Transpsoas L1-2 to L4-5 | Lateral retroperitoneal corridor | Lumbar plexus at risk
- The lateral transpsoas corridor avoids the great vessels. A lateral retroperitoneal approach (patient in lateral decubitus) traverses the psoas to reach the disc; the aorta and vena cava stay anterior and are not mobilised, so vascular injury is largely avoided and blood loss is low (commonly 50-150mL, about 23mL per level — Oliveira 2010).
- The lumbar plexus is the most vulnerable structure. The L2-L4 contribution to the lumbosacral plexus lies within the posterior psoas. Cadaveric mapping shows progressive ventral migration caudally — plexus-to-dorsal-endplate ratio 0 at L1-2, 0.11 at L2-3, 0.18 at L3-4, 0.28 at L4-5 (Benglis 2009), making L4-5 the highest-risk level. Motor weakness ranges 0.7-33.6% across series, the majority transient (Ahmadian/Uribe 2012).
- Neuromonitoring is standard of care. Triggered EMG with directional/threshold mapping during dilation and retraction. Falling thresholds (commonly less than 5-10mA) indicate the dilator is close to neural tissue — reposition or redirect more anteriorly rather than push through.
- Safe zones vary by level. L2-3 is safest (plexus most dorsal, target the anterior-to-mid disc), L3-4 intermediate, L4-5 highest risk (plexus most ventral, ratio 0.28 — Benglis 2009). Many surgeons avoid transpsoas XLIF at L4-5, favouring anterior-to-psoas (ATP) or pre-psoas (OLIF) corridors there.
- XLIF is generally not feasible at L5-S1. The iliac crest and iliac vessels block the lateral corridor in most patients; use ALIF or TLIF for L5-S1. Standard XLIF levels are L1-2 to L4-5.
- Psoas traversal technique is critical. Blunt sequential dilation parallel to the muscle fibres (anterior-to-posterior trajectory, never perpendicular), with EMG mapping at each step. Minimise total retraction/psoas-compression time — prolonged retraction drives higher rates of postoperative thigh symptoms and weakness.
- Indirect decompression via disc-height restoration. A tall, wide cage restores disc and foraminal height (mean disc height +42%, foraminal height +13.5%, foraminal area +24.7%, canal diameter +33% — Oliveira 2010), often avoiding direct posterior decompression. It fails where there is bony/congenital stenosis or locked facets.
- Supplemental fixation is usually required. Stand-alone XLIF can work in selected low-grade cases, but subsidence and pseudarthrosis are higher without posterior fixation; bilateral pedicle screws are the usual construct for multilevel, deformity and osteoporotic bone.
When & Why
The lateral lumbar interbody fusion (XLIF/LLIF) approach is a minimally invasive lateral retroperitoneal transpsoas corridor to the lumbar disc, used from L1-2 to L4-5. The patient lies in the lateral decubitus position; the surgeon bluntly dilates through the psoas to the disc and implants a large cage spanning both lateral apophyseal rims. Because the great vessels remain anterior and are never mobilised, vascular injury is largely avoided and blood loss is low (commonly 50-150mL, about 23mL per level in early stenosis cohorts — Oliveira 2010). The trade-off is the lumbar plexus, which lies within the posterior psoas and is the critical structure at risk. XLIF (NuVasive) and DLIF (Medtronic) are transpsoas variants of the same corridor. Anterior-to-psoas (ATP) and pre-psoas (OLIF) approaches are different — they pass anterior to the psoas to largely avoid plexus traversal, at the cost of reintroducing vascular, visceral and sympathetic-chain risk. The technique was developed by Pimenta (Brazil, 2001) as eXtreme Lateral Interbody Fusion.
XLIF (NuVasive) and DLIF (Medtronic) are transpsoas LLIF variants of the same corridor; LLIF is the generic term. ATP/anterior-to-psoas and pre-psoas/OLIF are different — they work anterior to the psoas, largely avoiding plexus traversal but reintroducing vascular, visceral and sympathetic-chain risk. Crucially, meta-analysis shows fusion rates are broadly similar across ALIF, PLIF, TLIF and LLIF (Teng/Phan 2017), so approach choice should be driven by level, decompression need and deformity goals — not by an assumed fusion-rate advantage.
Indications. The corridor is ideal for levels L1-2 to L4-5 where indirect decompression, coronal correction, or a virgin revision route is the goal: - Degenerative scoliosis (L2-L4 curves) — restores disc height and coronal alignment without posterior muscle disruption
- Foraminal stenosis (L2-3, L3-4) — indirect decompression via disc-height restoration (about 80% stenosis improvement — Oliveira 2010)
- Central stenosis with instability — interbody support, supplemented with posterior instrumentation for direct decompression
- Adjacent-segment disease above a fusion — extends the construct through a virgin corridor
- Pseudarthrosis after TLIF/ALIF — lateral revision through unscarred tissue
- Burst fractures (L2-L4) and Chance fractures — anterior-column reconstruction after posterior fixation
- Vertebral body tumour (L2-L4) — corpectomy with cage reconstruction
- Discitis/osteomyelitis — debridement and fusion avoiding ventral great vessels Contraindications. - Absolute: L5-S1 (iliac crest blocks access); prior retroperitoneal surgery (e.g. nephrectomy) obliterating the corridor with dense adhesions; vascular malformation or aneurysm in the corridor; active psoas abscess
- Relative: L4-5 in a high-risk patient (diabetes or pre-existing neuropathy, obesity degrading EMG signals, prior L4-5 surgery); severe osteoporosis (higher subsidence — use the widest cage, preserve the endplate rim, add posterior fixation); transitional lumbosacral anatomy (wrong-level risk); BMI greater than 35; prior lateral abdominal hernia repair (mesh-disruption risk)
- XLIF / LLIF
- Very low — great vessels stay anterior, not mobilised; segmental and iliolumbar vessels at risk
- ALIF
- Higher — great vessels mobilised; left iliac vein vulnerable
- TLIF
- Very low — posterior approach
- XLIF / LLIF
- Lumbar plexus: motor weakness 0.7-33.6%, sensory 0-75% across series, mostly transient (Ahmadian/Uribe 2012)
- ALIF
- Superior hypogastric or sympathetic plexus (retrograde ejaculation in males)
- TLIF
- Exiting or traversing nerve root and dural tear
- XLIF / LLIF
- Low — commonly 50-150mL (about 23mL per level — Oliveira 2010)
- ALIF
- Higher — great-vessel mobilisation
- TLIF
- Higher — posterior muscle and epidural venous bleeding
- XLIF / LLIF
- High — pooled anterior/lateral 95.9% in MIS deformity (Phan 2016)
- ALIF
- High — best disc-height and segmental-lordosis restoration (Teng/Phan 2017)
- TLIF
- High — similar across approaches (Teng/Phan 2017)
- XLIF / LLIF
- Grade II-III 30% with 18mm vs 11% with 22mm cages; worse with osteoporosis (Marchi 2013)
- ALIF
- Lower — large footprint distributes load
- TLIF
- Higher — smaller cage, less endplate contact
- XLIF / LLIF
- Effective — foraminal height +13.5%, area +24.7%, canal diameter +33% (Oliveira 2010)
- ALIF
- Good — relies on anterior disc-height restoration
- TLIF
- Allows direct decompression but less interbody distraction
- XLIF / LLIF
- Contraindicated — iliac crest and iliac vessels block the corridor
- ALIF
- Ideal — wide anterior exposure
- TLIF
- Feasible (a high crest may limit it in 10-15%)
- XLIF / LLIF
- Steep — about 30-50 cases (neuromonitoring interpretation, psoas navigation)
- ALIF
- Moderate — 20-30 cases
- TLIF
- Moderate — 20-30 cases
Position & landmarks. True lateral decubitus, with a table break at the iliac crest that opens the lateral disc space by 5-10mm; hips and knees flexed 30-45 degrees to relax the psoas; axillary roll and fibular-head padding to protect the brachial and common peroneal nerves. Mark the disc centre on AP and lateral fluoroscopy. Side: left side up for L2-3/L3-4 (the aorta is easier to retract than the vena cava); right side up for L4-5 (avoids the left iliac vessels).
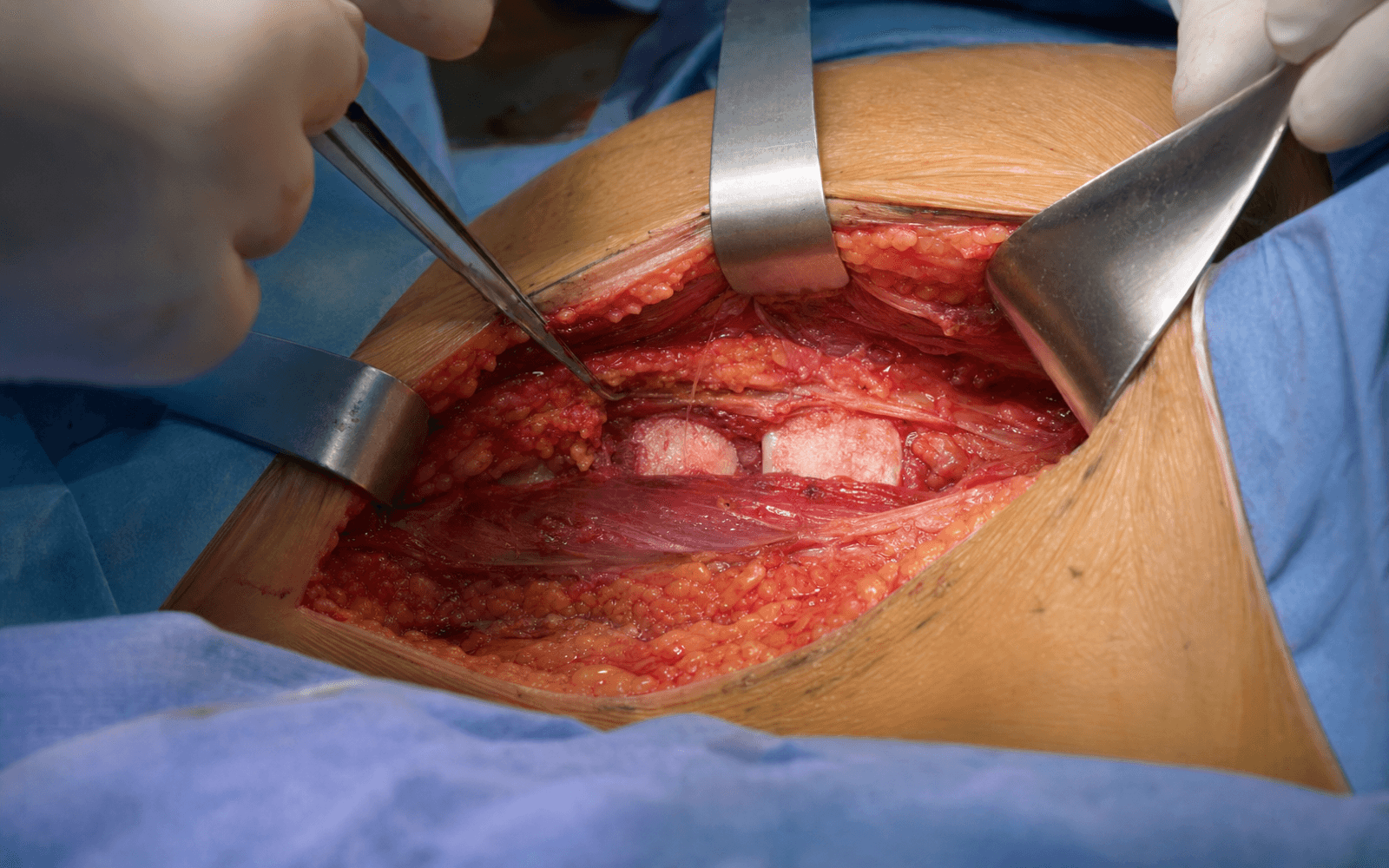
The Exposure
Work from skin to disc through the lateral abdominal wall, sweep the peritoneum anteriorly, then bluntly dilate through the psoas parallel to its fibres with continuous EMG mapping until a wide cage can be impacted across both lateral apophyseal rims. The lumbar plexus within the posterior psoas is the structure that governs the whole operation.
Exposure sequence
- General anaesthesia, endotracheal intubation; avoid muscle relaxant after induction — it abolishes the EMG you depend on for psoas navigation.
- True lateral decubitus; hips and knees flexed 30-45 degrees to relax the psoas; table break at the iliac crest to open the lateral disc space by 5-10mm; axillary roll and fibular-head padding.
- Tape the chest and pelvis securely to the table; confirm the level and disc-space opening on AP and lateral fluoroscopy.
- Side: left side up for L2-3/L3-4 (aorta easier to retract than the vena cava); right side up for L4-5 (avoids the left iliac vessels).
- Place needle electrodes in iliopsoas (L1-L2), vastus lateralis (L2-L4, femoral), tibialis anterior (L4-L5) and gastrocnemius (S1-S2).
- Stimulate from 0.5mA upward. Greater than 10mA means the probe is far from nerve (safe); 5-10mA is a warning (about 2-5mm); less than 5mA is danger (less than 2mm — abort and redirect more anteriorly).
- Optional somatosensory evoked potentials (tibial nerve) for multilevel deformity constructs.
- Localise the disc centre on AP and lateral fluoroscopy; make a 3-5cm oblique incision directly over it, about 8-12cm from the midline (varies with habitus).
- Incise external oblique fascia (fibres run inferiorly and medially), then blunt-split internal oblique and transversus abdominis parallel to their fibres (avoids denervation).
- Palpate retroperitoneal fat and sweep the peritoneum anteriorly off the psoas; identify the firm psoas anteriorly and quadratus lumborum posteriorly.
- Under lateral fluoroscopy place the K-wire in the disc centre — target the anterior third at L2-3/L3-4 and the middle third at L4-5 (the plexus is posterior cranially and migrates anteriorly caudally).
- Stimulate the K-wire (threshold greater than 10mA is safe); pass a 14-16mm blunt dilator over it parallel to the psoas fibres (anterior-to-posterior trajectory), stimulating as you go — if the threshold drops below 5mA, abort and redirect more anteriorly.
- Sequentially dilate (18-20mm, then 22-24mm), stimulating each dilator; dock the expandable retractor on the disc and expand gradually to a 30-40mm corridor, re-stimulating the blades after each expansion.
- Blunt, fibre-parallel dilation and minimal total retraction time are the keys to avoiding neuropraxia — never sharp dissection or aggressive retraction through the psoas.
- Remove annulus and nucleus with pituitary rongeurs, curettes and shavers; palpate the contralateral anterior vertebral body edge to confirm you have crossed the midline.
- Scrape the cartilaginous endplate to bleeding subchondral bone, but preserve the peripheral cortical/apophyseal rim — the strongest endplate bone, which resists subsidence.
- Pack the cage (typically 50-60mm AP by 18-22mm wide by 10-14mm tall) with local autograft, allograft cancellous chips or BMP.
- Impact a wide cage that spans both lateral apophyseal rims — wider cages roughly halve subsidence (Grade II-III 11% with 22mm vs 30% with 18mm — Marchi 2013).
- Confirm position on AP and lateral fluoroscopy — centred on the disc, parallel to the endplates, no vertebral-body breach.
- Gradually collapse the retractor (avoid sudden nerve traction from rapid decompression); achieve haemostasis on the psoas; close transversus abdominis, internal oblique and external oblique fascia with absorbable suture; subcuticular skin closure.
- Mobilise on day 0-1; brace selectively (stand-alone constructs, poor bone, deformity); examine hip flexion, knee extension and anterior thigh sensation immediately and at routine follow-up; X-rays at 6 weeks, 3, 6 and 12 months.
The lumbar contribution to the lumbosacral plexus (L2-L4) within the posterior psoas is the single most vulnerable structure in this approach. Across the literature postoperative motor weakness ranges 0.7-33.6% and sensory disturbance 0-75%, reflecting heterogeneous reporting and technique (Ahmadian/Uribe 2012); the great majority of deficits are transient. Cadaveric mapping shows the plexus migrates ventrally caudally — position ratio about 0.11 at L2-3 rising to about 0.28 at L4-5 (Benglis 2009) — making L4-5 the highest-risk level, where many surgeons prefer an ATP/pre-psoas (OLIF) corridor or TLIF. Safe traversal means: triggered or directional EMG throughout; blunt anterior-to-posterior dilation; targeting the anterior-to-mid disc; minimal psoas-retraction time; and redirecting more anteriorly (or abandoning the corridor) if thresholds fall. Anterior thigh sensory symptoms are the commonest early complaint; iliopsoas/quadriceps weakness also occurs and largely recovers — in one transpsoas series 54.9% had early weakness with 92.3% resolved by 3 months and all by 2 years, and every case of thigh numbness involved an L4-5 level (Le/Uribe 2013).
Three habits keep the psoas safe: dilate BLUNT and parallel to the muscle fibres (anterior-to-posterior, never perpendicular), target the anterior-to-mid disc (the plexus is posterior at L2-3 and migrates anteriorly caudally), and keep total retraction time as short as possible — prolonged compression is the main driver of postoperative thigh symptoms and weakness.
The lateral cage spans both lateral cortical rims — the strongest endplate bone (the apophyseal ring) — giving far greater endplate coverage and support than a posteriorly inserted TLIF cage. That wide footprint is what powers the indirect foraminal decompression and the coronal/sagittal correction, and it is why wider cages resist subsidence (Marchi 2013). Preserve the peripheral endplate rim so the footprint has something strong to rest on.
Dangers & Extensions
The dominant dangers are neurological (the lumbar plexus), vascular (segmental vessels and the iliolumbar vein at L4-5), and mechanical (cage subsidence). Visceral injury is rare because the peritoneum is swept anteriorly.
- Structure at risk
- Lumbar plexus — femoral nerve (L2-L4) worst; also genitofemoral, lateral femoral cutaneous, obturator
- How to protect it
- Triggered/directional EMG throughout; blunt anterior-to-posterior dilation; target anterior-to-mid disc; minimal retraction time
- Structure at risk
- Plexus most ventral here (ratio 0.28 — Benglis 2009); femoral and genitofemoral nerves closest
- How to protect it
- Prefer ATP/pre-psoas (OLIF) or TLIF; if transpsoas, use a mid-to-anterior target with low retraction time
- Structure at risk
- Segmental lumbar vessels (4 pairs) and ascending lumbar vein — avulsion during retractor placement
- How to protect it
- Direct pressure, expand retractor to compress vessel against the body, bipolar/Surgicel; vascular surgery if uncontrolled
- Structure at risk
- Iliolumbar vein crossing the L5-S1 disc — massive haemorrhage if lacerated (5-8mm, high-flow vessel)
- How to protect it
- Identify on preoperative imaging; careful caudal retractor placement; immediate laparotomy if injured
- Structure at risk
- Sympathetic trunk — displaced anteriorly by retraction
- How to protect it
- Usually subclinical (unilateral leg warmth); much lower risk than ALIF, where the superior hypogastric plexus is dissected
- Structure at risk
- Bowel (less than 0.5%) and kidney (less than 0.1%, low-lying kidney at L1-2)
- How to protect it
- Sweep the peritoneum anteriorly with blunt dissection; review kidney position on preoperative CT
Plexus most dorsal (ratio 0.11); the anterior-to-mid disc is the safer working window (Benglis 2009).
Plexus ratio 0.18; standard transpsoas target with EMG mapping.
Plexus most ventral (ratio 0.28); smallest safe dorsal window — consider ATP/OLIF or TLIF (Benglis 2009).
Iliac crest and iliac vessels block the corridor; use ALIF or TLIF.
Neurological complications. Anterior thigh dysesthesia (sensory neuropraxia of the genitofemoral and lateral femoral cutaneous nerves) is the commonest early complaint — immediate numbness about 19% in a refined single-surgeon series (Le/Uribe 2013), with wider ranges across the literature — and the large majority resolve over weeks to months; manage with reassurance, gabapentin or pregabalin, and desensitisation. Hip-flexor or quadriceps weakness (femoral nerve, L2-L4) is the most serious motor deficit: reported across a wide range (0.7-33.6%, Ahmadian/Uribe 2012), level-dependent (L4-5 highest), and largely transient (54.9% early weakness with 92.3% resolved by 3 months and all by 2 years — Le/Uribe 2013). Grade an EMG/NCS at about 3 weeks to distinguish neuropraxia (conduction block, good prognosis) from axonotmesis (no motor units, worse), start gait training and progressive strengthening, brace with a knee immobiliser if quadriceps is less than 3/5, and repeat EMG at 3, 6 and 12 months. Exploration is rarely indicated — reserved for suspected transection (immediate complete paralysis, no voluntary motor units) or a non-resolving compressive haematoma. Functional recovery can occasionally be late (documented up to about a year — Ahmadian/Uribe 2013, PMID 23432325). Cage subsidence is common, early (by about 6 weeks, predominantly at the inferior endplate), and worse with osteoporosis, endplate violation and narrow cages (Grade II-III about 30% with 18mm vs 11% with 22mm — Marchi 2013). Prevent it with the widest cage that spans both apophyseal rims, an intact peripheral endplate rim, supplemental posterior fixation, and bone-health optimisation. Manage mild (less than 3mm, asymptomatic) subsidence with observation; moderate (3-5mm, recurrent symptoms) with supplemental posterior pedicle-screw fixation; and severe (greater than 5mm or cage extrusion) with revision and strut/corpectomy reconstruction. Vascular complications (1-2%) are usually venous, from segmental-vessel avulsion during retractor placement — control with direct pressure, expanding the retractor against the vertebral body, bipolar electrocautery and haemostatic agents, with vascular-surgery ligation if uncontrolled. Iliolumbar vein injury at L4-5 is the feared event: sudden massive haemorrhage requiring immediate conversion to open laparotomy, common-iliac-vein control, and a massive transfusion protocol (1:1:1 PRBC:FFP:platelets). Visceral and infectious complications are rare. Bowel injury (less than 0.5%) from retractor perforation needs primary repair or resection with broad-spectrum (anaerobic) cover; kidney injury (less than 0.1%, low-lying kidney at L1-2) is graded on contrast CT and managed conservatively unless the collecting system or vascular pedicle is involved. Superficial wound infection (1-2%) is lower than TLIF; deep discitis or psoas abscess (0.5-1%) needs culture-directed IV antibiotics for 6-12 weeks and CT-guided drainage where appropriate. Extensile options. The corridor extends cephalad to thoracolumbar levels (for adult deformity, watching for a low-lying kidney and the diaphragm) and is used caudally to L4-5 where the iliac crest permits. Multilevel degenerative scoliosis is the archetypal indication, fusing several levels through the same small muscle-splitting corridor. Closure is in layers over the three abdominal-wall muscles, with selective bracing for stand-alone, poor-bone or deformity constructs.
Procedures Through This Approach
- Degenerative lumbar scoliosis (L2-L4 curves) — the archetypal XLIF indication: multilevel disc-height restoration and coronal correction through one muscle-splitting corridor.
- Foraminal stenosis at L2-3 and L3-4 — indirect decompression via disc/foraminal height restoration (Oliveira 2010), often avoiding a direct posterior decompression.
- Adjacent-segment disease above a prior fusion — extends the construct through a virgin lateral corridor.
- Pseudarthrosis revision after failed ALIF or TLIF — lateral route through unscarred tissue.
- Anterior-column reconstruction for L2-L4 burst fractures and Chance fractures (after posterior fixation).
- Lateral corpectomy for vertebral-body tumour (L2-L4), and debridement and fusion for discitis/osteomyelitis.
- Stand-alone or instrumented interbody fusion for low-grade degenerative listhesis where indirect decompression suffices.
Viva & Exam Focus
P-S-O-A-SPSOAS — safe psoas traversal for XLIF
L-A-T-E-R-A-LLATERAL — XLIF indications, limits and risks
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old woman undergoes L4-5 XLIF for foraminal stenosis. On day 1 she has difficulty climbing stairs with 3/5 hip-flexion and knee-extension strength on the surgical side, sensation intact. What has happened and how do you manage her?”
“A 62-year-old man with L4-5 foraminal stenosis and grade I spondylolisthesis, diabetes (HbA1c 7.8%), BMI 34, asks about 'that less invasive sideways approach'. Would you offer him XLIF or TLIF at L4-5, and why?”
“A 67-year-old woman had an L3-4 XLIF 6 months ago for degenerative scoliosis with good early relief, but now has recurrent left leg pain; X-rays show 4mm of cage subsidence. How do you manage her?”
Plexus position by level (Benglis 2009)
- L1-2 and L2-3: ratio 0 and 0.11 — plexus most dorsal; anterior-to-mid disc is safest
- L3-4: ratio 0.18 — intermediate risk
- L4-5: ratio 0.28 — plexus most ventral, smallest safe window (highest risk)
- L5-S1: generally not feasible — iliac crest and iliac vessels block the corridor
Nerves at risk and how they present
- Lateral femoral cutaneous (L2-L3): anterolateral thigh numbness, meralgia paraesthetica — pure sensory, usually transient
- Genitofemoral (L1-L2): runs on the anterior psoas surface — anterior thigh or groin sensory symptoms
- Femoral (L2-L4): most serious — hip-flexor or quadriceps weakness; majority recover (Le/Uribe 2013)
- Obturator (L2-L4): less common — adductor weakness, medial thigh sensory loss
Key evidence
- Motor weakness 0.7-33.6%, sensory 0-75% across series, mostly transient (Ahmadian/Uribe 2012)
- Pooled anterior/lateral fusion 95.9% in MIS deformity (Phan 2016); fusion similar across approaches (Teng/Phan 2017)
- Indirect decompression: disc height +42%, foraminal area +24.7%, canal diameter +33% (Oliveira 2010)
- Subsidence halved by wider cages — 11% with 22mm vs 30% with 18mm (Marchi 2013)
Technique essentials
- Lateral decubitus, table break at the iliac crest, hips and knees flexed 30-45 degrees; left side up for L2-3/L3-4, right for L4-5
- Blunt sequential dilation parallel to psoas fibres with triggered EMG at each step
- Target the anterior third of the disc at L2-3/L3-4, middle third at L4-5; preserve the peripheral endplate rim
- Wide apophyseal-ring cage spanning both rims; supplemental posterior fixation for multilevel, deformity and osteoporotic bone
Complications and management
- Femoral neuropraxia (highest at L4-5): EMG at about 3 weeks, therapy, knee immobiliser if less than 3/5; exploration rarely needed
- Cage subsidence: wider cage plus posterior fixation plus treat osteoporosis
- Iliolumbar vein injury at L4-5: immediate laparotomy, vascular surgery, massive transfusion (1:1:1)
Exam traps
- XLIF and DLIF are transpsoas; ATP/pre-psoas (OLIF) work anterior to the psoas and largely avoid the plexus
- XLIF is generally not feasible at L5-S1 — use ALIF or TLIF
- Stand-alone XLIF subsides and pseudarthroses more without posterior fixation
- Fusion is comparable across approaches — choose by level, decompression need and deformity, not by fusion rate
References
Cadaveric Mapping of the Lumbosacral Plexus for the Transpsoas Approach
- Cadaveric dissection study mapping the lumbar contribution of the lumbosacral plexus relative to each lumbar disc using radio-opaque wire and lateral fluoroscopy.
- Plexus lies within the psoas substance and is most dorsal at L1-2, with progressive ventral migration caudally.
- Plexus position ratio (location from dorsal endplate divided by total disc length): 0 at L1-2, 0.11 at L2-3, 0.18 at L3-4, and 0.28 at L4-5.
- Posteriorly placed dilators and retractors risk plexus injury, especially at L4-5.
Postoperative Lumbar Plexus Injury After Transpsoas Lateral Interbody Fusion
- Single-surgeon retrospective review of 71 consecutive transpsoas MIS lateral interbody fusions (L1-L5).
- Immediate postoperative ipsilateral thigh numbness 19.1% (14/71); every case occurred in a construct that included L4-5.
- Annual numbness rate fell from 26.1% (2008) to 10.7% (2010) as technique was refined (about a 60% reduction) — a learning-curve effect.
- Immediate iliopsoas or quadriceps weakness in 54.9% (39/71), with 92.3% resolved by 3 months and complete resolution in all by 2 years.
Lumbar Plexopathies After Lateral Transpsoas Fusion: Diagnostic Standardisation
- Systematic review of 18 studies (2,310 patients) reporting plexus and nerve injury after the minimally invasive lateral retroperitoneal transpsoas approach.
- Documented nerve or root injury 0-3.4% and abdominal wall paresis up to 4.2%.
- Motor weakness reported across a wide range (0.7-33.6%) and sensory disturbance 0-75%, with marked inconsistency in definitions and reporting.
- The authors propose standardised sensory dermatomal zones and a diagnostic paradigm to classify postoperative lumbar plexopathies.
Meta-analysis Comparing ALIF, PLIF, TLIF and LLIF
- Systematic review and meta-analysis of 30 studies comparing the four major interbody approaches.
- Fusion rates were similar across ALIF, PLIF, TLIF and LLIF (no significant difference).
- ALIF gave the best postoperative disc height and segmental lordosis; TLIF gave better Oswestry Disability Index scores; PLIF had the greatest blood loss.
- Overall complication rates were similar between approaches, though comparative data on LLIF specifically were limited.
Radiographic Assessment of Indirect Decompression by the XLIF Procedure
- Prospective study of 21 patients (43 levels) treated with stand-alone XLIF for degenerative conditions with central and/or lateral stenosis; mean operative time 47 min, about 23mL blood loss per level.
- Mean dimensional gains: disc height +41.9%, foraminal height +13.5%, foraminal area +24.7%, central canal diameter +33.1%.
- No intraoperative complications; transient psoas weakness in 3 cases (14.3%); mean stay 29.5 hours.
- Two patients (9.5%) required a second procedure for additional posterior decompression and/or instrumentation.
Cage Subsidence After Stand-alone Lateral Interbody Fusion: Effect of Cage Width
- Prospective comparative study of stand-alone short-segment lateral interbody fusion: 46 patients (61 levels) with 18mm cages versus 28 patients (37 levels) with 22mm wide cages; 12-month follow-up.
- Subsidence graded 0-III by loss of postoperative disc height; at 12 months Grade II-III subsidence occurred in 30% of standard (18mm) versus 11% of wide (22mm) cages.
- Subsidence was detected early (by 6 weeks), correlated with transient clinical worsening, occurred predominantly (68%) at the inferior endplate, and did not progress after 6 weeks.
- Fusion rate was not affected by cage width or by the occurrence of subsidence; pain and disability improved similarly in both groups.