Prone Position | Common Peroneal Nerve at Risk | Buttress Plate for the Posterolateral Column
- The posterolateral tibial plateau is inaccessible from a standard anterolateral approach — a dedicated posterolateral exposure is required for direct buttress plating of this fragment.
- Prone (or lateral / floating, as Frosch originally described) positioning is mandatory — the posterolateral tibia cannot be exposed supine.
- The common peroneal nerve wraps around the fibular neck 1 to 2cm distal to the fibular head and is the critical structure at risk — identify it early and protect it throughout.
- The deep inter-compartmental plane is between peroneus longus (superficial peroneal nerve) and soleus (tibial nerve); for the proximal Frosch variant the lateral head of gastrocnemius is retracted medially and the soleus origin detached subperiosteally.
- A buttress (antiglide) plate on the posterior tibial surface prevents posterior displacement under axial load — an anterolateral plate cannot provide this buttress.
When & Why
What it exposes. The posterolateral approach gives direct access to the posterolateral tibial plateau, the posterior tibial cortex, and — via the Frosch modification — the lateral articular surface for direct visualisation and posterior buttress plating. It is the workhorse exposure for displaced posterolateral corner fragments of the tibial plateau. Why this approach (and not anterolateral). The tibial plateau has an inherent 7 to 10 degree posterior slope, and posterolateral fragments displace posteriorly under axial load combined with valgus stress. The posterolateral corner is the least supported region, and a fragment here simply cannot be buttressed from an anterolateral approach. Only a true posterolateral exposure places the plate on the posterior surface to resist that posterior displacement; malreduction leads to posterior subluxation and early post-traumatic arthritis. Indications. - Posterolateral tibial plateau fractures (isolated posterolateral column)
- Schatzker II fractures with a significant posterolateral split-depression component
- Bicondylar fractures (Schatzker V/VI) requiring posterolateral column fixation
- Revision surgery for posterolateral fragment malunion
- Access to the posterior tibial cortex for bone grafting (diaphyseal variant) Contraindications. - Medical unfitness for prone positioning (spinal cord injury, recent myocardial infarction)
- Active infection of the skin over the approach
- Severe posterior soft tissue compromise (delay surgery until recovery)
- Isolated anterior or medial fractures (use the appropriate alternative approach) Alternative approaches. - Anterolateral approach — for lateral plateau split/depression without a posterolateral fragment
- Posteromedial approach — for posteromedial fragments (saphenous nerve at risk, sensory only; generally considered safer)
- Extended lateral with fibular osteotomy — when combined anterolateral and posterolateral access is needed in one incision
- Anteromedial approach — for medial plateau fractures Position and landmarks. The patient is placed prone on a radiolucent table with chest rolls or a Wilson frame, all pressure points padded (face, chest, pelvis, patellae, ankles), arms abducted less than 90 degrees, and the C-arm verified to access from the lateral aspect. The affected knee is slightly flexed over a bolster — this relaxes the common peroneal nerve and reduces traction risk. A high-thigh tourniquet is used if planned (tourniquet-free surgery is also reasonable). Palpable landmarks are the fibular head, the biceps femoris tendon (inserting on the fibular head), Gerdy's tubercle (anterolateral tibial insertion of the iliotibial band), the lateral joint line, and the common peroneal nerve rolling over the fibular neck. The incision is longitudinal, behind the fibular head and anterior to the biceps tendon proximally, curving distally along the lateral fibular border for 8 to 12cm depending on the exposure required.
The Exposure
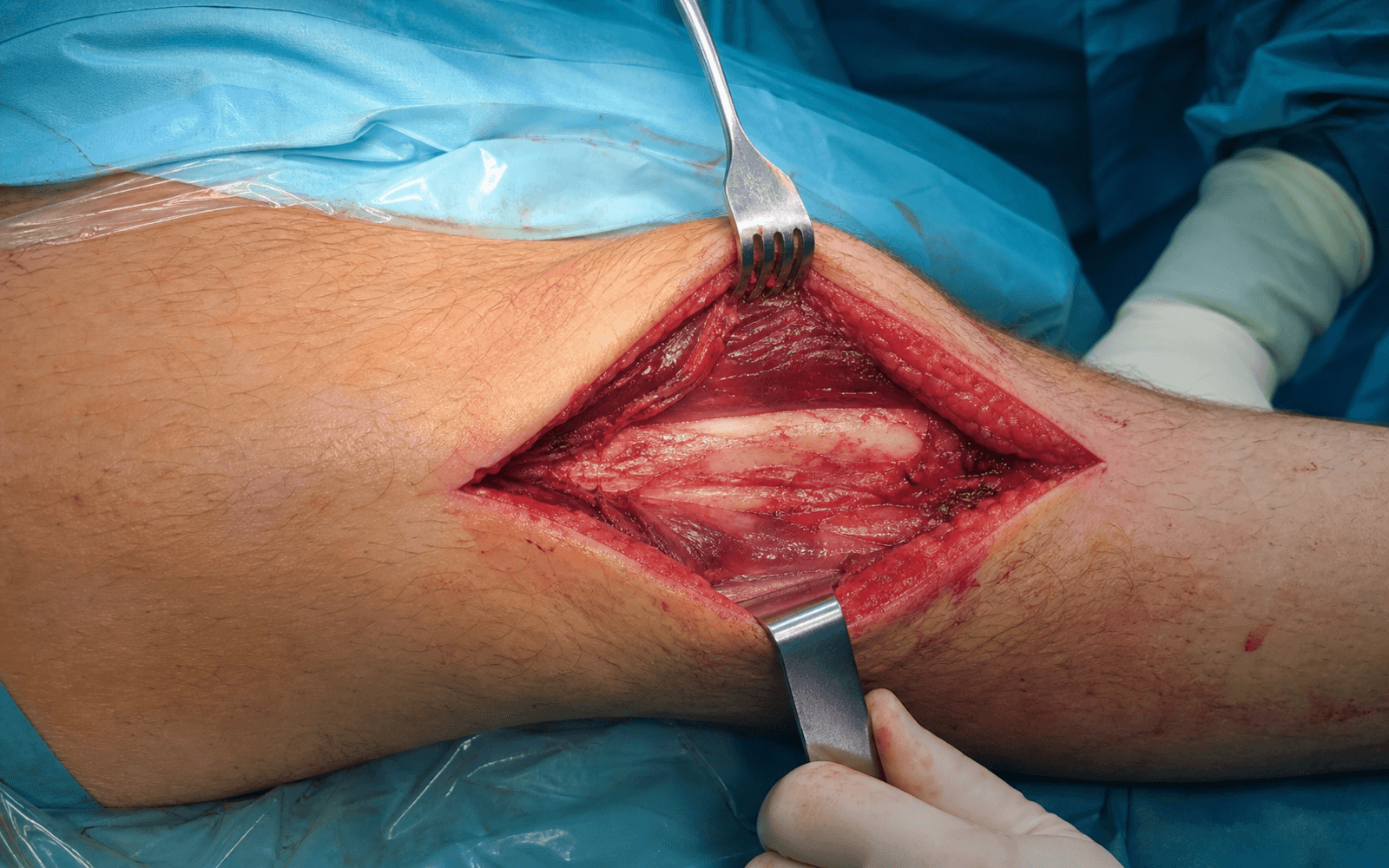
Work from skin down to the posterolateral tibial plateau along the fibular border, protecting the common peroneal nerve at every layer, then develop the peroneus-longus / soleus interval to apply a posterior buttress plate. The Frosch technique — a single incision combining a lateral arthrotomy with the posterolateral exposure, without fibular osteotomy — is the current standard.
Exposure sequence
- Confirm prone stability and radiolucent access; pad all pressure points and verify the C-arm.
- Mark the fibular head, biceps femoris tendon, Gerdy's tubercle and the lateral joint line; palpate the common peroneal nerve rolling over the fibular neck.
- Make a longitudinal incision behind the fibular head, anterior to the biceps tendon proximally, curving distally along the lateral fibular border for 8 to 12cm.
- Incise skin and subcutaneous tissue in line with the skin incision.
- Identify and protect the lateral sural cutaneous nerve if it is encountered crossing the field.
- Incise the fascia over the lateral (peroneal) compartment, which is supplied entirely by the superficial peroneal nerve — there is no true internervous plane in the superficial layer, so muscles are retracted rather than divided.
- The common peroneal nerve emerges from behind the biceps femoris tendon and wraps around the fibular neck 1 to 2cm distal to the fibular head.
- Identify it early, before any retraction, carefully trace its course, and pass a vessel loop or tape sling for gentle handling.
- Use knee flexion to relax nerve tension; never place metal or self-retaining retractors directly on the nerve and release retraction periodically.
- With the nerve slung and protected, perform a lateral arthrotomy below the lateral meniscus to visualise the articular surface.
- In the popliteal region, retract the lateral head of gastrocnemius medially (this carries the popliteal neurovascular bundle safely away, deep to it) and sharply detach the soleus origin from the posterior fibula and tibia, working toward the fibular neck where the CPN enters the peroneal musculature.
- Stay strictly subperiosteal to expose the posterolateral tibial plateau and the posterior cortex ready for plate application.
- In the more distal shaft variant, the plane is instead developed between peroneus longus (superficial peroneal nerve) and soleus / flexor hallucis longus (tibial nerve).
- Use bone tamps to elevate depressed articular fragments and pointed reduction clamps to reduce the split component.
- Hold the reduction with provisional K-wires while the plate is applied.
- Graft the metaphyseal void after elevation — options are cancellous autograft (same incision or distal femur), allograft, or a bone-graft substitute.
- Confirm on AP, lateral and oblique fluoroscopy; accept less than 2mm articular step-off and restore the posterior slope.
- Choose a 3.5mm T-plate, L-plate, or anatomic posterolateral tibial plateau plate (locking in poor bone), contoured to the posterior tibial surface.
- Apply the plate to the posterior tibial surface so it acts as a buttress against posterior displacement; proximal screws capture the posterolateral fragment and are directed anteriorly and medially.
- Use at least 3 to 4 screws in the proximal fragment and distal screws in healthy diaphyseal bone; check screw length under fluoroscopy to avoid intra-articular penetration.
- Copious irrigation, meticulous haemostasis; if a drain is used, exit it away from the CPN course.
- Close the capsule (if opened) and fascia with absorbable suture, then subcutaneous tissue and skin (staples or interrupted sutures).
- Document ankle dorsiflexion (CPN function) against the pre-operative baseline, immobilise for comfort, elevate the limb, and begin DVT prophylaxis.
The common peroneal nerve is the most important structure at risk in this approach. It wraps around the fibular neck only 1 to 2cm distal to the fibular head with very limited mobility, so traction or compression causes a foot drop. Identify it before any retraction, handle it only with a vessel loop, keep the knee flexed to relax tension, never place metal or self-retaining retractors on it, and release retraction regularly. Document ankle dorsiflexion before and after surgery.
There is no classical internervous plane in the superficial dissection; the approach relies on inter-compartmental dissection. For the proximal Frosch plateau variant, the deep interval is developed in the popliteal region by retracting the lateral head of gastrocnemius medially and detaching the soleus origin subperiosteally, exposing the posterolateral plateau while the popliteal bundle is protected medially. For the distal shaft variant, the interval lies between peroneus longus (superficial peroneal nerve) and soleus / flexor hallucis longus (tibial nerve). The unifying principles are early CPN identification and staying strictly on bone subperiosteally.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Common peroneal nerve (wraps the fibular neck 1 to 2cm distal to the head)
- Protection
- Identify before any retraction; vessel loop; knee flexion; no metal or self-retaining retractors on the nerve
- Structure at risk
- Peroneal artery and veins
- Protection
- Stay in the correct plane; ligate small branches, repair any major vessel injury
- Structure at risk
- Lateral inferior geniculate artery (popliteal branch at the joint line)
- Protection
- Ligate if bleeding during capsular incision — does not require repair
- Structure at risk
- Lateral meniscus
- Protection
- Incise the capsule carefully below the meniscus; protect during reduction; repair peripheral tears
CPN injury management. If the nerve is found transected intra-operatively, perform a primary repair. For a suspected neurapraxia, observe and document, then arrange urgent EMG / nerve conduction studies at 3 weeks (after Wallerian degeneration if the injury is axonal). For a post-operative foot drop with no clinical or EMG recovery by 3 months, consider nerve exploration; an established permanent foot drop is managed with an ankle-foot orthosis and, if refractory, tendon transfer (tibialis posterior to the dorsum).
Common peroneal nerve injury in tibial plateau surgery ranges from 3 to 20 percent depending on approach and complexity, with posterolateral approaches carrying higher risk than anterolateral. Most injuries are neurapraxias that recover, but permanent foot drop occurs in roughly 1 to 3 percent and is a devastating complication. Across this approach specifically, CPN palsy is quoted at about 3 to 5 percent.
Extensile options. - Fibular osteotomy — when the standard approach gives inadequate exposure of a large or complex posterolateral fragment: an oblique osteotomy of the fibular neck (posterolateral to anteromedial), performed only after the CPN is identified and protected, repaired at the end with a small plate or tension band. It adds morbidity — fibular nonunion in about 5 percent and higher CPN risk.
- Proximal extension — along the biceps femoris toward the posterolateral femoral condyle; the CPN becomes more superficial proximally, increasing risk.
- Distal extension — along the fibula to reach the tibial diaphysis for fractures extending into the shaft, staying in the same intermuscular plane.
- Combined approaches — for bicondylar Schatzker V/VI fractures: posterolateral for the PL fragment plus posteromedial (PM fragment) and/or anterolateral (lateral column), planned around positioning (see below). Complications
- Incidence
- 3-5%
- Prevention and treatment
- Careful technique, early identification, knee flexion; observe and AFO, EMG at 3 weeks, explore if no recovery by 3 months
- Incidence
- 2-5% (20-30% with poor soft tissue)
- Prevention and treatment
- Wait for wrinkle-test-positive soft tissues; antibiotics; irrigation and debridement if deep
- Incidence
- 20-40% long-term
- Prevention and treatment
- Anatomic articular reduction (less than 2mm step-off); analgesia, weight loss, eventual TKA if severe
- Incidence
- Under 5%
- Prevention and treatment
- Bone graft the metaphyseal void, stable fixation; revision ORIF or TKA if symptomatic
- Incidence
- 2-5%
- Prevention and treatment
- Chemoprophylaxis (LMWH or aspirin) until mobile, early mobilisation
Operating through compromised soft tissue raises infection risk from 2 to 5 percent up to 20 to 30 percent. Use the wrinkle test (skin that wrinkles on gentle compression has adequate dermal blood flow), wait for swelling and blisters to settle (typically 7 to 14 days), and bridge an unstable fracture with a spanning external fixator in the interim. Serous blisters indicate intact epidermis; haemorrhagic blisters indicate deeper injury.
Outcomes by fracture pattern. Good outcomes track anatomic articular reduction. Isolated posterolateral split fractures achieve good or excellent results in roughly 85 to 90 percent with 15 to 20 percent OA at 10 years; posterolateral split-depression 75 to 85 percent with 25 to 30 percent OA; and bicondylar (Schatzker V/VI) 60 to 75 percent with 40 to 50 percent OA. Of CPN injuries, about 60 percent recover fully, 30 percent partially, and 10 percent are permanent. Closure summary. Irrigate, achieve haemostasis, drain (away from the CPN) if preferred, close capsule and fascia with absorbable suture, approximate subcutaneous tissue and close skin. Rehabilitate with non-weight-bearing or touch weight-bearing for 6 to 12 weeks, early ROM aiming for 0 to 90 degrees by 6 weeks, and DVT prophylaxis until mobile.
Procedures Through This Approach
- Posterolateral tibial plateau fracture ORIF (isolated posterolateral column) — the principal operation, with posterior buttress plating.
- Schatzker II lateral split-depression with a significant posterolateral component.
- Bicondylar Schatzker V/VI — posterior column fixation (combined with posteromedial and/or anterolateral approaches in prone or floating position).
- Revision ORIF for posterolateral fragment malunion.
- Posterolateral tibial diaphyseal exposure and posterior tibial cortex bone grafting (distal/shaft variant).
- The fibular-osteotomy modification for complex or large fragments needing wider exposure.
Viva & Exam Focus
POSTEROLATPOSTEROLAT — the posterolateral exposure
CPN SAFECPN SAFE — protect the nerve
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old presents after a motorcycle accident with a tibial plateau fracture. CT shows a posterolateral split-depression fragment. How would you approach this?”
“During a posterolateral approach, the patient develops weak ankle dorsiflexion post-operatively. What is your assessment and management?”
“You are planning surgery for a Schatzker VI tibial plateau fracture with significant posteromedial and posterolateral fragments. How would you approach this?”
“What are the key differences between the posterolateral and posteromedial approaches to the tibia?”
“A patient has a posterolateral tibial plateau fragment but significant anterior soft tissue swelling and blistering. How does this affect your surgical planning?”
Patient position
- Prone is essential for posterolateral tibial access
- Alternative: lateral decubitus with the affected side up
- Cannot access the posterolateral plateau from supine
- Pad all pressure points; radiolucent table for fluoroscopy
CPN protection
- CPN wraps the fibular neck 1 to 2cm distal to the head
- Identify early — before any retraction
- Vessel loop or tape sling for protection
- No metal or self-retaining retractors on the nerve
- Knee flexion relaxes nerve tension
Internervous plane
- Between peroneus longus (superficial peroneal nerve) and soleus (tibial nerve)
- Inter-compartmental plane between lateral and posterior compartments
- Frosch variant: retract lateral gastrocnemius medially, detach soleus origin subperiosteally
- Stay strictly on bone to expose the posterolateral plateau
Buttress plate principle
- The posterolateral fragment displaces posteriorly under axial load
- Buttress plate on the posterior surface prevents displacement
- An anterolateral plate cannot buttress a posterolateral fragment
- 3.5mm T-plate, L-plate, or anatomic posterolateral plate
- Screws directed anteriorly and medially
CT planning
- CT is essential for all tibial plateau fractures
- Posterolateral fragments are frequently underappreciated on plain films
- The three-column concept guides approach selection
- Less than 2mm articular step-off is the goal
- Post-operative CT if any concern about reduction
Complications
- CPN injury 3 to 5 percent (most recover within 12 months)
- Post-traumatic arthritis 20 to 40 percent long-term
- Infection 2 to 5 percent (higher with soft tissue compromise)
- Fibular nonunion if osteotomy performed (about 5 percent)
- DVT prophylaxis until mobile
References
Guidelines, Registries & Global Practice Tibial plateau fractures are managed at trauma centres worldwide, and the principles are convergent across examination systems. CT-based assessment of every operatively considered plateau fracture and the three-column concept (Luo) are now near-universal in defining the posterior columns and selecting the approach. Side-by-side principles (where guidance converges): | Body | Position on plateau fractures |
|------|------------------------------| | AO Foundation | CT mandatory for articular fractures; posterior fragments need dedicated posterior / posterolateral approaches and buttress fixation; staged management with spanning external fixation for high-energy injuries with soft-tissue compromise | | BOA / BOAST (open and soft tissue) | Early soft-tissue assessment, photographic documentation, joint orthoplastic care for open injuries; definitive fixation only once soft tissues permit | | OTA / AAOS | Anatomic articular reduction and restoration of the mechanical axis as primary goals; CT-based planning is standard of care | Registry / population evidence: - Population-based incidence is approximately 10 per 100,000 per year, with a bimodal distribution (high-energy in younger men, fragility pattern in women older than 50).
- Long-term ORIF cohorts show post-traumatic arthritis in roughly 30 percent at long follow-up, strongly driven by residual malalignment greater than 5 degrees rather than age. Global practice variation. In high-resource settings, dedicated posterolateral plates, fragment-specific implants and routine CT are standard. In resource-limited settings, the same biomechanical principle (posterior buttress) is achieved with contoured one-third tubular or small-fragment T/L plates, and external fixation has a larger role for temporisation and occasionally definitive treatment. Consent (globally applicable): discuss common peroneal nerve injury (approximately 3 to 5 percent in this approach, mostly transient), infection (2 to 5 percent, higher with soft-tissue compromise), post-traumatic arthritis (long-term roughly 20 to 40 percent), stiffness, and the possibility of future total knee arthroplasty if articular damage is severe.
For the Operative Surgery station you must be able to describe the posterolateral approach systematically: prone positioning, CPN identification and protection, the inter-compartmental plane, and buttress-plate placement. Know the evidence for CT scanning of all tibial plateau fractures and when combined approaches are needed.
A New Posterolateral Approach Without Fibula Osteotomy
- Approximately 7 percent of tibial plateau fractures affect the posterolateral corner
- A single posterolateral skin incision combining lateral arthrotomy and posterolateral exposure allows direct articular visualisation and posterior buttress plating
- Fibular osteotomy is not required and posterolateral corner fragments are not stripped of their soft-tissue attachments
- Reduction and stable fixation achieved in 6 of 7 patients with no approach-related complications or loss of reduction
Operative Treatment of Tibial Plateau Fractures: 5- to 27-Year Follow-up
- 202 fractures treated by ORIF; 109 reviewed at a mean of 14 years (range 5 to 27 years)
- Secondary osteoarthritis developed in 31 percent but was well tolerated in most
- Residual malalignment greater than 5 degrees was associated with significantly more moderate-to-severe arthritis (27 percent vs 9.2 percent, p = 0.02)
- Monocondylar fractures had significantly better functional results than bicondylar fractures; age did not affect outcome
Three-Column Fixation for Complex Tibial Plateau Fractures
- Introduced the CT-based three-column concept (lateral, medial, posterior columns) for Schatzker V/VI fractures
- Posterior column fragments are best addressed through dedicated posterior approaches rather than from anterior windows
- 29 complex fractures fixed column-specifically in a floating position achieved satisfactory reduction in all but one case
- Mean HSS score 90 and mean knee ROM 2.7 to 123.4 degrees at 2 years
Frosch Approach for Posterolateral Tibial Plateau Fractures: Lateral Arthrotomy, Reduction, Plate Fixation
- 23 posterolateral plateau fractures (Schatzker II and V) treated via the Frosch approach with plate fixation
- Excellent radiographic reduction (MPTA, posterior slope angles) and mean HSS score 88.0 at mean 30.5 months
- Transient skin numbness in 3 patients (resolved by 6 months); no permanent common peroneal nerve injury
- A single incision allowed visualisation of both the posterolateral and lateral plateau
Population-Based Epidemiology of Tibial Plateau Fractures
- Population-based incidence of tibial plateau fractures was 10.3 per 100,000 per year
- Mean age 52.6 years; peak frequency between 40 and 60 years in both sexes
- Most common pattern was AO type 41-B3 (35 percent), followed by 41-C3 (17 percent) on validated CT-based classification
- Incidence rose in women older than 50 years (osteoporotic pattern) but fell in men older than 50