Posterior access to the proximal-middle radial shaft | Supinator split | PIN protected by supination
- Thompson approach: POSTERIOR access to proximal-middle radial shaft (radial head to middle 1/3), ideal for PIN exploration/decompression and posterior radial shaft fracture fixation
- Arcade of Frohse: Fibrous arch at the proximal supinator edge where the PIN enters the muscle (approx 22mm distal to the radiocapitellar joint, approx 3.8cm distal to the lateral epicondyle - Qawasmi 2025, Low 1994); classically the most common single site of PIN compression in radial tunnel syndrome (Spinner)
- Supinator splitting technique: Split the supinator IN LINE with its fibres from radial (lateral) to ulnar (medial) side - the PIN lies on the DEEP surface between the two supinator heads, surrounded by muscle (not directly on bone distal to the arcade - Qawasmi 2025)
- PIN innervation pattern: Innervates ALL posterior forearm muscles EXCEPT brachioradialis and ECRL (these are innervated by the radial nerve BEFORE PIN bifurcation, so they are preserved in PIN palsies - this distinguishes PIN palsy from high radial nerve injury)
- Forearm position protects the PIN: SUPINATION moves the PIN away from the radius and radial tuberosity (the PIN is closest to bone in pronation - Heidari 2010, Qawasmi 2025); supinate the forearm when exposing and protecting the nerve
- Approach choice for radius fractures: The Henry (anterolateral) volar approach is the workhorse for radial shaft fractures and avoids direct PIN exposure; reserve the Thompson approach for PIN exploration, posterior radial head access, or revision of a prior anterior approach
- Radial tunnel decompression: No single approach exposes ALL compression sites - the posterior (Thompson) approach gives the best view of the distal supinator border, while the arcade and leash of Henry are better reached anteriorly/anterolaterally (Urch 2015)
- “PIN innervates ALL posterior forearm muscles EXCEPT brachioradialis and ECRL - these are preserved in PIN palsy (wrist extension 5/5, but with radial deviation as ECU is lost; distinguishes from high radial nerve injury with complete wrist drop 0/5)
- “Arcade of Frohse is the most common single site of PIN compression - radial tunnel syndrome presents with lateral elbow/forearm pain WITHOUT motor weakness, while PIN palsy (posterior interosseous nerve syndrome) has finger/thumb extension weakness WITHOUT sensory loss
- “Thompson approach uses supinator SPLITTING (along muscle fibres); the Henry approach mobilises/reflects the supinator OFF the radius with the forearm SUPINATED - supination protects the PIN by carrying it away from the bone (Heidari 2010)
- “Radial shaft safe zones: the anterolateral (Henry) corridor is SAFE, while the posterior (Thompson) corridor becomes risky distal to the supinator where the PIN terminal branches fan out toward the interosseous membrane
When & Why
What it exposes. The Thompson (dorsal/posterior) approach gives direct access to the proximal and middle thirds of the radial shaft, the radial head and neck (posteriorly), and — uniquely among radial approaches — the posterior interosseous nerve (PIN) itself, from the arcade of Frohse to the distal edge of the supinator. It is the approach of choice whenever the surgical goal is to find, decompress or protect the PIN. Why posterior. No other approach exposes the PIN along its course through the supinator. The Thompson approach lets you release all three radial-tunnel compression sites (arcade of Frohse, leash of Henry, distal supinator border) — although no single incision visualises every site equally, and the posterior window is best for the distal border (Urch 2015). For routine radial shaft fractures, however, the Henry anterolateral approach is preferred because it does not directly expose the PIN: the supinator is reflected off the radius with the forearm supinated, carrying the nerve away from the bone (Heidari 2010). Reach for Thompson when the indication is the nerve or the posterior radial head, not for a straightforward shaft fracture. Position & landmarks. Supine, arm abducted 90 degrees on a radiolucent hand table, elbow flexed 90 degrees, forearm in neutral rotation (thumb up) to maximally expose the posterolateral radius. Upper-arm tourniquet inflated to 250mmHg after Esmarch exsanguination. Palpate and mark the lateral epicondyle (proximal landmark) and Lister's tubercle (distal landmark on the dorsal wrist); the incision runs along the posterolateral forearm centred on the mobile wad (brachioradialis, ECRL, ECRB).
PIN exploration & decompression
- Radial tunnel syndrome: chronic lateral forearm pain (NO motor weakness) failed conservative management (therapy, activity modification, NSAIDs, corticosteroid injection). It is largely a clinical diagnosis — electrodiagnostics are frequently normal
- PIN palsy: progressive finger/thumb extension weakness WITHOUT sensory loss, with no spontaneous recovery, or imaging showing compression (ganglion, lipoma, hourglass fascicular constriction — Wu 2014)
- PIN laceration (open trauma, iatrogenic injury) Proximal radius fixation
- Radial head fractures (Mason II–III) needing posterior access or excision/replacement
- Radial neck and proximal-shaft fractures Other
- Proximal-radius tumour (enchondroma, osteochondroma) or chronic osteomyelitis
- Rheumatoid synovitis compressing the PIN at the arcade
Absolute
- Active soft-tissue or bone infection of the forearm
- Acute closed fracture with a PIN palsy expected to recover (most do — observe) Relative
- Distal 1/3 shaft fractures — the PIN terminal branches fan onto the interosseous membrane; use the Henry volar approach
- Shaft fractures WITHOUT a PIN indication — the Henry approach is preferred (the PIN is not directly exposed)
- Prior Thompson approach with scar tissue around the nerve — consider a virgin Henry corridor for revision
Thompson vs Henry — choosing the approach. The single most common error is reaching for Thompson for a routine radial shaft fracture. The table below frames when each approach earns its place.
- Thompson (posterior)
- Higher — the PIN is directly exposed during supinator splitting (iatrogenic injury approx 1-3% across posterior proximal-radius series)
- Henry (anterolateral)
- Lower — the PIN is not directly exposed; the supinator is reflected off the radius with the forearm supinated, carrying the nerve away from bone (Heidari 2010)
- Preferred for
- Henry for shaft fractures
- Thompson (posterior)
- Good — posterior access to the radial head via supinator origin reflection, ideal for head excision/replacement
- Henry (anterolateral)
- Limited — anterolateral access, difficult to expose the posterior articular surface
- Preferred for
- Thompson for posterior head access
- Thompson (posterior)
- Good — extends to middle 1/3 by distal supinator splitting
- Henry (anterolateral)
- Excellent — extends from proximal 1/3 to distal metaphysis (full shaft)
- Preferred for
- Henry (length of exposure)
- Thompson (posterior)
- Excellent — designed for PIN exposure from arcade of Frohse to distal supinator edge
- Henry (anterolateral)
- None — the PIN remains deep to the supinator
- Preferred for
- Thompson (only approach for the PIN)
- Thompson (posterior)
- Potentially reduced — supinator is split and heals with scar
- Henry (anterolateral)
- Better preserved — supinator is reflected, not divided
- Preferred for
- Henry
- Thompson (posterior)
- Generally longer (careful supinator splitting plus PIN identification)
- Henry (anterolateral)
- Generally shorter (no formal PIN dissection)
- Preferred for
- Henry
- Thompson (posterior)
- 6 weeks limited forearm rotation to protect supinator healing
- Henry (anterolateral)
- Immediate forearm rotation (supinator intact)
- Preferred for
- Henry
- Thompson (posterior)
- Ideal — exposes arcade of Frohse, leash of Henry and distal supinator border
- Henry (anterolateral)
- Inadequate — does not expose PIN compression sites
- Preferred for
- Thompson (only approach for RTS)
- Thompson (posterior)
- Iatrogenic PIN injury, possible supinator weakness, heterotopic ossification, wound infection
- Henry (anterolateral)
- Lower PIN risk; the superficial radial nerve is the main nerve at risk; wound infection
- Preferred for
- Henry (lower nerve-injury profile)
- Thompson (posterior)
- PIN exploration (RTS, PIN palsy), radial head/neck fractures needing posterior access, proximal radius tumour
- Henry (anterolateral)
- Radial shaft fractures (proximal, middle, distal 1/3), non-union
- Preferred for
- Thompson for PIN only; Henry for most shaft fractures
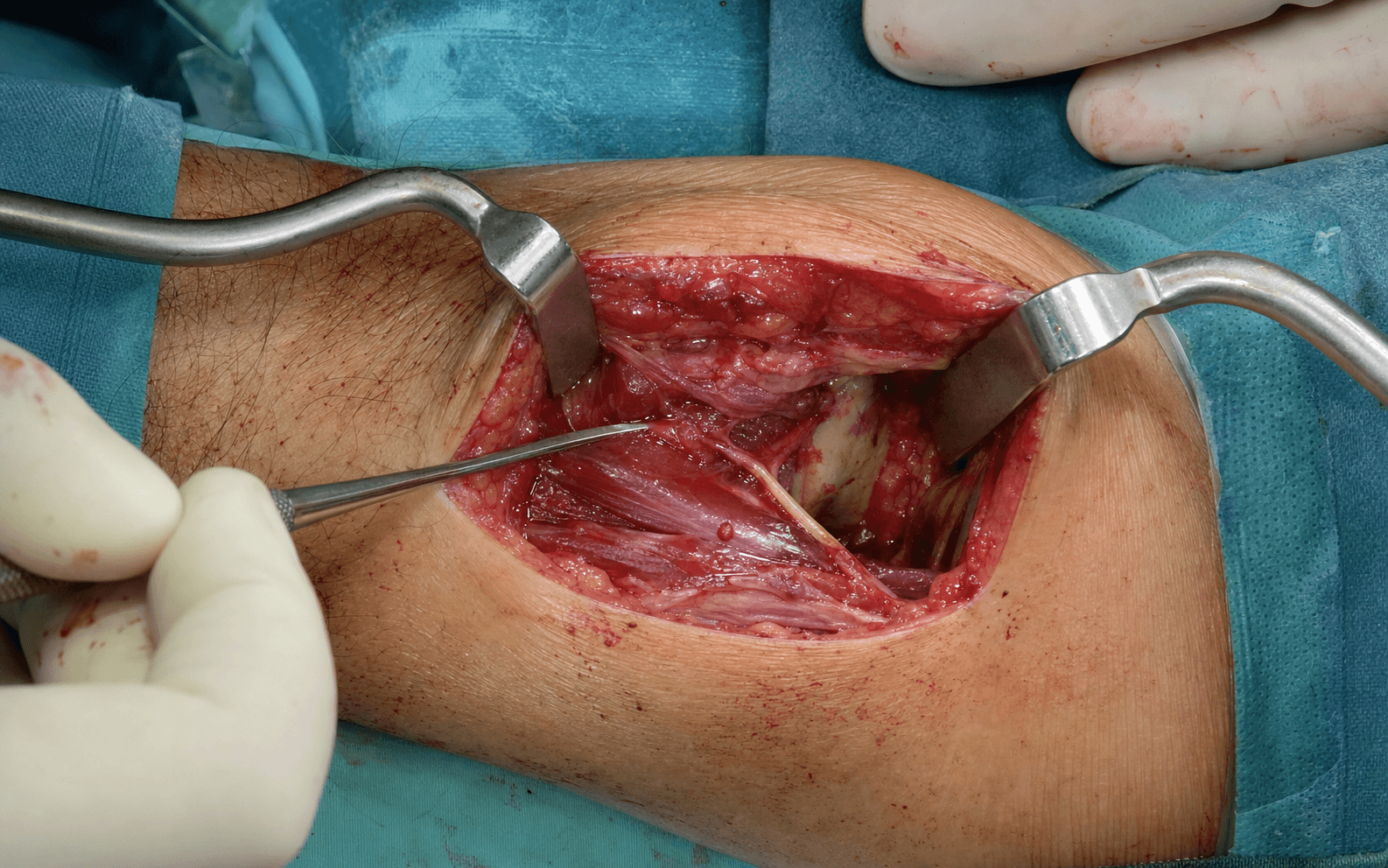
The Exposure
Work down through the layers along the posterolateral forearm, develop the interval between ECRB and extensor digitorum communis, then SUPINATE the forearm and split the supinator in line with the PIN to expose the nerve and the proximal-middle radius. Every step is built around one principle: supination carries the PIN away from the bone, and blunt, in-fibre dissection keeps it safe.
Exposure sequence
- Position: supine, arm abducted 90 degrees on a radiolucent hand table, elbow flexed 90 degrees, forearm in NEUTRAL rotation (thumb up — maximally exposes the posterolateral radius); upper-arm tourniquet 250mmHg after Esmarch exsanguination.
- Landmarks: lateral epicondyle (proximal) and Lister's tubercle (distal); the line of the incision bisects the extensor compartment.
- Incision: a longitudinal posterolateral incision 8–12cm long, from 3–4cm proximal to the lateral epicondyle (to allow identification of the radial-nerve bifurcation) to 6cm distal, centred on the mobile wad. Do NOT extend distally beyond the supinator's distal edge — the PIN terminal branches fan onto the interosseous membrane there.
- Dissect through subcutaneous fat to the fascia over the extensor muscles; preserve the cephalic vein if encountered and coagulate small perforators with bipolar.
- Incise the fascia in the Thompson interval — between ECRB (radial side) and extensor digitorum communis (ulnar side), a relatively avascular plane that carries down to the supinator.
- Mobilise the mobile wad (brachioradialis and ECRL, anterior to the interval) ANTERIORLY with self-retaining retractors to expose the supinator muscle.
- Supinate the forearm fully before any work on the supinator — this carries the PIN away from the radial neck and tuberosity (the nerve is closest to bone in pronation; supination increases its separation by approx 5mm — Heidari 2010, Qawasmi 2025).
- Palpate the proximal edge of the supinator (the arcade of Frohse) approx 3–4cm distal to the lateral epicondyle; the PIN enters the muscle approx 22mm distal to the radiocapitellar joint (Qawasmi 2025). The arcade may feel like a firm tendinous band or a thin fascial edge.
- If a taut fibrous band is present (more frequent in symptomatic radial-tunnel patients — Hong 1989), incise it longitudinally along the line of the PIN to release the constriction.
- Split the supinator from radial (lateral) to ulnar (medial), parallel to the PIN's course (the nerve spirals around the lateral radius), using blunt dissection — Mayo scissors or finger dissection to spread the muscle fibres in line with their oblique run.
- Stay within the muscle until the nerve is seen: split only the superficial head initially. Distal to the arcade the PIN is cushioned within muscle, not applied to bone (Qawasmi 2025), but it lies only a few mm from the radial neck (closest in pronation) — so keep the forearm supinated and avoid sharp dissection on the periosteum (Heidari 2010).
- The PIN appears as a white cord a few mm in diameter on the deep surface of the supinator, between its two heads, spiralling from proximal-radial to distal-ulnar.
- Isolate it with a Penrose drain or vessel loop using a right-angle clamp or nerve hook — BLUNT dissection only, and avoid sharp work within 2cm of the nerve.
- Control the leash of Henry: the radial recurrent artery branches cross the PIN at the mid-supinator (2–3 small branches, approx 2.7cm distal to the lateral epicondyle — Low 1994); ligate them with fine ties or bipolar to prevent brisk bleeding.
- For PIN decompression (RTS / PIN palsy): split the supinator along its entire length from the arcade to the distal border, release the distal supinator edge (the site best seen through this posterior approach — Urch 2015), and excise any compressing lesion (ganglion, lipoma, rheumatoid synovium). Confirm the PIN glides freely with pronation-supination.
- For fracture ORIF: once the PIN is identified and protected, perform subperiosteal dissection of the radius and apply a 3.5mm LCP/DCP plate to the anterolateral surface (NOT directly over the PIN on the posterior surface), 6–8 holes with bicortical screws that do NOT penetrate the posterior cortex into the interosseous membrane.
- Before closing, re-check PIN mobility — pronate and supinate to confirm the nerve glides freely and is not trapped under a plate or compressed by a screw.
- Loosely approximate the supinator with 2-0 Vicryl (do NOT close it tightly — this can recompress the PIN); close the extensor-compartment fascia with 0-Vicryl, subcutis with 2-0 Vicryl, and skin with staples or 3-0 Nylon (removed at 10–14 days).
- Release the tourniquet before skin closure to identify and ligate any arterial bleeders and prevent a postoperative haematoma.
Iatrogenic PIN injury is reported in roughly 1–3% of posterior proximal-radius exposures and is the defining risk of the Thompson approach. Five safeguards hold it safe: (1) fully supinate the forearm before touching the supinator; (2) split the muscle in line with its fibres from radial to ulnar; (3) stay within muscle until the nerve is seen — blunt dissection only; (4) identify the arcade of Frohse first and incise it longitudinally if taut; and (5) avoid sharp dissection on the radial neck/periosteum, where the nerve lies only a few mm from bone. Recognise an injury early — finger/thumb extension weakness with PRESERVED wrist extension and NO sensory loss — and re-explore within 72 hours.
The entire safety profile of the Thompson (and Henry) approach rests on forearm position. Supination moves the PIN away from the radial neck and tuberosity by roughly 5mm (Qawasmi 2025); pronation brings it closest to bone (approx 8mm at 50mm distal to the radial head in supination, and tighter still in pronation — Heidari 2010). Supinate before you split the supinator, keep the forearm supinated while the nerve is exposed, and re-check position as the dissection moves along the shaft.
Dangers & Extensions
Structures at risk, by layer
- Why it is at risk
- The single most vulnerable structure — iatrogenic injury in approx 1-3% of posterior proximal-radius exposures; the nerve lies only a few mm from the radial neck, closest in pronation
- How to protect it
- Fully SUPINATE the forearm; split the supinator in line with its fibres from radial to ulnar; blunt dissection only; identify the arcade before splitting; avoid sharp dissection on the radial neck
- Why it is at risk
- Radial recurrent artery branches cross the PIN at the proximal supinator and bleed briskly if injured
- How to protect it
- Identify the crossing vessels (approx 2.7cm distal to the lateral epicondyle) and ligate with fine ties or bipolar cautery before dividing
- Why it is at risk
- The ECRB branch arises at/near the radial-nerve bifurcation; injury weakens wrist extension
- How to protect it
- Stay within the ECRB–EDC interval and keep dissection subperiosteal on the radius
- Why it is at risk
- They fan toward the interosseous membrane distal to the supinator's distal edge
- How to protect it
- Do NOT extend posterior dissection beyond the distal supinator edge; use the Henry approach for the distal 1/3
Extensile options. Extend proximally along the mobile wad (2–3cm) to reach the radial-nerve bifurcation, the radiocapitellar joint and the radial head for articular reconstruction or replacement. Distal extension is NOT safe beyond the distal supinator edge — the PIN terminal branches fan onto the interosseous membrane; for the distal third of the shaft, convert to the Henry volar approach. Closure & postoperative care. Confirm PIN mobility, loosely re-approximate the supinator (tight closure recompresses the nerve), and release the tourniquet before skin closure. After PIN decompression alone, a posterior splint for 48–72 hours is followed by immediate forearm rotation. After ORIF through this approach, protect forearm rotation for about 6 weeks (the supinator has been split), then progress; no lifting greater than 5kg for 12 weeks.
Procedures Through This Approach
- Radial nerve exploration / PIN decompression — the principal operation: radial tunnel syndrome and PIN palsy decompression (arcade of Frohse, leash of Henry, distal supinator border).
- Radial head fracture ORIF and radial head arthroplasty — posterior access to the radial head/neck for Mason II–III fractures; reserve ORIF for three or fewer articular fragments (Ring 2002).
- Both-bone forearm ORIF — proximal radial-shaft fixation when posterior access is specifically required (e.g. revision of a prior anterior approach).
- Rheumatoid elbow synovectomy with radial head excision — synovitis compressing the PIN at the arcade.
- Proximal-radius tumour resection (enchondroma, osteochondroma) or chronic osteomyelitis debridement via the posterior surface.
Viva & Exam Focus
ARCADEARCADE — arcade of Frohse anatomy and PIN compression
THOMPSONTHOMPSON — approach indications and technique
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old female presents with 9 months of lateral elbow pain exacerbated by gripping and turning doorknobs. She has failed 6 months of physical therapy, activity modification, NSAIDs, and one corticosteroid injection. Examination reveals tenderness 4cm distal to the lateral epicondyle over the mobile wad, pain with resisted middle finger extension, and pain with resisted supination. Grip strength is 70% of contralateral. EMG shows prolonged PIN motor latency 5.2ms (normal less than 4.5ms). How do you manage this patient?”
“A 35-year-old male presents after a motorcycle accident with a Mason type III comminuted radial head fracture. On examination he has 0/5 finger extension at the MCP joints, 0/5 thumb extension, but 5/5 wrist extension (ECRL intact) and normal sensation in the first dorsal web space. How do you manage the PIN palsy?”
“You are planning to fix a proximal radius shaft fracture (8cm distal to the radial head, transverse) in a 28-year-old male. The registrar suggests a Thompson approach for 'direct posterior access'. Do you agree? Justify your approach selection.”
Arcade of Frohse & the three PIN compression sites
- PIN enters the supinator at the arcade of Frohse approx 22mm distal to the radiocapitellar joint and approx 3.8cm distal to the lateral epicondyle (Qawasmi 2025, Low 1994)
- Fibrous arch at the proximal supinator edge; a firm tendinous band is more frequent in symptomatic radial-tunnel patients than in unselected cadavers (Hong 1989)
- Three PIN compression sites: (1) arcade of Frohse (most common), (2) leash of Henry (radial recurrent vessels), (3) distal supinator border — no single approach exposes all three (Urch 2015)
- PIN course: enters at the arcade, spirals around the lateral radius between the two supinator heads (cushioned within muscle distal to the arcade, closest to bone in pronation — Heidari 2010), exits at the distal supinator border
Supinator muscle & PIN motor innervation
- Supinator: origin lateral epicondyle (superficial head) plus supinator crest of ulna (deep head); insertion anterolateral radius from radial neck to middle 1/3 (45–55mm length); primary supinator with the elbow extended
- PIN innervates: ECRB, EDC, EDM, ECU, APL, EPL, EPB, EIP — all posterior forearm muscles EXCEPT brachioradialis and ECRL
- Brachioradialis and ECRL are innervated by the radial nerve BEFORE PIN bifurcation, so they are spared in PIN palsies
- PIN palsy features: finger extension weak (0–2/5 EDC), thumb extension weak (0–2/5 EPL), wrist extension PRESERVED (5/5 ECRL), NO sensory loss
- Distinguish from high radial nerve injury: lost wrist extension (ECRL 0/5) AND lost sensation in the first dorsal web space
Forearm position protects the PIN (Heidari 2010, Qawasmi 2025)
- Heidari 2010 (20 cadaveric arms): PIN closest to the radial neck in PRONATION (approx 13.3mm) vs SUPINATION (approx 21.6mm); only approx 8mm from the radius at 50mm distal to the radial head in supination
- Qawasmi 2025 (29 arms): PIN enters the arcade approx 22mm distal to the radiocapitellar joint; supination increases its separation from the radial tuberosity by approx 5mm
- Mechanism: supinate the forearm and stay subperiosteal to carry the PIN away from bone
Radial tunnel decompression & fracture evidence (Urch 2015, Ring 2002, Wu 2014)
- Urch 2015 (30 cadavers): no single approach exposed all five radial-tunnel compression sites; the posterior (Thompson) approach best visualised the DISTAL supinator border
- Ring 2002 (56 radial head ORIF): reserve ORIF for fractures with three or fewer articular fragments; more comminuted heads do poorly with fixation and are better replaced
- Wu 2014 (41 spontaneous PIN palsies with hourglass constrictions): 13 of 17 recovered with conservative care; surgery (neurolysis or neurorrhaphy/grafting) for failures or severe constriction
Technique — positioning, interval & supinator split
- Supine, arm on a hand table, forearm NEUTRAL rotation to expose the posterolateral radius; upper-arm tourniquet 250mmHg
- Posterolateral skin incision 8–12cm, 3–4cm proximal to the lateral epicondyle to 6cm distal, centred on the mobile wad
- Thompson interval: develop between ECRB (radial) and EDC (ulnar); mobilise brachioradialis plus ECRL anteriorly to expose the supinator
- With the forearm SUPINATED, palpate the arcade of Frohse (approx 3–4cm distal to the lateral epicondyle) and incise it longitudinally if taut
- Split the supinator from radial (lateral) to ulnar (medial), parallel to the PIN course, keeping the forearm supinated
- Identify the PIN as a white cord a few mm in diameter between the supinator heads; isolate with a Penrose drain using BLUNT dissection only
PIN decompression, fracture exposure & closure
- Release the entire supinator length (arcade to distal edge); control the leash of Henry with fine ties/bipolar; release the distal supinator border
- Confirm PIN mobility: pronate/supinate — the nerve should glide freely without tethering
- For ORIF: subperiosteal exposure, 3.5mm LCP on the ANTEROLATERAL radius (not directly over the PIN); screws must not penetrate the posterior cortex
- Closure: check PIN mobility, loosely approximate the supinator (do not close tightly — may compress the PIN), release the tourniquet BEFORE closure
Complications & outcomes
- Iatrogenic PIN injury: risk factors are sharp dissection on the radial neck/periosteum, aggressive retraction, and screw penetration; higher in pronation (supinate to protect)
- Immediate postop PIN palsy: re-explore within 72 hours; primary repair for a laceration, neurolysis plus observation for a contusion
- RTS surgical outcomes: good-to-excellent pain relief in the majority; poorer with long-standing symptoms, workers' compensation, and concurrent lateral epicondylitis
- PIN palsy recovery after radius fractures: flicker of finger extension at 6–12 weeks, full strength around 4–6 months in those who recover; baseline EMG at 3–4 weeks, repeat at 12 weeks
Global practice, guidelines & registries
- Internationally, the Henry (anterolateral) approach is the default for radial shaft fractures (PIN not directly exposed; supination carries it off bone); Thompson is reserved for PIN exploration, posterior radial head access, or revision
- Radial head fractures: ORIF for three or fewer fragments, arthroplasty for more comminuted patterns (Ring 2002); implant availability varies by region
- Antibiotic prophylaxis: a single first-generation cephalosporin within 60 minutes of incision (adjust per local antibiograms and allergy)
- VTE prophylaxis: routine pharmacological prophylaxis is generally NOT required for isolated upper-limb surgery in low-risk patients
Exam traps & high-yield points
- Do NOT default to Thompson for all proximal radius fractures — the PIN-sparing Henry approach is the workhorse
- Do NOT immediately explore all PIN palsies with radius fractures — most closed traumatic palsies recover; explore only if recovery stalls (Wu 2014)
- RTS pain is a few cm DISTAL to the lateral epicondyle (arcade of Frohse); lateral epicondylitis pain is AT the lateral epicondyle
- RTS is a CLINICAL diagnosis — electrodiagnostics are frequently normal; do not demand an abnormal EMG before operating (after excluding epicondylitis and cervical referral)
- Arcade of Frohse is the principal PIN compression site (Spinner): the PIN enters approx 22mm distal to the radiocapitellar joint (Qawasmi 2025, Low 1994)
References
PIN Anatomy at the Arcade of Frohse and Safe Zones for Retractor Placement
- 29 fresh cadaveric upper limbs: radial nerve bifurcated approx 5 plus or minus 3mm proximal to the radiocapitellar joint (RCJ)
- PIN entered the supinator at the arcade of Frohse approx 22 plus or minus 1mm distal to the RCJ
- PIN lay approx 13 plus or minus 2mm from the radial border of the radial tuberosity in pronation versus approx 19 plus or minus 2mm in supination - supination increased separation by approx 5mm
- Distal to the arcade the PIN was surrounded by muscle in ALL specimens, with no direct contact with bone
- Safe retractor placement: ulnar to the tuberosity proximally and radial to it distally, with the forearm supinated
PIN Distance to the Radius in Proximal Radial Exposures - Forearm Position Matters
- 20 cadaveric arms measuring PIN-to-radius distances during standard proximal-radius exposure
- Shortest distance from PIN to the radial neck: approx 21.6mm in supination versus approx 13.3mm in pronation
- At 30mm distal to the radial head: PIN approx 12.3mm from the radius in supination versus approx 22.3mm in pronation (relative to interosseous border the relationship reverses distally)
- At 50mm distal to the radial head: PIN only approx 8mm from the radius in supination
- The PIN's distance from bone varies markedly with both forearm rotation and the level of dissection
Surgical Approaches to the Radial Tunnel - No Single Window Exposes All Sites
- 30 fresh-frozen cadavers: 10 anterior, 10 anterolateral, and 10 posterior approaches to the radial tunnel compared
- Anterior and anterolateral approaches best visualised the proximal sites - fibrous bands at the radial head, the leash of Henry, the ECRB origin and the arcade of Frohse
- The posterior (Thompson-type) approach best visualised the DISTAL border of the supinator
- No single approach allowed complete visualisation and release of all five documented compression sites
- A larger uncut portion of supinator remained after the anterior approach than after the posterior approach
Open Reduction and Internal Fixation of Radial Head Fractures - When ORIF Works
- 56 patients with intra-articular radial head fractures treated by ORIF, reviewed at a mean of 48 months (30 Mason type 2, 26 Mason type 3)
- All 15 isolated, non-comminuted Mason type 2 fractures had a satisfactory result
- 13 of 14 Mason type 3 fractures with MORE than three articular fragments had an UNSATISFACTORY result (early failure or nonunion)
- Mason type 3 fractures split into two or three simple fragments did well (forearm rotation arc 100 degrees or more in all)
- Associated fracture-dislocation of the elbow or forearm compromised the result, especially forearm rotation
Spontaneous PIN Palsy with Hourglass Fascicular Constrictions - Treatment and Recovery
- 41 patients with complete spontaneous PIN palsy and hourglass-like fascicular constrictions
- Of 17 patients treated conservatively, 13 (76 percent) recovered well (final MRC grade 4 or better)
- Of 24 surgically treated patients, 20 (83 percent) recovered well
- Severe constriction responded better to neurorrhaphy or autografting (12 of 14 good) than to neurolysis alone
- Outcomes were markedly worse in patients aged 50 years or older; ultrasound reliably identified the constrictions