Gold standard for ALIF L2 to S1 | Vascular protection | Minimal neural retraction | Retrograde ejaculation risk
- Left-sided approach preferred — right-sided risks liver retraction, IVC injury, and places the genitofemoral nerve at higher risk.
- Great vessels are anterior to the spine — mobilize them to the left to expose the disc space; the aortic bifurcation at L4 is the key landmark.
- Superior hypogastric plexus lies over the L5-S1 disc — injury causes retrograde ejaculation in 3 to 5 percent of males (higher with midline dissection).
- Sympathetic chain runs on the anterolateral vertebral body — preserve it to prevent vascular instability and sexual dysfunction.
- Psoas muscle contains the lumbar plexus — work medial to the muscle to avoid nerve injury and never retract it laterally.
When & Why
What it exposes. The retroperitoneal anterolateral approach gives direct anterior access to the vertebral bodies and disc spaces from L2 to S1, the anterior longitudinal ligament, and the whole disc space for a large interbody graft — with minimal neural retraction compared to posterior approaches. First described by Burns in 1932 for sympathectomy and adapted for spinal surgery in the 1940s, it is now the workhorse for anterior column reconstruction. Indications. - Anterior lumbar interbody fusion (ALIF) for degenerative disc disease
- Vertebral body corpectomy for tumour or infection
- Total disc replacement at L4-L5 and L5-S1
- Anterior column reconstruction after trauma
- Revision fusion after a failed posterior approach
- Correction of sagittal imbalance (lordosis restoration) Why anterior, not posterior. The anterior route offers biomechanical and clinical advantages over posterior interbody techniques: - Large graft area — the entire disc space is available for a wide cage footprint that maximises the fusion surface.
- High fusion rates — ALIF fusion rates are consistently reported around 90 to 95 percent, at least comparable to and often exceeding posterior interbody techniques.
- Indirect neural decompression — disc-height restoration opens the foramen without laminectomy or nerve-root retraction.
- Lordosis restoration — better sagittal-balance correction through anterior column lengthening.
- No paraspinal muscle damage — avoids posterior muscle denervation and atrophy.
- No posterior scar — facilitates later revision surgery if needed. Global utilisation. Lumbar interbody fusion is among the most commonly performed elective spinal procedures worldwide, and anterior approaches (ALIF, OLIF, LLIF) have seen rising utilisation over the last two decades as access techniques and standalone integrated cages have matured. Anterior approaches are favoured where maximal disc-height and lordosis restoration with a large interbody footprint is the priority.
A left-sided approach is strongly preferred. A right-sided approach risks liver retraction, IVC injury (the IVC wall is thinner than the aorta), and a higher rate of genitofemoral nerve injury.
Position & landmarks. Right lateral decubitus, left side up, on a radiolucent table. Flex the table at the waist to open the flank, stabilise with a beanbag or tape, and use 10 to 15 degrees of reverse Trendelenburg so the bowel falls away. Mandatory padding: an axillary roll two finger-breadths below the axilla (prevents brachial plexus injury), a pillow between the knees (protects the lateral knee and fibular head, guarding the common peroneal nerve), and gel pads at the iliac crest, dependent shoulder and ear. Gravity then pulls the bowel anteriorly, table flexion opens the retroperitoneal space, and left-side-up protects the IVC. Incision by level: L2-L3 along the 12th rib; L3-L4 midway between rib and iliac crest; L4-L5 just above the iliac crest; L5-S1 along the iliac crest or bikini line. Variations. Standard open, mini-open (tubular retractors), lateral transpsoas (XLIF/DLIF), oblique lateral (OLIF), and robotic-assisted. Outcomes. 95 percent fusion rate at two years, 80 to 85 percent clinical success, a 5 to 10 percent complication rate, and a 5 to 8 percent reoperation rate.
The Exposure
Work down through the flank in line with the muscle fibres to reach the retroperitoneal space, then mobilise the great vessels to the left to deliver the disc space — working medial to the psoas and lateral to the hypogastric plexus throughout.
Exposure sequence
- Incision location varies by target level: L2-L3 parallel to the 12th rib; L3-L4 midway between costal margin and iliac crest; L4-L5 just above the iliac crest, oblique; L5-S1 along the iliac crest or lower abdominal (bikini-line in supine).
- Standard oblique flank incision (L3-L5) is 8 to 15 cm depending on mini-open versus standard open technique.
- Begin 2 to 3 cm lateral to the rectus sheath and extend obliquely toward the flank; dissect subcutaneous tissue to identify the muscle layers.
- External oblique — fibres run inferomedially; split in line with them by blunt finger dissection or scissors and place a self-retaining retractor.
- Internal oblique — fibres run perpendicular (superomedially); split in line with them and retract to expose transversus abdominis.
- Transversus abdominis — fibres run transversely; split bluntly in line with them to expose the transversalis fascia (a white, glistening layer).
- The transversalis fascia is the critical layer marking entry to the retroperitoneal space — incise it carefully under direct vision to avoid entering the peritoneum.
- Insert a finger and gently sweep anteriorly; the peritoneum should peel away anteriorly as a smooth, glistening surface, with yellow lobulated retroperitoneal fat visible behind it.
- If bowel is visible through the peritoneum, the correct plane is confirmed. Too anterior enters the peritoneum (bowel injury); too lateral enters the psoas (plexus injury).
- Insert a hand and sweep the peritoneum anteriorly and medially with the fingers, bluntly mobilising the peritoneal sac and bowel away from the field.
- The ureter stays on the peritoneal surface and should mobilise anteriorly with the bowel (white cord-like structure running inferiorly).
- Feel posteriorly for the psoas muscle — firm and striated.
- Psoas muscle is the first deep structure encountered posteriorly; the genitofemoral nerve (small, white) lies on its surface at L2-L4 and is the most vulnerable nerve.
- Work medial to the psoas to avoid the lumbar plexus within it; never retract the psoas laterally.
- The peritoneal sac is thin and translucent with bowel visible through it — retract it gently anteriorly.
- L2-L3: aorta on the left of the vertebral body, IVC on the right; segmental lumbar vessels cross the disc space (ligate and divide if needed for exposure).
- L3-L4: aorta more anterior; identify the iliolumbar vein crossing posterior to the common iliac vessels and protect it to prevent catastrophic bleeding.
- L4-L5 (critical level): identify the aortic bifurcation (typically at the L4 body); the left common iliac vein crosses posterior to the right common iliac artery and is often adherent to the L4-L5 disc — the highest vascular risk in the approach.
- L5-S1: common iliac vessels diverge laterally; the middle sacral artery and vein cross the disc (must be ligated and divided); fine filaments of the superior hypogastric plexus lie over the disc.
- Identify vessels before mobilising; use gentle padded sponge-stick retraction and avoid rigid retractors directly on vessels; mobilise artery and vein together as a unit.
- Segmental vessels: dissect free, doubly ligate or clip artery and vein separately flush with the aorta/IVC, and divide between ligatures.
- L4-L5 sequence: identify the bifurcation and both common iliac arteries, then the left common iliac vein posterior to the right common iliac artery; ligate and divide the iliolumbar (and ascending lumbar if present) vein; gently elevate the right common iliac artery and sharply dissect the thin-walled left common iliac vein off the disc; mobilise the vessels as a unit to the left behind a padded retractor.
- L5-S1: doubly ligate and divide the middle sacral vessels; mobilise the common iliac vessels laterally; approach the disc laterally and bluntly only, preserving the superior hypogastric plexus and never stripping the midline presacral fascia.
- Release vascular retraction every 15 to 20 minutes, keep vessels moist with warm saline, and watch for vessel-wall haematoma (a sign of injury).
- Use a self-retaining retractor system: anterior blade retracts peritoneum and bowel, posterior blade gives gentle retraction on the psoas (do not over-retract laterally), and superior and inferior blades hold the mobilised vessels.
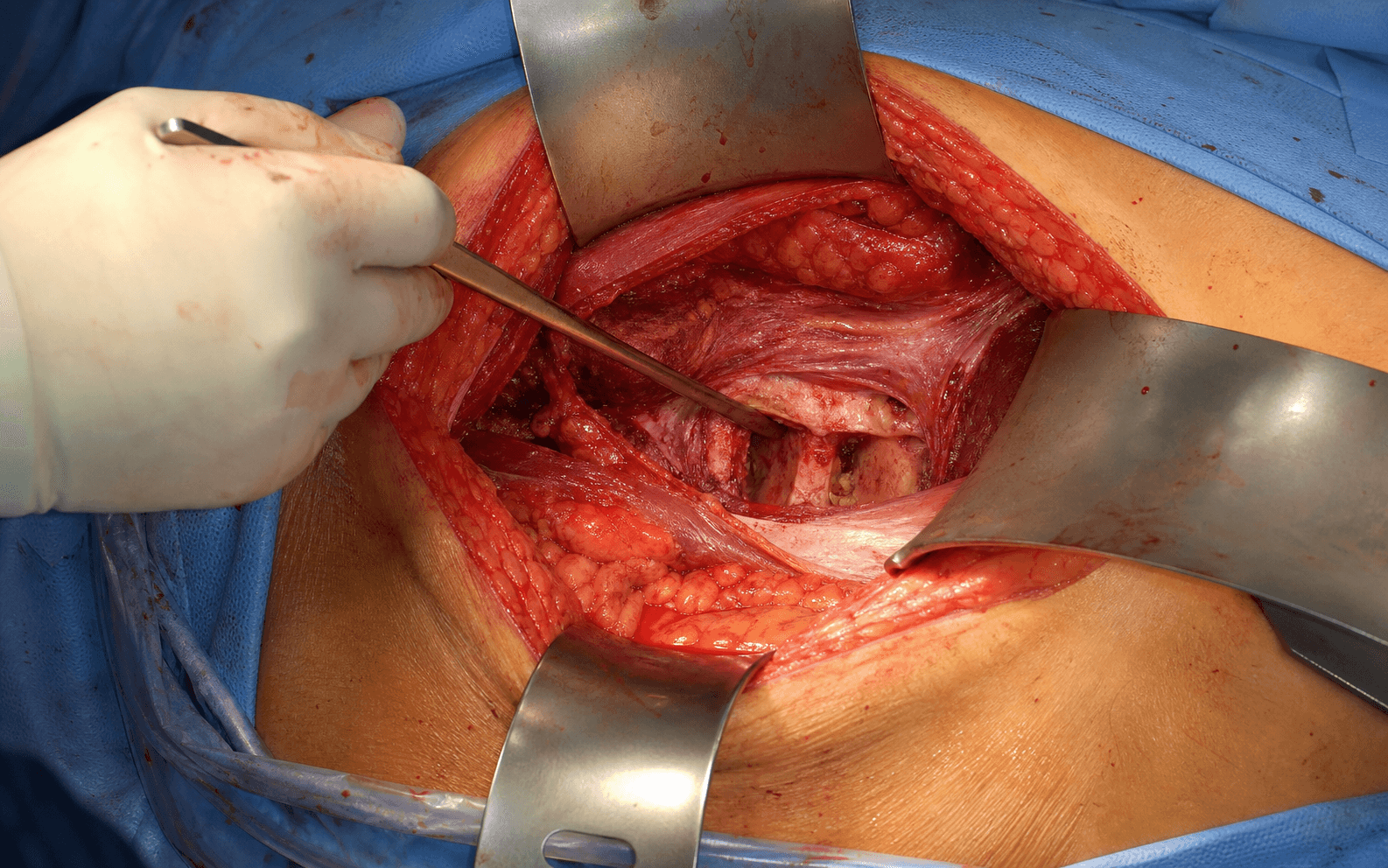
- A completed exposure shows the vertebral body anteriorly, the disc space centred in the wound, vessels safely mobilised to the left, the psoas visible laterally, and no peritoneal perforation (no bowel visible directly).
- Confirm the level with AP and lateral fluoroscopy before proceeding — count from the sacrum upward.
- The anterior longitudinal ligament (ALL) may be preserved or divided; if divided, make a rectangular window and save it for closure (repair reduces postoperative vascular adhesion and aids revision).
- Make a rectangular annulotomy, remove nucleus pulposus with pituitary rongeurs, and use curettes to remove the cartilaginous endplate while preserving the bony (subchondral) endplate.
- Complete the discectomy to the posterior annulus (preserve it as a barrier to retropulsion), remove anterior osteophytes, and create flat, parallel endplates with bleeding subchondral bone.
- Use trial spacers to choose the largest footprint that fits safely and confirm sizing and lordosis with fluoroscopy.
- Pack the cage with graft (autograft from the discectomy, allograft, or BMP) and choose the lordotic angle for the level (L5-S1 typically 6 to 8 degrees).
- Insert with a holder/impactor using gentle taps, confirm position with fluoroscopy — the cage should be flush with the anterior cortex or slightly recessed with no posterior protrusion on the lateral view.
The left common iliac vein is thin-walled, crosses posterior to the right common iliac artery, and is frequently adherent to the L4-L5 disc — it is the structure most often injured in this approach and the source of the catastrophic bleeds. Mobilise it gently to the left with a padded sponge-stick, free it with sharp dissection, and use only padded retractors. If it is injured, apply direct pressure with a laparotomy pad and call vascular surgery immediately — never blind-clamp, which enlarges the tear.
Stay medial to the psoas (the lumbar plexus lives within it) and lateral to the superior hypogastric plexus at L5-S1 (midline presacral stripping causes retrograde ejaculation). Between these two rules lies the safe anterior corridor to the disc.
Dangers & Extensions
Structures at risk, by layer
- Risk (rate)
- Thin-walled, adherent to disc, crosses posterior to the right common iliac artery (vascular injury 0.3 to 2 percent, highest at L4-L5)
- Protection
- Mobilise gently to the left with a padded sponge-stick; sharp dissection off the disc; padded retractors; direct pressure if injured, never blind-clamp
- Risk (rate)
- Cross the disc space; iliolumbar runs posterior to the common iliacs; a tear bleeds briskly
- Protection
- Doubly ligate or clip flush with the aorta/IVC before division; divide the iliolumbar vein to free the iliac vein
- Risk (rate)
- Cross the L5-S1 disc in the midline
- Protection
- Identify, doubly ligate and divide before L5-S1 exposure
- Risk (rate)
- Fine filaments over the L5-S1 disc; injury causes retrograde ejaculation in 3 to 5 percent of males
- Protection
- Lateral (not midline) presacral dissection; blunt only; never strip the presacral fascia; counsel all males preoperatively
- Risk (rate)
- Lies on the anterolateral vertebral body
- Protection
- Preserve during dissection to avoid vascular and sexual dysfunction
- Risk (rate)
- Genitofemoral on the psoas surface L2-L4; plexus within psoas (neural injury less than 1 percent)
- Protection
- Work medial to the psoas; never retract it laterally; gentle posterior retraction only
- Risk (rate)
- On the peritoneal surface overlying psoas (injury less than 0.5 percent)
- Protection
- Keep the peritoneum intact; mobilise anteriorly with it; identify and protect
- Risk (rate)
- Thin sac; perforation 2 to 5 percent
- Protection
- Develop the correct retroperitoneal plane; primary repair with 3-0 Vicryl plus anaerobic cover if torn
- Rate
- 0.3 to 2 percent
- Management
- Direct pressure, call vascular surgery, primary repair with 5-0 or 6-0 Prolene, patch or ligation; never blind-clamp
- Rate
- 3 to 5 percent
- Management
- No treatment available; counsel and document consent preoperatively; sperm retrieval if fertility is desired
- Rate
- 5 to 15 percent
- Management
- Preserve the subchondral plate, use the largest cage footprint, add posterior instrumentation if osteoporotic
- Rate
- less than 1 percent
- Management
- Most resolve over 3 to 6 months; prevented by working medial to the psoas
- Rate
- 2 to 5 percent
- Management
- Primary repair with 3-0 Vicryl, add anaerobic cover (metronidazole)
- Rate
- less than 0.5 percent
- Management
- Keep the peritoneum intact; if injured, primary repair over a stent
Stay calm and tell the anaesthetist immediately — request two large-bore IVs, cross-match four units, and prepare for massive transfusion. Achieve immediate control with direct pressure using a laparotomy pad; do not blind-clamp. Call for vascular surgery help at once. While maintaining pressure, widen the wound and improve exposure. Once controlled, assess the injury and repair primarily with 5-0 or 6-0 Prolene; use a patch for larger defects, or ligate the iliac vein if repair is impossible (tolerated, but may cause leg swelling). Complete the disc work only if the patient is stable, place a drain, and document the injury and repair.
Extensile options and variations. Extend the incision proximally along the 12th rib for higher lumbar levels, or distally toward the bikini line for L5-S1. Technique variants include mini-open ALIF with tubular retractors (smaller incision, less soft-tissue trauma but limited visualization), the lateral transpsoas XLIF/DLIF (avoids the great vessels but crosses the psoas and risks the lumbar plexus), the oblique lateral OLIF (retroperitoneal corridor between vessels and psoas), and robotic-assisted navigation. Closure. Meticulous haemostasis is critical to prevent retroperitoneal haematoma — check all segmental and middle sacral ligature stumps, apply bone wax to vertebral-body edges, and use bipolar cautery on muscle edges. If the ALL was divided, repair it with running or interrupted 2-0 Vicryl to reduce adhesions. No formal muscle repair is needed (the muscles were split, not divided) — they reapproximate spontaneously. Close the transversalis fascia with running 1 Vicryl (recreates the barrier to the retroperitoneum), approximate the oblique layers, close Scarpa fascia with 2-0 Vicryl, and close skin with subcuticular 3-0 Monocryl plus glue. Place a 19Fr round drain (Jackson-Pratt or Blake) in the retroperitoneal space through a separate lateral stab for large exposures or multilevel surgery; remove when output is less than 30 mL per 24 hours (typically day 1 to 3), and watch for milky chyle indicating lymphatic injury — keep the drain until it stops. Postoperative care. Day 0 to 1: neurovascular exam, AP and lateral X-ray to confirm cage position, VTE prophylaxis per local protocol (mechanical plus chemoprophylaxis such as LMWH or a DOAC once bleeding risk is acceptable, balanced against retroperitoneal-haematoma risk), and full weight bearing from day 1 with no brace if the standalone construct is stable; monitor haemoglobin (retroperitoneal bleeding is occult) and drain output. Weeks 1 to 6: full mobilisation, avoid lifting more than 5 kg for six weeks, X-rays at 2 and 6 weeks to check subsidence, return to sedentary work at 2 to 4 weeks and heavy labour at 12 weeks. Follow-up: CT at 6 months confirms fusion (95 percent rate); monitor for adjacent-segment disease (2 to 3 percent per year); expect 80 to 85 percent good-to-excellent results.
Procedures Through This Approach
- Anterior lumbar interbody fusion (ALIF) — the principal operation, for degenerative disc disease with 95 percent fusion rates and superior lordosis restoration.
- Vertebral body corpectomy for tumour, infection or trauma involving the anterior column.
- Total disc replacement at L4-L5 and L5-S1 in selected patients.
- Anterior column reconstruction after trauma, and revision fusion after a failed posterior approach (avoids posterior scar).
- Sagittal imbalance correction — ALIF restores 8 to 10 degrees of lordosis versus 4 to 6 degrees for TLIF, making it the preferred route when sagittal balance is the priority.
Viva & Exam Focus
ALIFApproach essentials
Hook:ALIF reminds you this is the Anterior Lumbar Interbody Fusion approach
VESSELSVascular protection strategy
Hook:The VESSELS protocol minimises the most catastrophic complication of this approach
Exam viva scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old male builder presents with chronic low back pain and right L5 radiculopathy. MRI shows severe L5-S1 disc degeneration with a high-intensity zone and right L5 nerve-root compression. He has failed six months of conservative treatment. You plan L5-S1 ALIF. How would you counsel this patient regarding the specific risks of this procedure?”
“You are performing L4-L5 ALIF via a left retroperitoneal approach. During mobilisation of the left common iliac vein, which is adherent to the L4-L5 disc, you notice sudden pooling of dark blood. The vein appears to have a 1 cm laceration and the patient becomes hypotensive, BP 85/50. What do you do?”
“A 55-year-old woman has severe L4-L5 degenerative disc disease with loss of lordosis and sagittal imbalance (SVA 8 cm). She had an L4 laminectomy five years ago for stenosis and has failed extensive conservative treatment. Compare ALIF versus TLIF for this patient and justify your approach selection.”
Key anatomy
- Retroperitoneal plane: between peritoneum (anterior) and psoas/vertebrae (posterior)
- Great vessels lie ANTERIOR to the spine: aorta left, IVC right, bifurcation at L4
- Left common iliac vein crosses POSTERIOR to the right common iliac artery at L4-L5
- Ureter on the peritoneal surface overlying psoas — mobilise anteriorly with the peritoneum
- Genitofemoral nerve on the psoas surface L2-L4 — most vulnerable nerve, causes anterior-thigh numbness
- Superior hypogastric plexus crosses the L5-S1 disc — injury causes retrograde ejaculation 3 to 5 percent
- Sympathetic chain on the anterolateral vertebral body — preserve for sexual function
Indications
- ALIF for degenerative disc disease — 95 percent fusion rate, superior lordosis restoration
- Corpectomy for tumour, infection or trauma involving the anterior column
- Total disc replacement L4-L5 and L5-S1 in selected patients
- Sagittal imbalance correction — ALIF restores 8 to 10 degrees versus 4 to 6 for TLIF
- Revision fusion after a failed posterior approach — avoids posterior scar
Positioning
- Right lateral decubitus for a left-sided approach (preferred)
- Table flexed at the waist to open the space between ribs and iliac crest
- Axillary roll mandatory — two finger-breadths below the axilla to prevent brachial-plexus injury
- Pad the fibular head of the upper leg — common-peroneal palsy if not padded
- 10 to 15 degrees reverse Trendelenburg helps the bowel fall away
Approach steps
- Oblique flank incision: location varies by level — L5-S1 along the iliac crest, L4-L5 above the crest
- Split the three muscle layers in line with fibres: external oblique (inferolateral), internal oblique (superomedial), transversus (transverse)
- Incise the transversalis fascia CAREFULLY — it marks entry to the retroperitoneal space
- Finger dissection to mobilise the peritoneum anteriorly and medially with the bowel
- Identify the psoas posteriorly — work MEDIAL to the muscle (lumbar plexus inside)
- Expose the great vessels BEFORE disc work — identify the bifurcation and vein position
Vascular mobilisation
- LEFT-sided approach preferred — avoids IVC injury, liver retraction, protects genitofemoral nerve
- L4-L5 is the HIGHEST-RISK level — aortic bifurcation, left common iliac vein adherent to disc
- Ligate segmental lumbar vessels flush with the aorta/IVC to prevent postoperative bleeding
- Left common iliac vein: GENTLE sharp dissection from the disc — thin-walled and easily injured
- L5-S1: ligate and divide the middle sacral vessels, preserve the superior hypogastric plexus LATERALLY
- Use padded sponge-stick retractors and release every 15 to 20 minutes to prevent vessel injury
Critical risks
- Vascular injury 0.3 to 2 percent: left common iliac vein most common — direct pressure then vascular repair
- Retrograde ejaculation 3 to 5 percent of males at L5-S1: hypogastric-plexus injury — MUST counsel preoperatively
- Lumbar-plexus injury less than 1 percent: genitofemoral nerve on the psoas surface — gentle retraction only
- Peritoneal perforation 2 to 5 percent: primary repair if recognised, antibiotics if contamination
- Ureter injury less than 0.5 percent: keep peritoneum intact, mobilise the ureter anteriorly with it
Disc work
- Confirm the level with AP and lateral fluoroscopy BEFORE proceeding — count from the sacrum
- Preserve or divide the ALL — repairing it at closure reduces adhesions
- Complete the discectomy to the posterior annulus with pituitary rongeurs
- Endplate preparation: remove cartilage, expose bleeding bone, preserve the subchondral plate
- Largest cage footprint that fits — maximises the fusion surface
- Lordotic cage for L4-L5 (4 to 6 degrees) and L5-S1 (6 to 8 degrees) restores sagittal balance
Closure
- Meticulous haemostasis is CRITICAL — check vessel ligatures, bone wax on vertebral edges
- NO formal muscle repair needed — muscles split not divided, reapproximate spontaneously
- Close the transversalis fascia with running 1 Vicryl — recreates the barrier to the retroperitoneum
- Drain recommended for large exposure or multiple levels — remove when output is less than 30 mL per 24 hours
- Watch for chyle in the drain (milky fluid) — lymphatic injury, keep the drain until it stops
Postoperative care
- Full weight bearing immediately — no brace if the standalone construct is stable
- VTE prophylaxis: mechanical plus chemoprophylaxis (LMWH or DOAC) per local protocol — weigh against retroperitoneal-haematoma risk
- Monitor for retroperitoneal bleeding: serial haemoglobin, flank pain, hypotension
- X-ray at 2 and 6 weeks — assess cage position and subsidence
- CT at 6 months to confirm fusion — bridging bone, no radiolucency, 95 percent fusion rate
- Return to work: sedentary 2 to 4 weeks, heavy labour 12 weeks
Complications management
- Vascular injury: direct pressure, call vascular surgery, NO blind clamping, primary repair with 5-0 Prolene
- Retrograde ejaculation: NO treatment available — counsel preop, document consent, sperm retrieval if fertility needed
- Peritoneal tear: primary repair 3-0 Vicryl, add anaerobic cover (metronidazole)
- Cage subsidence 5 to 15 percent: preserve subchondral bone, largest cage footprint, consider posterior instrumentation if osteoporotic
Level-specific points
- L2-L4: mobilise the psoas laterally, protect the genitofemoral nerve on its surface
- L4-L5: HIGHEST VASCULAR RISK — bifurcation level, vein adherent to disc, vascular standby recommended
- L5-S1: HIGHEST RETROGRADE-EJACULATION RISK — lateral dissection technique, preserve hypogastric plexus
- Mini-open ALIF: tubular retractors, smaller incision, reduced visualization versus standard open
Exam pearls
- Left-sided approach STRONGLY preferred — right-sided risks IVC injury and liver retraction
- ALIF fusion rate 95 percent is superior to PLIF/TLIF 85 to 90 percent because of the larger graft area
- Superior lordosis restoration: ALIF 8 to 10 degrees versus TLIF 4 to 6 degrees — critical for sagittal balance
- Counsel ALL male patients about retrograde-ejaculation risk — medicolegally critical
- Surgical prophylaxis: a first-generation cephalosporin (e.g. cefazolin) within 60 minutes of incision per standard guidance worldwide
References
Lumbar Interbody Fusion: Techniques, Indications and Comparison of Options
- Comprehensive comparative review of all interbody fusion routes (PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF, ALIF) with indications by level and pathology
- Anterior approaches (ALIF) avoid the spinal canal, cauda equina and nerve roots, and provide the largest interbody footprint with strong disc-height and lordosis restoration
- Posterior approaches are limited by thecal-sac and nerve-root retraction and iatrogenic paraspinal muscle injury
- ALIF carries approach-specific abdominal and vascular morbidity; lateral and OLIF techniques risk the lumbar plexus and psoas
- Proposes an evidence-based framework for selecting the interbody approach by indication and spinal level
Vascular Injury During Anterior Lumbar Surgery
- Overall vascular injury rate 1.9 percent across 1,315 consecutive anterior lumbar procedures from L2 to S1
- Major vein lacerations occurred in 1.4 percent and left iliac artery thrombosis in 0.45 percent
- Only 5 of 1,315 patients experienced significant clinical sequelae — most injuries managed without lasting morbidity
- Anterior lumbar surgery is comparatively safe when performed with meticulous respect for the great vessels
- Catastrophic outcomes are rare but possible, supporting access-surgeon involvement and vascular backup for high-risk levels
Retrograde Ejaculation After Anterior Interbody Lumbar Fusion
- In 40 male patients after anterior interbody fusion, retrograde ejaculation occurred in 9, becoming permanent in 7 (17.5 percent)
- All affected patients had been operated via a transabdominal (transperitoneal) approach, implicating presacral autonomic-plexus disturbance
- Multi-level (L4-S1) and previously operated patients were over-represented among those affected
- The complication had historically been underestimated, particularly in re-operated low-back patients
- Authors cautioned against the transabdominal route in male patients — underpinning the modern preference for a retroperitoneal approach with lateral presacral dissection
Retrograde Ejaculation After ALIF Using rhBMP-2: A Cohort-Controlled Study
- Retrograde ejaculation in 7.2 percent of male ALIF patients receiving rhBMP-2 versus 0.6 percent in controls without rhBMP-2
- For single-level L5-S1 ALIF the rates were 6.7 percent (rhBMP-2) versus 0 percent (control)
- Findings confirmed the elevated rhBMP-2-associated RE signal first noted in the original FDA dataset (8 percent versus 1.4 percent)
- Only half of affected patients (3 of 6) reported resolution by one year
- rhBMP-2 use at the anterior L5-S1 level should be weighed carefully in men concerned about fertility
ALIF With and Without an Access Surgeon: A Systematic Review and Meta-analysis
- Pooled analysis of 58 studies (8,028 patients) comparing ALIF performed with versus without a dedicated access surgeon
- Pooled arterial-injury rate 0.44 percent (no access) and 1.16 percent (access surgeon); retrograde ejaculation 0.41 percent versus 0.96 percent
- Neurological-injury rate was lower with an access surgeon (0.11 percent versus 0.99 percent) as was peritoneal injury (0.16 percent versus 0.44 percent)
- Total postoperative complications (4.08 percent versus 5.95 percent) and reoperation (1.31 percent versus 2.28 percent) were lower when an access surgeon was involved
- Higher vascular/RE figures in the access-surgeon group likely reflect selection of more complex exposures to access surgeons