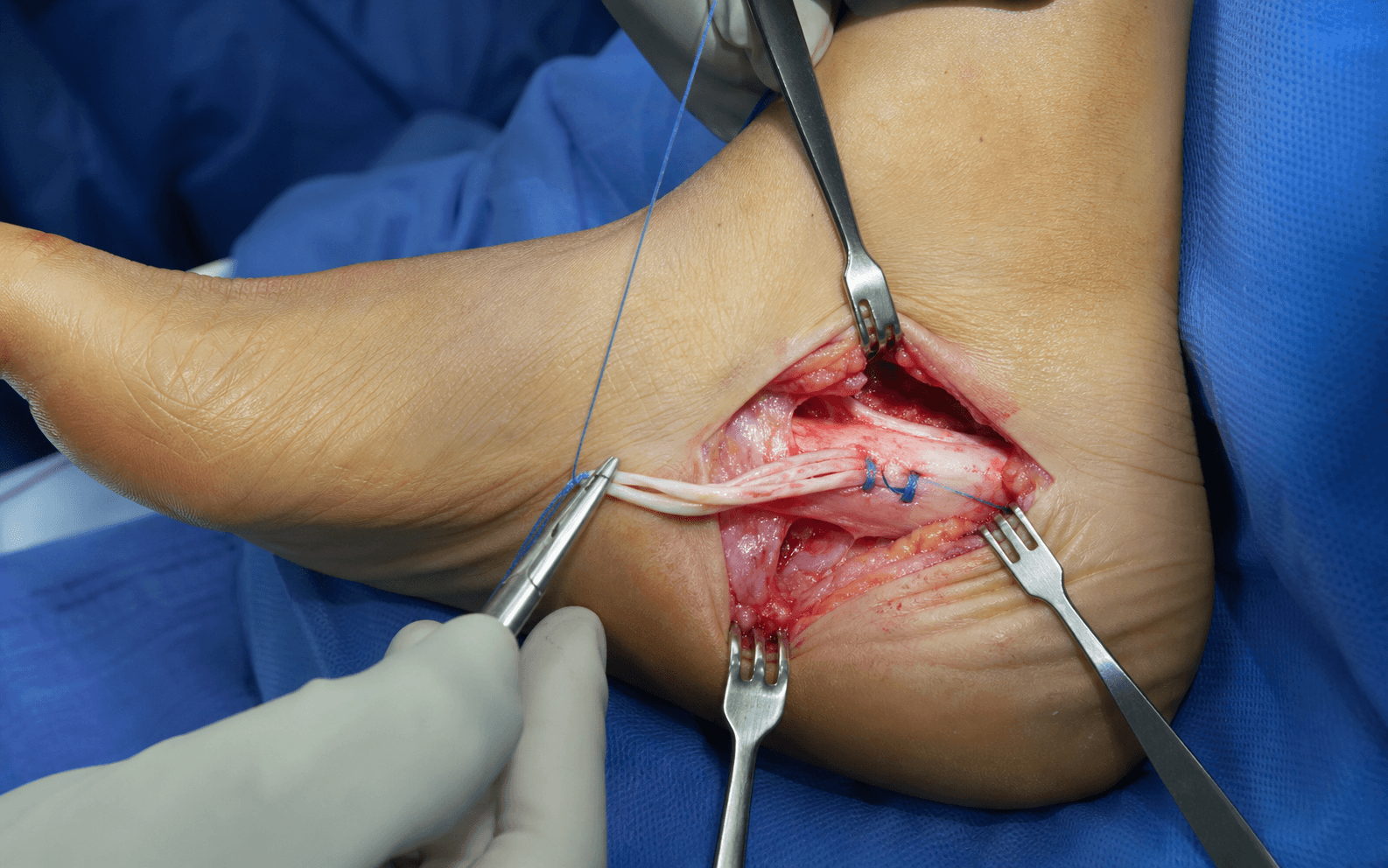
- A curvilinear medial incision starting about 8 cm proximal to the medial malleolus, curving posterior to the malleolus and extending distally to the navicular tuberosity (about 10-12 cm).
- This single incision exposes the PTT, the FDL in the tarsal tunnel and the navicular insertion.
- Protect the saphenous vein and nerve (anterior to the incision) and the posterior tibial neurovascular bundle (posterior, deep).
- Incise the flexor retinaculum to open the tarsal tunnel.
- Identify the PTT — the most superficial tendon in the tunnel — and follow it to its navicular insertion, noting whether it is attenuated, torn or ruptured.
- Identify the FDL deep to the PTT; the two share a common synovial sheath proximally. At the level of the sustentaculum tali they diverge — the PTT runs superficial and medial to the navicular, while the FDL continues distally and plantar.
- Excise grossly diseased PTT tissue. If a substantial remnant remains (Stage I-IIa), it can be used for a side-to-side anastomosis with the transferred FDL.
- Inspect the spring ligament complex (superomedial, inferoplantar and plantar components). If it is completely torn or severely attenuated, reconstruct it with a suture anchor repair or augmentation.
- Follow the FDL distally to the master knot of Henry, where it crosses superficial to the FHL in the midfoot.
- Make a small plantar incision over the FDL at this level and transect it distal to the knot of Henry; pull it proximally into the main incision (it strips from its insertions on the lateral four toes — expected, with minimal functional donor morbidity).
- Typical harvest length 12-15 cm.
- Expose the navicular tuberosity and the PTT insertion.
- Create a drill hole in a plantar-to-dorsal direction, starting just plantar to the PTT insertion and exiting the dorsal navicular.
- Drill size 6-8 mm to accommodate the tendon.
- Thread the FDL through the navicular tunnel from plantar to dorsal without kinking.
- Hold the foot in maximum plantarflexion and inversion (this restores the arch and sets the tension) and pull the tendon tight.
- Fix with an interference screw (preferred — compresses tendon against bone), a suture anchor on the dorsal navicular, or a bone tunnel with sutures tied over a dorsal bridge. Confirm the foot holds the arch under the tendon's tension.
- Through a separate 4-5 cm lateral oblique incision centred on the lateral calcaneus, starting 2 cm distal to the lateral malleolus — protect the sural nerve, which runs posterior to the incision.
- Elevate periosteum and mark the osteotomy 1.5-2 cm distal to the posterior calcaneal tuberosity, confirmed posterior to the calcaneocuboid joint on fluoroscopy.
- Cut perpendicular to the long axis of the calcaneus in the sagittal plane with a slight dorsal-to-plantar obliquity, completing the cut through the medial cortex.
- Translate the posterior fragment medially 10-12 mm (about 1 cm) with a bone clamp or laminar spreader — correct heel valgus to neutral or slight varus.
- Fix with two 6.5 mm or 7.0 mm partially threaded cancellous screws from lateral to medial under compression, confirming position on fluoroscopy.
- Lateral column lengthening (Evans) if the too many toes sign persists: osteotomy 1-1.5 cm proximal to the calcaneocuboid joint, distract 8-12 mm (keep to 8-10 mm to avoid calcaneocuboid overload), fill with a tricortical iliac crest allograft wedge and plate.
- Cotton osteotomy (medial cuneiform opening wedge) only if, with the hindfoot corrected, the medial column is plantarflexed (residual forefoot varus): dorsomedial incision, open-wedge osteotomy of the medial cuneiform, 4-8 mm graft.
- Release the tourniquet and achieve meticulous haemostasis; consider a drain for combination procedures.
- Close periosteum, deep fascia (2-0 absorbable) and subcutaneous (3-0 absorbable) without tension; skin with 3-0/4-0 nylon vertical mattress or running subcuticular.
- Apply a well-padded short leg splint in neutral ankle dorsiflexion and hindfoot neutral to slight varus, moulded to hold the arch.
Transecting the FDL proximal to the master knot of Henry sacrifices harvest length and risks disrupting the FHL, which crosses deep to the FDL at that point. Always harvest distal to the knot — the tendon then strips cleanly from its toe insertions as it is pulled proximally, and the loss of lateral-toe flexion is not functionally significant.
Foot and ankle surgery under tourniquet with multiple osteotomies raises compartment syndrome risk. Monitor for pain out of proportion, pain on passive toe stretch and a tense swollen foot. If suspected, release the splint immediately and measure pressures — foot compartment syndrome needs urgent fasciotomy of all nine compartments.
FDL transfer alone achieves only 60-70% success because the heel valgus persists and overpowers the tendon. MDCO alone cannot replace the lost tendon. Combined, FDL gives active dynamic arch support while MDCO shifts the ground reaction force medial to the ankle axis, converting the Achilles moment from eversion to inversion and offloading the reconstructed tendon — the synergy behind the 85-90% success rate.
- Anatomical detail
- Primary inverter and arch supporter; inserts on the navicular tuberosity
- Surgical significance
- Degenerates in PTTD — the structure being reconstructed or replaced
- Anatomical detail
- Deep to the PTT in the tarsal tunnel; inserts on the distal phalanges of toes 2-5
- Surgical significance
- The ideal transfer — similar vector, minimal donor morbidity
- Anatomical detail
- Superomedial, inferoplantar and plantar components supporting the talonavicular joint
- Surgical significance
- Often attenuated in PTTD — assess and reconstruct if torn
- Anatomical detail
- Medial calcaneal shelf supporting the talus
- Surgical significance
- Landmark where the PTT and FDL diverge
- Anatomical detail
- Crosses the lateral calcaneus posterior to the MDCO incision
- Surgical significance
- Most commonly injured nerve in MDCO — protect it
- Anatomical detail
- Superficial and deep medial ankle stabiliser
- Surgical significance
- Incompetent in Stage IV — ankle valgus tilt on the mortise view
- Indication
- Stage IIb/IIc — forefoot abduction (too many toes sign)
- Key technical points
- Osteotomy 1-1.5 cm proximal to the CC joint; distract 8-12 mm; tricortical graft plus plate
- Pearl and pitfall
- Over-distraction over 12 mm causes calcaneocuboid overload — keep to 8-10 mm
- Indication
- Residual forefoot varus after hindfoot correction (Stage IIc)
- Key technical points
- Opening wedge of the medial cuneiform, 4-8 mm graft, parallel to the first TMT joint
- Pearl and pitfall
- Only if the medial column is plantarflexed with the hindfoot corrected — do not overcorrect
- Indication
- Stage III — rigid fixed deformity
- Key technical points
- Fusion of talonavicular, subtalar and calcaneocuboid joints; correct heel to slight varus, restore the arch
- Pearl and pitfall
- Nonunion 10-15% (most often talonavicular); adjacent-joint arthritis 20-30% at 10 years
- Indication
- Stage IV without ankle arthritis
- Key technical points
- Triple arthrodesis plus deltoid reconstruction with allograft or semitendinosus autograft
- Pearl and pitfall
- Variable outcome, 60-70% success, risk of recurrent instability
- Indication
- Stage IV with established ankle valgus arthritis
- Key technical points
- Intramedullary nail from calcaneus through talus into tibia; correct valgus to neutral
- Pearl and pitfall
- Salvage procedure; 75-80% fusion; loss of ankle and hindfoot motion
Aftercare & Complications
Rehabilitation after FDL transfer plus MDCO. The 6-week non-weight-bearing period protects the FDL fixation (tendon-to-bone healing takes 6-8 weeks) while the MDCO unites.
Postoperative protocol — FDL transfer plus MDCO
- Well-padded short leg splint in neutral with the arch moulded; foot elevated above the heart for 48-72 hours.
- Strict non-weight-bearing with crutches or walker.
- Multimodal analgesia (consider a nerve block); DVT prophylaxis (aspirin 325 mg or LMWH if high risk); neurovascular checks.
- Keep the splint dry and intact; at week 2 convert to a well-moulded short leg cast maintaining the arch and neutral hindfoot.
- Continue strict non-weight-bearing for the full 6 weeks — the highest-risk period for FDL pullout and MDCO nonunion.
- Radiograph to confirm MDCO healing; transition to a removable CAM boot.
- Begin partial weight-bearing (25-50%) and gentle ankle range-of-motion exercises.
- Progress to full weight-bearing in the boot; begin strengthening (calf raises, resistance bands).
- Fabricate a custom UCBL or AFO orthosis for long-term support.
- Confirm complete MDCO healing; wean from the boot into a supportive shoe plus the custom orthosis.
- Progress strengthening, proprioception and gait; return to full activity at 4-6 months.
The FDL is fixed to the navicular with an interference screw or anchor; early weight-bearing can cause pullout before tendon-to-bone healing occurs at 6-8 weeks. The MDCO also needs 6-8 weeks for radiographic union. Patients who bear weight early have significantly higher rates of FDL failure and MDCO nonunion.
Rehabilitation after triple arthrodesis (Stage III). Non-weight-bearing in a short leg cast for 6 weeks, then progressive weight-bearing in a boot as bridging trabeculae appear (expect 80-90% union by 12 weeks), advancing to a supportive shoe by 12-16 weeks with return to activity at 6-9 months. Triple arthrodesis carries a 10-15% nonunion rate, most often at the talonavicular joint — revise a painful nonunion with iliac-crest autograft, rigid fixation and BMP augmentation. Complications — recognition, prevention, management
- Incidence
- 10-15% at 5 years
- Risk factors
- Inadequate MDCO shift, missed lateral column lengthening, obesity, non-compliance
- Management
- Mild: orthosis. Progressive: revision MDCO or conversion to triple arthrodesis
- Incidence
- 5-10%
- Risk factors
- MDCO translation over 12 mm, excessive lateral column lengthening
- Management
- Painful lateral foot — medial opening wedge calcaneal osteotomy or lateral column shortening
- Incidence
- 5-10%
- Risk factors
- Smoking, diabetes, inadequate fixation, excessive translation
- Management
- Asymptomatic: observe. Painful: revision ORIF with bone graft, consider BMP
- Incidence
- 5-8%
- Risk factors
- Inadequate fixation, pullout from the navicular, tendon rupture
- Management
- Re-transfer with stronger fixation, or convert to triple arthrodesis
- Incidence
- 2-5% temporary, 1% permanent
- Risk factors
- MDCO lateral incision — the nerve crosses the field
- Management
- Prevention by careful dissection; most recover; neurolysis if persistent
- Incidence
- 5-10%
- Risk factors
- Poor soft-tissue handling, smoking, diabetes
- Management
- Superficial: local care. Deep: debridement, VAC, possible flap
- Incidence
- 2-5%
- Risk factors
- More common after foot and ankle surgery
- Management
- Early aggressive therapy, desensitisation, gabapentin, sympathetic block
- Incidence
- Under 1%
- Risk factors
- FDL transfer — nerve and artery in the tarsal tunnel
- Management
- Meticulous dissection; nerve injury usually recovers, arterial injury needs repair
The most common cause of recurrence after FDL plus MDCO is inadequate correction at the index operation: assess the deformity in all three planes, add lateral column lengthening when the too many toes sign is present, translate the calcaneus a measured 10-12 mm, tension the FDL in plantarflexion and inversion, and enforce strict 6-week non-weight-bearing with long-term orthosis use.
Outcomes. FDL plus MDCO gives 85-90% good or excellent results with preservation of about 81% of subtalar motion and restoration of the single-leg heel rise; adding lateral column lengthening yields 80-85%. Triple arthrodesis gives 80-85% pain relief but sacrifices hindfoot motion, with adjacent-joint arthritis in 20-30% at 10 years. TTC fusion (Stage IV) is a salvage with 75-80% fusion and significant functional limitation. Long term, 80-85% of FDL-plus-MDCO patients maintain correction at 5 years.
Obesity (BMI over 35), diabetes, smoking, advanced Stage IIc triplanar deformity, non-compliance with non-weight-bearing, and underlying inflammatory arthritis all predict failure. Patients with several of these may be better served by a primary triple arthrodesis than an attempted soft-tissue reconstruction.
Viva & Exam Focus
SHIFTFDL Transfer Technique Steps
Hook:SHIFT the FDL from toe flexion to arch support — transfer the work!
CALCANEUSMDCO Indications and Effects
Hook:The CALCANEUS shift corrects heel valgus without fusion!
At what landmark should the FDL be transected to maximise harvest length while minimising donor morbidity? Distal to the master knot of Henry — the crossing where the FDL passes superficial to the FHL. Transecting distal to it lets the tendon be pulled proximally, stripping from the lateral four toes with minimal functional loss; transecting proximal to it sacrifices length and risks the FHL.
A patient has medial arch collapse and heel valgus that fully corrects on passive manipulation. This is Stage II — flexible flatfoot deformity — treated with FDL transfer plus MDCO (plus lateral column lengthening if forefoot abduction is present). A rigid, non-correctable deformity is Stage III and needs triple arthrodesis.
MDCO shifts the ground reaction force medial to the ankle joint axis, converting the Achilles moment from an eversion moment to an inversion moment. This passive correction offloads the reconstructed FDL. Without MDCO, FDL transfer alone achieves only 60-70%; combined, 85-90%.
The too many toes sign (more than 1-2 toes visible from behind) indicates forefoot abduction — a transverse-plane deformity classifying the patient as Stage IIb if flexible. Planning must include lateral column lengthening (Evans osteotomy or calcaneocuboid distraction arthrodesis) alongside the FDL transfer and MDCO, or the deformity will recur.
Stage IV adds deltoid ligament insufficiency with ankle valgus tilt to the rigid flatfoot of Stage III. On the mortise view the medial clear space is over 4 mm with talar tilt. Triple arthrodesis alone fails — management must address both hindfoot and ankle with triple plus deltoid reconstruction (no ankle arthritis) or tibiotalocalcaneal fusion (ankle arthritis present). Stage IV has the worst prognosis.
The most common cause of recurrent deformity after FDL plus MDCO is inadequate correction at the index operation: MDCO translation under 10 mm, a missing lateral column lengthening in a Stage IIb patient, or inadequate FDL tensioning — compounded by non-compliance, obesity and disease progression. Prevention needs adequate correction in all three planes and strict postoperative non-weight-bearing.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old obese woman has two years of progressive medial ankle pain and flatfoot, failing six months of UCBL orthosis and physiotherapy. She has heel valgus, medial arch collapse, cannot perform a single heel raise, and has a too many toes sign. Standing films show 15 degrees of hindfoot valgus and an AP talus-first metatarsal angle of 25 degrees, and the deformity is fully correctable passively. How do you manage her?”
“Walk me through your technique for a medial displacement calcaneal osteotomy — the key steps, how you assess adequate correction, and the pitfalls.”
“A 58-year-old has long-standing flatfoot with medial ankle pain. The heel is in valgus and the arch is collapsed, but when you passively correct it the heel valgus only partially corrects. How does this influence your management, and what would you recommend?”
Key anatomy
- FDL runs DEEP to the PTT in the tarsal tunnel — the ideal transfer donor
- Master knot of Henry = FDL crosses superficial to FHL — harvest the FDL distal to it
- Sustentaculum tali = the landmark where the PTT and FDL diverge
- Spring ligament complex supports the talonavicular joint — often torn, may need reconstruction
- Sural nerve crosses the lateral calcaneus — at risk in MDCO
Classification — Johnson and Strom
- Stage I = tenosynovitis, normal alignment = conservative, plus debridement if it fails
- Stage II = FLEXIBLE flatfoot = FDL plus MDCO, plus lateral column lengthening as needed
- Stage III = RIGID flatfoot = triple arthrodesis
- Stage IV = Stage III plus ankle valgus tilt (deltoid insufficiency) = triple plus deltoid reconstruction or TTC fusion
- KEY TEST: passive correction = flexible (II) versus rigid (III)
Surgical algorithm
- Stage IIa (valgus only): FDL transfer plus MDCO
- Stage IIb (valgus plus abduction/too many toes): FDL plus MDCO plus lateral column lengthening
- Stage IIc (plus forefoot varus): add a Cotton osteotomy
- FDL harvest: transect distal to the knot of Henry, transfer to the navicular through a drill hole
- MDCO: 10-12 mm medial translation, 1.5-2 cm distal to the tuberosity, fix with two screws
Surgical pearls
- Combination FDL plus MDCO = 85-90% success (FDL alone = 60-70%)
- MDCO shifts ground reaction force medially — converts the Achilles from eversion to inversion
- Protect the sural nerve during MDCO (posterior to the lateral incision)
- Assess the spring ligament intraoperatively — reconstruct if torn
- Tension the FDL with the foot in plantarflexion and inversion to restore the arch
Complications
- Undercorrection/recurrence: 10-15% — most often inadequate MDCO translation or a missing LCL in Stage IIb
- Overcorrection/cavovarus: 5-10% — MDCO over 12 mm or excessive LCL
- MDCO nonunion: 5-10% — smoking, diabetes, inadequate fixation
- Sural nerve injury: 2-5% temporary, 1% permanent — protect during MDCO
- FDL transfer failure: 5-8% — navicular pullout, inadequate fixation
Key evidence
- FDL plus MDCO: AOFAS improved 48.8 to 88.5, good or excellent in 43 of 44 at mean 51 months (Wacker and Saxby 2002)
- FDL plus MDCO restores the single-leg heel rise and preserves about 81% subtalar motion (Guyton 2001)
- The transferred FDL hypertrophies (plus 27% volume) as the posterior tibial muscle atrophies — the biology of the transfer (Rosenfeld and Saxby 2005)
- Triple arthrodesis: all ankles show degenerative change at long-term follow-up, yet 95% remain satisfied (Saltzman 1999)
- Lateral column lengthening plus medial reconstruction corrects forefoot abduction; the main hazard is calcaneocuboid overload (Hintermann 1999)
Background & Evidence
Epidemiology. PTTD is the most common cause of acquired adult flatfoot deformity. It typically presents in active adults aged 40-60 years with a strong female predominance (about 9 to 1). Risk factors include obesity (BMI over 30), diabetes, hypertension and steroid use, and 10-20% have contralateral involvement. Without treatment, roughly half of Stage I feet progress to Stage II within 2-5 years, and 30-40% of Stage II feet develop rigidity. Classification. Johnson and Strom described Stages I to III in 1989; Myerson added Stage IV (ankle valgus from deltoid failure) in 1997, and examiners worldwide still expect this four-stage framework. A 2020 international consensus renamed the condition Progressive Collapsing Foot Deformity (PCFD) and replaced staging with a flexible-or-rigid classification (Classes 1 to 5 by deformity component A to E). State that you are aware of both and lead with Johnson and Strom unless asked for the current consensus; all systems hinge on the flexible-versus-rigid distinction that decides joint-sparing reconstruction versus arthrodesis.
- Clinical findings
- Medial ankle pain and PTT tenderness, normal alignment, able to perform a single heel raise
- Radiographic findings
- Normal alignment, no deformity
- Treatment
- Conservative (orthosis, physiotherapy), plus debridement if it fails at 6 months
- Clinical findings
- Flatfoot deformity, heel valgus, too many toes sign, passively correctable, unable to perform a single heel raise
- Radiographic findings
- Hindfoot valgus, medial arch collapse, forefoot abduction (AP talus-first MT angle over 30 degrees), flexible on stress views
- Treatment
- FDL transfer plus MDCO, plus lateral column lengthening or Cotton osteotomy as needed
- Clinical findings
- Fixed flatfoot deformity, not passively correctable, rigid hindfoot valgus, arthritic change
- Radiographic findings
- Rigid hindfoot valgus, triple-joint arthritis, fixed forefoot abduction, no correction on stress views
- Treatment
- Triple arthrodesis (talonavicular, subtalar, calcaneocuboid fusion)
- Clinical findings
- All Stage III findings plus ankle pain, deltoid tenderness, ankle instability
- Radiographic findings
- All Stage III findings plus ankle valgus tilt on the mortise view (medial clear space over 4 mm, talar tilt)
- Treatment
- Triple arthrodesis plus deltoid reconstruction, or tibiotalocalcaneal fusion
- Deformity pattern
- Hindfoot valgus only, no forefoot abduction
- Surgical approach
- FDL transfer plus MDCO
- Deformity pattern
- Hindfoot valgus plus forefoot abduction (too many toes sign)
- Surgical approach
- FDL plus MDCO plus lateral column lengthening (Evans or calcaneocuboid distraction)
- Deformity pattern
- Hindfoot valgus plus forefoot abduction plus medial column instability
- Surgical approach
- FDL plus MDCO plus lateral column lengthening plus Cotton osteotomy
Pathophysiology and biomechanics. The posterior tibial tendon inverts the heel during stance, locks the transverse tarsal (Chopart) joint to form a rigid lever, and maintains the medial longitudinal arch. When it fails, the heel drifts into valgus (ground reaction force falls lateral to the ankle), the transverse tarsal joint unlocks, the arch collapses and the forefoot abducts (the too many toes sign). The FDL is the ideal transfer because it runs deep to the PTT in the tarsal tunnel on a similar vector with minimal donor morbidity; the MDCO complements it by shifting the ground reaction force medial to the ankle axis, converting the Achilles moment from eversion to inversion and offloading the reconstructed tendon.
- VTE prophylaxis: individualised risk assessment; NICE (UK) and AAOS/ACCP (US) support mechanical prophylaxis with or without aspirin or LMWH for major hindfoot surgery, with no universal mandate for low-risk isolated foot surgery. - Antibiotic prophylaxis: a first-generation cephalosporin (for example cefazolin) within 60 minutes of incision per WHO and SIGN guidance. - Diabetes optimisation: multidisciplinary perioperative glycaemic control before elective reconstruction reduces wound and nonunion risk. - Registries: no national joint registry tracks PTTD soft-tissue reconstruction (NJR, AJRR, AOANJRR, SHAR cover arthroplasty); evidence rests on cohort series.
- Document at least 6 months of failed conservative care before surgery. - Record the passive correction test, the too many toes sign and the radiographic measurements to justify procedure selection. - Counsel on success rates, the 6 weeks of non-weight-bearing, recurrence risk, sural nerve injury and the alternatives. - Document discussion of obesity, diabetes and smoking as risk factors; consider deferring surgery until they are optimised. - Common litigation issues: sural nerve injury, recurrence from inadequate correction or wrong procedure selection, missed compartment syndrome, and infection in diabetic patients.
References
Calcaneal Osteotomy plus FDL Transfer for Stage II PTTD: 3-5 Year Results
- Prospective series of 51 patients with classical Johnson and Strom Stage II PTTD treated with MDCO plus FDL transfer; 44 reviewed at mean 51 months
- Mean AOFAS ankle-hindfoot score improved from 48.8 pre-operatively to 88.5 at follow-up
- Good to excellent for pain and function in 43 of 44 patients; good to excellent alignment in 36 with no poor results
- Only 2 patients failed and required calcaneocuboid fusion
FDL Transfer plus MDCO Preserves Subtalar Motion: Middle-Term Follow-Up
- Retrospective review of 26 patients after FDL transfer plus MDCO, mean 32 months follow-up
- All but 3 patients could perform a single-leg heel rise post-operatively — a manoeuvre none could do pre-operatively
- Subtalar motion preserved at 81 percent of the contralateral side, confirming the procedure spares hindfoot motion
- Pain relief rated excellent in 75 percent and good in 16 percent; the 2 early failures were both loss of FDL fixation
Lateral Column Lengthening plus Medial Soft-Tissue Reconstruction for Flatfoot
- 19 patients with Stage II / II-III PTTD treated by lengthening the lateral column via a calcaneal (Evans-type) osteotomy plus medial soft-tissue reconstruction (FDL transfer, deltoid and spring ligament repair)
- All achieved restoration of the medial longitudinal arch and reduction of forefoot abduction at mean 23 months
- Result excellent in 6, good in 11, fair in 2; all but one patient satisfied
- 1 calcaneocuboid joint required arthrodesis for painful degeneration — the principal hazard of lateral column lengthening
Triple Arthrodesis: 25- and 44-Year Average Follow-Up
- 67 feet (57 patients) reviewed at average 25 and again at 44 years after triple arthrodesis (mostly neuromuscular or post-polio deformity)
- By the second review ALL ankles had radiographic degenerative change, with progressive arthritis also at the naviculocuneiform and tarsometatarsal joints
- Painful feet and ankles rose from 45 percent to 55 percent and the proportion needing walking support rose from 32 percent to 68 percent over time
- Despite progressive degeneration, 54 of 57 patients (95 percent) remained satisfied with the result
Muscle Response to FDL Transfer plus MDCO: Why the Transfer Works
- Prospective MRI volumetric study of 12 patients before and about 13 months after FDL transfer plus MDCO for Stage II PTTD
- FDL muscle hypertrophied (mean plus 27 percent volume) after transfer while the failing posterior tibial muscle continued to atrophy (minus 23 percent)
- AOFAS hindfoot score improved from 50 to 88 at one year
- Outcome was equivalent whether the diseased posterior tibial tendon was excised or left intact