Transosseous repair through patellar tunnels with a Krackow locking suture technique
- Quadriceps tendon rupture affects older patients (over 40) with medical comorbidities; patellar tendon rupture affects younger (under 40) athletic patients — the lateral radiograph shows patella BAJA versus patella ALTA.
- Complete ruptures need early surgical repair, ideally within two weeks; delay is the dominant modifiable predictor of a poor result.
- Transosseous tunnel repair is the historic reference standard and the safe default in the typical elderly, osteopenic patient; high-strength suture-anchor repair is an equal-strength alternative in good-quality bone.
- Tension the repair in FULL EXTENSION, then confirm 90 degrees flexion is achievable without gapping — over-tensioning causes stiffness, under-tensioning causes extensor lag.
- Augment (for example with a semitendinosus autograft) for chronic ruptures (over 2 to 3 weeks), poor tissue quality, or revision — primary repair alone in these settings carries a high failure rate.
When & Why
Indication. Surgical repair is for a complete quadriceps tendon rupture — the classic triad of acute pain, impaired active knee extension, and a palpable suprapatellar gap, with a positive inability to straight-leg-raise against gravity. Partial tears with preserved active extension can be managed non-operatively in a brace; complete ruptures do poorly without surgery. The diagnosis is usually clinical, and MRI is reserved for ambiguous cases (for example an obese patient, a suspected partial tear, or pre-operative planning of a chronic retracted stump). Timing matters. Repair is best performed early — ideally within two weeks. The systematic-review evidence (Ciriello) shows that delayed repair is the dominant modifiable predictor of a poor outcome, because the quadriceps muscle retracts and the tendon stump becomes atrophic and fatty. Bilateral ruptures, and ruptures in patients with renal disease, are often delayed because the presentation is missed. The one decision — transosseous, anchor, or augment. Every repair begins by re-attaching the tendon to a bleeding patellar bed. The fixation choice is driven by bone quality, not dogma:
The reference standard and the safe default in the typical elderly, osteopenic patient. Three patellar tunnels with a Krackow locking suture. Biomechanically the strongest construct in low-density bone.
Faster, with less patellar dissection. An equal-strength alternative at physiological loads in young patients with good bone, but lower pull-out strength in osteoporotic bone.
Required for chronic ruptures (over 2 to 3 weeks), poor tissue quality, or revision. Semitendinosus autograft woven in a figure-of-eight through the tunnels provides load-sharing during healing.
Consent specifically for infection (around 2 to 3 percent superficial, under 1 percent deep), re-rupture (about 2 percent pooled, higher with diabetes and delayed repair), knee stiffness (10 to 20 percent), extensor lag (15 to 25 percent), patellar fracture (1 to 2 percent), and infrapatellar nerve numbness. Setup. Supine on a radiolucent table with a small bump under the knee for slight flexion, a non-sterile thigh tourniquet inflated to 300mmHg after exsanguination, and fluoroscopy available for tunnel placement if needed. A single dose of perioperative antibiotics is given.
The Operation
The goal is to re-attach the retracted quadriceps tendon to a bleeding superior-patellar bed through a midline exposure, secure it with a Krackow locking suture passed through three transosseous tunnels, tension it in full extension, repair the retinaculum, and confirm a competent straight-leg-raise before closing. The exposure is laid out in full as the first steps below.
Operative sequence
- Supine on a radiolucent table with a small bump under the knee for 10 to 20 degrees of flexion.
- Non-sterile thigh tourniquet inflated to 300mmHg after exsanguination; fluoroscopy available.
- Mark a midline longitudinal incision from mid-thigh to the tibial tubercle (15 to 20cm) so the retracted proximal stump can be reached.
- Carry the midline incision through skin and subcutaneous tissue down to the extensor mechanism.
- Identify the retracted proximal tendon stump, which may lie 5 to 10cm proximal in complete ruptures because of quadriceps muscle contraction — extend proximally if it is not immediately visible.
- Evacuate the suprapatellar haemarthrosis and irrigate thoroughly; assess the medial and lateral retinacular tears that commonly accompany the rupture.
- Debride frayed, necrotic tissue back to healthy, bleeding tendon with a visible longitudinal collagen-fibre pattern.
- Preserve as much length as possible; poor-quality yellow, friable or fatty tissue signals the need for augmentation.
- In chronic ruptures the stump is contracted and must be mobilised proximally to restore length.
- Decorticate the superior pole of the patella with a rongeur or burr to expose bleeding cancellous bone — the healing surface for tendon-to-bone incorporation (the same principle as rotator-cuff footprint preparation).
- Mark three tunnel positions — central, medial and lateral — spaced at least 10mm apart.
- Drill three longitudinal tunnels with a 2.5 to 3mm drill from the superior pole toward the mid-patella, NOT through the articular surface.
- Use a curette to create a gentle curve so each tunnel exits anteriorly on the inferior patella.
- Pass a looped suture retriever through each tunnel from inferior to superior.
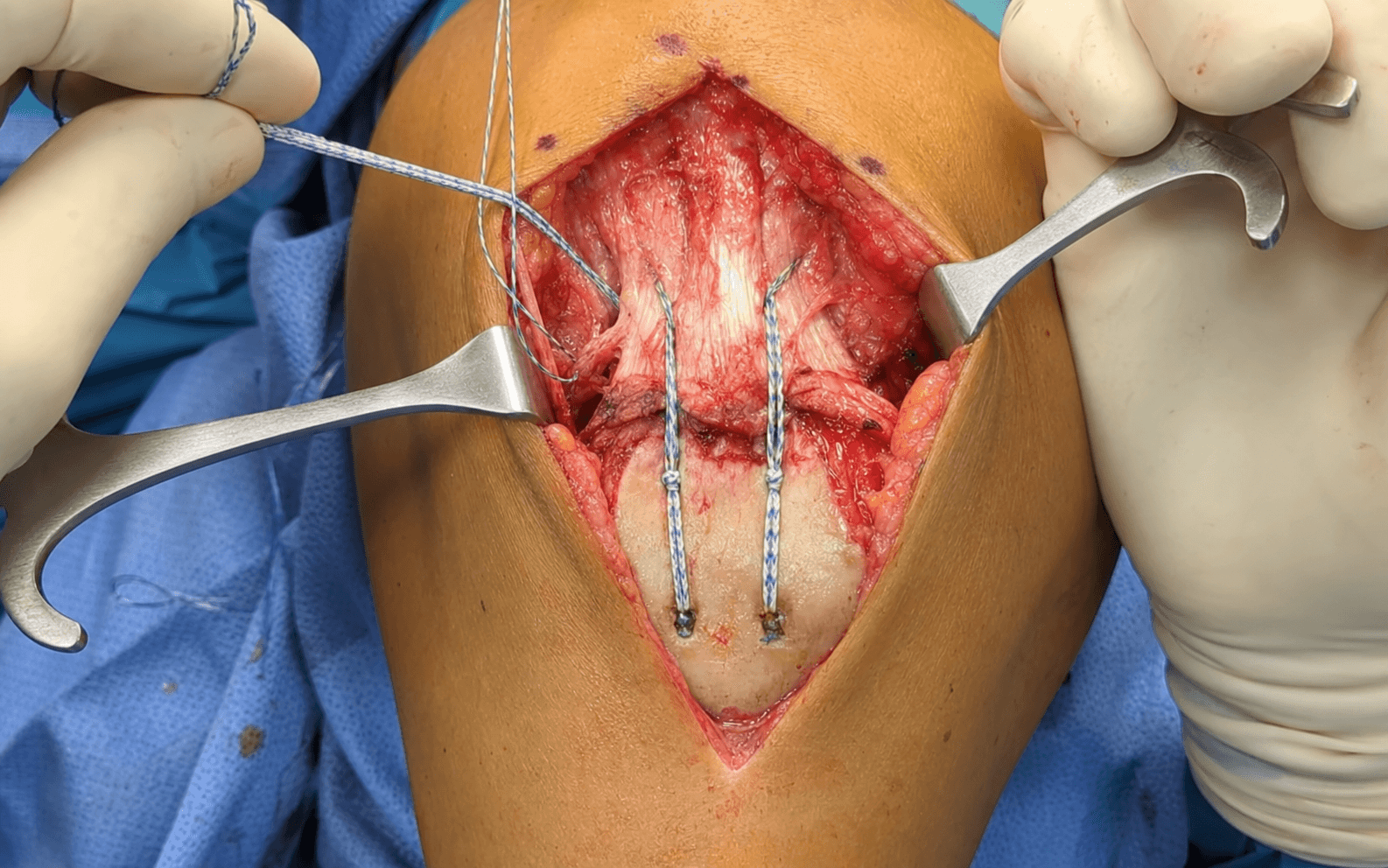
- Place Krackow locking sutures in the quadriceps tendon stump using heavy non-absorbable suture (number 2 or number 5 Ethibond or FiberWire).
- The interlocking loops grip the tendon and resist pulling through under tension; each passage takes roughly a 5mm bite.
- Use three sutures, one for each tunnel.
- Pass the suture limbs through the patellar tunnels using the retrievers and reduce the stump onto the decorticated surface.
- With the knee in FULL EXTENSION, sequentially tension and tie the sutures over a bone bridge at the inferior patella.
- Confirm tendon-to-bone apposition and that 90 degrees of passive flexion is achievable without repair gapping — if it gaps, the repair is too tight and will cause stiffness.
- Palpate systematically along both sides of the patella and repair the medial and lateral retinacular tears with interrupted sutures.
- Close in layers — synovium and capsule first, then the retinaculum. Unrepaired defects cause persistent weakness despite an intact tendon repair.
- Take care on the lateral side to avoid the infrapatellar branch of the saphenous nerve.
- Test an active straight-leg-raise to confirm repair integrity — if the patient cannot, the repair is inadequate and needs augmentation or revised fixation before closing.
- Verify passive range of motion to 90 degrees flexion; close the suprapatellar pouch watertight if it was violated.
- Irrigate and close in layers over a drain; apply a hinged knee brace locked in extension.
Transosseous tunnels concentrate stress in the patella, which is often osteoporotic in this elderly population. Prevent fracture by spacing the three tunnels at least 10mm apart and using a small (2.5 to 3mm) drill without excessive force. Aim each tunnel to exit anteriorly on the inferior pole, never through the articular surface — use fluorospy if the trajectory is unclear. If you breach the joint, abandon that tunnel, irrigate to clear debris, and re-drill in a corrected position; document the cartilage injury and counsel the patient about future patellofemoral arthritis.
At physiological loads in good-quality bone, modern high-strength suture-anchor constructs perform comparably to transosseous tunnels, and anchors need less peripatellar dissection. But the typical quadriceps-rupture patient is elderly and osteopenic, and in low bone-mineral-density bone transosseous suture is mechanically more reliable and its performance is independent of bone quality. The honest viva answer is: both are acceptable; I default to transosseous tunnels in the osteoporotic patient and consider anchors in a younger patient with good bone.
- Advantages
- Biological, minimal donor morbidity at the knee
- Disadvantages
- Hamstring weakness
- Advantages
- Strong, immediate load-sharing, no harvest morbidity
- Disadvantages
- Foreign body, cost
- Advantages
- Large graft, no donor morbidity
- Disadvantages
- Disease-transmission risk, cost
- Advantages
- Load-sharing, inexpensive
- Disadvantages
- Foreign-body reaction
- Advantages
- Simple
- Disadvantages
- Wire breakage, palpable, outdated
For chronic ruptures (over 2 to 3 weeks) the native tendon is usually contracted and of poor quality, so primary repair alone has a high failure rate. Harvest the semitendinosus through a separate anteromedial incision, weave it in a figure-of-eight through the patellar tunnels, and suture it to the native stump to provide load-sharing during healing. Synthetic tape augmentation is a reasonable alternative for immediate load-sharing without harvest morbidity.
The knee joint communicates with the field once the tendon retracts. Protect it, and close it watertight — violation causes haemarthrosis and increases infection risk.
Crosses the field obliquely from medial to lateral 3 to 5cm below the joint line, at risk during lateral retinacular exposure. Injury numbs the anterolateral knee.
A branch of the femoral artery running with the saphenous nerve medially, at risk during medial retinacular exposure — control with electrocautery before retraction.
At risk of drill penetration when creating the tunnels. Aim tunnels to the inferior pole and use fluoroscopy if unsure.
At risk of fracture during drilling, especially in osteoporotic bone. Use a 2.5 to 3mm drill, three tunnels at least 10mm apart, and avoid bicortical drilling on the articular side.
Aftercare & Complications
Rehabilitation | Phase | Timing | Brace & weight-bearing | Therapy | |-------|--------|------------------------|---------| | 1 | Weeks 0 to 2 | Hinged brace LOCKED IN EXTENSION for weight-bearing and sleep; full weight-bearing in the locked brace | Passive ROM 0 to 30 degrees only; quadriceps isometrics and straight-leg-raise in the brace | | 2 | Weeks 2 to 6 | Brace continues for weight-bearing | Progressive passive ROM, increasing 10 to 15 degrees per week toward 90 degrees by week 6; active-assisted ROM | | 3 | Weeks 6 to 12 | Unlock the brace for ambulation once 90 degrees flexion is achieved; wean by week 8 to 10 | Begin active extension; progressive strengthening | | 4 | Months 3 to 6 | None | Full ROM; progressive resistance; return to activity at 4 to 6 months once strength is over 80 percent of the other side |
Over-tensioning the repair is the commonest cause of a stiff knee (and secondary patella baja); under-tensioning causes extensor lag. The intra-operative test — full extension for tensioning, then confirm 90 degrees flexion without gapping — is what balances the two. Early passive ROM within the brace protects the repair while limiting adhesions.
Complications
- Recognition
- Loss of active extension, palpable gap, inability to straight-leg-raise
- Prevention
- Secure Krackow fixation, correct tensioning, protected rehab, avoid early active extension
- Management
- Early: revision repair with augmentation. Late (over 6 weeks): reconstruction
- Recognition
- Flexion under 90 degrees at 3 months, painful limited ROM
- Prevention
- Correct tensioning (test 90 degrees flexion intra-operatively), early passive ROM, avoid over-tensioning
- Management
- Physiotherapy; manipulation under anaesthesia at 6 to 8 weeks if under 70 degrees; arthroscopic lysis if refractory
- Recognition
- Inability to fully extend against gravity, quadriceps weakness
- Prevention
- Avoid under-tensioning, repair retinacular tears, start active extension when healed
- Management
- Usually improves with therapy; consider revision if a lag over 10 degrees persists
- Recognition
- Intra-operative visible crack; post-operative pain, crepitus, failed extension
- Prevention
- Space tunnels over 10mm apart, use a 2.5mm drill, avoid excessive force, assess bone quality
- Management
- Intra-operative: ORIF with cerclage. Post-operative: management depends on displacement
- Recognition
- Erythema, drainage, fever, elevated CRP or ESR
- Prevention
- Peri-operative antibiotics, meticulous haemostasis, a drain for a large haemarthrosis
- Management
- Superficial: oral antibiotics. Deep: washout, IV antibiotics, hardware removal if needed
- Recognition
- Numbness over the anterolateral knee and proximal tibia
- Prevention
- Careful lateral retinacular dissection, identify the nerve branches
- Management
- Usually sensory only — reassurance; a painful neuroma may need excision
Viva & Exam Focus
QUADRICEPSQUADRICEPS — risk factors for rupture
Hook:Quadriceps rupture is more common in older patients (over 40) with medical comorbidities; patellar tendon rupture is more common in younger, athletic patients (under 40). This demographic split is a classic exam question.
REPAIRREPAIR — the operative sequence
Hook:Transosseous repair is the gold standard — heavy non-absorbable sutures (number 2 or 5 Ethibond or FiberWire) with a Krackow locking configuration through three bone tunnels.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old diabetic man presents after stumbling down stairs. He has a palpable defect above the patella and cannot perform a straight-leg-raise. The lateral radiograph shows patella baja. How do you manage this patient?”
“You are repairing a quadriceps tendon rupture and the tissue quality is poor, with fatty infiltration. The rupture occurred four weeks ago. What are your concerns and how do you modify your approach?”
“While drilling your second transosseous tunnel in the patella you feel the drill break through and see fluid egress from the joint. What has happened and how do you manage it?”
Key demographics
- Quadriceps rupture: OLDER (over 40), patella BAJA, risk factors (diabetes, CRF, steroids, fluoroquinolones)
- Patellar tendon rupture: YOUNGER (under 40), patella ALTA, athletic population
- Quadriceps rupture predominates over age 40; patellar tendon rupture predominates under age 40
Reference technique
- TRANSOSSEOUS repair through three patellar tunnels (default in osteopenic bone)
- High-strength suture-anchor or suture-tape repair is an equal-strength alternative in good bone
- Krackow locking suture in the tendon stump (number 2 or 5 non-absorbable)
- Tension in FULL EXTENSION — confirm 90 degrees flexion achievable without gapping
- REPAIR the medial and lateral retinacular tears
Augmentation indications
- Chronic ruptures (over 2 to 3 weeks)
- Poor tissue quality (fatty, friable)
- Revision repairs
- Options: semitendinosus autograft (preferred), synthetic tape, allograft
Critical danger zones
- Suprapatellar pouch — haemarthrosis, close watertight
- Patella — fracture risk during drilling (space tunnels over 10mm)
- Articular surface — avoid drill penetration
- Infrapatellar branch of the saphenous nerve — during lateral retinacular dissection
Complications
- Re-rupture about 2 percent pooled (higher with diabetes, chronic or delayed repair; augment chronic ruptures)
- Stiffness 10 to 20 percent (avoid over-tensioning)
- Extensor lag 15 to 25 percent (repair the retinaculum, correct tension)
- Patellar fracture 1 to 2 percent (space tunnels over 10mm)
Exam tips
- Default to TRANSOSSEOUS tunnels but frame the choice around BONE QUALITY, not dogma
- Know the QUADRICEPS mnemonic for risk factors
- Suture anchors are comparable at physiological loads in good bone; transosseous wins in osteoporotic bone
- Augmentation is NOT optional for chronic ruptures
Background & Evidence
Epidemiology. Quadriceps tendon rupture is an injury of older patients (over 40), typically with underlying medical disease. The Ciriello systematic review pooled 319 patients with a mean age of 57 years (range 16 to 85); the commonest mechanism was a simple fall (61.5 percent). Most tears occur 1 to 2cm proximal to the superior pole of the patella, or at the osseotendinous junction in older patients. Bilateral spontaneous rupture is a red flag for systemic disease — classically gout, diabetes or steroid use. Quadriceps versus patellar tendon rupture. The demographic and radiographic contrast is a perennial exam question — the two injuries affect opposite ends of the extensor mechanism and opposite populations:
- Quadriceps tendon rupture
- Older patients (over 40)
- Patellar tendon rupture
- Younger patients (under 40)
- Quadriceps tendon rupture
- Eccentric contraction against a contracting quadriceps (a stumble or fall)
- Patellar tendon rupture
- Athletic activity, jumping
- Quadriceps tendon rupture
- Diabetes, chronic renal failure, steroids, fluoroquinolones
- Patellar tendon rupture
- Previous surgery, tendinopathy, steroid injection
- Quadriceps tendon rupture
- 1 to 2cm proximal to the superior pole of the patella
- Patellar tendon rupture
- Inferior pole of the patella
- Quadriceps tendon rupture
- Patella BAJA (low riding)
- Patellar tendon rupture
- Patella ALTA (high riding)
- Quadriceps tendon rupture
- Above the patella
- Patellar tendon rupture
- Below the patella
- Quadriceps tendon rupture
- Predominates over age 40
- Patellar tendon rupture
- Predominates under age 40
- Quadriceps tendon rupture
- More common (especially in chronic renal failure)
- Patellar tendon rupture
- Less common
Pathoanatomy. Degenerative changes (fatty infiltration, micro-tears, poor vascularity) accumulate at the osseotendinous junction with age and systemic disease, so the tendon fails there under a sudden eccentric load. Once it ruptures, the quadriceps retracts proximally and, with time, the stump shortens, atrophies and turns fatty — which is why delayed repair does badly and why augmentation becomes necessary. The biomechanical debate. Cadaveric evidence consistently favours transosseous suture in low-density bone: the Nice-knot-augmented transosseous construct failed at roughly twice the load of a knotless anchor construct (Duell), and transosseous suture outlasted anchors in cyclic loading and load-to-failure in osteoporotic bone (Seggewiss). But at physiological loads in non-osteoporotic bone the two techniques displace near-identically (Lighthart), which is why the choice is driven by bone quality rather than dogma. The clinical systematic review (Ciriello) found the type of repair did not significantly change outcome, but re-rupture after timely primary repair was low (about 2 percent).
References
Full reference list 1. Ciriello V, Gudipati S, Tosounidis T, et al. Clinical outcomes after repair of quadriceps tendon rupture: a systematic review. Injury. 2012;43(11):1931-1938. 2. Ilan DI, Tejwani N, Keschner M, Leibman M. Quadriceps tendon rupture. J Am Acad Orthop Surg. 2003;11(3):192-200. 3. O'Shea K, Kenny P, Donovan J, et al. Outcomes following quadriceps tendon ruptures. Injury. 2002;33(3):257-260. 4. Rasul AT Jr, Fischer DA. Primary repair of quadriceps tendon ruptures. Results in 21 patients. Clin Orthop Relat Res. 1993;(289):205-207. 5. Scuderi C. Ruptures of the quadriceps tendon. Study of twenty tendon ruptures. Am J Surg. 1958;95(4):626-634. 6. Siwek CW, Rao JP. Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg Am. 1981;63(6):932-937. 7. West JL, Keene JS, Kaplan LD. Early motion after quadriceps and patellar tendon repairs: outcomes with single-suture augmentation. Am J Sports Med. 2008;36(2):316-323. PMID: 17932403. 8. Konrath GA, Chen D, Lock T, et al. Outcomes following repair of quadriceps tendon ruptures. J Orthop Trauma. 1998;12(4):273-279. PMID: 9619463. 9. Duell B, Long MK, Divella M, Fogel J, Ruotolo C. Transosseous repair with Nice knot augmentation versus knotless suture anchor repair with suture tape for quadriceps tendon rupture: a cadaveric study. Orthopedics. 2023;46(3):135-140. PMID: 36508490. 10. Lighthart WA, Cohen DA, Levine RG, Parks BG, Boucher HR. Suture anchor versus suture through tunnel fixation for quadriceps tendon rupture: a biomechanical study. Orthopedics. 2008;31(5):441. PMID: 19292325. 11. Seggewiss J, Nicolini LF, Lichte P, et al. Transosseous suture versus suture anchor fixation for inferior pole fractures of the patella in osteoporotic bone: a biomechanical study. Eur J Med Res. 2022;27(1):270. PMID: 36463220.
Clinical outcomes after repair of quadriceps tendon rupture: a systematic review
- 12 studies, 319 patients, mean age 57 years (range 16 to 85); the commonest mechanism was a simple fall (61.5 percent)
- Most tears occur 1 to 2cm proximal to the superior pole of the patella, or at the osseotendinous junction in older patients
- Patellar drill-hole (transosseous) repair was the single most frequent technique (50 percent of patients); the type of repair did not significantly change outcome
- Overall pooled re-rupture rate was only 2 percent; deep infection 1.1 percent, superficial infection 1.2 percent, heterotopic ossification 6.9 percent; the worst results followed DELAYED repair
Quadriceps tendon rupture
- Predominantly affects individuals over 40, often with underlying medical conditions
- Bilateral spontaneous rupture is associated with gout, diabetes and steroid use
- Classic clinical triad: acute pain, impaired active knee extension, and a palpable suprapatellar gap
- Incomplete tears may be treated non-operatively; complete ruptures are best managed by early surgical repair
Transosseous repair with Nice knot augmentation versus knotless suture anchor repair with suture tape for quadriceps tendon rupture: a cadaveric study
- 10 matched cadaveric pairs (n equals 20)
- Transosseous repair with Nice-knot augmentation: ultimate load to failure 1489.5 N versus 717.7 N for knotless suture anchors (p less than 0.001)
- Less cyclic gapping with transosseous repair at both early (0.59 versus 2.1mm) and late (1.2 versus 3.9mm) cycles
- Higher construct stiffness with transosseous repair (80.7 versus 44.4 N/mm)
Transosseous suture versus suture anchor fixation for inferior pole fractures of the patella in osteoporotic bone: a biomechanical study
- 12 fresh-frozen cadaveric knees, extensor-mechanism cyclic loading 90 to 5 degrees
- Suture anchors failed earlier than transosseous suture (539 versus 1000 cycles, p equals 0.04)
- Anchor cycles-to-failure correlated positively with bone mineral density (r equals 0.60)
- Destructive load to failure higher for transosseous suture (825.7 N versus 422.4 N, p equals 0.04)
Suture anchor versus suture through tunnel fixation for quadriceps tendon rupture: a biomechanical study
- Cadaveric cyclic loading at 150 N, 0.5 Hz
- No significant difference in displacement between anchors and bone tunnels at initial loading
- After 1000 cycles displacement was near-identical: 4.65mm (anchors) versus 4.50mm (tunnels)
- Suture anchors require less peripatellar dissection but are more expensive